

Abstract
The case reported is of a 46 year old male who presented with a history of acute on chronic knee pain. The clinical features and investigations suggested a tear of the quadriceps tendon, with pre‐existing chronic calcific enthesopathy. The operative findings were of an acute collection of calcific material within the quadriceps tendon. This acute presentation and calcific collection have not previously been reported in the quadriceps tendon.
Keywords: calcific tendonitis, quadriceps
Calcific tendonitis most commonly affects the supraspinatus tendon of the shoulder. It has also been described around the wrist, hip, thigh, knee, ankle, and foot.1 Previous reports of calcific tendonitis of the quadriceps tendon have described whiskers2 and small flecks of calcium3 at the insertion into the patella. These reports have detailed changes on plain radiographs and computed tomography.4
We present here the case of a 46 year old man who presented with a history of acute on chronic knee pain. He had evidence of a chronic calcific enthesopathy and an acute collection of calcified material within the tendon. We believe that the latter variant of the condition and its radiological features have not previously been described.
Case report
A 46 year old healthy man presented one week after sudden onset knee pain, which occurred as he stumbled while walking. Self treatment with rest and analgesics had given no relief. He denied any constitutional symptoms.
The patient had suffered a rugby injury to the same knee seven years earlier. It was diagnosed as a partial quadriceps tendon rupture, based on an ultrasound examination. It was treated non‐operatively. Throughout the intervening years, the patient had chronic low grade pains in the knee.
On examination, the knee was cool with no erythema and a grade 1 effusion. There was tenderness of the quadriceps tendon but no palpable tendon defect. The patient was unable to perform a straight leg raise.
Plain radiographs of the knee showed whiskers of the superior aspect of the patella and an erosion near the quadriceps tendon insertion (fig 1).
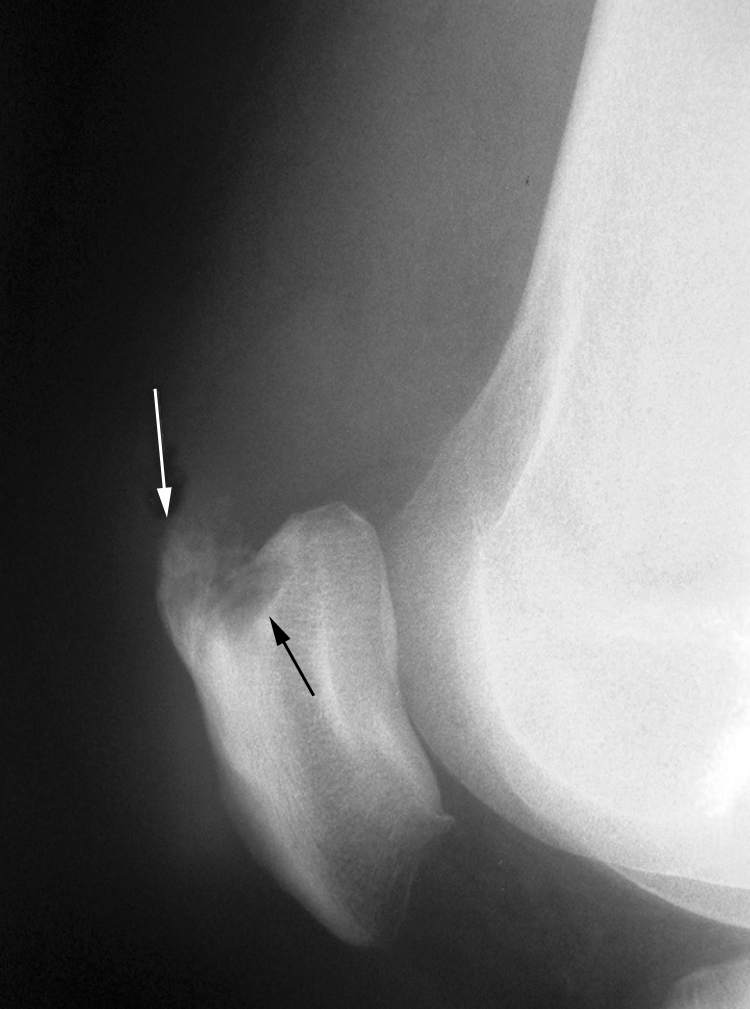
Figure 1 Lateral radiograph of the patella showing ill defined, new bone formation at the site of the quadriceps tendon insertion (white arrow). Patient consent has been obtained for publication of this figure.
Ultrasound examination of the knee showed at least a partly intact quadriceps tendon with a fluid collection within the tendon (fig 2). Magnetic resonance imaging (MRI) showed similar features with an encysted area of intermediate signal (fluid) within the distal quadriceps tendon (figs 3–5).
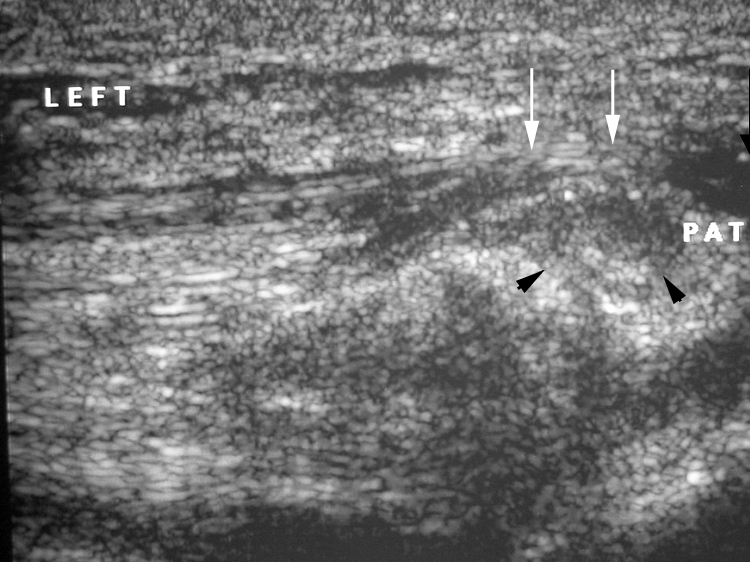
Figure 2 Sagittal ultrasound image showing anterior bulging of the distal quadriceps tendon (white arrows) over an ill defined soft tissue mass (arrowheads) close to the proximal pole of the patella (PAT). Patient consent has been obtained for publication of this figure.

Figure 3 (A) Sagittal T2 weighted magnetic resonance image showing encysted fluid (black arrow) within the distal quadriceps tendon (arrowhead). It is closely applied to a large erosion in the superior pole of the patella (white arrow). (B) Sagittal T1 weighted magnetic resonance image showing an encysted area of intermediate signal (fluid) within the distal quadriceps tendon (white arrow). There is a large erosion (black arrow) within the superior pole of the patella. Oedema is present in the adjacent soft tissue (arrowheads). Patient consent has been obtained for publication of this figure.

Figure 4 Coronal T1 weighted magnetic resonance image through the anterior patella. The quadriceps fibres (white arrowheads) have been displaced by mass (fluid) (arrow). Several small erosions (black arrowheads) are present at the proximal pole of the patella. Patient consent has been obtained for publication of this figure.
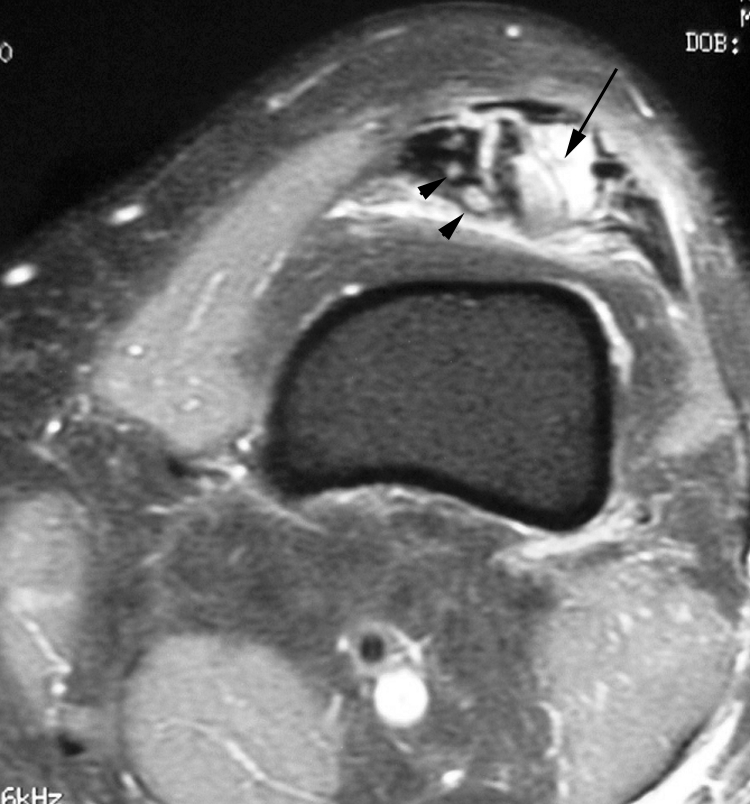
Figure 5 Axial T2 weighted magnetic resonance image showing that the large fluid filled cyst (arrow) is encased within the fibres of the distal quadriceps tendon, with several smaller cysts (arrowheads) seen within the adjacent tendon. Patient consent has been obtained for publication of this figure.
A working diagnosis of a partial rupture of the quadriceps tendon on a background of chronic calcific tendonitis was made. After an appropriate discussion with the patient, surgical exploration with a view to tendon repair was undertaken.
Intraoperatively, the findings were of a 4 cm diameter palpable collection within an intact quadriceps tendon. This was opened and revealed milky fluid and a chalky deposit of calcium similar to that typically found in calcific tendonitis of the shoulder. This collection was drained, and the cavity was washed out and curetted. In addition, there were small foci of calcified material at the insertion of the tendon in keeping with chronic enthesopathy.
Postoperatively there was spectacular relief of pain. This relief was maintained until follow up at six months when there was full function of the extensor mechanism.
Discussion
Calcific tendonitis is common around the shoulder where the calcified material forms a mass within the substance of the tendon. A few reports of the condition in the knee describe whiskers of calcification on the superior pole of the patella and flecks of calcification adjacent.1,2,3 These changes represent a chronic enthesopathy. One report described it in the patellar tendon.5 Plain radiographic and computed tomographic features are well described. MRI was described in only one of the studies.6
The collection seen on ultrasound and MRI was not seen on plain radiographs. This led to the assumption that the collection represented a haematoma as a feature of an acute injury to the tendon. In an acute presentation of calcification of the soft tissues where the calcium is still in a liquid form, it is radiolucent. The MRI showed signs of acute inflammatory reaction in the soft tissues around the deposit.
This is, to our knowledge, the first description of a calcific tendonitis of the quadriceps presenting clinically as a suspected tendon rupture. The calcific mass may be invisible on plain radiograph, in its acute phase. Calcific tendonitis should be part of differential diagnosis of acute dysfunction of the extensor mechanism of the knee with atypical findings.
Footnotes
Competing interests: none declared
Patient consent has been obtained for publication of the figures.
References
- 1.Holt P D, Keats T E. Calcific tendonitis: a review of the usual and unusual. Skeletal Radiol 1993221–9. [DOI] [PubMed] [Google Scholar]
- 2.Trujeque L. Patellar whiskers and acute calcific quadriceps tendonitis in a general hospital population. Arthritis Rheum 1977201409–1412. [DOI] [PubMed] [Google Scholar]
- 3.Macurak R B, Goldman J A, Hirsh E.et al Acute calcific quadriceps tendonitis. South Med J 198073322–325. [DOI] [PubMed] [Google Scholar]
- 4.Archer B D, Friedman L, Stilgenbauer S.et al Symptomatic calcific tendinitis at unusual sites. Can Assoc Radiol J 199243203–207. [PubMed] [Google Scholar]
- 5.Dey A, Godsiff S P, Pandey R. Acute calcific tendinitis mimicking patella tendon rupture. Injury Extra 200435104–107. [Google Scholar]
- 6.Ramon F A, Degryse H R, De Schepper A M.et al Calcific tendonitis of the vastus lateralis muscle. A report of three cases. Skeletal Radiol 19912021–23. [DOI] [PubMed] [Google Scholar]