

Abstract
Streptococcus pneumonia and Haemophilus influenzae account for more than 50% of bacterial acute sinusitis. Isolated sphenoid sinusitis is a rare disease with potentially devastating complications such as cranial nerve involvement, brain abscess, and meningitis. It occurs at an incidence of about 2.7% of all sinus infections. There have been no previous reported cases of unilateral sphenoid sinusitis presenting as septicaemia in an otherwise healthy young immunocompetent adult.
Keywords: headache, Haemophilus septicaemia , sphenoid sinusitis
A 42 year old meat inspector presented with a 2 week history of worsening headache and a high temperature. He had no history of any significant illness except mild asthma controlled with inhalers. Physical and neurological examinations were unremarkable on the day of presentation.
In view of his pyrexia, septic screen including full blood count, urea and electrolytes, liver function tests, blood culture, mid‐stream urine culture, chest x ray, and lumbar puncture were performed. Blood result showed a raised white blood cell count and a raised C‐reactive protein. Chest x ray was normal. CSF was clear and showed no growth of any pathogens after 48 h. The blood cultures were positive for Haemophilus influenzae confirming the diagnosis of septicaemia.
After receiving intravenous antibiotics the patient showed remarkable improvement and was discharged home in a satisfactory condition.
However, he returned 2 weeks later with severe headache. A CT scan of his head was requested which showed an isolated right sphenoid opacification with a rounded mass within the sphenoid sinus close to the ostium (fig 1A,B).

Figure 1 (A) CT scan showing opacity and mass in the right sphenoid sinus. (B) CT scan showing a mass occluding the sphenoid sinus ostium.
Subsequently, the patient underwent right sphenoidotomy, which revealed a yellow coloured polypoid mass in the sphenoethmoidal recess with pus extruding below it (fig 2). The ostium was opened and at least 10 ml of pus aspirated. The polypoid mass was sent for histology and the pus for culture. Histology confirmed the diagnosis of inflammatory polyp. Culture failed to grow any pathogen.

Figure 2 Pus and inflammatory mass at the sphenoid sinus ostium.
On a subsequent visit the patient reported to be asymptomatic and a repeat CT scan of the sinuses 2 weeks post operation showed clear sphenoid sinus (fig 3).
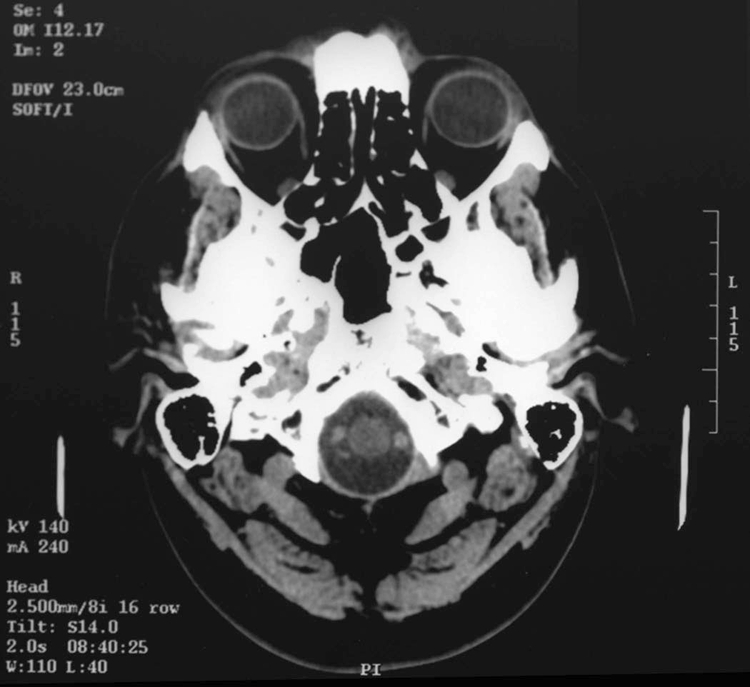
Figure 3 Post operation CT showing normal aerated sphenoid sinus.
Discussion
Streptococcus pneumonia and H influenzae account for more than 50% of bacterial acute sinusitis.1H influenzae grows both aerobically and anaerobically and is an exclusively human pathogen. The organism is spread by airborne droplets or by direct contact with secretions or fomites. Non‐typable strains colonise the upper respiratory tract of up to three fourths of healthy adults.
The main symptom of sinusitis is a throbbing pain and pressure around the eyeball, which is made worse by bending forwards. Although the sphenoid sinuses are less frequently affected, infection in this area can cause earache, neck pain, or an ache behind the eyes, at the top of the head, or in the temples. In addition, drainage of mucus from the sphenoid down the back of the throat (postnasal drip) can cause a sore throat and can irritate the membranes lining the larynx.
Isolated sphenoid sinusitis is a rare disease with potentially devastating complications such as cranial nerve involvement, brain abscess, and meningitis. It occurs at an incidence of about 2.7% of all sinus infections.2 Although headache is the most common presentation symptom, there is no typical headache pattern.2
There have been reported cases of isolated sphenoid sinusitis presenting with unilateral VI nerve palsy in children,3 isolated fungal granuloma presenting with III nerve palsy,4 acute pansinusitis with bacteraemia due to beta‐haemolytic group C streptococcus,5 and isolated Cryptococcus sphenoid sinusitis with septicaemia, meningitis, and skull base osteomyelitis,6 but there are no reported cases of unilateral sphenoid sinusitis presenting as septicaemia in an otherwise healthy young immunocompetent adult.
Disease of the sphenoid sinus is often vague and non‐specific in its clinical presentation. Therefore, the physician must maintain a high index of suspicion when evaluating patients who present with such non‐specific symptoms.7
Footnotes
Competing interests: none declared
References
- 1.Gwaltney J M., Jr Acute community‐acquired sinusitis. Clin Infect Dis 1996231209–1225. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Ng Y T, Butler I J. Sphenoid sinusitis masquerading as migraine headaches in children. J Child Neurol 200116(12)882–884. [DOI] [PubMed] [Google Scholar]
- 3.Ada M, Kaytaz A, Tuskan K.et al Isolated sphenoid sinusitis presenting with unilateral VIth nerve palsy. Int J Pediatr Otorhinolaryngol 200468(4)507–510. [DOI] [PubMed] [Google Scholar]
- 4.Petrick M, Honegger J, Daschner F.et al Fungal granuloma of the sphenoid sinus and clivus in a patient presenting with cranial nerve III paresis: case report and review of the literature. Neurosurgery 200352(4)955–958. [DOI] [PubMed] [Google Scholar]
- 5.El‐Guizaoui A E, Watanakunakorn C. Acute pansinusitis with bacteremia due to a beta‐hemolytic group C streptococcus: Streptococcus milleri. South Med J 199790(12)1248–1249. [DOI] [PubMed] [Google Scholar]
- 6.Prendiville S, Bielamowicz S, Hawrych A.et al Isolated cryptococcal sphenoid sinusitis with septicaemia, meningitis and subsequent skull base osteomyelitis in an immunocompetent patient. Otolaryngol Head Neck Surg 2000123277–279. [DOI] [PubMed] [Google Scholar]
- 7.Grillone G A, Kasznica P. Isolated sphenoid sinus disease. Otolaryngol Clin North Am 200437(2)435–451. [DOI] [PubMed] [Google Scholar]