

Abstract
Objectives
Clinical guidelines recommend that when breast-conserving surgery is provided as primary therapy for early-stage breast cancer, radiation therapy should follow. We do not know whether racial/ethnic disparities in this therapy exist and how disparities may have changed over time.
Design and Patients
We studied 89,110 women who were diagnosed with incident early-stage (American Joint Committee on Cancer stages I-II) breast cancer at ≥20 years of age from 1992 through 2002 in 12 geographic areas of the National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) tumor registries. These women had no history of other cancers and received breast-conserving surgery. Of these subjects, 81,577 (91.5%) were Caucasians and 7,533 (8.5%) were African Americans.
Results
From 1992 to 2002, the percentage of cases who received breast-conserving surgery without radiotherapy increased from 10.8% to 19.8% for Caucasian women and from 13.6% to 27.7% for African Americans. The gap between African American and Caucasian women slightly increased during this period. When data were controlled for patient and tumor characteristics, year of diagnosis, and geographic area, African American women were 24% less likely than Caucasians to receive the recommended therapy (95% confidence interval: 1.18-1.32).
Conclusions
Although current clinical guide-lines recommend that women with early-stage breast cancer who are treated with breast-conserving surgery should have subsequent radiation therapy, the percentage of women who did not receive this regimen increased from 1992 to 2002. The gap between African American and Caucasian women has continued from 1992 to 2002.
Keywords: Breast Cancer, Racial Disparity, Radiotherapy, Surgery, Treatment
Introduction
Evidence of racial and ethnic disparities in health care is consistent across a range of diseases and healthcare services as recently reported by the Institute of Medicine.1 Because these disparities in health care may lead to poorer quality of care and subsequently poorer outcomes (including poorer survival),1-11 one of the goals of Healthy People 2010 is to eliminate racial/ethnic disparities in health care.3
A major racial difference in health care exists for women diagnosed with breast cancer. Breast cancer is the most commonly diagnosed cancer in women both in Caucasian and African American women in the United States.12-14 Numerous studies consistently demonstrated that African American women, compared to Caucasian women with breast cancer, were more likely to be diagnosed with breast cancer at a late stage,15-23 less likely to receive the standard of care,24-29 and more likely to die.4-11,30-32 However, few studies have addressed how the treatment of breast cancer has changed over time on the basis of racial difference.
The recommended medical care for breast cancer underwent radical changes at the end of the last century. For many decades, mastectomy was the standard of care for women with early-stage breast cancer. By the middle 1980s, breast-conserving surgery had been consistently demonstrated to provide equivalent efficacy to traditional mastectomy
Few studies have addressed how the treatment of breast cancer has changed over time on the basis of racial difference.
in large clinical trials in the United States and around the world.33-37 On the basis of this strong evidence, the National Institutes of Health and many authoritative medical professional societies recommended breast-conserving surgery for women with early-stage breast cancer in the early 1990s.38 Previous studies showed that nearly 50% of women with early-stage breast cancer received breast-conserving surgery by the 1990s.39-42 According to the evidence and clinical guidelines, breast-conserving surgery should be followed by radiation therapy.38 In other words, if women with breast cancer underwent breast-conserving surgery, they should receive radiation after surgery in order to minimize disease recurrence.
We studied the treatment regimens of a large cohort of women diagnosed with early-stage (stage I-II) breast cancer from 1992 through 2002 to determine whether racial/ethnic disparities in primary treatment for breast cancer changed over time from 1992 to 2002. These cases were identified from the nationwide, population-based Surveillance, Epidemiology, and End Results (SEER) cancer registry data. Results of this study may help identify racial disparities in health care, specifically for breast cancer patients. The study may also add to our understanding of the factors contributing to those disparities and may lead to the development of policy or institutional changes that can address these differences.
Patients and Methods
Data Sources
Data used in this paper were from the National Cancer Institute’s SEER 1992-2002 Public Use Data Set (CD-ROM) released in April 2005.43 The SEER program supports population-based tumor registries in seven metro-politan areas (San Francisco/Oakland, Detroit, Atlanta, Seattle, San Jose-Monterey, Los Angeles, and rural Georgia) and five states (Connecticut, Iowa, New Mexico, Utah, and Hawaii), covering >14% of the US population. The registries ascertain all newly diagnosed (incident) breast cancer cases from multiple reporting sources, such as hospitals, outpatient clinics, laboratories, private medical practitioners, nursing/convalescent homes, hospices, autopsy reports, and death certificates. Information includes tumor location and size; lymph node and distant organ metastases; histologic type and grade of tumor; demographic characteristics such as age, sex, race and marital status; and type of treatments provided in the first course of therapy (within four months of initial therapy after diagnosis). The SEER public use dataset also includes information on the types of surgical procedures and radiation therapy received.
Study Population
We identified 89,110 women who were diagnosed with incident early-stage (American Joint Committee on Cancer [AJCC] stage I-II) breast cancer at ≥20 years of age from 1992 through 2002 in 12 SEER areas; these patients had no history of other cancers and received breast-conserving surgery only. Of these 89,110 subjects, 81,577 (91.5%) were Caucasians and 7,533 (8.5%) were African Americans. We studied cases diagnosed with breast cancer from 1992 through 2002 because cases from 12 SEER areas only became available since 1992, although cases from 9 of these areas were available since the late 1970s. The Committee for Protection of Human Subjects at the University of Texas Health Science Center at Houston approved this study.
Study Variables
Tumor and Patient Characteristics
Tumor and patient characteristics included tumor size (categorized as <1.0, 1.0-<2.0, 2.0-<3.0, 3.0-<4.0, ≥4.0 cm or unknown); stage (AJCC stages I and II); tumor grade (well, moderately, and poorly differentiated or unknown); hormone-receptor status (estrogen- or progesterone-receptor positive, negative, or unknown); number of positive lymph nodes; age at diagnosis (<45, 45-49, 50-54, 55-59, 60-64, 65-74, 75-79, or ≥80 years); marital status (married, unmarried, or unknown marital status); race/ethnicity (Caucasian or African American); time period (1992 to 2002); and geographic area (12 SEER regions).43
Treatment for Breast Cancer
Breast-conserving surgery was defined as receiving segmental mastectomy, lumpectomy, quadrantectomy, tylectomy, wedge resection, nipple resection, excisional biopsy, or partial mastectomy unspecified (SEER surgery codes 10-29).44 SEER records radiation therapy provided within four months after diagnosis. Radiation therapy included beam radiation, radioactive implants, brachytherapy, radioisotopes, or other radiation.44
Data Analysis
Initial descriptive analyses generated the rates of women who received breast-conserving surgery but no radiation therapy by patient and tumor characteristics, SEER areas, and the year of diagnosis. The test for linear trend from 1992 to 2002 for differences in the rates of breast-conserving surgery without radiation therapy was performed with an ordinary linear square regression model. Logistic regression models were used to assess the effects of time and ethnicity on the likelihood of receiving breast-conserving surgery without radiotherapy. In these multivariate analyses, the odds ratios of receiving breast-conserving surgery without radiation therapy were adjusted for age, race, marital status, cancer stage, tumor size, number of positive lymph nodes, hormone-receptor status, time period, and geographic area. All analytical procedures were performed by using the SAS software package.45
Results
Table 1 presents the distribution of patient and tumor characteristics between African American and Caucasian patients who were diagnosed with early-stage (stage I-II) breast cancer between 1992 and 2002 in the 12 SEER regions in the United States. Median age for African American women with breast cancer at diagnosis was 55 years and ranged from 20 to 106 years, whereas median age for Caucasians was 61 years and ranged from 20 to 107 years. A greater proportion of cases were diagnosed at younger age in African American women than in Caucasian women. For example, 21.7% of African American women had breast cancer diagnosed at ≤45 years of age and 6.1% diagnosed at ≥80 years of age, compared to 13.5% and 10.7%, respectively, in Caucasian women. More than 58% of Caucasian women were married at the time of diagnosis, compared to 38% of African American women. Significantly higher percentages of African American women were diagnosed at higher tumor stage, larger tumor size, and higher tumor grade; African American women had more hormone receptor-negative tumors and more positive lymph nodes at diagnosis than did Caucasian women.
Table 1.
Comparison of patient and tumor characteristics between Caucasian and African American women diagnosed with early-stage (stage I-II) breast cancer
| Patient or Tumor Characteristic | Caucasians |
African Americans |
P value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| Age (years) | <.001 | ||||
| <45 | 10,201 | 12.5 | 1543 | 20.5 | |
| 45-49 | 9028 | 11.1 | 1038 | 13.8 | |
| 50-54 | 10,431 | 12.7 | 1082 | 14.4 | |
| 55-59 | 9857 | 12.1 | 898 | 11.9 | |
| 60-64 | 9021 | 11.1 | 782 | 10.4 | |
| 65-69 | 8959 | 11.0 | 659 | 8.8 | |
| 70-74 | 8660 | 10.6 | 587 | 7.8 | |
| 75-79 | 7308 | 9.0 | 493 | 6.5 | |
| ≥80 | 8112 | 9.9 | 451 | 6.0 | |
| Marital status | <.001 | ||||
| Married | 48,225 | 59.1 | 3008 | 39.0 | |
| Unmarried | 31,479 | 38.6 | 4275 | 56.8 | |
| Unknown | 1873 | 2.3 | 250 | 3.3 | |
| Tumor AJCC stage | <.001 | ||||
| Stage I | 53,737 | 65.9 | 3986 | 52.9 | |
| Stage II | 27,840 | 34.1 | 3547 | 47.1 | |
| Tumor size (cm) | <.001 | ||||
| <1.0 | 20394 | 25.0 | 1262 | 16.8 | |
| 1.0-<2.0 | 37728 | 46.3 | 3072 | 40.8 | |
| 2.0-<3.0 | 16125 | 19.8 | 1921 | 25.5 | |
| 3.0-<4.0 | 4594 | 5.6 | 787 | 10.5 | |
| ≥4.0 | 2367 | 2.9 | 450 | 6.0 | |
| Unknown size | 369 | .5 | 41 | .5 | |
| Tumor grade | <.001 | ||||
| Well differentiated | 17,819 | 21.8 | 960 | 12.7 | |
| Moderately differentiated | 31,907 | 39.1 | 2332 | 31.0 | |
| Poorly differentiated | 22,777 | 27.8 | 3179 | 42.2 | |
| Unknown | 9074 | 11.2 | 1062 | 14.1 | |
| Hormone-receptor status | <.001 | ||||
| Positive | 58,340 | 71.5 | 4137 | 54.9 | |
| Negative | 11,729 | 14.4 | 2054 | 27.3 | |
| Unknown | 11,508 | 14.1 | 1342 | 17.8 | |
| Number of positive nodes | <.001 | ||||
| 0 (Node negative) | 51,162 | 62.7 | 4300 | 57.1 | |
| 1 | 7672 | 9.4 | 862 | 11.4 | |
| 2-5 | 6119 | 7.5 | 762 | 10.1 | |
| ≥6 | 1907 | 2.3 | 277 | 3.7 | |
| Unknown numbers | 14,717 | 18.0 | 1332 | 17.7 | |
| Total | 81,577 | 100.0 | 7533 | 100.0 | |
AJCC=American Joint Committee on Cancer.
Table 2 presents the crude and age-adjusted rates of receiving breast-conserving surgery without radiation therapy by both African American and Caucasian women with breast cancer. The rate was age-adjusted to the case population in 2002 among Caucasians. The percentage of patients who received breast-conserving surgery without radiotherapy increased from 24.7% in 1992 to 30.8% in 2002 for Caucasian women with breast cancer (P<.001 for trend) and from 34.0% to 44.7% for African American women (P<.001 for trend). The disparities between African American and Caucasian women were 10.5% overall and slightly increased over time. This disparity and change over time are illustrated in Figure 1.
Table 2.
The crude and age-adjusted percentage of women who received breast-conserving surgery without radiation therapy for early-stage breast cancer over time in Caucasians compared to African Americans
| Year of Diagnosis | Total Number of Cases with BCS and % Without Radiation in Caucasians |
Total Number of Cases with BCS and Percent (%) without Radiation in African Americans |
Disparity Between African Americans and Caucasians |
|||||
|---|---|---|---|---|---|---|---|---|
| n | % Without Radiation | Age-Adjusted* % Without Radiation | n | % Without Radiation | Age-Adjusted % Without Radiation | Crude Rate | Age-Adjusted Rate | |
| 1992 | 4767 | 26.0 | 24.7 | 425 | 34.1 | 34.0 | 8.1 | 9.3 |
| 1993 | 5187 | 26.0 | 24.8 | 442 | 33.3 | 35.8 | 7.3 | 11.0 |
| 1994 | 5608 | 23.8 | 23.5 | 517 | 32.9 | 33.9 | 9.1 | 10.4 |
| 1995 | 6184 | 23.2 | 22.5 | 592 | 27.7 | 28.0 | 4.5 | 5.5 |
| 1996 | 6893 | 24.2 | 23.9 | 641 | 33.2 | 33.0 | 9.0 | 9.1 |
| 1997 | 7658 | 27.0 | 26.4 | 709 | 38.8 | 38.5 | 11.8 | 12.1 |
| 1998 | 8417 | 22.8 | 22.6 | 787 | 31.6 | 32.1 | 8.8 | 9.5 |
| 1999 | 8816 | 26.1 | 25.6 | 806 | 35.4 | 36.7 | 9.3 | 11.1 |
| 2000 | 9150 | 28.0 | 27.8 | 860 | 39.5 | 40.1 | 11.5 | 12.3 |
| 2001 | 9292 | 28.9 | 28.8 | 824 | 40.7 | 40.9 | 11.8 | 12.1 |
| 2002 | 9605 | 30.8 | 30.8 | 930 | 44.4 | 44.7 | 13.6 | 13.9 |
| Total | 81,577 | 26.4 | 26.0 | 7533 | 36.3 | 36.9 | 10.5 | 10.9 |
Percentages were age-adjusted for the Caucasian women diagnosed in 2002 (in five-year age interval from <40 to ≥80 years).
BCS=breast conserving surgery.
Fig 1.
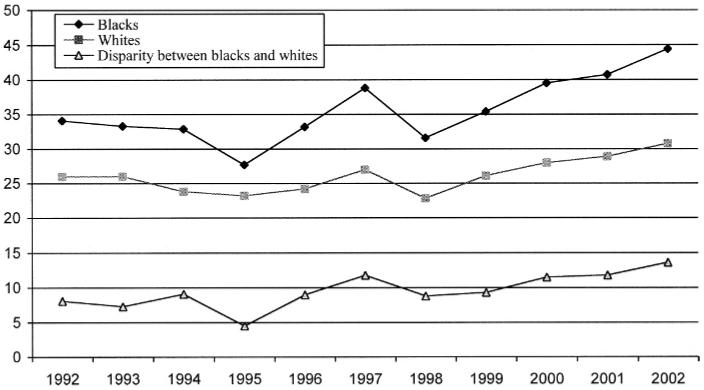
Racial difference and trend in receipt of breast-conserving surgery without radiation thearpy for breast cancer from 1992-2002
Table 3 presents how this disparity has persisted over time, which was stratified by age groups. Overall, disparity between African American and Caucasian women on the use of breast-conserving surgery without radiation was 8.5% in 1992-1997 and 11.1% in 1998-2002. Stratified analyses by age showed that the disparity increased only in women ≥50 years of age, whereas the gap slightly decreased for women <50 years old. In the analysis stratified by race and year of diagnosis, the increased percentage of women <50 years of age who received no radiation was greater in Caucasians (from 20.8% in 1992 to 34.1% in 2002) than in African Americans (from 35.0% to 47.3%), whereas in those women ≥50 years of age, the increase was greater in African Americans (from 33.6% to 43.2%) than in Caucasian (from 27.8% to 29.9%).
Table 3.
Disparity and change over time in percentage of women who received breast-conserving surgery without radiation therapy in Caucasians compared to African Americans
| Age (years) | Percent of BCS Without Radiation Therapy in 1992-1997 |
Percent of BCS Without Radiation Therapy in 1998-2002 |
Change in Disparity Over Time | ||||
|---|---|---|---|---|---|---|---|
| Whites | Black | Disparity | Whites | Black | Disparity | ||
| <50 | 22.9 | 33.7 | 10.8 | 28.0 | 38.2 | 10.2 | -.6 |
| 50-59 | 18.3 | 29.0 | 10.7 | 23.8 | 37.1 | 13.3 | +2.6 |
| 60-69 | 17.7 | 25.5 | 7.8 | 21.2 | 35.8 | 14.6 | +6.8 |
| ≥70 | 37.4 | 44.9 | 7.5 | 35.1 | 44.1 | 9.0 | +1.5 |
| All patients | 25.0 | 33.5 | 8.5 | 27.5 | 38.6 | 11.1 | +2.6 |
BCS=breast conserving surgery.
Table 4 presents five different models for the comparison between African American and Caucasian patients on the receipt of breast-conserving surgery without radiation therapy for breast cancer and for the comparison among patients diagnosed from 1992 to 2002, while controlling for patient and tumor characteristics as well as geographic area. Regardless of age, marital status, tumor stage, size, grade, hormone receptor status, node positivity, year of diagnosis, and geographic area, African American women were significantly more likely than Caucasian women to receive this surgery without radiation therapy. After adjusting for all above variables, African American women were 24% less likely to receive breast-conserving surgery followed by radiation therapy than Caucasian women with early-stage breast cancer (1.18-1.32). Patients diagnosed in recent years were significantly more likely to receive conserving surgery without radiation therapy.
Table 4.
Stratified and multivariable analyses on receiving breast-conserving surgery without radiation therapy in Caucasian women compared to African Americans with breast cancer
| Patient and Tumor Characteristics | Odds Ratio (95% Confidence Interval) of Receiving Breast Conserving Surgery Without Radiation Therapy |
||||
|---|---|---|---|---|---|
| Model 1* | Model 2 | Model 3 | Model 4 | Model 5 | |
| Race/Ethnicity | |||||
| Caucasians | 1.00 | 1.00 | 1.00 | 1.00 | 1.00 |
| African Americans | 1.59 (1.52-1.67) | 1.60 (1.52-1.68) | 1.63 (1.55-1.72) | 1.44 (1.36-1.52) | 1.24 (1.18-1.32) |
| Year of Diagnosis | |||||
| 1992 | - | 1.00 | 1.00 | 1.00 | 1.00 |
| 1993 | - | .99 (.91-1.09) | 1.00 (.92-1.10) | 1.02 (.93-1.12) | 1.02 (.93-1.12) |
| 1994 | - | .89 (.82-.97) | .92 (.84-1.00) | .92 (.84-1.01) | .93 (.84-1.02) |
| 1995 | - | .85 (.78-.92) | .86 (.79-.93) | .85 (.78-.94) | .87 (.79-.95) |
| 1996 | - | .92 (.84-.99) | .94 (.86-1.02) | .98 (.90-1.07) | 1.00 (.91-1.09) |
| 1997 | - | 1.07 (.98-1.16) | 1.10 (1.02-1.20) | 1.17 (1.08-1.28) | 1.21 (1.11-1.32) |
| 1998 | - | .85 (.78-.92) | .87 (.81-.95) | .97 (.89-1.06) | 1.00 (.92-1.09) |
| 1999 | - | 1.01 (.94-1.09) | 1.04 (.96-1.13) | 1.24 (1.14-1.35) | 1.27 (1.17-1.38) |
| 2000 | - | 1.13 (1.04-1.21) | 1.17 (1.08-1.27) | 1.44 (1.33-1.56) | 1.48 (1.36-1.61) |
| 2001 | - | 1.18 (1.09-1.27) | 1.23 (1.14-1.33) | 1.60 (1.47-1.74) | 1.65 (1.51-1.78) |
| 2002 | - | 1.29 (1.20-1.39) | 1.39 (1.29-1.50) | 1.85 (1.70-2.00) | 1.94 (1.79-2.11) |
Model 1 was without adjustment for other factors.
Model 2 adjusted for the year of diagnosis.
Model 3 adjusted for patient age (nine categories in five-year interval), marital status, in addition to factor in Model 2.
Model 4 adjusted for tumor stage, size, grade, number of positive lymph nodes, in addition to factors in Model 3.
Model 5 adjusted for the geographic areas (12 SEER regions), in addition to factors in Model 4.
Discussion
This study compared the differences in breast cancer treatment for African American and Caucasian patients with early-stage breast cancer. We found that African American women were less likely to receive radiation therapy after breast conserving surgery, regardless of the year of diagnosis and patient or tumor characteristics. The percentage of
We found that African American women were less likely to receive radiation therapy after breast conserving surgery, regardless of the year of diagnosis and patient or tumor characteristics.
patients who did not receive radiation increased over time for both ethnic groups. This African American and Caucasian gap continued over time from 1992 to 2002.
Differences in breast cancer treatment between African American and Caucasian patients have been documented in numerous studies.1,24-29 The Institute of Medicine’s report in 2002 described the extent of racial and ethnic disparities in health care and concluded that racial/ethnic disparities in the quality of health care do exist, even after controlling for stage of disease presentation, co-morbidity, age, insurance status, and income.1 Physicians with different backgrounds may have played a role in these racial disparities in healthcare delivery.46 Reports also indicated that minority patients may be more likely to refuse recommended care than Caucasians.1
From 1992 to 2002, we saw a substantial increase in the use of breast conserving surgery. Unfortunately, the percentage of patients who received concomitant radiotherapy decreased over time because the use of breast conserving surgery increased over time at a sharper rate than did the use of radiation therapy after surgery.47,48 Because breast-conserving surgery requires less surgical equipment than does traditional mastectomy, technology could have diffused more quickly.42 Purchasing and maintaining technology for radiation therapy, however, often requires a major commitment that is usually under control of hospital administration. In addition, radiotherapy is often administered daily (five days per week) for five weeks at outpatient clinics, which requires commitments from the patient and her family members, and may also be associated with increased cost. Because information on socioeconomic factors was not available in this dataset, we cannot say whether socioeconomic factors may have explained all or part of the racial disparities we noted.
Although not confirmed in randomized controlled clinical trials, observational studies showed that the receipt of breast-conserving surgery without radiation therapy was associated with decreased survival.49 Further study is needed to examine whether the difference in this therapy between African American and Caucasian women with breast cancer contributes to the racial disparities in mortality.
This study has several limitations. First, we do not have information on patients’ socioeconomic status (eg, insurance and income) and their personal or cultural preferences. Therefore, we cannot say whether the ethnic differences in the receipt of breast conserving surgery without radiotherapy might be explained by the differences in insurance, income, and preferences. Second, information on radiation therapy from SEER registries may have been slightly underestimated according to previous studies,50,51 but this underestimation, if any, was unlikely to be differential between African Americans and Caucasians over time. Third, we did not have information on physician and hospital characteristics, which are associated with the receipt of recommended care for breast cancer. Fourth, we could not control for patient factors that led to the selection of a specific treatment, particularly co-morbidity, functional status, and individual preferences. In addition, we could not assess the use of other therapies such as adjuvant chemotherapy and hormonal therapy, since these systematic therapies may be used to control disease recurrence and achieve a similar goal as radiation therapy. We also do not have information on mammography-detected early-stage tumors, which may vary between racial/ethnic groups. However, these should have minimum effect on radiation therapy that is recommended to follow breast-conserving surgery in those diagnosed with stages I-II, not including in situ tumors. In addition, although we adjusted for tumor size, residual confounding may not have been fully controlled in the analysis. Finally, although the study population is a large cohort of women from the 12 SEER areas, the study findings may not be generalizable to the entire United States.
In conclusion, the percentage of women who were treated with breast-conserving surgery without radiation therapy for early-stage breast cancer has increased over a 10-year period for both African American and Caucasian women. The gap between these two racial/ethnic groups has continued from 1992 to 2002.
Acknowledgments
This study was supported by a grant from the National Cancer Institute (R01-CA090626 to XLD), and BJG was supported in part by a grant from the National Center for Minority Health and Health Disparities (P60-MD000503). We acknowledge the efforts of the National Cancer Institute in the creation of the SEER cancer registry data for public use, and sincerely thank Monica Rasmus for her editorial review and assistance.
References
- 1.Institute of Medicine . Unequal Treatment: Confronting Racial and Ethnic Disparities in Health Care. National Academy Press; Washington, DC: 2002. [Google Scholar]
- 2.American College of Physicians Racial and ethnic disparities in health care: a position paper of the American College of Physicians. Ann Intern Med. 2004;141:226–232. doi: 10.7326/0003-4819-141-3-200408030-00015. [DOI] [PubMed] [Google Scholar]
- 3.US Department of Health and Human Services . Healthy People 2010: Understanding and Improving Health. 2nd ed. US Government Printing Office; Washington, DC: Nov, 2000. [Google Scholar]
- 4.Shavers VL, Harlan LC, Stevens JL. Racial/ethnic variation in clinical presentation, treatment, and survival among breast cancer patients under age 35. Cancer. 2003;97:134–147. doi: 10.1002/cncr.11051. [DOI] [PubMed] [Google Scholar]
- 5.Bradley CJ, Given CW, Roberts C. Disparities in cancer diagnosis and survival. Cancer. 2001;91:178–188. doi: 10.1002/1097-0142(20010101)91:1<178::aid-cncr23>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- 6.Bradley CJ, Given CW, Roberts C. Race, socioeconomic status, and breast cancer treatment and survival. J Natl Cancer Inst. 2002;94:490–496. doi: 10.1093/jnci/94.7.490. [DOI] [PubMed] [Google Scholar]
- 7.Yood MU, Johnson CC, Blount A, et al. Race and differences in breast cancer survival in a managed care population. J Natl Cancer Inst. 1999;91:1487–1491. doi: 10.1093/jnci/91.17.1487. [DOI] [PubMed] [Google Scholar]
- 8.Li CI, Malone KE, Daling JR. Differences in breast cancer stage, treatment, and survival by race and ethnicity. Arch Intern Med. 2003;163:49–56. doi: 10.1001/archinte.163.1.49. [DOI] [PubMed] [Google Scholar]
- 9.Clegg LX, Li FP, Hankey BF, Chu K, Edwards BK. Cancer survival among US whites and minorities: a SEER (surveillance, epidemiology, and end results) program population-based study. Arch Intern Med. 2002;162:1985–1993. doi: 10.1001/archinte.162.17.1985. [DOI] [PubMed] [Google Scholar]
- 10.Hershman D, McBride R, Jacobson JS, et al. Racial disparities in treatment and survival among women with early-stage breast cancer. J Clin Oncol. 2005;23:6639–6646. doi: 10.1200/JCO.2005.12.633. [DOI] [PubMed] [Google Scholar]
- 11.Tammemagi CM, NerenzDavid, Neslund-Dudas C, Feldkamp C, Nathanson D. Comorbidity and survival disparities among Black and White patients with breast cancer. JAMA. 2005;294:1765–1772. doi: 10.1001/jama.294.14.1765. [DOI] [PubMed] [Google Scholar]
- 12.Hankinson S, Hunter D. Breast cancer. In: Adami HO, Hunter D, Trichopoulos D, editors. Textbook of Cancer Epidemiology. Oxford University Press; New York, NY: 2002. pp. 301–339. [Google Scholar]
- 13.Ries LAG, Eisner MP, Kosary CL, et al. SEER cancer statistics review, 1975-2002. National Cancer Institute; [Accessed on: 5/24/05]. Available at: http://seer. cancer.gov/csr/1975_2002. [Google Scholar]
- 14.Jemal A, Clegg LX, Ward E, et al. Annual report to the nation on the status of cancer, 1975-2001, with a special feature regarding survival. Cancer. 2004;101:3–27. doi: 10.1002/cncr.20288. [DOI] [PubMed] [Google Scholar]
- 15.Henson DE, Chu KC, Levine PH. Histologic grade, stage, and survival in breast carcinoma: comparison of Black and White women. Cancer. 2003;98:908–917. doi: 10.1002/cncr.11558. [DOI] [PubMed] [Google Scholar]
- 16.Elmore JG, Nakano CY, Linden HM, et al. Racial inequities in the timing of breast cancer detection, diagnosis, and initiation of treatment. Med Care. 2005;43:141–148. doi: 10.1097/00005650-200502000-00007. [DOI] [PubMed] [Google Scholar]
- 17.Chlebowski RT, Chen Z, Anderson GL, et al. Ethnicity and breast cancer: factors influencing differences in incidence and outcome. J Natl Cancer Inst. 2005;97:439–448. doi: 10.1093/jnci/dji064. [DOI] [PubMed] [Google Scholar]
- 18.Lannin DR, Mathews HF, Mitchell J, Swanson MS, Swanson FH, Edwards MS. Influence of socioeconomic and cultural factors on racial differences in late-stage presentation of breast cancer. JAMA. 1998;279:1801–1807. doi: 10.1001/jama.279.22.1801. [DOI] [PubMed] [Google Scholar]
- 19.Hunter CP, Redmond CK, Chen VW, et al. Black/White Cancer Survival Study Group Breast cancer: factors associated with stage at diagnosis in Black and White women. J Natl Cancer Inst. 1993;85:1129–1137. doi: 10.1093/jnci/85.14.1129. [DOI] [PubMed] [Google Scholar]
- 20.Schwartz KL, Crossley-May H, Vigneau FD, Brown K, Banerjee M. Race, socioeconomic status and stage at diagnosis for five common malignancies. Cancer Causes Control. 2003;14(8):761–766. doi: 10.1023/a:1026321923883. [DOI] [PubMed] [Google Scholar]
- 21.Ghafoor A, Jemal A, Ward E, Cokkinides V, Smith R, Thun M. Trends in breast cancer by race and ethnicity. CA Cancer J Clin. 2003;53:342–355. doi: 10.3322/canjclin.53.6.342. [DOI] [PubMed] [Google Scholar]
- 22.Ward E, Jemal A, Cokkinides V, et al. Cancer disparities by race/ethnicity and socioeconomic status. CA Cancer J Clin. 2004;54:78–93. doi: 10.3322/canjclin.54.2.78. [DOI] [PubMed] [Google Scholar]
- 23.Jemal A, Murray T, Ward E, et al. Cancer statistics, 2005. CA Cancer J Clin. 2005;55:10–30. doi: 10.3322/canjclin.55.1.10. [DOI] [PubMed] [Google Scholar]
- 24.Shavers VL, Brown ML. Racial and ethnic disparities in the receipt of cancer treatment. J Natl Cancer Inst. 2002;94:334–357. doi: 10.1093/jnci/94.5.334. [DOI] [PubMed] [Google Scholar]
- 25.Mandelblatt JS, Kerner JF, Hadley J, et al. Variations in breast carcinoma treatment in older Medicare beneficiaries: is it Black or White? Cancer. 2002;95:1401–1414. doi: 10.1002/cncr.10825. [DOI] [PubMed] [Google Scholar]
- 26.Coates RJ, Bransfield DD, Wesley M, et al. Black/White Cancer Survival Study Group Differences between Black and White women with breast cancer in time from symptom recognition to medical consultation. J Natl Cancer Inst. 1992;84:938–950. doi: 10.1093/jnci/84.12.938. [DOI] [PubMed] [Google Scholar]
- 27.Caplan LS, Helzlsouer KJ, Shapiro S, Freedman LS, Coates RJ, Edwards BK. System delay in breast cancer in Whites and Blacks. Am J Epidemiol. 1995;142:804–812. doi: 10.1093/oxfordjournals.aje.a117719. [DOI] [PubMed] [Google Scholar]
- 28.Breen N, Wesley MN, Merrill RM, Johnson K. The relationship of socio-economic status and access to minimum expected therapy among female breast cancer patients in the National Cancer Institute Black-White Cancer Survival Study. Ethn Dis. 1999;9:111–125. [PubMed] [Google Scholar]
- 29.Joslyn SA. Racial differences in treatment and survival from early-stage breast carcinoma. Cancer. 2002;95:1759–1766. doi: 10.1002/cncr.10827. [DOI] [PubMed] [Google Scholar]
- 30.Eley JW, Hill HA, Chen VW, et al. Racial differences in survival from breast cancer. Results of the National Cancer Institute Black/White Cancer Survival Study. JAMA. 1994;272:947–954. doi: 10.1001/jama.272.12.947. [DOI] [PubMed] [Google Scholar]
- 31.Wojcik BE, Spinks MK, Optenberg SA. Breast carcinoma survival analysis for African American and White women in an equal-access healthcare system. Cancer. 1998;82:1310–1318. doi: 10.1002/(sici)1097-0142(19980401)82:7<1310::aid-cncr14>3.0.co;2-9. [DOI] [PubMed] [Google Scholar]
- 32.Jatoi I, Becher H, Leake CR. Widening disparity in survival between White and African American patients with breast carcinoma treated in the US Department of Defense Healthcare system. Cancer. 2003;98:894–899. doi: 10.1002/cncr.11604. [DOI] [PubMed] [Google Scholar]
- 33.Veronesi U, Saccozzi R, del Vecchio M, et al. Comparing radical mastectomy with quadrantectomy, axillary dissection, and radiotherapy in patients with small cancers of the breast. N Engl J Med. 1981;305:6–11. doi: 10.1056/NEJM198107023050102. [DOI] [PubMed] [Google Scholar]
- 34.Sarrazin D, Le M, Rouesse J, et al. Conservative treatment versus mastectomy in breast cancer tumors with macroscopic diameter of 20 millimeters or less. The experience of the Institut Gustave-Roussy. Cancer. 1984;53:1209–1213. doi: 10.1002/1097-0142(19840301)53:5<1209::aid-cncr2820530531>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 35.Fisher B, Bauer M, Margolese R, et al. Five-year results of a randomized clinical trial comparing total mastectomy and segmental mastectomy with or without radiation in the treatment of breast cancer. N Engl J Med. 1985;312:665–673. doi: 10.1056/NEJM198503143121101. [DOI] [PubMed] [Google Scholar]
- 36.Fisher B, Redmond C, Poisson R, et al. Eight-year results of a randomized clinical trial comparing total mastectomy and lumpectomy with or without irradiation in the treatment of breast cancer. N Engl J Med. 1989;320:822–828. doi: 10.1056/NEJM198903303201302. [DOI] [PubMed] [Google Scholar]
- 37.Veronesi U, Banfi A, Salvadori B, et al. Breast conservation is the treatment of choice in small breast cancer: long-term results of a randomized trial. Eur J Cancer. 1990;26:668–670. doi: 10.1016/0277-5379(90)90113-8. [DOI] [PubMed] [Google Scholar]
- 38.NIH Consensus Conference Treatment of early-stage breast cancer. JAMA. 1991;265:391–395. [PubMed] [Google Scholar]
- 39.Nattinger AB, Gottlieb MS, Hoffman RG, Walker AP, Goodwin JS. Minimal increase in use of breast-conserving surgery from 1986 to 1990. Med Care. 1996;34:479–489. doi: 10.1097/00005650-199605000-00009. [DOI] [PubMed] [Google Scholar]
- 40.Riley GF, Potosky AL, Klabunde CN, Warren JL, Ballard-Barbash R. Stage at diagnosis and treatment patterns among older women with breast cancer: an HMO and fee-for-service comparison. JAMA. 1999;281:720–726. doi: 10.1001/jama.281.8.720. [DOI] [PubMed] [Google Scholar]
- 41.Lazovich D, Caucasian E, Thomas DB, Moe RE, Taplin S. Change in the use of breast-conserving surgery in western Washington after the 1990 NIH Consensus Development Conference. Arch Surg. 1997;132:418–423. doi: 10.1001/archsurg.1997.01430280092014. [DOI] [PubMed] [Google Scholar]
- 42.Du XL, Freeman DH, Syblik DA. What drove changes in the use of breast conserving surgery for breast cancer since the early 1980s? The role of the clinical trial, celebrity action and an NIH consensus statement. Breast Cancer Res Treat. 2000;62:71–79. doi: 10.1023/a:1006414122201. [DOI] [PubMed] [Google Scholar]
- 43.National Cancer Institute [Accessed on: 5/5/05];SEER 1973-2002 Public-Use Data. Available at: http://seer.cancer.gov/publicdata/
- 44.National Cancer Institute . The SEER Program Code Manual. Rev ed. National Cancer Institute; Bethesda, Md: 1994. NIH Publication No. 94-1999. [Google Scholar]
- 45.Stokes ME, Davis CS, Koch GG. Categorical Data Analysis Using the SAS System. SAS Institute Inc; Cary, NC: 1997. [Google Scholar]
- 46.Bach PB, Pham HH, Schrag D, Tate RC, Hargraves JL. Primary care physicians who treat Blacks and Whites. N Engl J Med. 2004;351:575–584. doi: 10.1056/NEJMsa040609. [DOI] [PubMed] [Google Scholar]
- 47.Du XL, Freeman JL, Freeman DH, Syblik DA, Goodwin JS. Temporal and regional variation in the use of breast conserving surgery and radiotherapy for older women with early stage breast cancer from 1983 to 1995. J Gerontol A Bio Sci Med Sci. 1999;54:474–478. doi: 10.1093/gerona/54.9.m474. [DOI] [PubMed] [Google Scholar]
- 48.Du XL. Increase in the use of breast-conserving surgery. JAMA. 1999;282:326–327. doi: 10.1001/jama.282.4.326. [DOI] [PubMed] [Google Scholar]
- 49.Vinh-Hung V, Verschraegen C. Breast-conserving surgery with or without radiotherapy: pooled-analysis for risks of ipsilateral breast tumor recurrence and mortality. J Natl Cancer Inst. 2004;96:115–121. doi: 10.1093/jnci/djh013. [DOI] [PubMed] [Google Scholar]
- 50.Du XL, Freeman JL, Goodwin JS. Information on radiation treatment in patients with breast cancer: the advantages of the linked Medicare and SEER data. J Clin Epidemiol. 1999;52:463–470. doi: 10.1016/s0895-4356(99)00011-6. [DOI] [PubMed] [Google Scholar]
- 51.Virnig BA, Warren JL, Cooper GS, Klabunde CN, Schussler N, Freeman J. Studying radiation therapy using SEER-Medicare-linked data. Med Care. 2002;40(8suppl):49–54. doi: 10.1097/00005650-200208001-00007. [DOI] [PubMed] [Google Scholar]