

Abstract
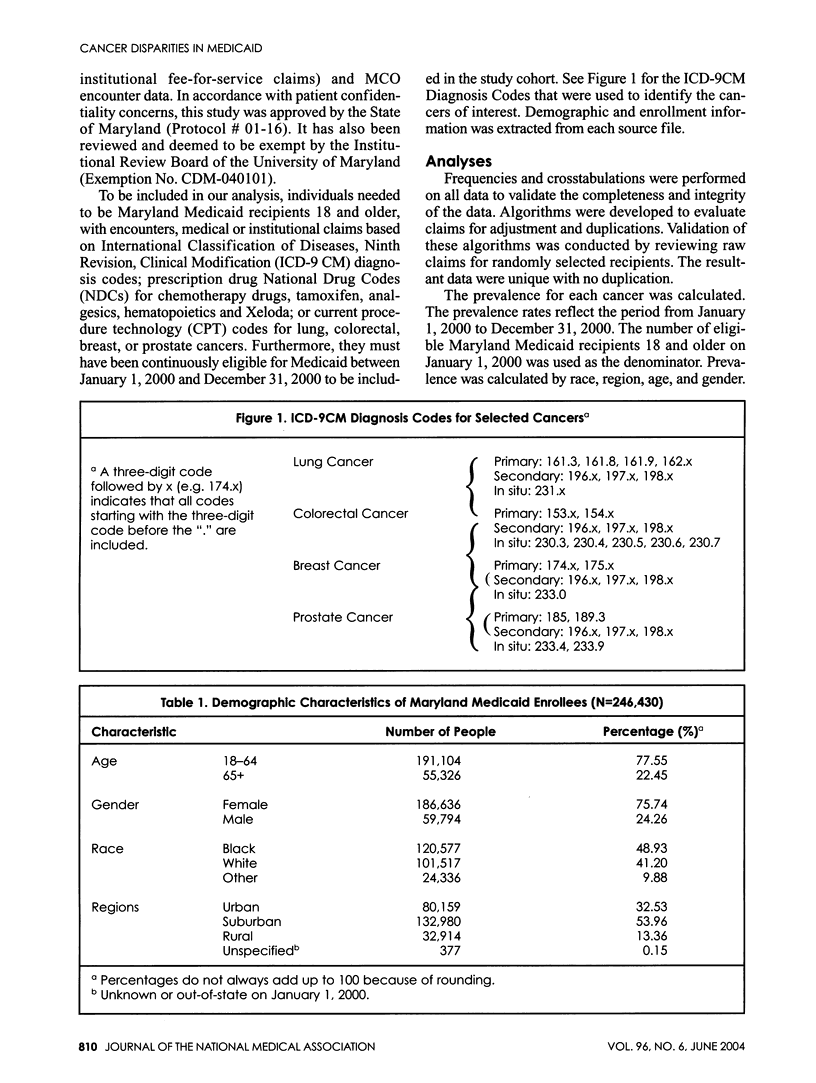
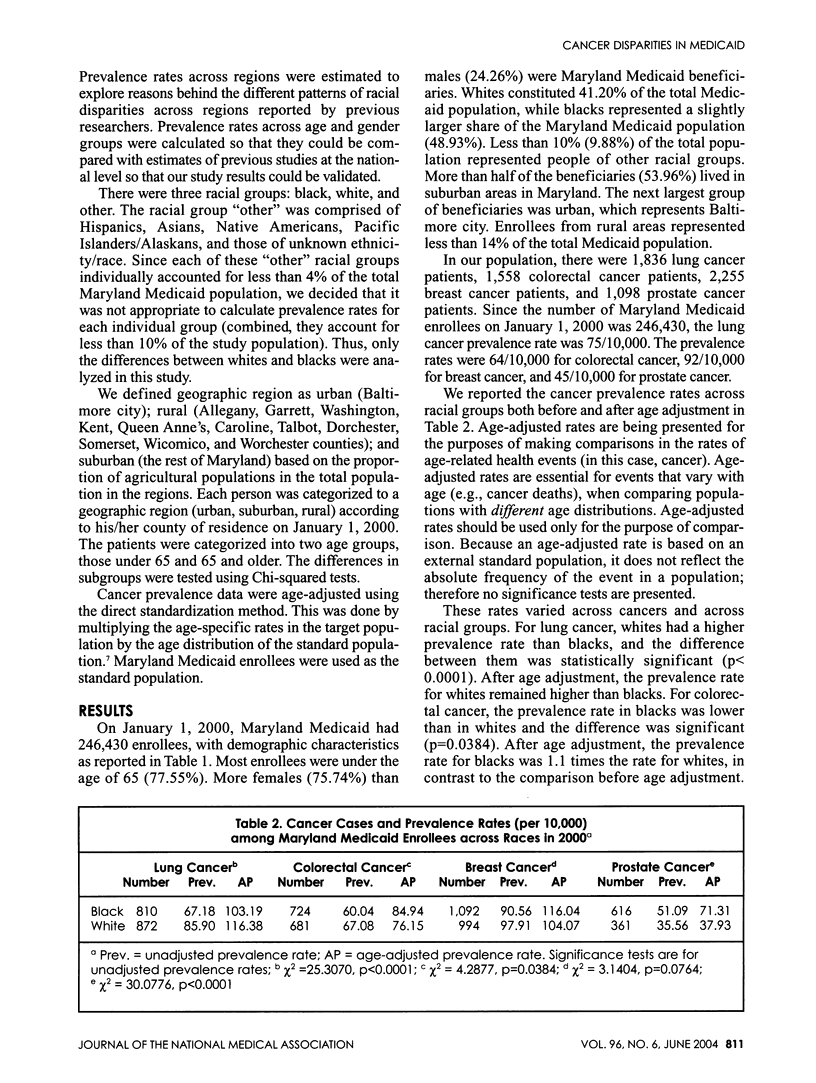
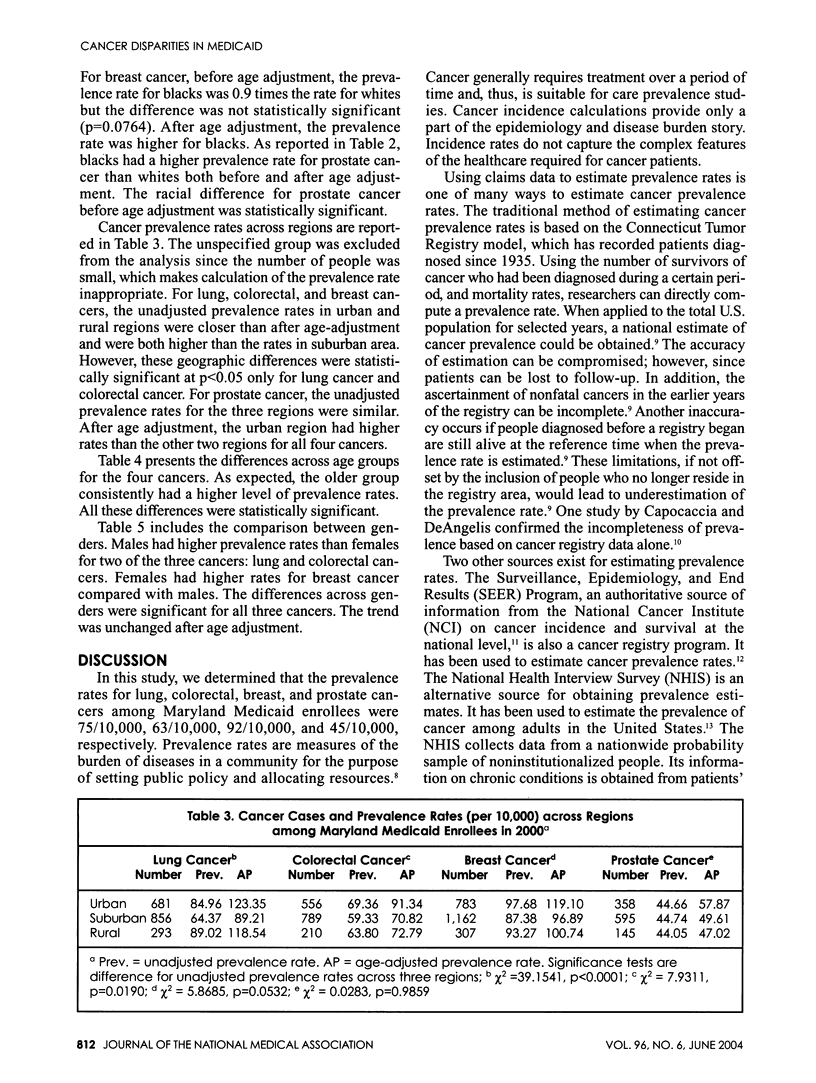
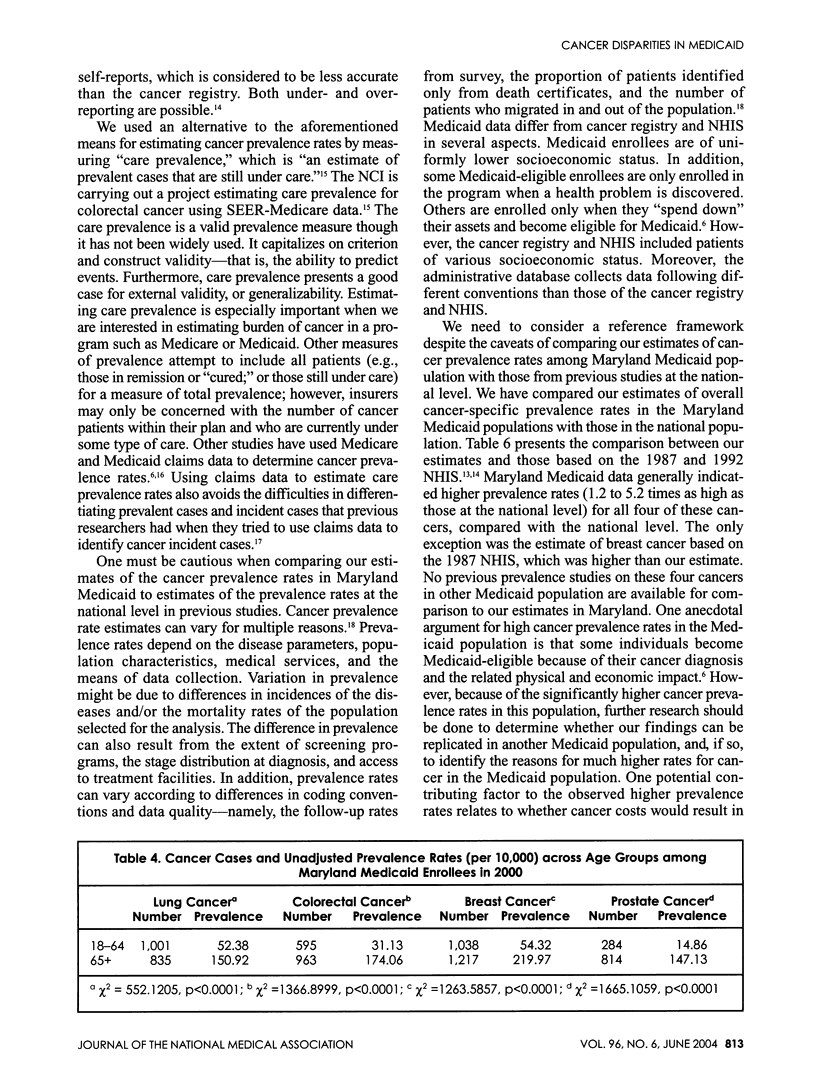
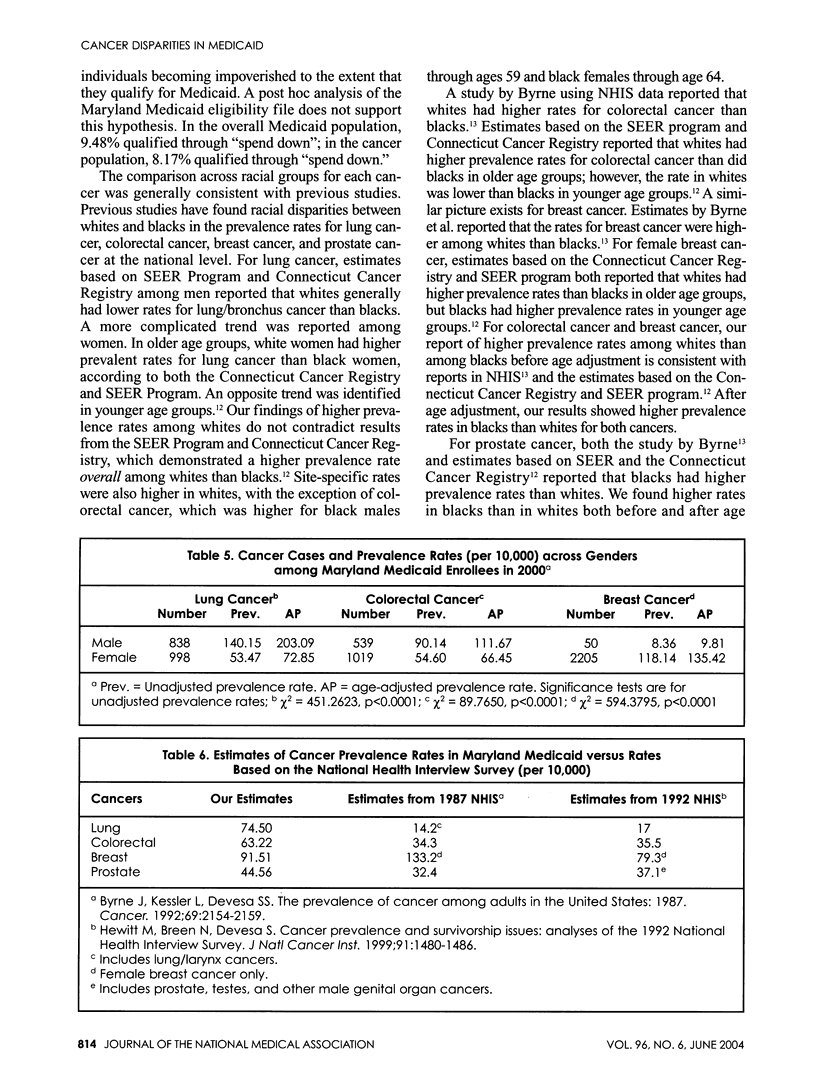
BACKGROUND: Given previous reports of variations in prevalence of cancer in low-income individuals, we sought to determine if disparities in cancer prevalence existed in a similarly-insured Medicaid population. METHODS: Using Maryland Medicaid administrative claims data, prevalence rates of lung, colorectal, breast, and prostate cancers were calculated for Maryland Medicaid recipients who were continuously eligible during the period from January 1, 2000 to December 31, 2000. Chi-squared tests were used to test the differences across subgroups. Cancer prevalence data were age-adjusted using Maryland Medicaid enrollees as the standard population. RESULTS: The care prevalence rates for lung, colorectal, breast, and prostate cancers were 75/10,000, 63/10,000, 92/10,000, and 45/10,000, respectively. These rates were 1.2 to 5.2 times those reported at the national level. Generally, higher cancer prevalence rates in certain racial groups in Maryland Medicaid were consistent with previous studies. Regional differences in cancer prevalence existed for each cancer studied. CONCLUSIONS: Limiting our study sample to a population of uniformly low socioeconomic individuals did not eliminate the disparity in prevalence rates between blacks and whites. Different patterns of racial disparity across regions reported by previous researchers might be due to small area variation in addition to socioeconomic status.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bradley C. J., Given C. W., Roberts C. Disparities in cancer diagnosis and survival. Cancer. 2001 Jan 1;91(1):178–188. doi: 10.1002/1097-0142(20010101)91:1<178::aid-cncr23>3.0.co;2-s. [DOI] [PubMed] [Google Scholar]
- Bradley Cathy J., Given Charles W., Roberts Caralee. Race, socioeconomic status, and breast cancer treatment and survival. J Natl Cancer Inst. 2002 Apr 3;94(7):490–496. doi: 10.1093/jnci/94.7.490. [DOI] [PubMed] [Google Scholar]
- Byrne J., Kessler L. G., Devesa S. S. The prevalence of cancer among adults in the United States: 1987. Cancer. 1992 Apr 15;69(8):2154–2159. doi: 10.1002/1097-0142(19920415)69:8<2154::aid-cncr2820690823>3.0.co;2-r. [DOI] [PubMed] [Google Scholar]
- Capocaccia R., De Angelis R. Estimating the completeness of prevalence based on cancer registry data. Stat Med. 1997 Feb 28;16(4):425–440. doi: 10.1002/(sici)1097-0258(19970228)16:4<425::aid-sim414>3.0.co;2-z. [DOI] [PubMed] [Google Scholar]
- Fowles J. B., Lawthers A. G., Weiner J. P., Garnick D. W., Petrie D. S., Palmer R. H. Agreement between physicians' office records and Medicare Part B claims data. Health Care Financ Rev. 1995 Summer;16(4):189–199. [PMC free article] [PubMed] [Google Scholar]
- Giles G. How important are estimates of cancer prevalence? Ann Oncol. 2002 Jun;13(6):815–816. doi: 10.1093/annonc/mdf204. [DOI] [PubMed] [Google Scholar]
- Hewitt M., Breen N., Devesa S. Cancer prevalence and survivorship issues: analyses of the 1992 National Health Interview Survey. J Natl Cancer Inst. 1999 Sep 1;91(17):1480–1486. doi: 10.1093/jnci/91.17.1480. [DOI] [PubMed] [Google Scholar]
- Howe H. L., Wingo P. A., Thun M. J., Ries L. A., Rosenberg H. M., Feigal E. G., Edwards B. K. Annual report to the nation on the status of cancer (1973 through 1998), featuring cancers with recent increasing trends. J Natl Cancer Inst. 2001 Jun 6;93(11):824–842. doi: 10.1093/jnci/93.11.824. [DOI] [PubMed] [Google Scholar]
- Jollis J. G., Ancukiewicz M., DeLong E. R., Pryor D. B., Muhlbaier L. H., Mark D. B. Discordance of databases designed for claims payment versus clinical information systems. Implications for outcomes research. Ann Intern Med. 1993 Oct 15;119(8):844–850. doi: 10.7326/0003-4819-119-8-199310150-00011. [DOI] [PubMed] [Google Scholar]
- Joseph A. K., Mark T. L., Mueller C. The period prevalence and costs of treating nonmelanoma skin cancers in patients over 65 years of age covered by medicare. Dermatol Surg. 2001 Nov;27(11):955–959. doi: 10.1046/j.1524-4725.2001.01106.x. [DOI] [PubMed] [Google Scholar]
- McClish D. K., Penberthy L., Whittemore M., Newschaffer C., Woolard D., Desch C. E., Retchin S. Ability of Medicare claims data and cancer registries to identify cancer cases and treatment. Am J Epidemiol. 1997 Feb 1;145(3):227–233. doi: 10.1093/oxfordjournals.aje.a009095. [DOI] [PubMed] [Google Scholar]
- Merrill R. M., Capocaccia R., Feuer E. J., Mariotto A. Cancer prevalence estimates based on tumour registry data in the Surveillance, Epidemiology, and End Results (SEER) Program. Int J Epidemiol. 2000 Apr;29(2):197–207. doi: 10.1093/ije/29.2.197. [DOI] [PubMed] [Google Scholar]
- Polednak A. P. Estimating the prevalence of cancer in the United States. Cancer. 1997 Jul 1;80(1):136–141. [PubMed] [Google Scholar]
- Roetzheim R. G., Pal N., Tennant C., Voti L., Ayanian J. Z., Schwabe A., Krischer J. P. Effects of health insurance and race on early detection of cancer. J Natl Cancer Inst. 1999 Aug 18;91(16):1409–1415. doi: 10.1093/jnci/91.16.1409. [DOI] [PubMed] [Google Scholar]
- Sung J. F., Blumenthal D. S., Alema-Mensah E., McGrady G. A. Racial and urban/rural differences in cervical carcinoma in Georgia Medicaid recipients. Cancer. 1997 Jul 15;80(2):231–236. [PubMed] [Google Scholar]
- Wennberg John E. Unwarranted variations in healthcare delivery: implications for academic medical centres. BMJ. 2002 Oct 26;325(7370):961–964. doi: 10.1136/bmj.325.7370.961. [DOI] [PMC free article] [PubMed] [Google Scholar]