

Abstract
Objective
To describe a series of five patients with isolated fracture of the manubrium of the malleus.
Design
Retrospective case series.
Subjects
Five patients aged 44−64 years with isolated fracture of the manubrium who presented to our institution over a five-year period (2000−2005).
Results
All patients presented with a history of digitally manipulating the external auditory canal, leading to the manubrial fracture, which we presume was due to a suction-type mechanism. Otomicroscopy often revealed a break in the smooth contour of the manubrium. All patients had air–bone gaps on audiometry, especially at higher frequencies. Tympanometry showed hypermobility of the tympanic membrane in four patients who were tested. Laser-Doppler vibrometry revealed increased umbo velocity in four out of five patients. Four patients were treated conservatively. One patient underwent exploratory tympanotomy with successful ossiculoplasty.
Conclusions
Isolated fracture of the manubrium is a rare condition which may present as sudden-onset hearing loss after digital manipulation of the external auditory canal. The diagnosis can be made on the basis of otomicroscopy, audiometry, tympanometry and laser-Doppler vibrometry. Conservative treatment is often successful.
Keywords: Malleus, Fracture, Conductive Deafness
Introduction
Isolated fracture of the manubrium of the malleus is rare; only about 11 cases have been reported in the English language literature over the past 50 years.1-5 We describe our experience with five patients with isolated fracture of the manubrium.
Materials and methods
We encountered five patients in our clinical practice, over a five-year period (2000−2005), who were diagnosed with an isolated fracture of the manubrium. We noted patients’ symptoms and signs at the time of presentation, together with their audiological results and outcomes. All five patients also underwent measurements of umbo velocity using laser-Doppler vibrometry. The technique of laser-Doppler vibrometry has been described in detail previously.6-8
This study was approved by our institutional review board.
Results
Case one
A 44-year-old man complained of sudden-onset hearing loss and tinnitus in his right ear while digitally manipulating the right external auditory canal after a shower. As he removed his finger from the ear canal, he heard a sudden pop and experienced otalgia as well as aural fullness. He could improve his hearing transiently by either pressing on the tragus or by performing a Valsalva manoeuvre.
On otomicroscopy, the right tympanic membrane showed an abnormal outline of the manubrium. Pneumatic otoscopy revealed excessive movement of the umbo compared with the lateral process. The left ear was normal. With a 512 Hz tuning fork, the Rinne test was positive bilaterally, while the Weber test lateralised to the right.
An audiogram showed an air–bone gap at mid- to high frequencies (Figure 1a). Tympanometry revealed increased mobility on the right. Laser-Doppler vibrometry showed an increase in umbo velocity at mid-frequencies (1−2 kHz) on the right (Figure 2a).
Fig. 1.
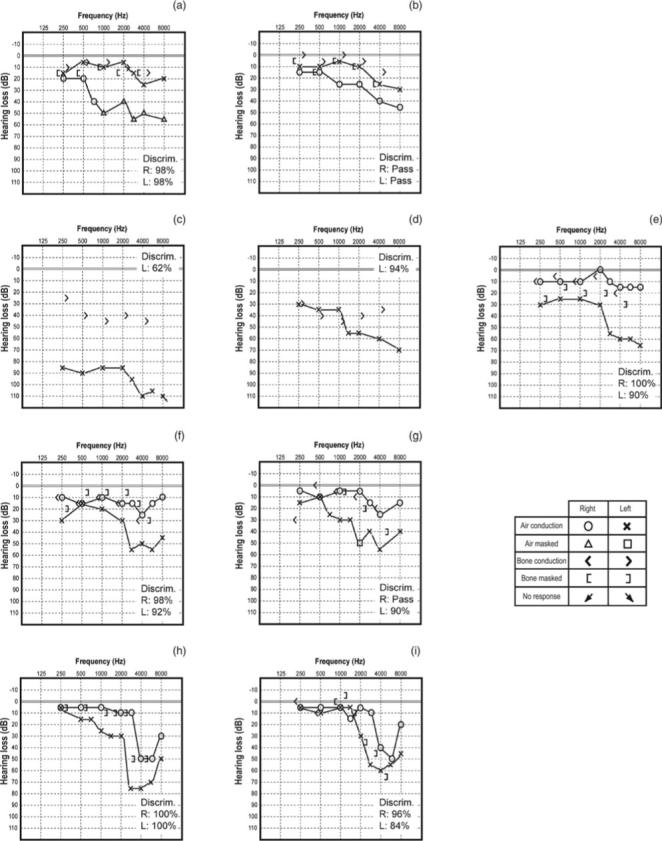
Audiograms of cases 1 to 5. Speech discrimination scores (Discrim) are shown in each audiogram; ‘Pass’ indicates >92 per cent. (a) Case 1, pre-operative; (b) case 1, post-operative; (c) case 2, initial audiogram; (d) case 2, follow-up audiogram; (e) case 3; (f) case 4, initial audiogram; (g) case 4, follow-up audiogram; (h) case 5, initial audiogram; (i) case 5, follow-up audiogram.
Fig. 2.
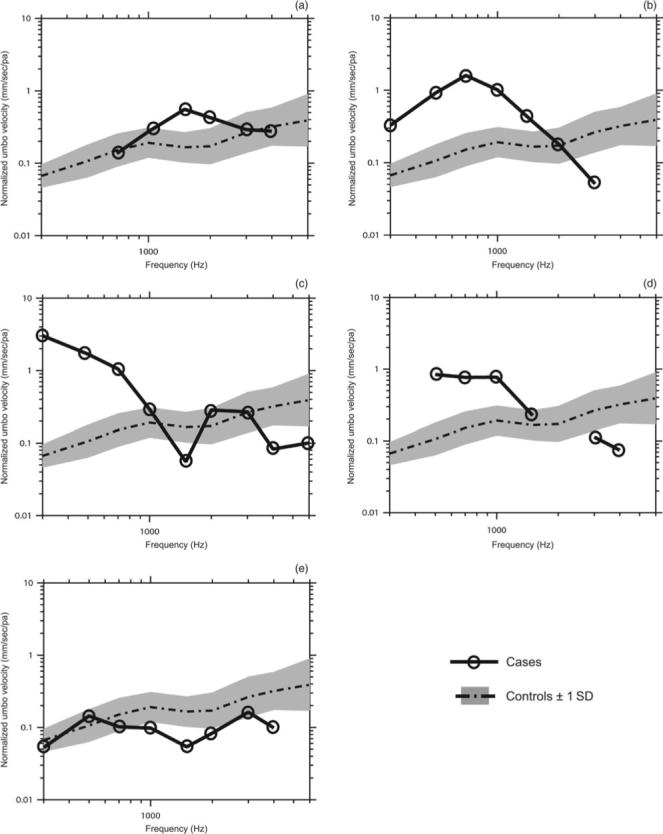
Umbo velocity measured by laser-Doppler vibrometry in cases (a) 1, (b) 2, (c) 3, (d) 4 and (e) 5. The control plotline indicates the mean umbo velocity for 56 normal subjects;8 the shaded areas represent ±1 standard deviation (SD) from the mean. The solid black line with circles represents the umbo velocity measured in each of the 5 cases in the present study. Data are reported only at those frequencies for which the signal-to-noise ratio was >10 dB (shown in circles). In both normal subjects and the 5 cases, the measured umbo velocity was divided by the measured sound pressure in the ear canal, reported as the normalised umbo velocity. Note that the umbo velocity was greater than normal in cases 1 to 4, all of whom had air–bone gaps at the time of the laser measurement. The umbo velocity measurement in case 5 was made 4 months after the injury, by which time his air–bone gap had resolved; therefore, the measured umbo velocity was in the normal range in this case.
Over the next eight months, the patient continued to have fluctuating conductive hearing loss on the right, with distortion of sound and a sensation of aural fullness. He elected to undergo surgical repair.
A transcanal exploratory tympanotomy was performed, and a fracture of the manubrium just below the lateral process was noted. The remainder of the ossicular chain was normal. The incus was removed, and a 2.5 mm, titanium, partial ossicular replacement prosthesis (Heinz Kurz, Dusslingen, Germany) was placed between the stapes head and the tympanic membrane.
Post-operatively, the patient reported resolution of his complaints of fluctuation of hearing, distortion of sound and aural fullness.
An audiogram performed three months post-operatively showed improvement in the right-sided air–bone gap (Figure 1b).
Case two
A 64-year-old woman with a history of right-sided, profound, sensorineural hearing loss since early childhood presented three days after sudden onset of hearing loss in the left ear due to digital manipulation of the external auditory canal. She had placed her finger in the ear canal and, upon retracting it, had experienced sudden otalgia and a significant reduction in hearing.
On otomicroscopic examination, the left tympanic membrane was intact but had a small amount of haemorrhage around the manubrium. The Rinne test was positive on the left, and the Weber test lateralised to the left.
An audiogram showed a severe, mixed hearing loss on the left, with a 50−60 dB air–bone gap (Figure 1c). Tympanometry showed increased mobility on the left, and the ipsilateral acoustic reflex on the left was absent in response to a broad-band stimulus. Laser-Doppler vibrometry showed a marked increase in umbo velocity at low frequencies in the left ear (Figure 2b), which is consistent with partial or complete ossicular discontinuity.7
The patient returned for follow up three weeks later, and reported some improvement in her hearing. On otomicroscopic examination, the tympanic membrane showed an irregularity in the contour of the manubrium, with an unusual wrinkle on the tympanic membrane. A follow-up audiogram showed a significant improvement in hearing (Figure 1d), with the puretone average improving from 85 to 45 dB and the air–bone gap reducing to 15−25 dB. The patient was referred for amplification.
Case three
A 63-year-old woman complained of sudden-onset hearing loss in her left ear, five months prior to presentation. She had been rubbing her left ear when she suddenly had developed acute otalgia, aural fullness and hearing loss. She had been diagnosed with sudden sensorineural hearing loss by her primary care physician and had been commenced on a course of oral prednisone, which she did not complete due to side effects.
On otomicroscopy, the left tympanic membrane was intact, but the contour of the manubrium was noted to be irregular, suggestive of a fracture. The Rinne test was positive bilaterally, and the Weber test was midline.
An audiogram showed a mild, mixed hearing loss on the left, with a high-frequency air–bone gap (Figure 1e). Tympanometry was not performed. Laser-Doppler vibrometry showed a marked increase in umbo velocity at low frequencies in the left ear (Figure 2c).
The patient was managed by watchful waiting.
Case four
A 58-year-old woman presented with aural fullness in the left ear after inserting her finger into her left external auditory canal while showering two months previously. Upon retracting the finger, she had noticed a popping sensation and an immediate sense of fullness with mild otalgia on the left.
On otomicroscopy, the left tympanic membrane was intact, but the contour of the manubrium was noted to be irregular, suggestive of a fracture. The Rinne test was positive bilaterally, and the Weber test lateralised to the left.
An audiogram showed a mild high-frequency air–bone gap (15−25 dB) on the left (Figure 1f). Tympanometry showed increased mobility on the left. Laser-Doppler vibrometry showed a marked increase in umbo velocity at low frequencies in the left ear (Figure 2d).
The patient returned for a follow-up visit four months later. Otoscopic examination was normal. A follow-up audiogram four months after the injury showed a similar high-frequency air–bone gap on the left (Figure 1 g). The management options of amplification vs surgical repair were discussed; at the time of writing, the patient was considering her options.
Case five
A 64-year-old man complained of sudden-onset hearing loss during digital manipulation of his left external auditory canal. He had experienced a momentary, sharp pain followed by an immediate hearing loss. He had initially been evaluated by a local otolaryngologist. The status of the manubrium had not been documented. An audiogram performed at the time had shown a high-frequency, mixed hearing loss with a high-frequency air–bone gap (Figure 1 h). He had been treated with a course of oral prednisone, with no improvement in his hearing. Tympanometry had shown increased mobility on the left.
The patient was referred to us four months after the onset of his hearing loss. He reported that his hearing had improved over the past two months, but that the left ear was still somewhat worse than the right.
On otomicroscopic examination, the external auditory canal and the tympanic membrane were normal bilaterally. The Rinne test was positive bilaterally, and the Weber test was midline.
An audiogram showed closure of the high-frequency air–bone gap (Figure 1i). Tympanometry again showed increased mobility on the left. Laser-Doppler vibrometry showed normal to low-normal umbo velocity on the left (Figure 2e).
Conservative management was advised.
Discussion
The malleus is involved in only 2 per cent of traumatic lesions involving the middle ear.2 Isolated fractures of the manubrium are even less common, and only 11 cases have been reported in the English language literature over the past 50 years (Table I).1-5
TABLE I.
REPORTS OF MANUBRIAL FRACTURE PUBLISHED IN ENGLISH LITERATURE OVER LAST 50 YEARS
| Study | Cases (n) | Mechanism of injury | Air—bone gap (dB) | Otoscopy | Management |
|---|---|---|---|---|---|
| Harris & Butler1 | 4 | Head trauma | 5−30 | Manubrial fracture on neumatic otoscopy (cases 1−3) | Conservative (cases 1−3) |
| Ear striking water | 5−15 | Surgical (case 4) | |||
| Unknown | 0−20 | ||||
| Scuba diving | 0−40 | ||||
| Pedersen2 | 2 | Digital manipulation of ear canal (both cases) | 5−30 | Normal | Surgical (both cases) |
| 10−15 | Free motion of manubrium with immobile lateral process | ||||
| Iurato & Quaranta3 | 3 | Jet of water striking ear | 5−25 | Fracture of manubrium (all cases) | Conservative (all cases) |
| Unknown | 5−15 | ||||
| Digital manipulation of ear canal | 10−20 | ||||
| Applebaum & Goldin4 | 1 | Unknown | 15−25 | Poorly mobile malleus | Surgical |
| Orabi5 | 1 | Digital manipulation of ear canal | 20−25 | Normal | Conservative |
The number of individual cases reported in each of these previous papers ranged from one to four. Iurato and Quaranta3 performed an exhaustive review of the literature from 1855 to 1999 and found a total of about 43 cases. Thus, the present study of five cases comprises a large case series.
The diagnosis of manubrium fracture was confirmed at surgery in one of our cases (case one). In cases two, three and four, we had the opportunity to carefully examine the tympanic membrane at the time of injury and were able to document a break in the contour of the manubrium, under the high magnification afforded by otomicroscopy. In addition, case two showed haemorrhage around the manubrium. These findings enabled us to make a diagnosis of manubrium fracture. It is of interest that cases one to four all had very similar clinical presentations and test findings, including: (1) the peculiar nature of the triggering injury (digital manipulation of the external auditory canal, and withdrawal of the finger causing a sudden decrease in hearing with otalgia); (2) an irregularity in the contour of the manubrium on otoscopy; (3) an air–bone gap that was larger at higher frequencies; (4) increased mobility of the tympanic membrane on tympanometry; and (5) hypermobility of the umbo on laser-Doppler vibrometry. The latter three findings are indicative of ossicular discontinuity, which in association with the peculiar history and otoscopic findings allowed us to make a diagnosis of fracture of the manubrium. Case five differed from the others in that we did not have the opportunity to examine the patient at the time of injury. However, we believe that he too had a manubrial fracture, because his clinical presentation was very similar to cases one to four, including the inciting event, the air–bone gap at high frequencies, and the increased tympanic membrane mobility on tympanometry.
The aetiological event triggering the manubrial fracture in all five cases was digital manipulation of the external auditory canal. This mechanism of injury has also been reported by others.2,3,5 It is hypothesised that when the finger is rapidly withdrawn from the ear canal, a negative pressure is created that draws the tympanic membrane and the manubrium laterally. Since the malleus head is relatively fixed in the epitympanum, the sudden, lateral movement of the manubrium is believed to result in its fracture just below the level of the lateral process. Other events that involve creation of negative pressure in the ear canal, such as tympanometry and ascent in an elevator or in an airplane, are not generally associated with this type of injury. It may be that the rate of change of pressure in the ear canal in these latter situations is relatively slow, and insufficient to cause a sudden, lateral displacement of the manubrium, unlike the case of digital manipulation of the ear canal.
The diagnosis of a fracture of the manubrium may be overlooked because of its rarity, and a high index of suspicion is necessary in order to make an accurate diagnosis. A history of sudden-onset hearing loss while digitally manipulating the external auditory canal should arouse suspicion. Patients may also complain of aural fullness, otalgia, distortion of sound and tinnitus. The hearing loss may fluctuate, especially with autoinflation. There is usually no vertigo. Otoscopy and otomicroscopy reveal an intact tympanic membrane, but there is often a break or irregularity in the smooth contour of the manubrium, which is exaggerated with pneumatic insufflation. Pneumatic insufflation may also demonstrate hypermobility of the manubrium relative to the lateral process.
Isolated fracture of the manubrium of the malleus is rare
This paper describes the authors’ experience with five patients with isolated fracture of the manubrium
All patients presented with a history of digitally manipulating the external auditory canal, leading to the manubrial fracture
All patients had air–bone gaps on audiometry, especially at higher frequencies; tympanometry showed hypermobility of the tympanic membrane
Four patients were treated conservatively. One patient underwent exploratory tympanotomy with successful ossiculoplasty
Tuning fork and audiometric testing usually reveal an air–bone gap in these patients. It is noteworthy that the air–bone gap is usually larger in the higher frequencies compared with the lower ones; this differs from the audiometric findings for most lesions of the middle ear, such as ossicular fixation or middle-ear fluid. It is likely that there is still sufficient contact between the fractured ends of the manubrium to permit sound transmission at low frequencies, with progressively greater dissipation (shunting) of sound energy away from the ossicular chain at the fracture site at higher frequencies. Tympanometry often shows hypermobility of the tympanic membrane, which was seen in all four cases in our series in which tympanometry was performed.
Another finding that is helpful in the diagnosis is an increased umbo velocity when measured using laser-Doppler vibrometry. An increase in umbo velocity is indicative of partial or complete ossicular discontinuity.7 Increased umbo velocity was observed in all four cases in our series which were tested when there was an air–bone gap on audiometry. Case five (with normal umbo velocity) had the measurement performed four months after the initial event, by which time his audiogram showed resolution of the air–bone gap. While laser-Doppler vibrometry is helpful in the diagnosis, it is not essential, and an accurate diagnosis can still be made based on the other clinical and audiometric features.
Our clinical observations suggest that the ear has a capacity for spontaneous improvement or resolution of the hearing loss and other symptoms, as was observed in cases two and five. It is doubtful that there is true bony union of the fractured manubrium, since the ossicles show very little capacity for bony healing and remodelling.9 It is more likely that fibrosis between the fractured ends results in restoration of sound transmission, at least to some degree.
We recommend that patients with isolated fracture of the manubrium should undergo a period of watchful waiting. Surgical exploration is warranted if a significant air–bone gap persists, or if other symptoms such as aural fullness and fluctuation of the hearing level are particularly troublesome. The typical finding at surgery is a fracture of the manubrium just inferior to the lateral process. Various techniques have been described for surgical repair, including the use of a bone chip between the fractured ends1 and a sculpted bone graft placed as an interposition between the manubrium and the incus.4 In our patient who underwent surgical repair (case one), we chose to bypass the malleus head in the epitympanum and to repair the ossicular chain using a prosthesis placed between the stapes and the tympanic membrane. This patient had a good outcome, as evidenced by improvement of his hearing and resolution of aural fullness and other symptoms.
Conclusions
We report our experience with five patients with isolated fracture of the manubrium. All of our patients presented with a sudden-onset hearing loss after digitally manipulating the external auditory canal. The tympanic membrane often revealed an abnormal contour of the manubrium. Audiometry showed a high-frequency air–bone gap, and tympanometry showed hypermobility of the tympanic membrane. Laser-Doppler vibrometry showed a marked increase in umbo velocity. Watchful waiting is recommended initially. If the hearing loss persists, then amplification or surgical repair can be considered.
Acknowledgements
We thank Mike Ravicz, Melissa Wood and Jocelyn Songer for assistance with laser vibrometry measurements, and Richard Cortese for computer graphics assistance. The authors were supported in part by the National Institutes of Health grant number DC04798 (to SNM), the Silverstein Young Investigator Award (to WC), and Mr Lakshmi Mittal.
Footnotes
Dr W Chien takes responsibility for the integrity of the content of the paper.
Competing interests: None declared
References
- 1.Harris JP, Butler D. Recognition of malleus handle fracture in the differential diagnosis of otologic trauma. Laryngoscope. 1985;95:665–70. doi: 10.1288/00005537-198506000-00006. [DOI] [PubMed] [Google Scholar]
- 2.Pedersen CB. Traumatic middle ear lesions. Fracture of the malleus handle, aetiology, diagnosis and treatment. J Laryngol Otol. 1989;103:901–3. doi: 10.1017/s0022215100110461. [DOI] [PubMed] [Google Scholar]
- 3.Iurato S, Quaranta A. Malleus-handle fracture: historical review and three new cases. Am J Otol. 1999;20:19–25. [PubMed] [Google Scholar]
- 4.Applebaum EL, Goldin AD. Surgical management of isolated malleus handle fractures. Laryngoscope. 2000;110:171–3. doi: 10.1097/00005537-200001000-00031. [DOI] [PubMed] [Google Scholar]
- 5.Orabi AA. Isolated malleus neck fracture. Acta Otolaryngol. 2006;126:321–3. doi: 10.1080/00016480410022895. [DOI] [PubMed] [Google Scholar]
- 6.Merchant SN, Whittemore KR, Poon B, Lee C-Y, Rosowski JJ. Clinical measurements of tympanic membrane velocity using laser Doppler vibrometry: preliminary results, methodological issues and potential applications. In: Rosowski JJ, Merchant SN, editors. The Function and Mechanics of Normal, Diseased and Reconstructed Ears. Kugler; The Hague: 2000. pp. 367–82. [Google Scholar]
- 7.Rosowski JJ, Mehta RP, Merchant SN. Diagnostic utility of laser-Doppler vibrometry in conductive hearing loss with normal tympanic membrane. Otol Neurotol. 2003;24:165–75. doi: 10.1097/00129492-200303000-00008. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Whittemore KR, Jr, Merchant SN, Poon BB, Rosowski JJ. A normative study of tympanic membrane motion in humans using a laser Doppler vibrometer (LDV). Hear Res. 2004;187:85–104. doi: 10.1016/s0378-5955(03)00332-0. [DOI] [PubMed] [Google Scholar]
- 9.Schuknecht HF. Pathology of the Ear. 2nd edn. Pennsylvania: Lea & Febiger; Media: 1993. [Google Scholar]