

Abstract
To examine effects of group (Attention-Deficit/Hyperactivity Disorder [ADHD] versus Typically Developing [TD]), sex, and ADHD subtype on “process/optional” measures of executive functioning, children (n = 123; 54 ADHD, 69 TD) aged 8−16 completed subtests from the D-KEFS. No group, sex, or ADHD subtype effects were found on optional measures from the Trail Making, Color–Word Interference, and Tower tests. A significant interaction was found for Verbal Fluency Total Repetition Errors; boys with Combined/Hyperactive-Impulsive (ADHD-C/HI) type ADHD performed better than ADHD-C/HI girls, whereas girls with Inattentive type ADHD (ADHD-I) performed better than ADHDI boys. Overall, children with ADHD did not differ from TD on most optional measures from the D-KEFS. When sex and ADHD subtype were considered, children with the subtype of ADHD less common for sex were at greater risk for poorer performance.
Keywords: Process approach, ADHD, Executive function, D-KEFS
INTRODUCTION
The process approach in neuropsychology
The “process approach” to neuropsychological assessment purports to offer additional information to the examiner when considering brain–behavior relationships. The focus on process, the parsing of factors on multifactorial standardized tests, the systematic testing of limits, and the development of experimental procedures permit a better understanding of the role of individual variables, task variables, and stimulus parameters in brain–behavior relations. Specifically, the process approach can be defined as taking into account both personal and strategic factors related to task completion, and providing insight into the methodological process (adaptive or maladaptive) by which individuals approach a novel task (Kaplan, 1990).
Examinee process (or task approach) has been examined through “testing of limits” (e.g., providing multiple-choice test format after a subtest had been completed). For example, Kaplan (1990) reported that by providing additional blocks for the Block Design subtest of the Wechsler Adult Intelligence Scale – Revised (WAIS-R; Wechsler, 1974), she was able to demonstrate that individuals with documented vascular lesions or cerebral disconnection approached the task differently (e.g., attempted to use additional blocks); thus providing information beyond that typically quantified (through scaled score) in standardized administration. The incremental validity of the process approach has also been demonstrated in other adult-based studies (Akshoomoff, Delis, & Kiefner, 1989), which argued that relying only on summary scaled scores, without the examination of additional process variables, potentially limits the clinical utility and validity of the measurement of brain–behavior functioning.
The recent attempts to standardize limit-testing (e.g., Wechsler Adult Intelligence Scale – Revised – as a Neuropsychological Instrument [WAIS-R-NI], Kaplan, Fein, Morris, & Delis, 1991; Wechsler Intelligence Scale for Children – Third Edition – Process Instrument [WISC-III-PI], Kaplan, Fein, Kramer, Delis, & Morris, 1999; Wechsler Intelligence Scale for Children – Fourth Edition, Integrated [WISC-IV Integrated], Kaplan, Fein, Kramer, Delis, & Morris, 2004; Delis-Kaplan Executive Function System [D-KEFS], Delis, Kaplan, & Kramer, 2001; NEPSY, Korkman, Kirk, & Kemp, 1998) have the potential to better elucidate brain–behavior relations; however, little research on the validity of these methods has been published.
Validity of process approach in children
As with many neuropsychological methods, the process approach was initially designed for use with adults, but has been applied to children through a downward extension of adult-based practice. Therefore, there is less support for its use with children. Attempts have been made, however, to quantify the process by which children approach novel problem-solving and learning tasks by providing additional process-related scores on tests (e.g., standardized measures of learning strategy on the CVLT-C, Delis, Kramer, Kaplan, & Ober, 1994), which take into account developmental patterns and expected neuroanatomical changes during development. In this regard, the process by which a child approaches a task appears to overlap with certain elements of executive function (i.e., response preparation, inhibitory control, set maintenance, self-monitoring). Therefore, process measures obtained in the course of performance-based testing are often reported as executive function variables.
The majority of research examining the validity of the process approach in children has focused on the relationship between process scores and measures of executive function, and the differences in performance on these additional measures between clinical samples and controls. Results of these lines of research have been mixed. Beebe, Ris, and Dietrich (2000) examined the correlation of process scores (e.g., semantic clustering, percent recall consistency, perseverations, intrusions) from the CVLT-C with established measures of executive function (i.e., Wisconsin Card Sorting Test, Heaton, Chelune, Talley, Kay, & Curtiss 1993; Conners’ Continuous Performance Test, Conners, 1995). They found that CVLT-C outcome scores, but not process scores, were associated with measures of executive function, and concluded that the clinical interpretation of process measures from the CVLT-C as indices of executive function was not supported. In contrast, Kramer, Delis, Kaplan, O'Donnel, and Prifitera (1997) found sex differences on the CVLT-C in a community sample, such that girls outperformed boys on both summary (i.e., total words recalled in trials 1−5) and process scores (i.e., semantic clustering), even though boys had higher estimated Verbal IQ. Among clinical samples (e.g., head injury, low birth weight, reading disability), researchers have documented deficits in both summary and process scores from the CVLT-C (Hoffman, Donders, & Thompson, 2000; Levin et al., 2000; Roman et al., 1998; Taylor, Klien, Minich, & Hack, 2000). Thus, further investigation of the validity of these attempts to quantify the process approach in children appears warranted.
Executive functioning and the process approach in ADHD
Recent models of ADHD suggest that deficits in executive function (EF), rather than attention, represent the core deficit in ADHD (Barkley, 1997, 2000). Initiation, planning, organization, shifting of thought or attention, inhibition of inappropriate thought or behavior, and efficiently sustained and sequenced behavior are all crucial elements of EF, and as such it should be viewed as a multidimensional construct (Harris et al., 1995). While group differences in performance on measures of executive functioning are relatively consistently described in the literature comparing children with ADHD to controls, there is less clarity supporting the use of executive function measures to correctly discriminate between children with ADHD and controls. Barkley (1997) argued that neuropsychological tests have adequate sensitivity, but limited specificity, in contributing to the diagnosis of ADHD. In contrast, Berlin and colleagues reported adequate discriminative power (76.2% sensitivity and 90.5% specificity) of executive function tests in classifying children with ADHD (Berlin, Bohlin, Nyberg, & Janols, 2004), and other groups have also supported the utility of neuropsychological testing in discriminating children with ADHD from controls (Pineda, Ardila, & Rosselli, 1999; Rubia, Smith, & Taylor, 2007). It should be noted, however, that discriminating children with ADHD from controls is different than discriminating children with ADHD from other clinical samples, for which measures of executive functioning (e.g., the Stroop Test, Stroop, 1935) have not been shown to be as particularly effective (e.g., Homack & Riccio, 2004).
Process scores that decompose the skills required to perform tasks assessing the different components of EF may thus have particular value in characterizing unique patterns of dysfunction among different subgroups of children with ADHD (i.e., boys versus girls, ADHD subtypes), and may add valuable information for the clinician. In a study examining total versus process scores in children with either Tourette syndrome (TS) or ADHD, Mahone, Koth, Cutting, Singer, and Denckla (2001) found that process scores on the CVLT-C (i.e., number of spontaneous intrusion errors committed before cueing trials) were greater in both the TS and ADHD groups than in controls, whereas total scaled scores for recall were not different among the groups. In a related study, Cutting, Koth, Mahone, and Denckla (2003) examined group (ADHD versus control) and sex differences on process scores from the CVLT-C in children screened for reading disorders. While children with ADHD initially learned a similar amount of information as controls, they had significantly more trouble retaining information after a delay (even with cueing, and in recognition format). No differences were noted between groups on other process variables (e.g., perseverations, learning style – semantic clustering); however, sex differences were described, such that girls used semantic clustering more than boys, even though boys had higher Verbal IQ (Cutting et al., 2003), highlighting the importance of considering different strategies used by girls and boys.
D-KEFS and ADHD
The Delis Kaplan Executive Function System (D-KEFS, Delis et al., 2001) is a unique measure of EF because it provides information based on adaptations of well-established tests (e.g., Stroop Test, Stroop, 1935; Trailmaking Test, Army Individual Test Battery, 1944) through “primary measures” (i.e., summary scores and contrast scores that compare skills involving greater executive demand with those requiring less executive demand). In addition, it also provides “optional measures” that quantify the process by which these total scores are achieved. Previous research from our lab (Wodka et al., 2006) investigated the validity of D-KEFS primary measures. Children with ADHD performed significantly worse than typically developing children (TD) on only summary scores, with no group differences observed on any of the contrast scores. Measures of planning (i.e., Tower) best discriminated girls with ADHD from TD girls, while measures requiring speed/efficiency (Color–Word Interference) best discriminated boys with ADHD from TD. Sex by ADHD subtype interactions were observed on Color–Word Interference, such that children with the subtype of ADHD less likely to occur in their sex (i.e., Combined/Hyperactive-Impulsive subtype for girls, Inattentive subtype for boys) performed worse on the tasks.
Purpose of the study
To date, there have been no published studies investigating the validity of the D-KEFS optional “process” scores in children, nor does the D-KEFS manual report any data on the validity of these scores. Therefore, this study was exploratory in nature, the purpose being to examine group (ADHD versus typically developing [TD] children), sex, and ADHD subtype differences on process measures of EF, as quantified by the D-KEFS.
METHOD
Participants
Participants for the present study are from the same cohort as those examined in a recent study describing the discriminability of the primary measures from the D-KEFS (Wodka et al., 2006). Participants (n = 123) were recruited from outpatient service providers (e.g., clinics at the Kennedy Krieger Institute, local area physicians and psychologists), as well as schools, community organizations, and local chapters of Children and Adults with Attention-Deficit/Hyperactivity Disorder (CHADD). Children included in the study were between 8 years 0 months and 16 years 11 months, and had a Full Scale IQ estimate of 80 or higher, based on present performance on Wechsler Intelligence Scale for Children – Fourth Edition (WISC-IV; Wechsler, 2003) or school assessment within 1 year of study participation. Children were excluded from participation if there was history of speech/language disorder or a reading disability (RD) either screened out before a visit or based on prior school assessment (completed within 1 year of the current assessment). Further exclusion criteria included evidence of visual or hearing impairment, or history of other neurological or psychiatric disorder.
To minimize the likelihood of confound between sex and subtype, we oversampled for the type of ADHD less likely to occur in each sex. Specifically, we recruited girls with Combined Type (to comprise at least 40% of the sample) and boys with Inattentive Type (to comprise at least 40% of the sample). Structured parent interview, Diagnostic Interview for Children and Adolescents, Fourth Edition (DICA-IV, Reich, Welner, & Herjanic, 1997) and ADHD-specific and broad behavior rating scales (Conners’ Parent and Teacher Rating Scale – Revised, Long Form, CPRS-R/CTRS-R, Conners, 1997) were used to confirm ADHD diagnosis.1 Children with DSM-IV diagnoses other than Oppositional Defiant Disorder and Simple Phobias were excluded. The CPRS-R/CTRS-R and DSM-IV criteria were also used to evaluate ADHD subtype (i.e., Predominantly Hyperactive-Impulsive: ADHD-HI, Predominantly Inattentive: ADHD-I, or Combined: ADHD-C). As only two children met criteria for ADHD-HI, the ADHD-C and ADHD-HI children were combined into one ADHD-C/HI group. Every attempt was made to match the groups on the basis of age, FSIQ, sex, and minority status. Children with ADHD were excluded from the present study if they were taking longer-acting psychoactive medications (i.e., other than stimulants).
Additional exclusion criteria for TD included history of mental health services for behavior or emotional problems, parent or teacher report of previous diagnosis of Oppositional Defiant Disorder (ODD) or Conduct Disorder (CD), history of academic problems requiring school-based intervention services, or history of defined primary reading or language-based learning disability. Parents of children in the TD group also completed the DICA-IV and CPRS-R, and teachers completed the CTRS-R. TD with T-scores greater than 60 on the ADHD (DSM-IV Inattention; DSM-IV Hyperactivity) subscales of CPRS-R or CTRS-R were also excluded from the study.
Procedures
Parents of participants were screened over the phone to obtain demographic information, referral source, school, and developmental history. Parents of children with ADHD were asked not to administer stimulant medication on the day of and day prior to testing. Participants provided written consent (caregivers) and assent (children) before beginning testing and received a copy of the consent form. On the day of the assessment, children were administered the WISC-IV (if no prior estimate of intelligence was available), the Word Reading subtest from the Wechsler Individual Achievement Test – Second Edition (WIAT-II, Wechsler, 2002), and the Color–Word Interference, Tower, Trail Making, and Verbal Fluency subtests of the D-KEFS; the battery took approximately 2½ hours to administer/complete. While children completed the assessment, parents completed a brief background questionnaire and the CPRS-R; Teacher forms were mailed to the child's school (upon qualifying for the study) to be completed and returned by mail.
The D-KEFS (Delis et al., 2001) was used to measure executive functioning. The D-KEFS was developed to assess key components of executive functions and many subtests were based on well-established tests of executive function found in the literature. The advantage of this battery is that each of these separate tests is normed on the same national normative sample (1,750 children and adults); further, in addition to the traditional executive task, other measures of basic “ingredient skills” necessary for successful completion of the executive tasks are included. Standardized information regarding error performance across tests is also available, based on the performance of the normative sample.
Four of the eight tests from the D-KEFS were selected for this study based on their demonstrated utility in the literature to assess executive functions in child populations: Trail Making, Verbal Fluency, Color–Word Interference, and Tower tests; the tests are described below. Furthermore, these tests provide an adequate sample of the various components of executive function (i.e., response preparation, inhibition, working memory, planning, cognitive flexibility), and present several process scores for examination (i.e., error, interval, and ratio). In the present study, process scores were examined and are quantified as standard score or cumulative percentile (discussed in detail below).
Trail Making
This test consists of a visual cancellation task and a series of four “connect-the-circle” tasks, and was based on the original trail making test (Army Individual Test Battery, 1944). There are five conditions of the task. Four conditions assess the basic “ingredient skills” necessary to complete the primary executive function task (Condition 4: Number–Letter Switching), which assesses flexibility of thinking on a visual–motor sequencing task. Normative information is available for primary, contrast, and error performance. For the present study, error measures (omission, commission, sequencing, set loss, and time discontinue) by test condition (quantified by cumulative percentile) and total errors for Condition 4 (quantified by standard score) were examined.
Verbal Fluency
This test includes six 1-minute trials arranged into three conditions: Letter Fluency (three trials), Category Fluency (two trials), and Category Switching (one trial). The executive condition in this test is Category Switching, which requires the examinee to generate words, alternating between two different semantic categories as quickly as possible. This test measures the examinee's ability to generate words fluently in an effortful, phonemic format (Letter Fluency), from overlearned concepts (Category Fluency), and while simultaneously shifting between overlearned concepts (Category Switching); for each condition, responses are recorded per 15-second interval. In the present study, total responses for all three conditions per 15-second interval (quantified by standard score), total set-loss and repetition errors (quantified by standard score), as well as percent set-loss errors, repetition errors, and switching accuracy (quantified by cumulative percentile) were examined.
Color–Word Interference
This test includes four conditions: Color Naming, Word Reading, Inhibition, and Inhibition/Switching; two of which measure “ingredient skills” and two of which are the executive conditions. The primary executive function measured with this test is the examinee's ability to inhibit an overlearned verbal response (i.e., reading the printed words) in order to generate a conflicting response of naming the dissonant ink colors in which the words are printed (Condition 3). This is similar to the traditional Stroop task, for which the examinee must inhibit reading the words in order to name the dissonant ink colors in which those words are printed. The D-KEFS test also includes a new executive function task (Condition 4), for which the examinee is asked to switch back and forth between naming the dissonant ink colors and reading the words. This condition is thus a means of evaluating both inhibitory control and cognitive flexibility, as well as adding significant demand for working memory (i.e., remembering the rule while completing the task). In the present study, corrected and uncorrected errors (Conditions 3 and 4, quantified by cumulative percentile), and total errors (Conditions 1 and 2, quantified by cumulative percentile, Conditions 3 and 4 quantified by standard score) were examined.
Tower
The objective of this task is to move disks, varying in size from small to large, across three pegs to build a designated tower in the fewest number of moves possible. In constructing the target towers, the examinee must follow two rules: (1) move only one disk at a time; and (2) never place a larger disk over a smaller disk. This test assesses several key executive functions, including spatial planning, rule learning, inhibitory control of impulsive and perseverative responding, and the ability to establish and maintain the instructional set. In the present study, time to first move, time-per-move ratio, move accuracy ratio, and rule-violations-per-item ratio (quantified by standard score) and total rule violations (quantified by cumulative percentile) were examined.
Data analyses
A total of 35 measures were examined in the present study and were quantified as either scaled scores (M = 10, SD = 3; 16 variables) or cumulative percentiles (range = 0−100%; 19 variables). Due to the high rate of perfect scores on measures quantified by cumulative percentile, dichotomous variables were created for those who demonstrated perfect performance (i.e., cumulative percentile = 100%) and those who made one or more errors (i.e., cumulative percentile < 100%). Variables in which the cumulative percentile was >90 for each child in both groups (ADHD and control) were not included in analyses (total of 9 variables); therefore, a total of 26 variables were analyzed. First, group and sex comparisons for variables quantified by scaled scores were made using 2 × 2 factorial ANCOVAs, covarying for IQ. Second, separate group and sex comparisons were made using chi-square analyses for dichotomized cumulative percentile variables. Finally, children with ADHD-C/HI were compared to children with ADHD-I on scaled score variables (ANOVA) and dichotomized cumulative percentile variables (chi-square).
Effect size values were computed for comparisons using the d statistic. Effect size is a standardized quantitative index that can represent the magnitude of change that one variable produces in another variable as reflected in the difference between two means, independent of sample size (Cohen, 1988). Interpretation of the effect size d was based on a convention suggested by Cohen, such that 0.20 is considered a “small” effect size, 0.50 is considered “medium,” and 0.80 or greater is a “large” effect size. To protect against Type I error, a more conservative significance level of .01 was used throughout.
RESULTS
Demographic information
Demographic information for the sample is provided in Table 1. The sample was predominantly Caucasian (76% Caucasian, 11% African-American, 1% Asian, 2% Hispanic, and 10% mixed race or other ethnic/racial groups), drawn from a largely middle-class SES, and predominantly male (ADHD: 59.3%; TD: 50.7%). Children ranged in age from 8 to 16 years (M = 11.3, SD = 2.1). The ADHD and TD groups did not differ in SES, F(110) = 1.0, p = .32, sex (χ2 = 0.9, p = .35), racial distribution (χ2 = 3.7, p = .72), or handedness (χ2 = 2.6, p = .27); however, children in the TD group had significantly higher FSIQ scores than the ADHD group, F(121) = 10.8, p = .001, while there was a strong trend towards children with ADHD being significantly older than children in the TD group, F(121) = 5.1, p = .03.
Table 1.
Demographic information
| TD |
ADHD |
|||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Boys (n = 35) |
Girls (n = 34) |
Total (n = 69) |
Boys (n = 32) |
Girls (n = 22) |
Total (n = 54) |
|||||||
| Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | Mean | SD | |
| Age | 11.1 | 1.7 | 11.0 | 2.2 | 11.0 | 1.9 | 12.4 | 2.1 | 11.0 | 2.1 | 11.8 | 2.2 |
| SES | 51.5 | 11.2 | 54.7 | 8.4 | 53.1 | 9.9 | 54.8 | 10.8 | 55.2 | 7.8 | 54.9 | 9.6 |
| FSIQ* | 115.9 | 12.4 | 114.9 | 10.3 | 115.6 | 11.7 | 107.8 | 13.5 | 110.8 | 14.1 | 108.1 | 13.4 |
ADHD = Attention Deficit Hyperactivity Disorder; SES = Hollingshead Index; SES data not available for five participants in the TD group and six in the ADHD group; **TD > ADHD, p < .01.
Children with ADHD were further described (per parent report on the DICA-IV and CPRS-R/CTRS-R) by ADHD subtype (i.e., Combined type, n = 33; Hyperactive-Impulsive type, n = 2; Inattentive type, n = 19), and were combined into one group for the main analyses. Due to documented reduced sensitivity of tasks of EF in children with higher IQ scores (Mahone et al., 2002) and IQ differences between ADHD and TD groups, IQ was used as a covariate when comparing scaled scores via analysis of variance (ANCOVA).
Boys and girls in the sample did not differ significantly in racial distribution (χ2 = 2.4, p = .88) or handedness (χ2 = 2.3, p = .31), nor did they differ in the rate of ADHD (χ2 = 0.9, p = .35). Boys and girls were not significantly different in SES, F(110) = 1.0, p = .33, IQ, F(121) = 0.4, p = .55, or age, F(121) = 3.2, p = .08.
To examine performance subtype, two ADHD subtype groups were formed: Inattentive (n = 19) and Combined/Hyperactive-Impulsive (n = 35). The sex ratio was similar in these two ADHD subtype groups: 42% female for the Inattentive group and 39% female for the Combined/Hyperactive-Impulsive group (χ2 = 0.04, p = .85) and there was no difference in racial distribution (χ2 = 4.1, p = .53), handedness (χ2 = 0.2, p = .92), IQ, F(50) = 0.7, p = .42, age, F(50) = 0.01, p = .94, or SES, F(44) = 0.2, p = .64, between groups.
Group comparisons on process scores for executive function measures
Performance by group is reported in Table 2. No significant differences were noted between groups on any optional measure from the Trail Making, Verbal Fluency, Color–Word Interference, and Tower Tests.
Table 2.
Performance on D-KEFS process variables for ADHD and TD groups
| TD n = 69 |
ADHD n = 54 |
|||||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Mean (SD) | Min. | Max. | % Perfect Score | Mean (SD) | Min. | Max. | % Perfect Score | pa | db |
| TRAILS — Scaled Score | ||||||||||
| Condition 4 Total Errors | 11.0 (1.5) | 5 | 12 | — | 10.6 (1.4) | 6 | 12 | — | .475 | 0.1 |
| TRAILS — Cumulative Percentile | ||||||||||
| Condition 1 Omission Errors | 90.6 (26.3) | 6 | 100 | 88.4 | 94.2 (20.9) | 14 | 100 | 92.6 | .437 | 0.1 |
| Condition 4 Sequencing Errors | 79.9 (32.3) | 9 | 100 | 71.0 | 72.0 (36.1) | 10 | 100 | 61.1 | .248 | 0.2 |
| Condition 4 Set-Loss Errors | 72.3 (36.2) | 11 | 100 | 62.3 | 76.6 (35.1) | 5 | 100 | 68.5 | .474 | 0.1 |
| VERBAL FLUENCY — Scaled Score | ||||||||||
| 1st Interval Total Correct | 13.5 (3.1) | 5 | 19 | — | 11.8 (3.2) | 6 | 19 | — | .102 | 0.4 |
| 2nd Interval Total Correct | 11.6 (3.4) | 5 | 19 | — | 10.5 (3.3) | 5 | 19 | — | .702 | 0.1 |
| 3rd Interval Total Correct | 11.4 (2.7) | 5 | 18 | — | 10.3 (3.4) | 4 | 19 | — | .252 | 0.2 |
| 4th Interval Total Correct | 11.1 (2.8) | 6 | 17 | — | 10.0 (3.1) | 4 | 19 | — | .590 | 0.1 |
| Set Loss Errors | 11.5 (2.2) | 3 | 13 | — | 11.3 (2.5) | 1 | 13 | — | .387 | 0.1 |
| Repetition Errors | 8.9 (2.0) | 1 | 12 | — | 8.6 (2.3) | 1 | 12 | — | .332 | 0.2 |
| Percent Set-Loss Errors | 11.9 (2.5) | 3 | 14 | — | 11.5 (2.9) | 1 | 14 | — | .309 | 0.2 |
| Percent Repetition Errors | 10.1 (3.3) | 1 | 13 | — | 9.6 (3.7) | 1 | 13 | — | .425 | 0.1 |
| Category Switching: Percent Accuracy | 11.0 (2.1) | 2 | 12 | — | 10.8 (2.3) | 1 | 12 | — | .501 | 0.1 |
| COLOR—WORD — Scaled Score | ||||||||||
| Condition 3 Total Errors | 10.4 (2.7) | 1 | 14 | — | 8.8 (3.4) | 1 | 13 | — | .066 | 0.5 |
| Condition 4 Total Errors | 9.8 (2.8) | 1 | 15 | — | 8.7 (2.9) | 3 | 13 | — | .100 | 0.4 |
| COLOR—WORD — Cumulative Percentile | ||||||||||
| Condition 1 Total Errors | 57.7 (33.7) | 2 | 100 | 34.8 | 53.2 (37.5) | 1 | 100 | 35.2 | .963 | 0.0 |
| Condition 2 Total Errors | 64.2 (40.6) | 1 | 100 | 55.1 | 65.5 (42.6) | 1 | 100 | 59.3 | .642 | 0.0 |
| Condition 3 Corrected Errors | 48.3 (26.7) | 1 | 100 | 15.9 | 36.6 (31.2) | 2 | 100 | 14.8 | .864 | 0.0 |
| Condition 3 Uncorrected Errors | 69.0 (32.7) | 4 | 100 | 46.4 | 69.1 (34.3) | 2 | 100 | 48.1 | .845 | 0.0 |
| Condition 4 Corrected Errors | 42.6 (30.7) | 1 | 100 | 17.4 | 32.4 (30.7) | 1 | 100 | 13.0 | .500 | 0.1 |
| Condition 4 Uncorrected Errors | 69.2 (31.8) | 1 | 100 | 43.5 | 65.4 (30.0) | 10 | 100 | 35.2 | .351 | 0.2 |
| TOWER — Scaled Score | ||||||||||
| Mean to First-Move Time | 12.1 (1.6) | 7 | 15 | — | 11.7 (2.3) | 1 | 15 | — | .541 | 0.1 |
| Time-Per-Move-Ratio | 10.9 (1.7) | 6 | 15 | — | 10.0 (2.8) | 1 | 15 | — | .249 | 0.2 |
| Move Accuracy Ratio | 8.9 (2.2) | 3 | 13 | — | 8.9 (2.9) | 2 | 16 | — | .501 | 0.1 |
| Rule-Violations-Per-Item-Ratio | 10.1 (1.4) | 4 | 11 | — | 9.9 (1.3) | 5 | 11 | — | .474 | 0.1 |
| TOWER — Cumulative Percentile | ||||||||||
| Total Rule Violations | 61.0 (31.1) | 4 | 100 | 30.4 | 60.1 (35.0) | 8 | 100 | 38.9 | .326 | 0.2 |
ADHD = Attention Deficit Hyperactivity Disorder; D-KEFS = Delis Kaplan Executive Function System
Scaled score variables were compared with ANCOVA, covarying for IQ; cumulative percentile variables were dichotomized (perfect score versus not) and compared with chi-Square analyses
Effect size (Cohen's d) for group comparison (ADHD vs. TD); — no value available as all children made no errors (perfect scores). The following variables were not included in analyses due to >90% of children in ADHD and control groups achieving perfect scores: Trail Making — Condition 1 Commission Errors, Condition 2 Sequencing Errors, Condition 2 Set-Loss Errors, Condition 2 Time-Discontinue Errors, Condition 3 Sequencing Errors, Condition 3 Set-Loss Errors, Condition 3 Time-Discontinue Errors, Condition 4 Time-Discontinue Errors, Condition 5 Time-Discontinue Errors.
Sex comparisons (total sample) on executive function measures
Girls (total sample) performed significantly better, F(1, 117) = 11.5, p = .001, d = 0.6, than boys on the Verbal Fluency First Interval Total Correct. There were no other significant sex or group-by-sex interaction effects for any other variables (error, ratio, or interval) examined above on individual D-KEFS measures.
ADHD subtype by sex comparisons on process scores
ADHD subtype comparisons were completed using the two ADHD subtype groups reported above (ADHD-I, n = 19 and ADHD-C/HI, n = 35). A significant interaction effect (ADHD subtype-by-sex) was observed for only Verbal Fluency Repetition Total Errors, F(49)= 7.5, p = .01, d = 0.8 (Figure 1); boys with ADHDC/HI better than girls with ADHD-C/HI, whereas girls with ADHD-I performed better than boys with ADHD-I. There were no other significant group (ADHD subtype), sex, or group-by-sex interaction effects noted for other variables examined on the individual D-KEFS measures.
Figure 1.
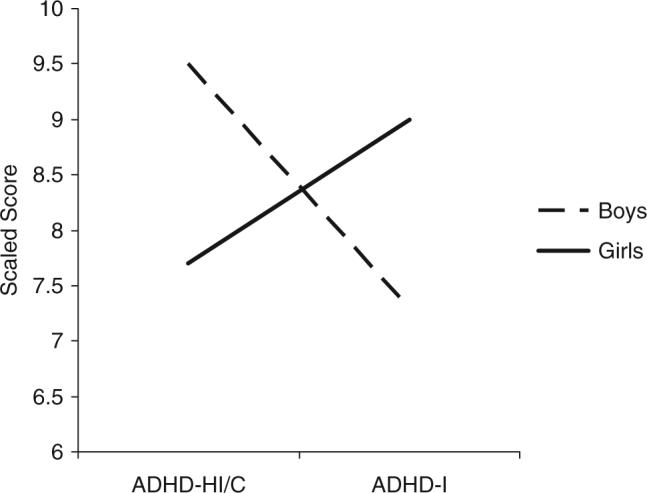
ADHD Subtype by sex interaction for verbal fluency total repetition errors. ADHD = Attention Deficit Hyperactivity Disorder; HI/C = Hyperactive/Impulsive + Combined sub-types; I = Inattentive subtype; 2 × 2 ANOVA; main effects for subtype and sex ns; interaction effect significant p <.01, d = 0.8.
DISCUSSION
The present results suggest that the optional “process” scores generated on four D-KEFS tests commonly used by pediatric neuropsychologists (i.e., Trails, Verbal Fluency, Color–Word, Tower) have limited sensitivity in identifying behavioral differences between children with ADHD and typically developing children (TD). Of the 35 optional D-KEFS scaled scores and cumulative percentiles analyzed, we were unable to identify any significant group differences. In fact, analyses were not performed on nine of the cumulative percentile scores obtained from the Trail Making Test, as over 90% of children in both the ADHD and TD groups had perfect scores (i.e., no errors) for these variables; on five variables, all children in both groups achieved perfect scores. In short, we found no process score on these four tests in which children with ADHD were deficient or significantly different than TD. These results are in contrast to findings in previous research from our lab in which significant group differences (favoring TD) were identified on primary scores from both the Color–Word and Tower tests (Wodka et al., 2006).
Most previous research examining sex differences in components of executive function among children with ADHD has not accounted for sex-related differences in ADHD subtype (Seidman et al., 2005). In the present study, we oversampled for girls with ADHD, and for the ADHD subtypes less common in each sex. As a result, our sample of children with ADHD was 41% female (compared with the rate of rate of girls with ADHD in the general population, estimated to be around 20% of all children with ADHD; DSM-IV-TR, American Psychiatric Association, 2000). Further, in clinical samples, girls with ADHD are more likely to present with Inattentive subtype, while boys with ADHD are more likely to present with Combined subtype (Weiler, Bellinger, Marmor, Rancier, & Waber, 1999). We oversampled in an attempt to make our ADHD groups more closely matched on subtype within sex. In the entire sample, we did identify significant sex differences on the first 15-second interval of Verbal Fluency, favoring girls, suggesting that girls of similar age may be more efficient than boys at task initiation when rapid oral output is required. While no main effects for ADHD subtype were identified, a sexby-group interaction for Verbal Fluency Total Repetition errors was found, highlighting the relative vulnerability of girls with ADHD (compared to boys) for these types of errors. Such repetition errors on Verbal Fluency can potentially be related to deficits in working memory (e.g., forgetting which words have already been said), or possibly to inhibitory deficits (e.g., blurting words out instead of subvocalizing). Regardless, most of the D-KEFS optional scores examined did not demonstrate either sex differences or sex-by-group interactions.
Our results are consistent with previous research by Beebe et al. (2000), who argued that these quantified process scores add little to understanding the behavioral differences expressed in children with ADHD. It is possible that these scores on the D-KEFS are less sensitive because they fail to quantify the strategy used by children. It is also possible that group differences were minimized in our sample because our groups had relatively high IQ scores (mean FSIQ 115 for TD group, 108 for ADHD group). Previous research has shown a strong relationship between IQ and performance-based tests of EF, such that these tests are less sensitive in children with high average IQ and above (Mahone et al., 2002), and group effects may be stronger among samples with a wider range of IQ, or among samples of children with ADHD in which a wider range of learning and psychiatric comorbidities are allowed. However, because we purposely recruited children with relatively “pure” ADHD as part of a larger study using neuroimaging, the severity of executive dysfunction and range of IQ typically observed among clinical groups may have been minimized. Even though we covaried for IQ differences, the fact that so many children in our sample had above average IQ may have reduced the number having these “process” type errors. It is entirely possible that future research may identify more ADHD-related executive dysfunction in children with lower IQ, or those with a more representative range of comorbidities, since our sample of children with ADHD was screened for low IQ, reading disorders, and most psychiatric disorders.
Clinicians using the D-KEFS obtain an exceptionally large number of variables to consider when making clinical decisions. The results of the present study, along with our recent findings when assessing primary scores (Wodka et al., 2006), suggest that the primary summary scores, rather than primary contrast scores or optional process scores, appear to be most sensitive in identifying executive dysfunction in children with ADHD. A large proportion of children (both ADHD and TD) obtain perfect scores on some of the process-related variables, and as such, studies examining group data may not highlight the utility of these scores. The process scores that generate cumulative percentiles may provide the clinician with useful information about the individual child, especially when these uncommon errors are observed. Indeed, it may be the within-individual variability that is ultimately of most use clinically, and future research with the D-KEFS in children should consider these data in addition to group means.
The strengths of this study include its large sample size, careful screening for ADHD/exclusion of children with comorbid reading or psychiatric disorders, and selective matched control group of typically developing children. Furthermore, this study provided an examination of optional contrast/process scores provided by the D-KEFS that have little support in the literature. However, our findings were limited by several factors. First, as there are many optional scores provided by the D-KEFS, many analyses were necessary. Therefore, the likelihood for Type I error was considered in the interpretation of results and given that few significant results were found, the limited sensitivity of D-KEFS process scores is further supported through multiple analyses. Second, methods of diagnosing ADHD may have contributed to the limited findings, as no measures of neuropsychological functioning were used in making ADHD diagnosis. Future research should continue to explore the utility of the combination of tests, rating scales, and interview in diagnosing ADHD. Third, as our findings are entirely specific to the D-KEFS, null findings may be related, at least in part, to the low reliability of the D-KEFS at younger ages (Delis et al., 2001). Future research should also consider other process measures of executive functioning (e.g., NEPSY) in examining children with ADHD, and the effects of sex and ADHD subtype in this population.
In conclusion, the optional process scores from the D-KEFS do not appear to be sensitive in distinguishing children with ADHD from typically developing controls. As perfect performance is commonly noted on many optional error scores, any score less than 100% accuracy may be clinically significant on an individual level. When considering ADHD subtype and sex, preliminary evidence suggests that children with the ADHD subtype less common for sex may demonstrate relative deficits on these process measures.
ACKNOWLEDGMENTS
Supported by HD-24061 (Mental Retardation and Developmental Disabilities Research Center), R01 NS043480, K08 NS02039, K02 NS044850, R01 NS047781, HRSA 6R03MC00030, M01 RR00052 (Johns Hopkins General Clinical Research Center).
Footnotes
Children in the ADHD group were recruited into the study based on previous diagnoses of ADHD in the community. Once recruited, ADHD diagnosis was confirmed using DSM-IV criteria, which require that symptoms be present in at least two settings. Participants were required to meet DSM-IV criteria for ADHD based on the Diagnostic Interview for Children and Adolescents-IV (DICA-IV; Reich et al., 1997) interview conducted with the parent; signs/symptoms must have been present before age 7 years and must have persisted for longer than 6 months. In addition, two questionnaires were administered to each child's parent and teacher, and participants were required to meet criteria on one of the two parent questionnaires/rating scales (Conners, 1997; DuPaul, 1998) and on one of the two teacher questionnaires/rating scales (Conners, 1997; DuPaul, 1998).
REFERENCES
- Akshoomoof NA, Delis DC, Kiefner MG. Block constructions of alcoholic and unilateral brain-damaged patients: A test of the right hemisphere vulnerability hypothesis of alcoholism. Archives of Clinical Neuropsychology. 1989;4:275–281. [PubMed] [Google Scholar]
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders, fourth edition – text revision. American Psychiatric Association; Washington, DC: 2000. [Google Scholar]
- Army Individual Test Battery . Manual of directions and scoring. War Department, Adjutant General's Office; Washington, DC: 1944. [Google Scholar]
- Barkley RA. Behavioral inhibition, sustained attention, and executive functions: Constructing a unifying theory of ADHD. Psychological Bulletin. 1997;121:65–94. doi: 10.1037/0033-2909.121.1.65. [DOI] [PubMed] [Google Scholar]
- Barkley RA. Genetics of childhood disorders XVII: ADHD Part 1. The executive functions and ADHD. Journal of the American Academy of Child and Adolescent Psychiatry. 2000;39:1064–1068. doi: 10.1097/00004583-200008000-00025. [DOI] [PubMed] [Google Scholar]
- Beebe DW, Ris DM, Dietrich KM. The relationship between CVLT-C process scores and measures of executive functioning: Lack of support among community adolescents. Journal of Clinical and Experimental Neuropsychology. 2000;22:779–792. doi: 10.1076/jcen.22.6.779.950. [DOI] [PubMed] [Google Scholar]
- Berlin L, Bohlin G, Nyberg L, Janols OL. How well do measures of inhibition and other executive functions discriminate between children with ADHD and controls? Child Neuropsychology. 2004;10:1–13. doi: 10.1076/chin.10.1.1.26243. [DOI] [PubMed] [Google Scholar]
- Cohen J. Statistical power analysis for the behavioral sciences. 2nd ed. Lawrence Erlbaum Associates, Inc.; Hillsdale, NJ: 1988. [Google Scholar]
- Conners CK. Conners’ Rating Scales – Revised. Multi-Health Systems Inc.; North Tonawanda, NY: 1997. [Google Scholar]
- Conners CK. Conners’ Continuous Performance Test. Multi-Health Systems, Inc.; Toronto: 1995. [Google Scholar]
- Cutting LE, Koth CE, Mahone EM, Denckla MB. Children with Attention/Deficit Hyperactivity Disorder without Reading Disabilities. Journal of Learning Disabilities. 2003;36:259–269. doi: 10.1177/002221940303600305. [DOI] [PubMed] [Google Scholar]
- Delis D, Kaplan E, Kramer J. Delis-Kaplan Executive Function Scale. The Psychological Corporation; San Antonio, TX: 2001. [Google Scholar]
- Delis DC, Kramer JH, Kaplan E, Ober BA. California Verbal Learning Test —Children's Version: Manual. The Psychological Corporation; San Antonia, TX: 1994. [Google Scholar]
- DuPaul GJ, Power TJ, Anastopoulos AD, Reid R. ADHD Rating Scale–IV. Guilford Press; New York: 1998. [Google Scholar]
- Harris EL, Singer HS, Reader MJ, Brown J, Cox C, Mohr J, et al. Executive function in children with Tourette syndrome and/or attention deficit hyperactivity disorder. Journal of the International Neuropsychological Society. 1995;1:511–516. doi: 10.1017/s1355617700000631. [DOI] [PubMed] [Google Scholar]
- Heaton RK, Chelune GJ, Talley JL, Kay GG, Curtiss G. Wisconsin Card Sorting Test Manual: Revised and Expanded. Psychological Assessment Resources; Odessa, FL: 1993. [Google Scholar]
- Hoffman N, Donders J, Thompson EH. Novel learning abilities after traumatic brain injury in children. Archives of Clinical Neuropsychology. 2000;15:47–58. [PubMed] [Google Scholar]
- Homack S, Riccio CA. A meta-analysis of the sensitivity and specificity of the Stroop Color and Word Test with children. Archives of Clinical Neuropsychology. 2004;19:725–743. doi: 10.1016/j.acn.2003.09.003. [DOI] [PubMed] [Google Scholar]
- Kaplan E. The process approach to neuropsychological assessment of psychiatric patients. Neuropsychological Update Series. 1990;2:72–87. doi: 10.1176/jnp.2.1.72. [DOI] [PubMed] [Google Scholar]
- Kaplan E, Fein D, Morris R, Delis DC. Wechsler Adult Intelligence Scale – Revised as a Neuropsychological Instrument. The Psychological Corporation; San Antonio, TX: 1991. [Google Scholar]
- Kaplan E, Fein D, Kramer J, Delis DC, Morris R. Wechsler Intelligence Scale for Children – Process Instrument. The Psychological Corporation; San Antonio, TX: 1999. [Google Scholar]
- Kaplan E, Fein D, Kramer J, Delis DC, Morris R. Wechsler Intelligence Scale for Children – Fourth Edition, integrated. The Psychological Corporation; San Antonio, TX: 2004. [Google Scholar]
- Korkman M, Kirk U, Kemp S. NEPSY. A developmental neuropsychological assessment. The Psychological Corporation; San Antonio, TX: 1998. [Google Scholar]
- Kramer JH, Delis DC, Kaplan E, O'Donnell L, Prifitera A. Developmental sex differences in verbal learning. Neuropsychology. 1997;11:577–584. doi: 10.1037//0894-4105.11.4.577. [DOI] [PubMed] [Google Scholar]
- Levin HS, Culhane KA, Hartmann J, Evankovich K, Mattson AJ, Harward H, et al. Developmental changes in performance on tests of purported frontal lobe functioning. Developmental Neuropsychology. 1991;7:377–395. [Google Scholar]
- Levin HS, Song J, Scheibel RS, Fletcher JM, Harward HN, Chapman SB. Dissociation of frequency and recency processing from list recall after severe closed head injury in children and adolescents. Journal of Clinical and Experimental Neuropsychology. 2000;22:1–15. doi: 10.1076/1380-3395(200002)22:1;1-8;FT001. [DOI] [PubMed] [Google Scholar]
- Mahone EM, Hagelthorn KM, Cutting LE, Schuerholz LJ, Pelletier SF, Rawlins C, et al. Effects of IQ on executive function measures in children with ADHD. Child Neuropsychology. 2002;8:41–51. doi: 10.1076/chin.8.1.52.8719. [DOI] [PubMed] [Google Scholar]
- Mahone EM, Koth CW, Cutting L, Singer HS, Denckla MB. Executive function in fluency and recall measures among children with Tourette Syndrome and ADHD. Journal of the International Neuropsychological Society. 2001;7:102–111. doi: 10.1017/s1355617701711101. [DOI] [PubMed] [Google Scholar]
- Pineda D, Ardila A, Rosselli M. Neuropsychological and behavioral assessment of ADHD in seven- to twelve-year-old children: A discriminant analysis. Journal of Learning Disabilities. 1999;32:159–173. doi: 10.1177/002221949903200206. [DOI] [PubMed] [Google Scholar]
- Reich W, Welner Z, Herjanic B. The diagnostic interview for children and adolescents-IV. Multi-Health Systems; North Tonawanda, NY: 1997. [Google Scholar]
- Roman MJ, Delis DC, Willerman L, Magulac M, Demadura TL, de la Pena JL, et al. Impact of pediatric brain injury on components of verbal memory. Journal of Clinical and Experimental Neuropsychology. 1998;20:245–258. doi: 10.1076/jcen.20.2.245.1168. [DOI] [PubMed] [Google Scholar]
- Rubia K, Smith A, Taylor E. Performance of children with Attention Deficit Hyperactivity Disorder (ADHD) on a test battery of impulsiveness. Child Neuropsychology. 2007;13:276–304. doi: 10.1080/09297040600770761. [DOI] [PubMed] [Google Scholar]
- Seidman LJ, Biederman J, Monuteaux MC, Valera E, Doyle AE, Farone SV. Impact of sex and age on executive functioning: Do girls and boys with and without attention deficit hyperactivity disorder differ neuropsychologically in preteen and teen years? Developmental Neuropsychology. 2005;27(1):79–105. doi: 10.1207/s15326942dn2701_4. [DOI] [PubMed] [Google Scholar]
- Stroop JR. Studies of interference in serial verbal reactions. Journal of Experimental Psychology. 1935;18:643–662. [Google Scholar]
- Taylor HG, Klien N, Minich NM, Hack M. Verbal memory deficits in children with less than 750 g birth weight. Child Neuropsychology. 2000;16:49–63. doi: 10.1076/0929-7049(200003)6:1;1-B;FT049. [DOI] [PubMed] [Google Scholar]
- Wechsler DL. Wechsler Intelligence Scale for Children—Revised. The Psychological Corporation; San Antonio, TX: 1974. [Google Scholar]
- Wechsler DL. Wechsler Individual Achievement Test – II. The Psychological Corporation; San Antonio, TX: 2002. [Google Scholar]
- Wechsler DL. Wechsler Intelligence Scale for Children. Fourth Edition The Psychological Corporation; San Antonio, TX: 2003. [Google Scholar]
- Weiler M, Bellinger D, Marmor J, Rancier S, Waber D. Mother and teacher reports of ADHD symptoms: DSM-IV questionnaire data. Journal of the American Academy of Child and Adolescent Psychiatry. 1999;38:1139–1147. doi: 10.1097/00004583-199909000-00018. [DOI] [PubMed] [Google Scholar]
- Wodka EL, Mostofsky SH, Prahme MC, Gidley Larson JC, Denckla MB, Mahone EM. Discriminant value of executive function measures in children with ADHD [Abstract]. Journal of the International Neuropsychological Society. 2006;12(51):39. [Google Scholar]