

Abstract
This paper examined whether individual differences in children’s vagal reactivity to peer provocation was related to domestic violence within the family. It also examined the question of whether conduct-problem children who show vagal augmentation to peer provocation come from families with high levels of domestic violence. During the peer provocation, children were expecting to interact with a difficult peer while vagal reactivity was assessed. Groups were divided into children who showed vagal augmentation and vagal suppression to the stressful peer interaction. Findings indicated that conduct-problem children who showed vagal augmentation to interpersonal challenge came from families with the highest levels of domestic violence. Vagal augmentation was also associated with a greater number of conduct-related problems for those children exposed to high levels of domestic violence. Discussion highlights the role of individual differences in physiological reactivity in understanding children’s behavior problems in relation to domestic violence.
Keywords: Cardiac vagal control, Cardiac vagal tone, Conduct-problems, Psychophysiology, Domestic violence
Domestic Violence and Vagal Reactivity to Peer Provocation
In his seminal paper, Porges (1995) suggested that the tonus of the vagus nerve provides a theoretical basis for the child’s ability to focus attentional processes, inhibit irrelevant activity, regulate emotion, and appropriately engage with the environment. While early work on vagal tone largely examined individual differences in baseline vagal functioning, more recently investigators have turned their attention to understanding individual differences in children’s physiological response to environmental challenge (e.g., Calkins & Dedmon, 2000).
In general, children’s ability to suppress vagal tone has been found to be the adaptive response to challenge. In infancy, a reduction in vagal tone during challenging situations is related to better state regulation, greater self-soothing and more attentional control. For example, DeGangi, DiPietro, Greenspan and Porges (1991) reported that regulatory-disordered infants with high vagal tone exhibited the least vagal suppression during cognitive challenge. Infants who exhibited relatively small reductions in vagal tone during administration of the Bayley Scales were rated by their mothers as more aggressive, more depressed, and more withdrawn at age three than were infants who exhibited larger vagal reductions (Porges, Doussard-Roosevelt, Portales & Greenspan, 1996). Similarly, reductions in vagal tone have also been linked with fewer behavior problems and more appropriate emotion regulation in toddlers and preschoolers (Calkins, 1997; Calkins & Dedmon, 2000; Porges et al, 1996) and sustained attention in school-aged children (Suess et al, 1994).
Yet recent findings suggest that some children not only fail to suppress vagal tone but may in fact exhibit vagal augmentation during challenge. For example, DiPietro, Porges and Uhly (1992) found that infants who showed increases in vagal tone during presentation of a surprising stimulus (i.e., a jack-in-the-box toy) were more attentive to the stimulus than infants who showed decreases in vagal tone. However, the psychological significance of an augmentation in vagal reactivity is unclear. DiPietro et al (1992) interpreted their findings to suggest that in infants vagal augmentation may reflect heightened attentiveness and the ability to detect environmental change. This interpretation is consistent with Porges’ (1995) Social Engagement System model, which would predict that enhanced parasympathetic activation would occur during increased engagement with the environment. Increased attentiveness may help the child resist unintentional shifting to irrelevant or distracting information and, in the context of challenging circumstances, support emotion regulation efforts necessary for the child to effectively manage the challenge (Derryberry & Rothbart, 1988; Wilson & Gottman, 1996).
At the extreme, increased engagement or attentiveness may reflect hypervigilance to environmental events. Hypervigilance may develop in response to threatening environmental conditions, and may in fact be an adaptive response to particularly challenging life circumstances. For children, the family is a key social context that fosters socioemotional development. In family environments in which threat and hostility are habitual and salient social processes, children may learn to become hypervigilant to even mild forms of interpersonal negativity, as they portend escalation in conflict and may signal the potential for harm to themselves or family members. Children in these types of family environments may show heightened parasympathetic activation, particularly when they are in social situations that are stressful or conflictual since these types of settings may be reminders of the negative interactions they have observed at home (Katz, 2001).
In this paper, we examine vagal augmentation in children and its relation to the interpersonal environment. Exposure to domestic violence is examined as a salient interpersonal context that may be associated with vagal augmentation. Katz (2001) suggested that children from domestically violent homes may need to be hypervigilant to their surroundings, scanning their environment for cues of threat so that threat is detected early and an action plan can be developed. In this way, hypervigilance may help the child effectively monitor their own safety and support the emotion regulation efforts necessary to prepare for danger.
To the extent that vagal augmentation indexes hypervigilance, children who exhibit conduct-problem behavior may be particularly likely to show a heightened parasympathetic response since they have been described as being hypervigilant to interpersonal threat. Social information processing models suggest that aggressive children have a hostile attributional bias, characterized by a tendency to see hostility in the environment even with ambiguous social cues (Crick & Dodge, 1994). Because children with conduct problems have a tendency towards hypervigilance, they may be particularly sensitized to domestic violence and may be at risk for developing a pattern of heightened parasympathetic activation that generalizes to other difficult interpersonal situations. That is, one possibility is that for conduct-problem children vagal augmentation develops in response to a hostile and threatening social environment. If this is the case, we would expect that for conduct-problem children, vagal augmentation will be associated with higher levels of domestic violence while for typically developing children, there would be less of an association between vagal augmentation and domestic violence.
A related possibility is that vagal augmentation to interpersonal challenge is an endophenotype (e.g., Gottesman & Gould, 2003; Iacono, 1998) of those at risk for conduct-problems. An endophenotype is a heritable internal phenotype discoverable by analysis of biological functioning (Gottesman & Gould, 2003) that functions as a vulnerability factor. If vagal augmentation to interpersonal challenge is an endophenotype of risk for conduct problems, growing up in a family environment with high levels of violence may act as a catalyst and increase the child’s likelihood of exhibiting conduct-problem behaviors. To the extent that this is true, vagal augmentation should be associated with a greater number of conduct-related problems for those children exposed to high levels of domestic violence.
Both of these hypotheses will be tested in the present study. To provide a context for these arguments, we begin with a review of findings related to domestic violence and child adjustment. We then review the current state of knowledge on domestic violence and children’s vagal functioning, and suggest that examining vagal tone to interpersonal stress that is personally relevant more closely indexes their physiological response to the stressful interpersonal interactions children exposed to domestic violence experience in their daily home lives. The notion of individual differences in children’s vagal response to domestic violence is then discussed, and hypotheses related to differential reactions of conduct-problem children to exposure to DV are presented.
Domestic Violence and Child Adjustment
One of the most salient contexts for children’s development is the family environment, and when family relations go awry, children exhibit a variety of behavior problems (Mash & Barkley, 2003). Being exposed to domestic violence (DV) is perhaps one of the most stressful life circumstances for children. Consequently, children from domestically violent homes show a variety of mental health problems. One of the most consistent findings is that children from DV homes show externalizing problems, such as aggression, delinquency, and hostility towards others (Fantuzzo, DePaola, Lambert, Martino, Anderson & Sutton, 1991; Jouriles, Norwood, McDonald & Peters, 2001; Jaffe, Wolfe, Wilson & Zak, 1986; O’Keefe, 1994; Wolfe, Jaffe, Wilson & Zak, 1985; Wolfe & Korsch, 1994). They are also at increased risk for difficulties with anxiety (Christopolous et al, 1987; Hughes, 1988), depression (Spaccarelli, Sandler & Roosa, 1994; Sternberg et al, 1993), and self-esteem (Hughes, 1988).
The majority of research on children exposed to DV has examined children’s global psychological functioning, perhaps because of its over-reliance on parental report of child functioning. Little is known about the specific contexts that are most difficult for children who have experienced DV. Observational studies of marital and parent-child interaction suggest that children of battered women live in a family environment characterized by high levels of anger and hostility. When attempting to resolve marital conflict, DV couples use more provocative forms of negative affect such as contempt and belligerence than their maritally distressed but nonviolent counterparts (Burman, John & Margolin, 1992; Jacobson, Gottman, Waltz, Rushe, Babcock & Holtzworth-Munroe, 1994; Margolin, John & Gleberman, 1988), escalate negative interactions by reciprocating their partner’s negative affect (Coan, Gottman, Babcock & Jacobson, 1997), and are less likely to accept influence from their partners (Coan, Gottman, Babcock & Jacobson, 1997). In studies of parenting, domestic violence is associated with increased levels of conflict and controlling behavior (Holden & Ritchie, 1991; Margolin, John, Ghosh & Gordis, 1996), and higher rates of parent-child aggression (Jouriles & Norwood, 1995; O’Keefe, 1995). Since their family environments are replete with hostile and negative interactions, children in DV homes may not have learned the necessary skills to handle stressful interpersonal interactions. Furthermore, children from domestically violent homes may be sensitized to marital conflict (Cummings & Davies, 1994), and this increased sensitivity to conflict may generalize to other interpersonal relations, such as increased sensitivity to and difficulty managing conflict with peers.
One of the goals of this paper is to assess children’s reactions during peer interactions that involve negativity and hostility, since these types of interactions may parallel the interpersonal strain that children who have experienced DV observe at home. To do so, we examine peer provocation as an interpersonal context that may be particularly difficult for children exposed to DV. Peer provocation was examined for a variety of reasons. First, being provoked by a friend was hypothesized to be a peer-based equivalent of the type of interpersonal threat or hostility children may experience at home. Second, peer provocation was examined because it is a difficult, emotionally charged situation for all children and teachers have rated times at which children are teased, hit, or insulted by another child as very likely to cause problems (Dodge, McClaskey & Feldman, 1985). Provocation by peers may cause a range of emotional reactions, however, the optimal social response to provocation is to appear unfazed, as when ignoring or turning the situation into a joke (Gottman & Parker, 1986). However, since children from domestically violent homes have difficulty in the area of emotional expression and regulation (Graham-Bermann & Levendosky, 1998; Lee, 2001) they may have particular trouble in stressful peer interactions that require them to inhibit inappropriate behavior and choose effective interpersonal strategies to de-escalate conflict or neutralize a potentially volatile interpersonal interaction. Failure at doing so may explain why children have difficulty in social and emotional domains.
Domestic Violence and Vagal Functioning
Children’s reactivity to interpersonal stress may reflect an adaptation to living in a domestically violent home (Katz, 2001). In the adult literature, evidence from male batterers indicates that in some batterers the parasympathetic nervous system is activated during times of interpersonal stress. Gottman, Jacobson, Rushe, Shortt, Babcock, La Taillade and Waltz (1995) found a subgroup of male batterers (i.e. Type 1 batterers) who lowered their heart rates below baseline levels during a marital conflict interaction. When compared to other male batterers (i.e., Type 2 batterers), Type 1 batterers were more verbally aggressive toward their wives, were more violent towards others (e.g., friends, strangers, coworkers), and were more likely to have observed both parents acting violently toward each other. In follow-up analyses, Jacobson, Gottman and Shortt (1995) reported that Type 1 batterers increased their vagal tone from baseline to marital interaction whereas Type 2 batterers showed a decrease. They reasoned that the vagal increase in response to marital conflict was in the service of focused attention in that Type 1 batterers focus their attention to maximize the impact of their verbal aggression.
Although there have been no studies of vagal reactivity to interpersonal challenge in children from DV homes, El-Sheikh, Harger & Whitson (2001) found that baseline vagal tone moderated associations between physical marital conflict and children’s physical health for boys, but did not moderate associations between physical marital conflict and children’s psychological adjustment. Boys from maritally violent homes who had higher baseline vagal tone showed better physical health than boys who had lower baseline vagal tone. The present study extends these findings by examining vagal tone in response to interpersonal stress that is personally relevant, which may more closely resemble the types of stressful interpersonal interactions children from violent homes may experience in their home lives.
Conduct Problem Children’s Reactions to Domestic Violence
While many children in DV homes experience psychological distress, there are individual differences in how children respond to domestic violence with some children showing more profound behavioral disturbances than others (Ware, Jouriles, Spiller, McDonald, Swank, & Norwood, 2001). Children who exhibit behavior problems or have difficult temperaments may be at a higher risk for becoming sensitized to violence because they are more vulnerable or reactive to stress (Graham-Bermann, 2001).
Children with conduct problems may be particularly sensitized to violence because they have a tendency towards hypervigilance to interpersonal threat. Social information processing models suggest that aggressive children have a hostile attributional bias, characterized by a tendency to see hostility in the environment even with ambiguous social cues (Crick & Dodge, 1994). In this sense, their attentional systems may be operating in overdrive, continuously monitoring their environment for signals of social threat. Consistent with this view, Katz (2004) reported that aggressive children showed vagal augmentation to social challenge from a peer, but not to other stressors that did not have personal relevance. Moreover, vagal augmentation in response to a laboratory-based social challenge was related to observations of more negative interactions with a close friend.
Vagal augmentation may also help explain why children exposed to DV are at increased risk for problems with aggression. Social learning theories of the intergenerational transmission of violence suggest that children exposed to DV become aggressive because they model their parent’s aggressive behavior (Kwong, Bartholomew, Henderson & Trinke, 2003). If vagal augmentation during interpersonal challenge is associated with hypervigilance, conduct-problem children may be paying especially close attention to the forms of interpersonal aggression exhibited by parents in DV homes. This heightened attention may increase their encoding of aggressive behavior, which may be a necessary first step towards their enactment of aggressive and hostility towards others.
In this paper, we examine domestic violence as an environmental factor related to vagal augmentation. Individual differences in vagal augmentation were examined as a function of children’s risk status, and we test the hypothesis that conduct-problem children who show vagal augmentation in response to interpersonal challenge come from families with high levels of domestic violence. While it is impossible to tease out direction of effects in a cross-sectional study, we reasoned that for typically developing children, variations in vagal reactivity may reflect normal variations in the allocation of attentional resources and emotion regulation abilities, while for behaviorally-disordered children who tend to be more reactive to adverse environmental risk factors, individual differences in vagal functioning may have developed in response to the environment because of the need for increased attention to environmental risks and dangers (i.e., domestic violence). We also test the complementary idea that vagal response to interpersonal challenge signifies an internal, biological vulnerability for conduct-problems that is only manifest when domestic violence is a catalyst (e.g., Gottesman & Gould, 2003; Iacono, 1998). To test this hypothesis, we examine whether vagal augmentation is associated with a greater number of conduct-related problems for those children exposed to high levels of domestic violence.
Method
Participants
One hundred and thirty families with a pre-school aged child were recruited for participation in a study of children at risk for the development of conduct problems. Four to six year old children and their families were recruited through advertisements in pre-schools, newspapers, and doctors’ offices. Children were on average 60.5 months old (range = 49–71). Inclusion into the study was determined by scores on a telephone version of the Eyberg Child Behavior Inventory (ECBI; Robinson, Eyberg, & Ross, 1980). Following established cut-offs, children who received a score of 11 or higher on the ECBI were assigned to the conduct-problem group and children who received a score of 7 or lower were assigned to the control group. Sixty-five families had children who met criteria for the conduct problem group (41 male, 24 female), and 65 families had children who met criteria for the control group (40 males, 25 females). Groups were case-matched for age, socioeconomic status and neighborhood. With the exception of one child, groups were also case-matched for gender.
Mother’s report on the Child Behavior Checklist was also obtained (CBCL; Achenbach & Edelbrock, 1983). Mean T-scores on the Aggression subscale were 68 for the conduct-problem group and 53 for the control group. To determine the degree to which children were exhibiting symptoms consistent with a diagnosis of Oppositional Defiant Disorder or Conduct Disorder, mothers were also administered the Diagnostic Interview Schedule for Children (DISC 2.3; Shaffer et al, 1996). Mothers were administered the DISC by a bachelor’s level research assistant trained to reliability by a Ph.D. clinical psychologist who had previously been trained by the developers of the DISC. Two DISC administrators were trained and conducted all the DISC interviews during the initial home visit. The DISC administrator was not blind to the child’s score on the Eyberg. Approximately half the children in the conduct-problem group met criteria for Oppositional Defiant Disorder or Conduct Disorder. As expected for children within this age group, very few children met criteria for CD (N=5).
The predominant ethnic identification was Anglo-European (88.5%), and the remainder of the sample was Hispanic (6.2%), African American (3.8%), and Native American (1.5%). Sixty-two percent of the sample was male (N=81); 38% was female (N=49).
Procedures
Overview of physiological assessment
To obtain relatively artifact-free physiological data from preschool-aged children, we used an astronaut fantasy theme in which children were dressed in a space suit and seated in a mock-up space capsule during assessments of physiological functioning (Katz & Gottman, 1993, 1995). All procedures were administered in the space capsule, beginning with the baseline assessment. To assess vagal tone, the child’s cardiac interbeat interval (IBI) was assessed continuously by measuring the time between successive R-waves of the electrocardiogram (EKG). Physiological data was recorded continuously using a Coulbourn Instruments (Allentown, PA) system with a multipurpose high gain bioamplifier (S75-01), with the low pass filter set at 40 Hz and the high pass filter set at 0.1 Hz. Miniature Beckman silver-silver chloride electrodes were applied to either side of the child’s chest after lightly abrading the area with Omni-prep solution. Beckman electrolyte was used to facilitate conductivity of electrical signals. The physiological data were recorded using an analog-to-digital board (Metrabyte) and a custom program (ASYST) in a PC environment. IBI was averaged into 1-second intervals to allow synchronization with behavior for other analyses. The EKG waveform was digitized at a sampling rate of 128 Hz and stored using ASYST programs during the session. Subsequently, an ASYST data reduction program was used that read and displayed the EKG waveform data, detected and flagged R-spikes, and allowed manual verification of R-spike locations by the operator. This program produced the IBI series data file. The IBI series data file was then cleaned with another custom program which detected and split long IBI's which resulted from missed R-spikes.
Baseline Condition
Two assessments of baseline physiological functioning were obtained, once while children listened to a neutral story about a boy named Charlie (60 seconds) and then again while children viewed two scenes of children playing together (57 seconds).
Peer Provocation Paradigm
Dodge and Somberg’s interpersonal threat procedure was used as our peer provocation paradigm (Dodge & Somberg, 1987). Children viewed nine standardized videorecorded vignettes depicting paid actors involved in a play activity. Prior to the presentation of the vignettes, each child was exposed to a threat manipulation. The threat manipulation involved the child expecting to interact with a peer with whom he might get into a conflict. However, instead of meeting an unfamiliar peer, the target child heard a prerecorded audiotape consisting of a staged “conversation” between the experimenter and “another child” in which the child stated his dislike for the experimenter and for any child with whom he would have to work. After the “conversation,” the experimenter explained that the other child “was in a bad mood,” and would not be coming in to play. This audiotaped segment lasted for 67 seconds.
Measures
Conduct-problem behavior
The number of Oppositional Defiant Disorder and Conduct Disorder symptoms endorsed by mothers on the DISC was used as the continuous measure of conduct-problem behavior (DISC 2.3; Shaffer et al, 1996). The DISC 2.3 has good test-retest reliability (range = .77–.93) and adequate inter-rater agreement (range = .56–.68) for disruptive behavior disorder diagnoses (Schwab-Stone et al, 1996; Shaffer et al, 1996).
Child’s Vagal Tone
Vagal tone was computed as the amount of variance in the interbeat interval spectrum that was within the child's respiratory sinus frequency band using spectral time-series analysis. The exact width and anchors of the frequency band associated with respiratory sinus arrhythmia depends on the respiration rate. Children in this age group breathe at a rate of 20–25 times a minute (Vaughan & McKay, 1975), which corresponds to the frequency band of 0.33–0.42 Hz. The sum of the power densities in the IBI spectrum within the 0.33–0.42 Hz band over the total amount of power across all frequency bands was used as the measure of vagal tone. For our computations, we used the program SPEC from the Gottman-Williams computer program time-series package to conduct spectral analyses (Williams & Gottman, 1981). Vagal tone computed using the Gottman-Williams programs correlates very highly with vagal estimates obtained using MXEDIT (r=.96; Gottman, Katz & Hooven, 1997). This method of calculating children’s vagal tone has also been used in previous studies and has strong validity. It has been found to be related to observations of parenting behavior, parental approaches to emotion socialization, children’s emotion regulation abilities and child adjustment (e.g., Gottman, Katz & Hooven, 1997; Gottman & Katz, 2002).
Baseline vagal tone was obtained by averaging the child’s vagal tone while they listened to a story about Charlie and watched the scenes of children playing (r=.37, p<.0001 for vagal tone between these 2 baseline conditions). Children’s physiological reactivity to the peer provocation was assessed while the child was listening to the audiotape of the staged “conversation” between the experimenter and the “other child,” and during a subsequent period of 25 seconds. This additional 25-second period was included to increase the stability of the vagal tone estimate. There was also a substantial correlation between vagal tone during the staged conversation and during the subsequent 25 second period (r=.47, p<.0001). Following recommendations by Willett and colleagues (Willett, 2000; Willett & Keiley, 2000) and Rogosa (1995) regarding the merits of using difference scores, vagal reactivity to peer provocation was estimated as a difference between baseline vagal tone and the child’s vagal tone during the peer provocation. Some data loss occurred due to equipment failure, operator error, or poor quality physiological signals (N=6 for peer provocation; N=8 for baseline). There was also one instance in which procedures were stopped due to the child’s difficult behavior.
Self-Report of Domestic Violence
Parents individually completed the Conflict Tactics Scale (CTS; Straus, 1979) as a measure of the amount of physical aggression between spouses. The CTS is the most widely used measure of aggression between spouses. The subscales have adequate reliability, with alphas ranging from .50 to .76 for the Reasoning subscale, .79–.88 for the Verbal Aggression subscale, and .82 to .88 for the Physical Aggression subscale. In our analyses, we examined husband and wife report of their own aggressive acts over the past 12 months. Although the correlation between husband and wife report of DV was .54, p<.0001, each partner’s report of physical aggression was used because of consistent evidence of male underreporting of DV (Straus, 1990).
Items that measure physical aggression include: threw something that hit the other one; pushed, grabbed or shoved the other one; kicked, bit, or hit with a fist; and threatened partner with a knife or gun. As would be expected from a community-based sample, severity of violence was low. None of the families endorsed any of the more severe CTS items, such as beat up partner, threatened partner with a knife or gun, used a knife or gun. The majority of the incidents of DV endorsed involved pushing, grabbing, or shoving partner (14.6% and 11.5% of wives and husbands respectively); throwing something at partner (9.2% of wives); throwing something that hit partner (3.8% and 2.3% of wives and husbands respectively); and blocking partner from leaving the room (3.8% and 19.2% of wives and husbands respectively). Families varied widely in the frequency with which violent tactics were used during marital conflict. Using Straus’ data indicating that couples who report two or more violent incidents fall at the 90th percentile of a national sample (Straus, 1979), we found that 24% of our sample fell into the violent range. The number of violent acts endorsed by husbands and wives as occurring within the last 12 months ranged between 0 and “more than 20 times”.
Although physical violence was of low severity in our sample, this is very typical of community-based samples of domestic violence. For example, in their community-based sample, Straus and Gelles (1990) found that couples who report 1 instance of DV are in the 85th percentile of their distribution, suggesting that even 1 incident of physical aggression is at the extreme end of the distribution and is potentially harmful for children. They also found that of the women in their sample who experienced at least one instance of DV, 71% of women experienced minor assault (pushing, shoving, slapping, throwing things) and 29% experienced severe violence. Thus, what might be considered low severity violence is very common and may have quite significant effects on children.
Results
Descriptive Statistics
Means and standard deviations of independent and dependent variables are presented in Table 1. Correlations among study variables are presented in Table 2. Since conduct-problem behaviors tend to be more prevalent in boys than girls, one-way ANOVA’s were computed to determine whether there were gender differences in domestic violence or vagal tone variables. Because no gender differences emerged, gender was not considered in further analyses.
Table 1.
Descriptive statistics for study variables
| Variable | Mean | Standard Deviation |
|---|---|---|
| Baseline Vagal Tone | 11.67 | 7.55 |
| Vagal Tone to Peer Provocation | 12.03 | 9.52 |
| Change in Vagal Tone from Baseline to Peer Provocation | 1.27 | 9.94 |
| Husband Report of Marital Violence | .67 | 1.73 |
| Wife Report of Marital Violence | 1.02 | 2.32 |
Table 2.
Correlations between all study variables
| Variables | 1 | 2 | 3 | 4 | 5 | 6 |
|---|---|---|---|---|---|---|
| 1. Basal Vagal Tone | .28*** | −.39** | −.28** | −.12 | −.01 | |
| 2. Vagal reaction to challenge | .77*** | .10 | .01 | .02 | ||
| 3. Vagal change from baseline to challenge | .28* | .11 | .04 | |||
| 4. ODD symptoms | .34*** | |||||
| 5. Wife violence | .30*** | |||||
| 6. Husband violence | .54*** |
p < .01;
p < .001
Domestic Violence and Children’s Vagal Reactivity to Peer Provocation
Question 1: Is vagal augmentation more strongly associated with domestic violence for CP children than for controls ?
To test this hypothesis, two-way analyses of variance were conducted using vagal reactivity and group status as factors. Children were divided into two groups based on their vagal reactivity to peer provocation. One group consisted of children whose vagal tone increased from baseline to peer provocation and the second group consisted of children whose vagal tone either stayed the same or decreased from baseline to peer provocation. The group status variable was computed by dividing children into conduct-problem (CP) and control groups. Two ANOVA’s were conducted, one using husband and the other using wife’s report of marital violence as indices of physical marital aggression.
The pattern of findings is illustrated in Figure 1. Using husband’s report of his own marital violence, the main effect for group status was not significant and the main effect for vagal reactivity approached significance (F (1,113) =2.92, p=.09). However, the two-way interaction between vagal reactivity and group status was statistically significant (F (1,113) = 3.73, p<.05). LSD post-hoc analyses indicated that for the control group there were no differences in marital violence between those children who showed vagal increases to peer provocation and those children who showed either a decrease or no change in vagal reactivity (F (1,109) = .03, p=.88; M = .41 and .48 for control group children with vagal increase to peer provocation, and control group children with decrease or no change in vagal reactivity, respectively). In contrast, within the CP group, children who showed vagal increases to peer provocation came from families with higher levels of marital violence than CP children who showed either a decrease or no change in vagal reactivity (F(1,109) = 6.56, p<.01; M = 1.50 and .29 for CP children with vagal increase to peer provocation, and CP children with decrease or no change in vagal reactivity, respectively). Similarly, there were no differences in marital violence between CP and control children who showed either a decrease or no change in vagal reactivity (F(1,109) = .14, p = .71). However, for children who showed an increase in vagal reactivity to peer provocation, CP children came from homes with higher levels of marital violence than controls (F(1,109) = 6.27, p<.01). The number of children showing vagal augmentation and either no change or a vagal decrease to interpersonal challenge by risk status is displayed in Table 3.
Figure 1.
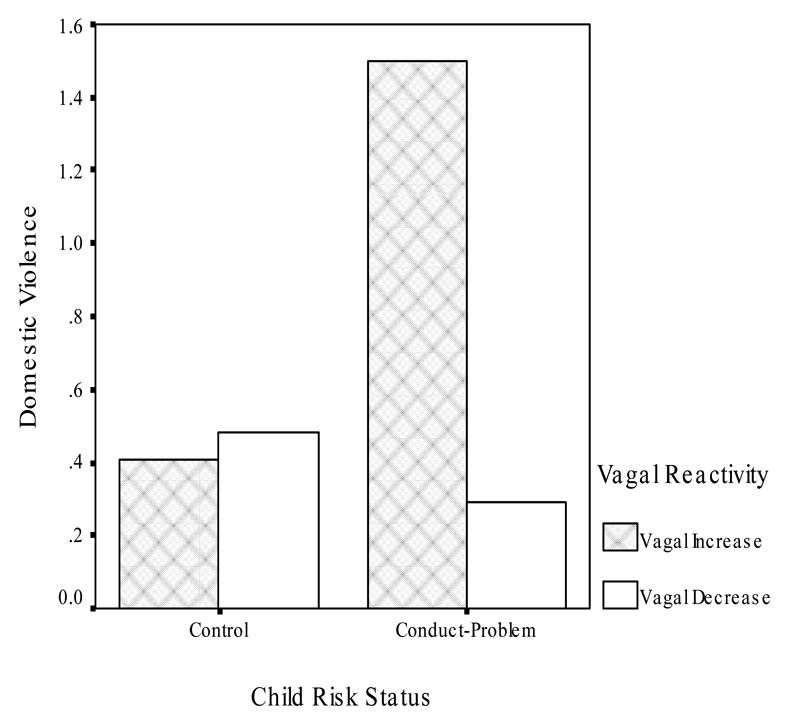
Relations between vagal reactivity and domestic violence as a function of child risk status.
Table 3.
Number of children by risk status showing vagal augmentation and no change/decrease in vagal tone to interpersonal challenge
| Control | Target | |
|---|---|---|
| Vagal Reactivity | ||
| No change or decrease in vagal tone | 26 | 25 |
| Vagal augmentation | 33 | 33 |
To better determine whether effects were due to reactivity to the stressor or to recovery from the stressor, follow-up analyses were conducted by separating out the period of time that children listened to the staged provocation from the 25 second recovery period. Because the recovery period only lasted 25 seconds, which is below the recommended 60 second minimum for computing a vagal response (Berntson et al, 1997), analyses were only conducted examining children’s vagal response to the staged provocation. Using husband’s report of his own marital violence, there were no main effects for group status (F(1,117)=2.12, p=.15) or vagal reactivity (F(1,117)=.01, p=.96) and the two-way interactions between vagal reactivity and group status was not significant (F (1,117) = .25, p=.62).
Using wife’s report of her own marital violence, there were no significant main effects or interactions.for either the combined reactivity and recovery variable or for the reactivity variable alone.
Question #2: Does children’s vagal response to interpersonal challenge signify a vulnerability for conduct-problems that is only manifest when domestic violence is a catalyst ?
To test this hypothesis, we examined whether vagal augmentation is associated with a greater number of conduct-related problems for those children exposed to high levels of domestic violence. Two-way analyses of variance were conducted using vagal reactivity and domestic violence as factors. Children were divided into two groups based on parental report of domestic violence. One group consisted of children whose parent reported at least one instance of physical aggression in the past year, and the second group consisted of children whose parent reported no instances of physical aggression in the past year. The number of ODD and CD symptoms endorsed by mothers on the DISC was used as the continuous measure of conduct-problem behavior. Two ANOVA’s were conducted, one using husband and the other using wife’s report of marital violence as indices of physical marital aggression.
Findings are displayed in Figure 2. Using husband’s report of his own marital violence, the main effect for vagal reactivity was significant (F(1,107)=3.83, p<.05) and the main effect for father violence approached significance (F (1,107) =3.65, p=.06). However, the two-way interaction between vagal reactivity and father violence was also statistically significant (F (1,107) = 6.57, p<.01). LSD post-hoc analyses indicated that for children with vagal augmentation to interpersonal challenge there was a significant difference in conduct-problem symptoms between those from homes in which father violence occurred and those from homes in which there was no father violence (F (1,103) = 9.41, p<.003; M = 3.38 and 1.50 for high and low violence, respectively). In contrast, for children with no change or a decrease in vagal tone to interpersonal challenge, there was no difference in conduct-problem symptoms between those from homes in which father violence occurred and those in which where was no father violence (F (1,103) = .81, p=.37; M = .50 and 1.23 for high and low violence, respectively). The number of children showing vagal augmentation and either no change or a vagal decrease to interpersonal challenge by father violence status is displayed in Table 4.
Figure 2.
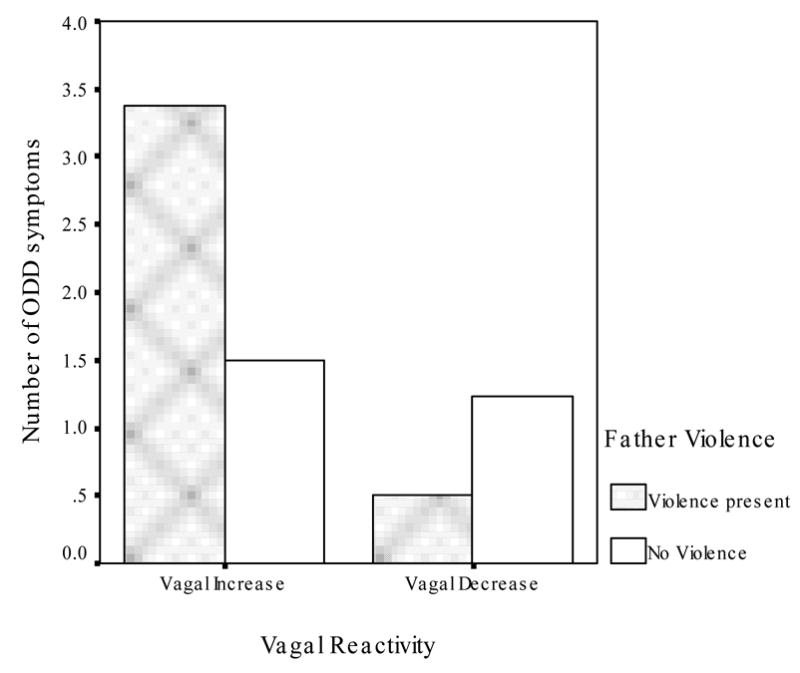
Relations between vagal reactivity and number of symptoms of Oppositional Defiant Disorder as a function of father violence.
Table 4.
Number of children by father violence status showing vagal augmentation and no change/decrease in vagal tone to interpersonal challenge
| No father violence | Presence of father violence | |
|---|---|---|
| Vagal Reactivity | ||
| No change or decrease in vagal tone | 40 | 9 |
| Vagal augmentation | 48 | 16 |
Using wife’s report of her own marital violence, the main effect for vagal reactivity (F(1,111)=3.82, p<.05) and the main effect for mother violence (F (1,111) =6.41, p<.01) were significant. However, the two-way interaction between vagal reactivity and mother violence was not significant (F (1,111) = .39, p=.53). Inspection of means indicated that children with vagal augmentation had more conduct-problem symptoms than children with no change or a decrease in vagal tone to challenge. Similarly, children from homes in which mothers endorsed perpetrating violence had more conduct-problem symptoms than children from homes in which no maternal violence was endorsed.
To determine whether effects were due to reactivity to the stressor or to recovery from the stressor, follow-up analyses were again using only the children’s vagal response during the staged provocation. Using husband’s report of his own marital violence, there was a main effect for violence (F(1,111)=4.27, p<.05) but no vagal reactivity (F(1,111)=1.50, p=.22) or interaction effects (F (1,111) = 1.19, p=.17). Using wife’s report of her own marital violence, there was again a main effect for violence (F(1,115)=6.19, p<.01) but no vagal reactivity (F(1,115)=.12, p=.73) or interaction effects (F (1,115) = .01, p=.95).
Discussion
The present findings indicate that conduct-problem children who increased their vagal tone to peer provocation came from families with the highest levels of domestic violence. Through repeated exposure to conflict that escalates out of control, these children may have learned to be hypervigilant to even subtle signs of interpersonal negativity, and their heightened vagal activity supports this increased attentiveness. Consistent with Porges’ (1995) description of the functioning of vagal efference to the heart, vagal augmentation occurred when the interpersonal negativity involved a threat to the self. Porges (1995) suggests that the “smart” vagus, which originates in the nucleus ambiguous, mediates cardiac activity when environmental demands require coping. To cope, we must either attend to and engage with the threat or respond with fight or flight. In our data, heightened vagal reactivity is consistent with active engagement with environmental demands that require sustained attention.
The observed increase in vagal tone to the peer provocation is also consistent with the physiological responses of Type 1 male batterers who increased their vagal tone when they are engaged in a conflictual marital interaction (Jacobson, Gottman & Shortt, 1995). Conduct-problem children who demonstrated the pattern of increased vagal reactivity to peer provocation came from families with the highest level of domestic violence. The peer provocation involved a threat in an interpersonal context that had personal relevance. Children were led to believe that they would soon be interacting with the provocative child, so that the child’s behavior had immediate implications for them personally. It may be that for conduct-problem children exposed to DV, the threat of interacting with a hostile child more closely resembles the types of threats these children experience in their home environment.
The vagal increase in response to peer provocation may be a unique adaptation for conduct-problem children exposed to DV. The high level of threat and sense of insecurity in maritally aggressive families (Cummings & Davies, 1994) may lead these children to develop an expectation that disagreement and anger are threatening and unpredictable. The sense of unpredictability sustained over long periods of time may generate a hypervigilance towards threat, leading children to scan the environment for cues of threat to monitor their own safety or prepare for danger by mobilizing aggressive coping strategies (Katz, 2001). The increase in vagal tone may support this heightened hypervigilance and motor readiness. Heightened vagal tone in response to threat may help with attention deployment and threat detection so the child is readily prepared for action.
Children with conduct problems may be particularly sensitized to violence because they may be more hypervigilant to interpersonal threat and negativity. This may be especially true for CP children with high vagal reactivity to interpersonal threat. According to social information processing models, CP children tend to see hostility around them even when social cues are ambiguous (Crick & Dodge, 1994), and our data raise the possibility that this may be especially true for CP children who are exposed to domestic violence. Thus, if the social environment is sufficiently threatening as in the case for CP children in DV homes, vagal augmentation may serve the goal of helping children monitor their environment for signals of social threat. For typically-developing children whose families are less likely to exhibit maladaptive and frightening interactive processes, vagal augmentation may reflect normal variation in attentional processes and emotion regulation, with their physiological reactivity being less tied to hostile interactions at home.
Vagal augmentation may also help explain why some children exposed to domestic violence are at increased risk for problems with aggression. Modeling theories suggest that the intergenerational transmission of violence occurs because children mimic their parent’s aggressive behavior (Kwong, Bartholomew, Henderson & Trinke, 2003). If conduct-problem children with vagal augmentation are hypervigilant during situations involving interpersonal challenge, they may show increased attention to the aggressive tactics employed by parents during marital conflict. This heightened attention may increase their encoding of aggressive behavior, and function as an important step towards their enactment of aggression and hostility towards others (Crick & Dodge, 1990).
It is interesting to note that vagal augmentation in conduct-problem children was associated with high levels of husband but not wife violence. Although it has been suggested that violence is bi-directional in community-based samples of DV (Johnson, 1995), it may be that male’s violence has stronger signal value to children than female violence. Since violence by men is likely to result in greater physical injury and damage than violence by women (Straus & Gelles, 1990), children may learn to monitor male violence more closely than female violence because it has greater safety implications both for their parents as well as for themselves.
These data are also consistent with emerging evidence on the influence of early adverse experiences on children’s selective attention to threat-related signals. Physically abused children take longer to disengage from angry facial expressions compared to non-physically abused children (Pollak & Tolley-Schell, in press), perceive angry faces as highly salient and more distinctive relative to other emotional faces (Pollak, Cicchetti, Hornung & Reed, 2000), display broader perceptual category boundaries for perceiving anger than nonabused children (Pollak & Kistler, 2002), and require less visual information to detect the presence of angry facial expressions than non-physically abused children (Pollak & Sinha, 2002). Physically abused children also display increases in P3b, a component of the event-related potential that is thought to reflect attentional resource allocation (Coles & Rugg, 1995; Kramer & Spinks, 1991). While nonmaltreated children respond uniformly when attending to happy, fearful and angry faces, physically abused children display increases in P3b amplitude only when searching for angry faces. Our data suggests that the threat of interacting with a difficult peer may trigger a similar attentional mechanism in conduct-problem children exposed to domestic violence. Future research should be directed at better understanding whether children exposed to domestic violence who are exhibiting behavior problems show a consistent pattern of increased attention to threat-related signals, and determining whether this increased deployment of attention is due to a rapid engagement of threatening information (Williams, Matthews & MacLeod, 1996) or difficulty disengaging from threatening information (Derryberry & Reed, 2002; Fox, Russo & Dutton, 2002).
Findings also support the notion that vagal augmentation to challenge represents a vulnerability for conduct-problems that is only manifest when domestic violence is a catalyst. For children with vagal augmentation to interpersonal challenge, children from homes in which fathers were violent had more conduct-problem symptoms than children from homes in which there was no father violence. These findings are consistent with the idea that vagal augmentation to challenge is an endophenotype (Gottesman & Gould, 2003; Gottesman & Shields, 1973) that requires environmental influence for expression. Evidence from behavioral genetic studies indicate both significant genetic and environmental influences on vagal tone (Sneider, Boomsma, van Doornen, & DeGeus,1997; Kupper, Willemsen, Posthuma, deBoer, Boomsma & DeGeus, 2005). Since some children who are exposed to domestic violence develop into adult batterers (Hotaling & Sugarman, 1986), children’s vagal reactivity to stressful interpersonal interaction may reflect a genetic predisposition that sets children at risk for violent behavior. In combination with environmental processes such as parental modeling of interpersonal aggression or child emotion dysregulation consequent to violence exposure, this vulnerability is more likely to be expressed as conduct-problem behavior. This combination of internal physiological and external environmental events may also set the stage for the intergenerational transmission of violence. Clearly, our study cannot tease apart genetic from environmental influences. Longitudinal research on the heritability of vagal tone combined with careful analysis of family process is needed to further understand the degree to which vagal augmentation to interpersonal challenge reflects genetic and/or environmental effects.
Efforts were made to tease apart whether vagal effects were due to reactivity to or recovery from a stressor. These findings suggest that children’s recovery from the stressor rather than their initial reactivity was an important component underlying observed effects. However, because the recovery period lasted below the minimum 30 second period recommended for computing a vagal response, we were only able to examine children’s vagal response to the staged provocation and not directly assess vagal response to the recovery period itself in relation to domestic violence. As a result, it is unclear whether effects of domestic violence were observed because combining reactivity and recovery period resulted in a longer time period that added to the stability of the data, or whether children’s vagal response during recovery from the stressor is the essential component of the parasympathetic nervous system response related to domestic violence. Further research directly assessing both children’s initial vagal reaction to interpersonal challenge and their recovery from challenge will be important in understanding the specific components of the vagal response that is related to domestic violence.
Limitations to the current study must be addressed, however. Sample characteristics present limitations to the data since findings were based on a sample of families screened for conduct-problems rather than domestic violence. Although 24% of the sample experienced two or more instances of violence in the past year, the severity of the violence was low. Parents endorsed pushing, grabbing, shoving, kicking and hitting their partner, but there were no instances of more severe violence, such as threatening the partner with a knife or gun. The limited range in severity may have reduced effect sizes, and it is unclear whether these results would apply equally to children who live in homes exhibiting more severe types of domestic violence (Babcock, Yerington, Green, Costa & Miller, 2001). Replication using domestically violent samples that vary in severity and frequency of violence is needed to better understand whether children in these homes exhibit vagal reactivity to stressful interpersonal interactions, and to determine whether there are other familial characteristics that mediate this relationship.
Another limitation of the current study is that violence was determined based on husband and wife’s report of their own violence. Because marital conflict and violence can occur behind closed doors, we do not know whether variability in the extent to which the child witnessed the violence plays a role in observed effects. While this may be difficult to assess in children as young as those tested in the current study, future research with older children should examine whether vagal reactivity differs as a function of child exposure to domestic violence.
The current study provides initial support for the notion that vagal reactivity in behaviorally-disordered children may be associated with negative interpersonal processes in the family environment. Domestic violence appears to be one such negative life circumstance. Continued investigation of interactions between the interpersonal environment and children’s biological functioning is likely to reveal many other ways in which each child’s unique set of biological reactions and adaptations interact with and are impacted by their social world.
Footnotes
This research was supported by a research grant from the National Institute of Mental Health to the author (1 R01 MH49141). The authors thank the families and peers involved in this research for their participation.
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Achenbach TM, Edelbrock CS. Manual for the Child Behavior Checklist and Revised Child Behavior Profile. Burlington: University of Vermont Department of Psychiatry; 1983. [Google Scholar]
- Babcock JC, Yerington T, Green C, Costa D, Miller S. Psychophysiological profiles of batterers: The relationship between heart rate reactivity, psychopathy and domestic violence; Poster presented at the 41st annual meeting of the Society for Psychophysiological Research; October; Montreal. 2001. [Google Scholar]
- Burman B, John RS, Margolin GG. Observed patterns of conflict in violent, nonviolent, and nondistressed couples. Behavioral Assessment. 1992;14:15–37. [Google Scholar]
- Calkins SD. Cardiac vagal tone indices of temperamental reactivity and behavioral regulation in young children. Developmental Psychobiology. 1997;31:125–135. doi: 10.1002/(sici)1098-2302(199709)31:2<125::aid-dev5>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Dedmon SE. Physiological and behavioral regulation in two-year-old children with aggressive/destructive behavior problems. Journal of Abnormal Child Psychology. 2000;28:103–118. doi: 10.1023/a:1005112912906. [DOI] [PubMed] [Google Scholar]
- Christopolous C, Cohn DA, Shaw DS, Joyce S, Sullivan-Hanson J, Draft SP, Emery RE. Children of abused women: adjustment at time of shelter residence. Journal of Marriage and the Family. 1987;49:611–619. [Google Scholar]
- Coan J, Gottman JM, Babcock J, Jacobson N. Battering and the male rejection of influence from women. Aggressive Behavior. 1997;23:375–388. [Google Scholar]
- Coles MG, Rugg MD. Event-related brain potentials: An introduction. In: Coles MG, Rugg MD, editors. Electrophysiology of mind: Event-related brain potentials and cognition. New York, NY: Oxford University Press; 1995. pp. 1–26. Oxford psychology series, No. 25. [Google Scholar]
- Crick NR, Dodge KA. A review and reformulation of social information-processing mechanisms in children’s social adjustment. Psychological Bulletin. 1994;115:74–101. [Google Scholar]
- Cummings EM, Davies D. Children and Marital Conflict: The Impact of Family Dispute and Resolution. New York, NY: Guilford; 1994. [Google Scholar]
- DeGangi GA, DiPietro JA, Greeenspan SI, Porges SW. Psychophysiological characteristics of the regulatory disordered infant. Infant Behavior and Development. 1991;14:37–50. [Google Scholar]
- Derryberry D, Reed MA. Anxiety-related attentional biases and their regulation by attentional control. Journal of Abnormal Psychology. 2002;111:225–236. doi: 10.1037//0021-843x.111.2.225. [DOI] [PubMed] [Google Scholar]
- Derryberry D, Rothbart MK. Emotion, attention and temperament. In: Izard CE, Kagan J, Zajonc RB, editors. Emotions, cognitions and behavior. New York, N.Y: Cambridge University Press; 1988. pp. 132–166. [Google Scholar]
- DiPietro JA, Porges SW, Uhly B. Reactivity and developmental competence in preterm and full-term infants. Developmental Psychology. 1992;28:831–841. [Google Scholar]
- Dodge KA, McClaskey CL, Feldman E. Situational approach to the assessment of social competence in children. Journal of Consulting and Clinical Psychology. 1985;53:344–353. doi: 10.1037//0022-006x.53.3.344. [DOI] [PubMed] [Google Scholar]
- Dodge KA, Somberg DR. Hostile attributional biases among aggressive boys are exacerbated under conditions of threats to the self. Child Development. 1987;58:213–224. doi: 10.1111/j.1467-8624.1987.tb03501.x. [DOI] [PubMed] [Google Scholar]
- El-Shiekh M, Harger J, Whitson SM. Exposure to interparental conflict and children's adjustment and physical health: The moderating role of vagal tone. Child Development. 2001;72(6):1617–1636. doi: 10.1111/1467-8624.00369. [DOI] [PubMed] [Google Scholar]
- Eyberg S, Colvin A. Restandardization of the Eyberg Child Behavior Inventory; Poster presented at the annual meeting of the American Psychological Association.Aug, 1994. [Google Scholar]
- Fantuzzo JW, DePaola LM, Lambert L, Martino T, Anderson G, Sutton S. Effects of interparental violence on the psychological adjustment and competencies of young children. Journal of Consulting and Clinical Psychology. 1991;59:258–265. doi: 10.1037//0022-006x.59.2.258. [DOI] [PubMed] [Google Scholar]
- Fox E, Russo R, Dutton K. Attentional bias for threat: Evidence for delayed disengagement from emotional faces. Cognition and Emotion. 2002;16:355–379. doi: 10.1080/02699930143000527. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gottesman II, Gould TD. The endophenotype concept in psychiatry: Etymology and strategic intentions. American Journal of Psychiatry. 2003;160:636–645. doi: 10.1176/appi.ajp.160.4.636. [DOI] [PubMed] [Google Scholar]
- Gottman JG, Jacobson NS, Rushe RH, Shortt JW, Babcock J, LaTaillade JJ, Waltz J. The relationship between heart rate reactivity, emotionally aggressive behavior, and general violence in batterers. Journal of Family Psychology. 1995;9:227–248. [Google Scholar]
- Gottman JM, Katz LF, Hooven C. Meta-emotion: How families communicate emotionally. Hillsdale, N.J: Lawrence Erlbaum; 1997. [Google Scholar]
- Gottman JM, Parker JG, editors. Conversations of Friends: Speculations on Affective Development. Cambridge, England: Cambridge University Press; 1986. [Google Scholar]
- Graham-Bermann SA. Designing intervention evaluations for children exposed to domestic violence: Applications of research and theory. In: Graham-Bermann SA, Edleson JL, editors. Domestic violence in the lives of children: The future of research, intervention and social policy. American Psychological Association; Washington, D.C: 2001. pp. 237–267. [Google Scholar]
- Graham Bermann SA, Levendosky AA. Traumatic stress symptoms in children of battered women. Journal of Interpersonal Violence. 1998;13:111–128. [Google Scholar]
- Holden GW, Ritchie KL. Linking extreme marital discord, child rearing, and child behavior problems: Evidence from battered women. Child Development. 1991;62:311–327. doi: 10.1111/j.1467-8624.1991.tb01533.x. [DOI] [PubMed] [Google Scholar]
- Hotaling GT, Sugarman DB. An analysis of risk markers in husband to wife violence: The current state of knowledge. Violence and Victims. 1986;1:101–124. [PubMed] [Google Scholar]
- Hughes HM. Psychological and behavioral correlates of family violence in child witnesses and victims. American Journal of Orthopsychiatry. 1988;58:77–90. doi: 10.1111/j.1939-0025.1988.tb01568.x. [DOI] [PubMed] [Google Scholar]
- Jacobson NS, Gottman JM, Shortt JW. The distinction between type 1 and type 2 batterers. Journal of Family Psychology. 1995;9:272–279. – further considerations: Reply to Ornduff et al (1995), Margolin et al (1995), and Walker (1995) [Google Scholar]
- Jacobson NS, Gottman JM, Watlz J, Rushe R, Babcock &, Holtzworth Munroe. Affect, verbal content, and psychophysiology in the arguments of couples with a violent husband. Journal of Consulting and Clinical Psychology. 1994;62:982–988. doi: 10.1037//0022-006x.62.5.982. [DOI] [PubMed] [Google Scholar]
- Jaffe P, Wolfe DA, Wilson S, Zak L. Emotional and physical health problems of battered women. Canadian Journal of Psychiatry. 1986;31:625–629. doi: 10.1177/070674378603100705. [DOI] [PubMed] [Google Scholar]
- Johnson MP. Patriarchal Terrorism and Common Couple Violence: Tow Forms of Violence Against Women. Journal of Marriage and the Family. 1995;57:283–294. [Google Scholar]
- Jouriles EN, Norwood WD. Physical aggression toward boys and girls in families characterized by the battering of women. Journal of Family Psychology. 1995;9:69–78. [Google Scholar]
- Jouriles EN, Norwood WD, McDonald R, Peters B. Domestic violence and child adjustment. In: Grych JH, Fincham FD, editors. Interparental conflict and child development: Theory, research, and applications. New York, NY: Cambridge University Press; 2001. pp. 315–336. [Google Scholar]
- Katz LF. Living in a hostile world: Toward an integrated model of family, peer and physiological processes in aggressive preschoolers. In: Kerns KA, Contreras J, Neal-Barnett AM, editors. Linking two social worlds: Family and peers. Sage Publications Inc; 2001. [Google Scholar]
- Katz LF, Gottman JM. Patterns of marital conflict predict children’s internalizing and externalizing behaviors. Developmental Psychology. 1993;29(6):940–950. [Google Scholar]
- Katz LF, Gottman JM. Vagal tone protects children from marital conflict. Development and Psychopathology. 1995;7:83–92. [Google Scholar]
- Kramer A, Spinks J. Capacity views of human information processing. In: Jennings RJ, Coles MG, editors. Handbook of cognitive psychophysiology: Central and autonomic nervous system approaches. New York: N.Y.: 1991. pp. 179–249. [Google Scholar]
- Kwong M, Bartholomew K, Henderson A, Trinke S. The intergenerational tranmission of relationship violence. Journal of Family Psychology. 2003;17:288–301. doi: 10.1037/0893-3200.17.3.288. [DOI] [PubMed] [Google Scholar]
- Lee MY. Marital violence: impact on children’s emotional experiences, emotional regulation and behaviors in a post-divorce/separation situation. Child and Adolescent Social Work Journal. 2001;18:137–163. [Google Scholar]
- Margolin G, John RS, Ghosh CM, Gordis EB. Family interaction process: An essential tool for exploring abusive relations. In: Cahn DD, Lloyd SA, editors. Family violence from a communication perspective. Thousand Oaks, CA: Sage Publications, Inc; 1996. pp. 37–58. [Google Scholar]
- Margolin G, John RS, Gleberman L. Affective responses to conflictual discussions in violent and nonviolent couples. Journal of Consulting and Clinical Psychology. 1988;56:24–33. doi: 10.1037//0022-006x.56.1.24. [DOI] [PubMed] [Google Scholar]
- Mash EJ, Barkley RA. Child psychopathology. New York, N.Y: Guilford Press; 2003. [Google Scholar]
- Miller GM, Chapman JP. Misunderstanding analysis of covariance. Journal of Abnormal Psychology. 2001;110:40–48. doi: 10.1037//0021-843x.110.1.40. [DOI] [PubMed] [Google Scholar]
- O’Keefe M. Racial/ethnic differences among battered women and their children. Journal of Child and Family Studies. 1994;3:283–305. [Google Scholar]
- O’Keefe M. Adjustment of children from maritally violent homes. Families in Society. 1995;75:403–415. [Google Scholar]
- O’Keefe M. Predictors of child abuse in maritally violent families. Journal of Interpersonal Violence. 1995;10:3–25. [Google Scholar]
- Pollak SD, Cicchetti D, Hornung K, Reed A. Recognizing emotion in faces: Developmental effects of child abuse and neglect. Developmental Psychology. 2000;36 (5):679–688. doi: 10.1037/0012-1649.36.5.679. [DOI] [PubMed] [Google Scholar]
- Pollak SD, Kistler D. Early experience alters categorical representations for facial expressions of emotion. Proceedings of the National Academy of Sciences. 2002;99:9072–9076. doi: 10.1073/pnas.142165999. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pollak SD, Sinha P. Effects of early experience on children’s recognition of facial displays of emotion. Developmental Psychology. doi: 10.1037//0012-1649.38.5.784. in press. [DOI] [PubMed] [Google Scholar]
- Pollak SD, Tolley-Schell SA. Selective attention to facial emotion in physically abused children. Journal of Abnormal Psychology. doi: 10.1037/0021-843x.112.3.323. in press. [DOI] [PubMed] [Google Scholar]
- Porges SW. Orienting in a defensive world: Mammalian modifications of our evolutionary heritage: A Polyvagal Theory. Psychophysiology. 1995;32:301–318. doi: 10.1111/j.1469-8986.1995.tb01213.x. [DOI] [PubMed] [Google Scholar]
- Porges SW, Doussard-Roosevelt JA, Portales AL, Greenspan SI. Infant regulation of the vagal “brake” predicts child behavior problems: A psychobiological model of social behavior. Developmental Psychobiology. 1996;29:697–712. doi: 10.1002/(SICI)1098-2302(199612)29:8<697::AID-DEV5>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- Robinson EA, Eyreeberg SM, Ross AW. The standardization of an inventory of child conduct problem behaviors. Journal of Clinical Child Psychology. 1980;9:22–28. [Google Scholar]
- Rogosa D. Myths and methods: “Myths about longitudinal research” plus supplemental questions. In: Gottman JM, editor. The analysis of change. Mahwah, N.J.: Lawrence Erlbaum Press; 1995. pp. 3–66. [Google Scholar]
- Spaccarelli S, Sandler IN, Roosa M. History of spouse violence against mother: Correlated risks and unique effects in child mental health. Journal of Family Violence. 1994;9:79–98. [Google Scholar]
- Sternberg KH, Lamb ME, Greenbaum, Cicchetti Dawud, Coretes Krispin, O’Leary Effects of domestic violence on children’s behavior on children’s behavior problems and depression. Developmental Psychology. 1993;29:44–52. [Google Scholar]
- Straus MA. Measuring intrafamily conflict and violence: The Conflict Tactics (CT) Scales. Journal of Marriage and the Family. 1979;41:75–88. [Google Scholar]
- Straus MA, Gelles RJ. Physical violence in american families. New Brunswick, N.J: Transaction Publishers; 1990. [Google Scholar]
- Strauss CC, Lahey BB, Frick P, Frame CL, Hynd P. Peer social status of children with anxiety disorders. Journal of Consulting and Clinical Psychology. 1988;56:137–141. doi: 10.1037//0022-006x.56.1.137. [DOI] [PubMed] [Google Scholar]
- Suess PA, Porges SW, Plude DJ. Cardiac vagal tone and sustained attention in school-age children. Psychophysiology. 1994;31:17–22. doi: 10.1111/j.1469-8986.1994.tb01020.x. [DOI] [PubMed] [Google Scholar]
- Vaughn VC, McKay RJ, editors. Nelson textbook of pediatrics. 10. Philadelphia: Saunders; 1975. [Google Scholar]
- Ware HS, Jouriles EN, Spiller LC, McDonald R, Swank PR, Norwood WD. Conduct problems among children at battered women’s shelters: Prevalence and stability of maternal reports. Journal of Family Violence. 2001;16:291–307. [Google Scholar]
- Willett JB, Keiley MK. Using covariance structure analysis to model change over time. In: Tinsley HEA, Brown SD, editors. Handbook of applied multivariate statistics and mathematical modeling. San Diego, CA: Academic Press; 2000. pp. 665–694. [Google Scholar]
- Willett JB. Measuring change: What individual growth modeling buys you. In: Amsel E, Renninger KA, editors. Change and development: Issues of theory, method and application. 2000. pp. 213–243. The Jean Piaget symposium series. [Google Scholar]
- Williams E, Gottman JM. A user’s guide to the Gottman-Williams time-series programs. New York: Cambridge University Press; 1981. [Google Scholar]
- Williams JMG, Matthews A, MacLeod C. The emotion stroop task and psychopathology. Psychological Bulletin. 1996;120 (1):3–24. doi: 10.1037/0033-2909.120.1.3. [DOI] [PubMed] [Google Scholar]
- Wilson BJ, Gottman JM. Attention – the shuttle between emotion and cognition: Risk, resiliency and physiological bases. In: Hetherington EM, Blechman EA, editors. Stress, coping and resiliency in children and families. Hillsdale, N.J: Lawrence Erlbaum Associates; 1996. pp. 189–228. [Google Scholar]
- Wolfe DA, Korsch B. Witnessing domestic violence during childhood and adolescence. Pediatrics. 1994;94:594–599. [PubMed] [Google Scholar]
- Wolfe DA, Jaffe P, Wilson SK, Zak L. Children of battered women: The relation of child behavior to family violence and maternal stress. Journal of Consulting and Clinical Psychology. 1985;53:657–665. doi: 10.1037//0022-006x.53.5.657. [DOI] [PubMed] [Google Scholar]