

Abstract
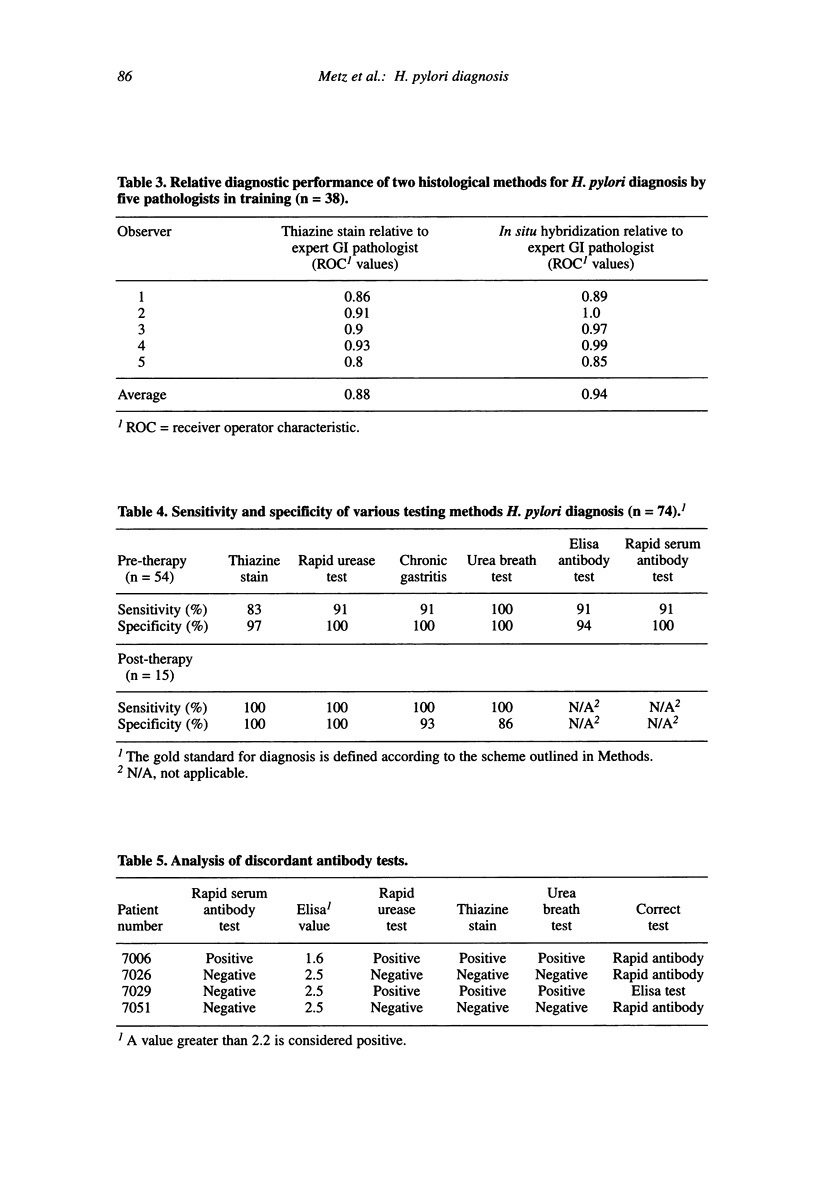
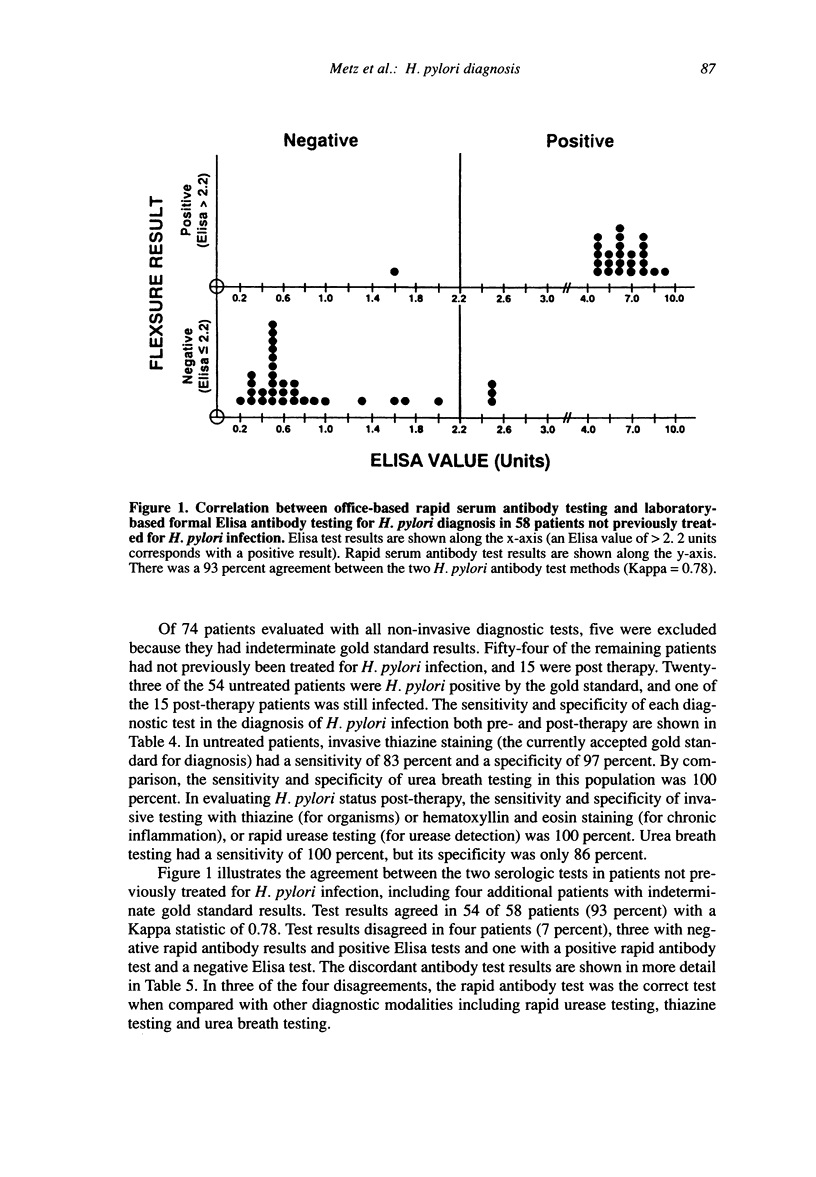
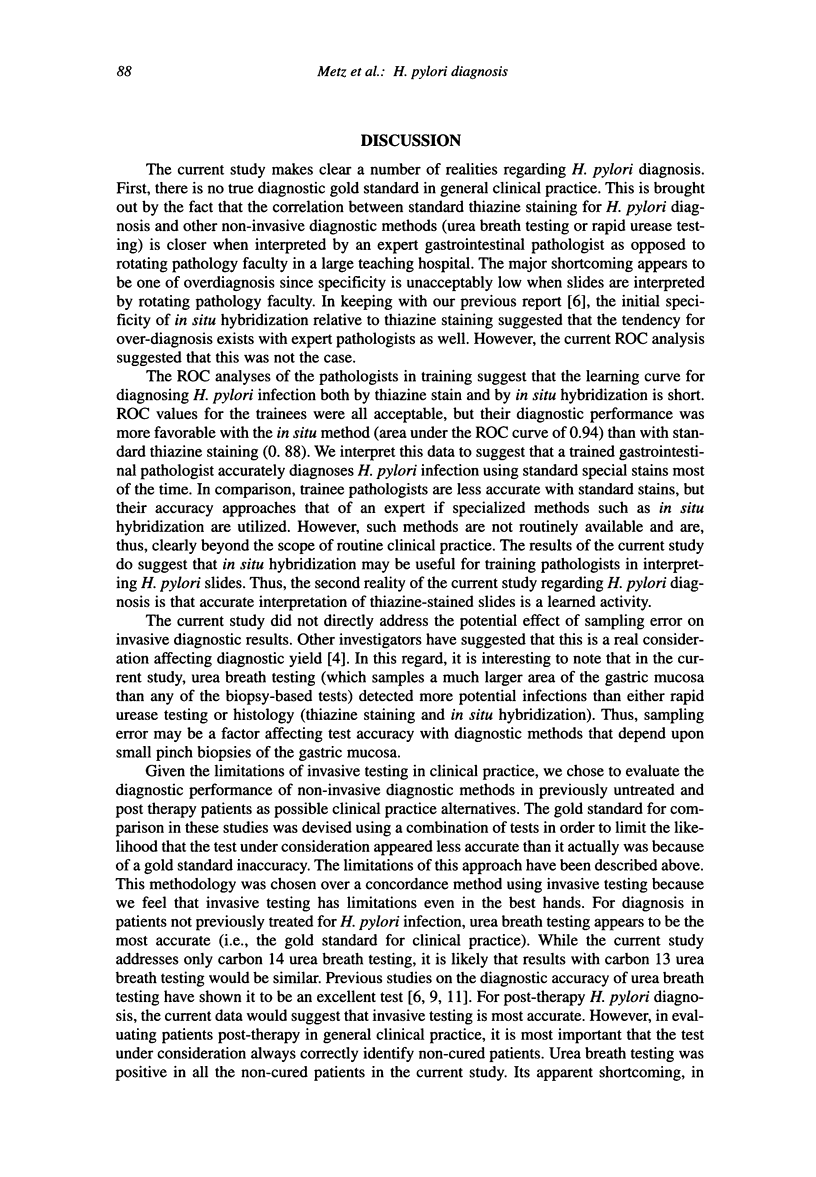
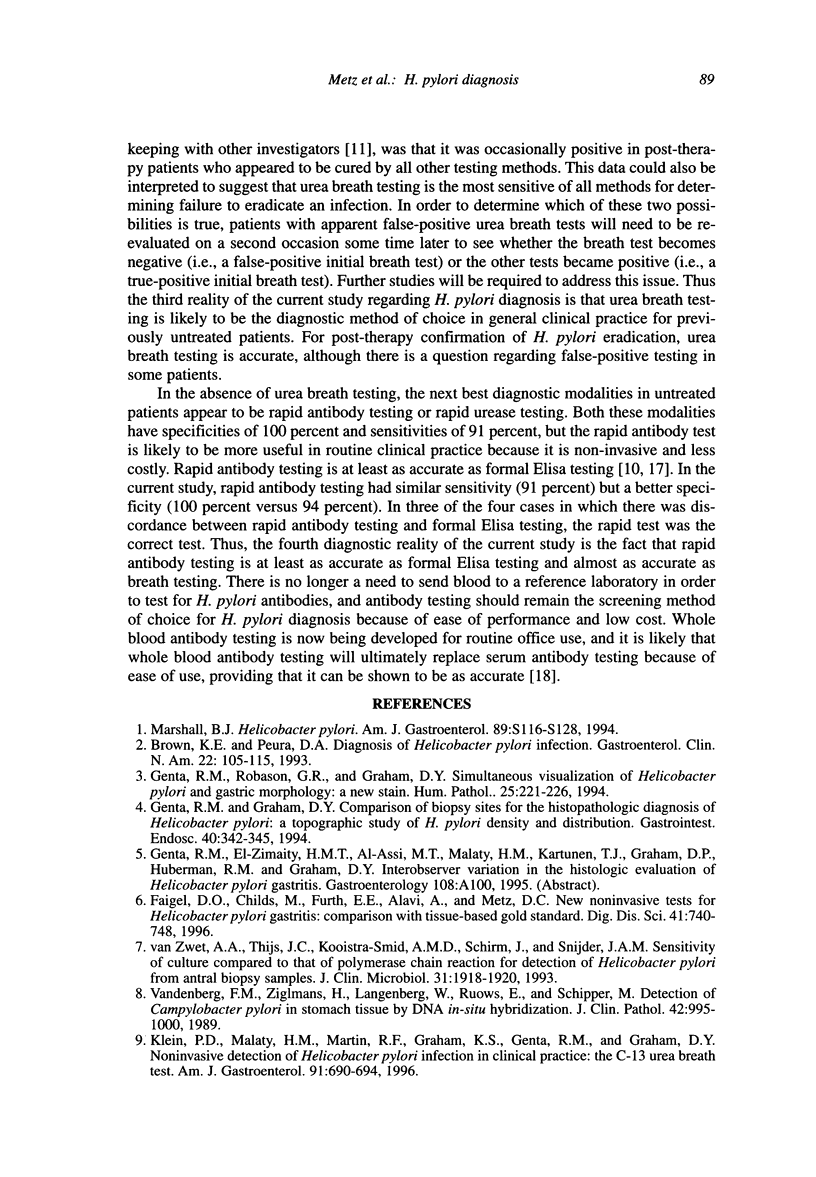
BACKGROUND: The current, arbitrarily defined gold standard for the diagnosis of H. pylori infection requires histologic examination of two specially stained antral biopsy specimens. However, routine histology is potentially limited in general clinical practice by both sampling and observer error. The current study was designed to examine the diagnostic performance of invasive and non-invasive H. pylori detection methods that would likely be available in general clinical practice. METHODS: The diagnostic performance of rotating clinical pathology faculty using thiazine staining was compared with that of an expert gastrointestinal pathologist in 38 patients. In situ hybridization stains of adjacent biopsy cuts were also examined by the expert pathologist for further comparison. Receiver operator characteristic (ROC) analysis was performed to evaluate whether the diagnostic performance of the expert pathologist differed depending upon the histologic method employed. A similar analysis was made to evaluate the diagnostic performance of pathology trainees relative to the expert. In the absence of an established invasive gold standard, non-invasive testing methods (rapid serum antibodies, formal Elisa antibodies and carbon-14 urea breath testing) were evaluated in 74 patients by comparison with a gold standard defined using a combination of diagnostic tests. RESULTS: Using either rapid urease testing of biopsy specimens or urea breath testing as the gold standard for comparison, the diagnostic performance of the rotating clinical pathology faculty was inferior to that of the expert gastrointestinal pathologist especially with regard to specificity (e.g., 69 percent for the former versus 88 percent, with the latter relative to rapid urease testing). Although interpretation of in situ hybridization staining by the expert appeared to have an even higher specificity, ROC analysis failed to show a difference. The mean ROC areas for thiazine and in situ hybridization staining for trainee pathologists relative to the expert were 0.88 and 0.94, respectively. In untreated patients, urea breath testing had a sensitivity and specificity of 100 percent as compared with thiazine staining with a sensitivity of 83 percent and a specificity of 97 percent. Post-therapy, breath testing had a sensitivity of 100 percent but a specificity of only 86 percent as compared with invasive testing with a sensitivity and specificity of 100 percent. Rapid serum antibody testing and formal Elisa antibody testing agreed in 93 percent of cases (Kappa 0.78) with the rapid test being correct in three of the four disagreements. CONCLUSIONS: The current study illustrates a number of realities regarding H. pylori diagnosis. There is no diagnostic gold standard in general clinical practice. Accurate interpretation of specially stained slides is a learned activity with a tendency towards overdiagnosis early on. Urea breath testing is likely to be the diagnostic method of choice for untreated patients in general clinical practice although antibody testing is almost as accurate. Rapid antibody tests are at least as accurate as formal Elisa antibody tests. Urea breath testing is useful for confirming cure after therapy, but false-positive results may occur in some patients.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Brown K. E., Peura D. A. Diagnosis of Helicobacter pylori infection. Gastroenterol Clin North Am. 1993 Mar;22(1):105–115. [PubMed] [Google Scholar]
- Cutler A. F., Havstad S., Ma C. K., Blaser M. J., Perez-Perez G. I., Schubert T. T. Accuracy of invasive and noninvasive tests to diagnose Helicobacter pylori infection. Gastroenterology. 1995 Jul;109(1):136–141. doi: 10.1016/0016-5085(95)90278-3. [DOI] [PubMed] [Google Scholar]
- Faigel D. O., Childs M., Furth E. E., Alavi A., Metz D. C. New noninvasive tests for Helicobacter pylori gastritis. Comparison with tissue-based gold standard. Dig Dis Sci. 1996 Apr;41(4):740–748. doi: 10.1007/BF02213130. [DOI] [PubMed] [Google Scholar]
- Faigel D. O., Furth E. E., Childs M., Goin J., Metz D. C. Histological predictors of active Helicobacter pylori infection. Dig Dis Sci. 1996 May;41(5):937–943. doi: 10.1007/BF02091534. [DOI] [PubMed] [Google Scholar]
- Genta R. M., Graham D. Y. Comparison of biopsy sites for the histopathologic diagnosis of Helicobacter pylori: a topographic study of H. pylori density and distribution. Gastrointest Endosc. 1994 May-Jun;40(3):342–345. doi: 10.1016/s0016-5107(94)70067-2. [DOI] [PubMed] [Google Scholar]
- Genta R. M., Robason G. O., Graham D. Y. Simultaneous visualization of Helicobacter pylori and gastric morphology: a new stain. Hum Pathol. 1994 Mar;25(3):221–226. doi: 10.1016/0046-8177(94)90191-0. [DOI] [PubMed] [Google Scholar]
- Graham D. Y., Evans D. J., Jr, Peacock J., Baker J. T., Schrier W. H. Comparison of rapid serological tests (FlexSure HP and QuickVue) with conventional ELISA for detection of Helicobacter pylori infection. Am J Gastroenterol. 1996 May;91(5):942–948. [PubMed] [Google Scholar]
- Klein P. D., Malaty H. M., Martin R. F., Graham K. S., Genta R. M., Graham D. Y. Noninvasive detection of Helicobacter pylori infection in clinical practice: the 13C urea breath test. Am J Gastroenterol. 1996 Apr;91(4):690–694. [PubMed] [Google Scholar]
- Metz C. E. Basic principles of ROC analysis. Semin Nucl Med. 1978 Oct;8(4):283–298. doi: 10.1016/s0001-2998(78)80014-2. [DOI] [PubMed] [Google Scholar]
- Van den Berg F. M., Zijlmans H., Langenberg W., Rauws E., Schipper M. Detection of Campylobacter pylori in stomach tissue by DNA in situ hybridisation. J Clin Pathol. 1989 Sep;42(9):995–1000. doi: 10.1136/jcp.42.9.995. [DOI] [PMC free article] [PubMed] [Google Scholar]
- van Zwet A. A., Thijs J. C., Kooistra-Smid A. M., Schirm J., Snijder J. A. Sensitivity of culture compared with that of polymerase chain reaction for detection of Helicobacter pylori from antral biopsy samples. J Clin Microbiol. 1993 Jul;31(7):1918–1920. doi: 10.1128/jcm.31.7.1918-1920.1993. [DOI] [PMC free article] [PubMed] [Google Scholar]