

Abstract
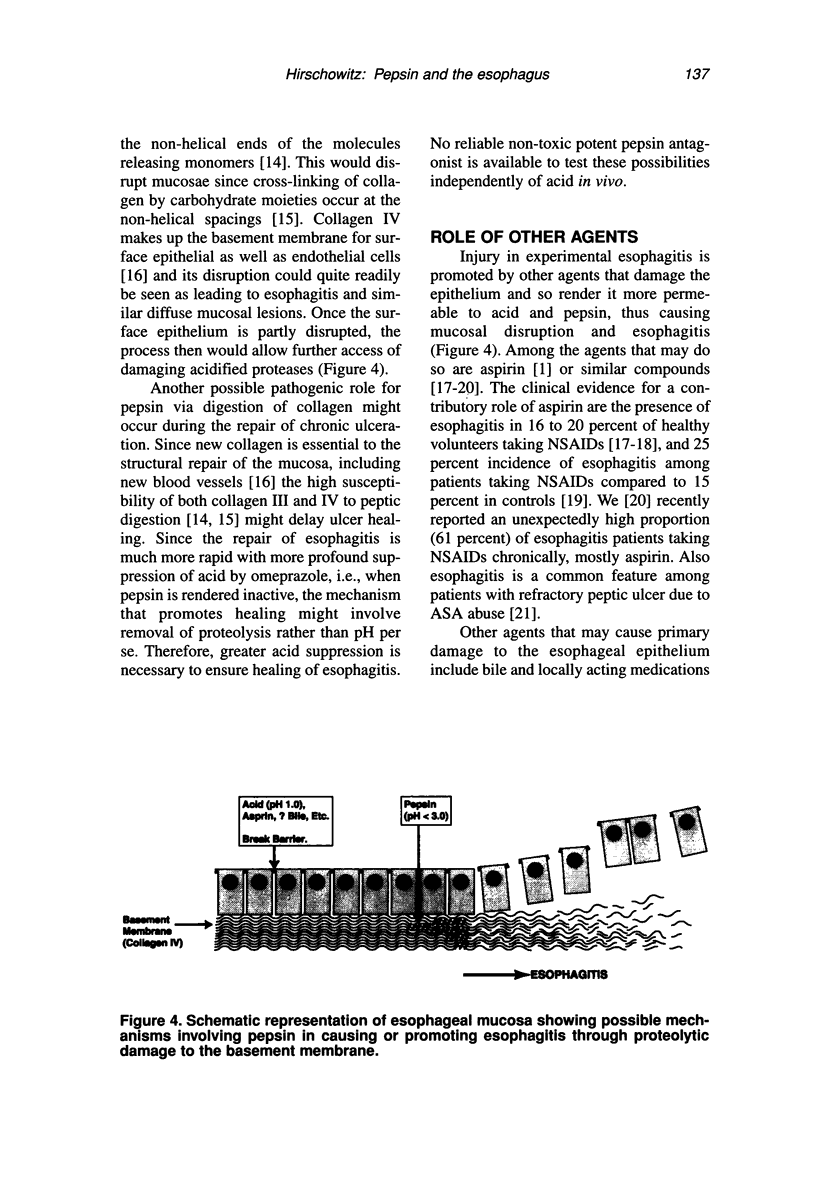
Esophagitis results from excessive exposure of the esophagus to gastric juice through an ineffective or dysfunctional lower esophageal sphincter mechanism. A possible role of pepsin in damaging the esophageal mucosa with consequent esophagitis may be examined directly by testing pepsin under various conditions in experimental models of esophagitis. Since gastric juice contains both acid and pepsin, all experiments examine separately effects of perfusion of the esophagus by acid without and with pepsin in various combinations. Acid perfusion alone at concentrations represented by pH 1.3 or above does not produce esophagitis. The addition of pepsin to acid between pH 1 and 3.5 causes considerable acute esophageal damage. Outside the proteolytic range, i.e., higher than pH 3.5, pepsin does not damage the esophagus. The damage caused by acidified pepsin may be made much worse by the further addition of aspirin or other NSAIDs, presumably by further breaking down mucosal barriers.
Full text
PDF
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Bell N. J., Burget D., Howden C. W., Wilkinson J., Hunt R. H. Appropriate acid suppression for the management of gastro-oesophageal reflux disease. Digestion. 1992;51 (Suppl 1):59–67. doi: 10.1159/000200917. [DOI] [PubMed] [Google Scholar]
- Burget D. W., Chiverton S. G., Hunt R. H. Is there an optimal degree of acid suppression for healing of duodenal ulcers? A model of the relationship between ulcer healing and acid suppression. Gastroenterology. 1990 Aug;99(2):345–351. doi: 10.1016/0016-5085(90)91015-x. [DOI] [PubMed] [Google Scholar]
- Dent J., Yeomans N. D., Mackinnon M., Reed W., Narielvala F. M., Hetzel D. J., Solcia E., Shearman D. J. Omeprazole v ranitidine for prevention of relapse in reflux oesophagitis. A controlled double blind trial of their efficacy and safety. Gut. 1994 May;35(5):590–598. doi: 10.1136/gut.35.5.590. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dölz R., Engel J., Kühn K. Folding of collagen IV. Eur J Biochem. 1988 Dec 15;178(2):357–366. doi: 10.1111/j.1432-1033.1988.tb14458.x. [DOI] [PubMed] [Google Scholar]
- Ford T. F., Grant D. A., Austen B. M., Hermon-Taylor J. Intramucosal activation of pepsinogens in the pathogenesis of acute gastric erosions and their prevention by the potent semisynthetic amphipathic inhibitor pepstatinyl-glycyl-lysyl-lysine. Clin Chim Acta. 1985 Jan 15;145(1):37–47. doi: 10.1016/0009-8981(85)90017-8. [DOI] [PubMed] [Google Scholar]
- Goldberg H. I., Dodds W. J., Gee S., Montgomery C., Zboralske F. F. Role of acid and pepsin in acute experimental esophagitis. Gastroenterology. 1969 Feb;56(2):223–230. [PubMed] [Google Scholar]
- Hallerbäck B., Unge P., Carling L., Edwin B., Glise H., Havu N., Lyrenäs E., Lundberg K. Omeprazole or ranitidine in long-term treatment of reflux esophagitis. The Scandinavian Clinics for United Research Group. Gastroenterology. 1994 Nov;107(5):1305–1311. doi: 10.1016/0016-5085(94)90531-2. [DOI] [PubMed] [Google Scholar]
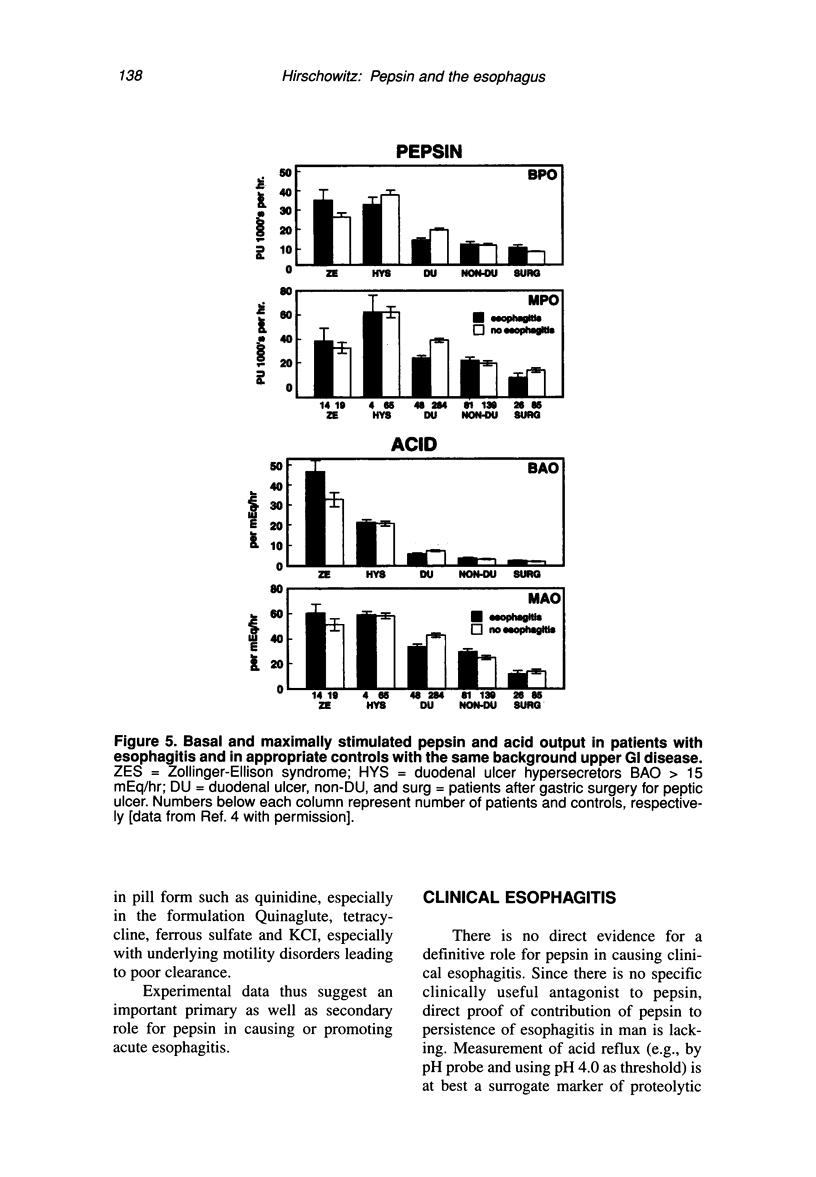
- Hirschowitz B. I. A critical analysis, with appropriate controls, of gastric acid and pepsin secretion in clinical esophagitis. Gastroenterology. 1991 Nov;101(5):1149–1158. doi: 10.1016/0016-5085(91)90062-p. [DOI] [PubMed] [Google Scholar]
- Hirschowitz B. I. Acid and pepsin secretion in patients with esophagitis refractory to treatment with H2 antagonists. Scand J Gastroenterol. 1992 Jun;27(6):449–452. doi: 10.3109/00365529209000104. [DOI] [PubMed] [Google Scholar]
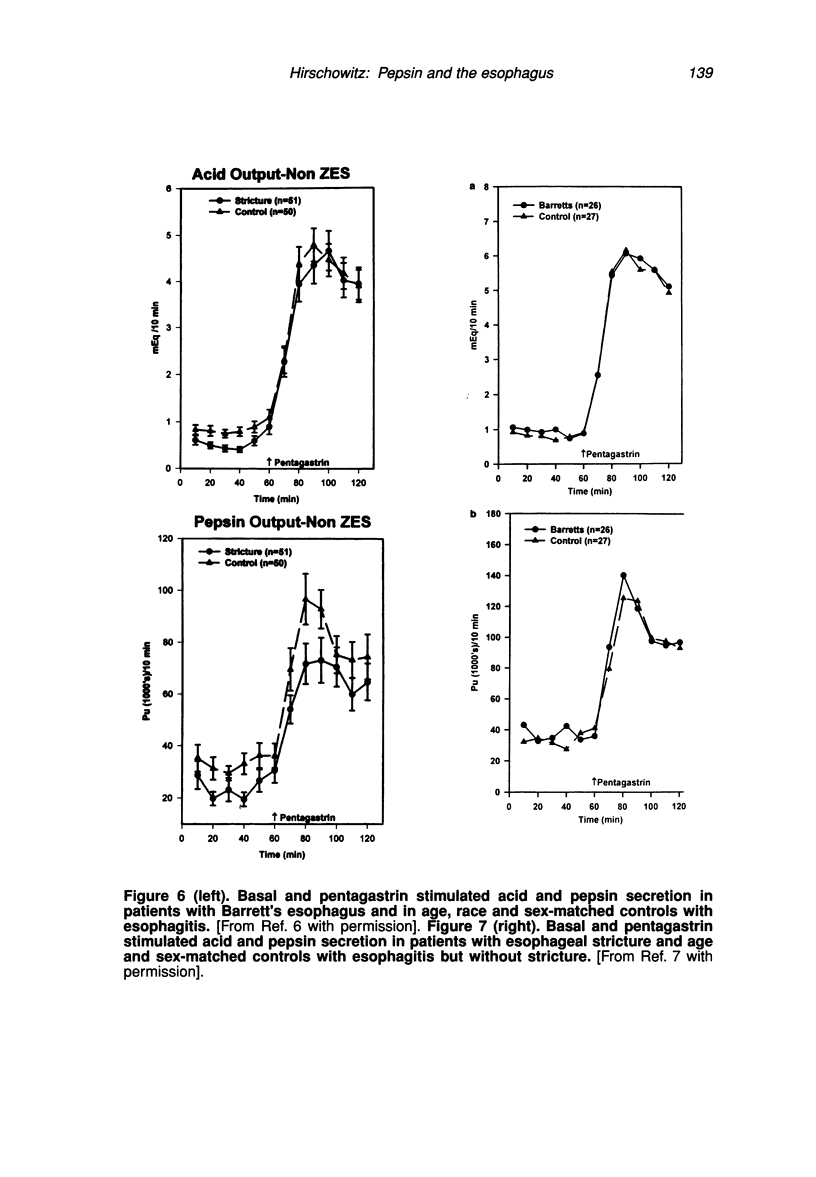
- Hirschowitz B. I. Gastric acid and pepsin secretion in patients with Barrett's esophagus and appropriate controls. Dig Dis Sci. 1996 Jul;41(7):1384–1391. doi: 10.1007/BF02088563. [DOI] [PubMed] [Google Scholar]
- Hirschowitz B. I. Gastric secretion of acid and pepsin in patients with esophageal stricture and appropriate controls. Dig Dis Sci. 1996 Nov;41(11):2115–2122. doi: 10.1007/BF02071389. [DOI] [PubMed] [Google Scholar]
- Hirschowitz B. I., Lanas A. NSAID association with gastrointestinal bleeding and peptic ulcer. Agents Actions Suppl. 1991;35:93–101. [PubMed] [Google Scholar]
- Hirschowitz B. I. Medical management of esophageal reflux. Yale J Biol Med. 1994 May-Aug;67(3-4):223–231. [PMC free article] [PubMed] [Google Scholar]
- Ingber D. E., Folkman J. How does extracellular matrix control capillary morphogenesis? Cell. 1989 Sep 8;58(5):803–805. doi: 10.1016/0092-8674(89)90928-8. [DOI] [PubMed] [Google Scholar]
- Klinkenberg-Knol E. C., Festen H. P., Jansen J. B., Lamers C. B., Nelis F., Snel P., Lückers A., Dekkers C. P., Havu N., Meuwissen S. G. Long-term treatment with omeprazole for refractory reflux esophagitis: efficacy and safety. Ann Intern Med. 1994 Aug 1;121(3):161–167. doi: 10.7326/0003-4819-121-3-199408010-00001. [DOI] [PubMed] [Google Scholar]
- Klinkenberg-Knol E. C., Jansen J. B., Lamers C. B., Nelis F., Snel P., Meuwissen S. G. Use of omeprazole in the management of reflux oesophagitis resistant to H2-receptor antagonists. Scand J Gastroenterol Suppl. 1989;166:88–94. doi: 10.3109/00365528909091251. [DOI] [PubMed] [Google Scholar]
- Klinkenberg-Knol E. C., Meuwissen S. G. Combined gastric and oesophageal 24-hour pH monitoring and oesophageal manometry in patients with reflux disease, resistant to treatment with omeprazole. Aliment Pharmacol Ther. 1990 Oct;4(5):485–495. doi: 10.1111/j.1365-2036.1990.tb00495.x. [DOI] [PubMed] [Google Scholar]
- Kresina T. F., Miller E. J. Isolation and characterization of basement membrane collagen from human placental tissue. Evidence for the presence of two genetically distinct collagen chains. Biochemistry. 1979 Jul 10;18(14):3089–3097. doi: 10.1021/bi00581a028. [DOI] [PubMed] [Google Scholar]
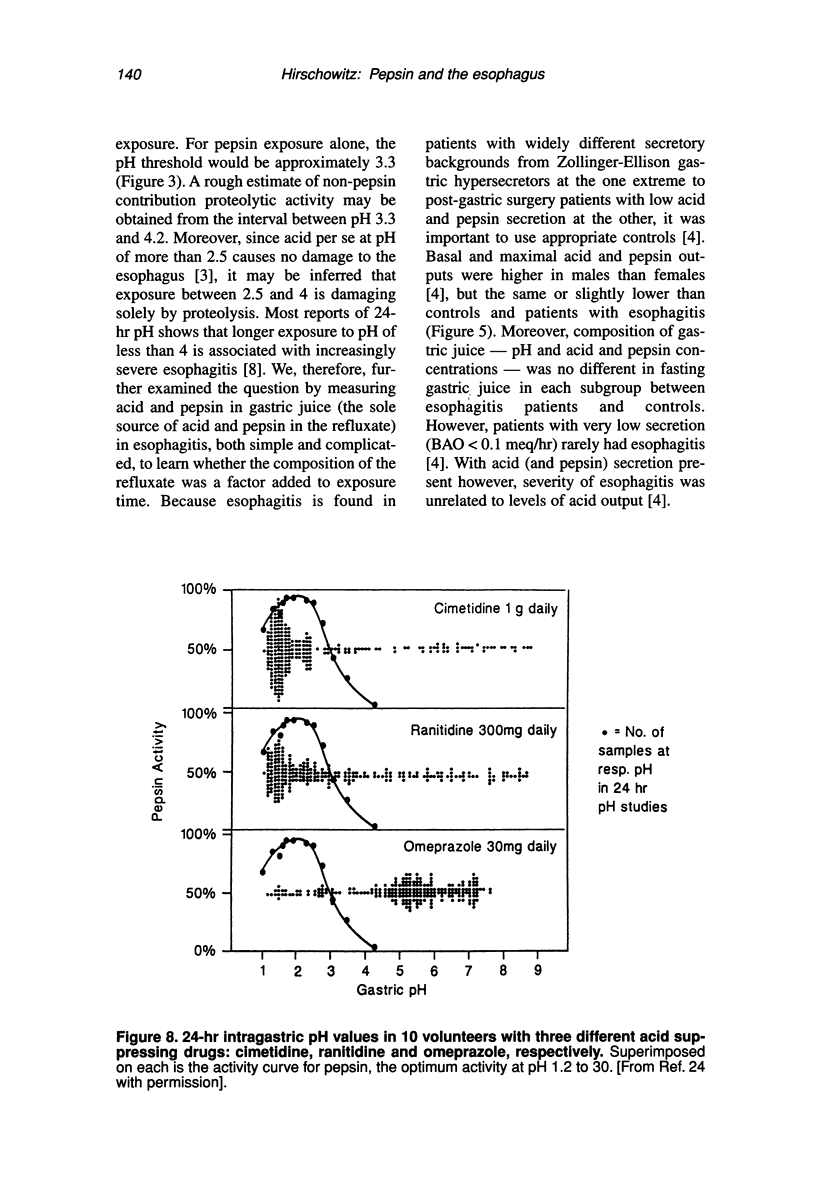
- Lanas A. I., Blas J. M., Ortego J., Soria J., Sáinz R. Adaptation of esophageal mucosa to acid- and pepsin-induced damage: role of nitric oxide and epidermal growth factor. Dig Dis Sci. 1997 May;42(5):1003–1012. doi: 10.1023/a:1018837003196. [DOI] [PubMed] [Google Scholar]
- Lanas A. I., Sousa F. L., Ortego J., Esteva F., Blas J. M., Soria J., Sáinz R. Aspirin renders the oesophageal mucosa more permeable to acid and pepsin. Eur J Gastroenterol Hepatol. 1995 Nov;7(11):1065–1072. doi: 10.1097/00042737-199511000-00009. [DOI] [PubMed] [Google Scholar]
- Lanas A., Hirschowitz B. I. Significant role of aspirin use in patients with esophagitis. J Clin Gastroenterol. 1991 Dec;13(6):622–627. doi: 10.1097/00004836-199112000-00005. [DOI] [PubMed] [Google Scholar]
- Layden T. J., Agnone L. M., Schmidt L. N., Hakim B., Goldstein J. L. Rabbit esophageal cells possess an Na+,H+ antiport. Gastroenterology. 1990 Oct;99(4):909–917. doi: 10.1016/0016-5085(90)90606-2. [DOI] [PubMed] [Google Scholar]
- Lundell L., Backman L., Ekström P., Enander L. H., Fausa O., Lind T., Lönroth H., Sandmark S., Sandzén B., Unge P. Omeprazole or high-dose ranitidine in the treatment of patients with reflux oesophagitis not responding to 'standard doses' of H2-receptor antagonists. Aliment Pharmacol Ther. 1990 Apr;4(2):145–155. doi: 10.1111/j.1365-2036.1990.tb00459.x. [DOI] [PubMed] [Google Scholar]
- Ohe K., Ueno N., Yokoya H., Miyoshi A. The activation of pepsinogen inside the gastric mucosa caused by the hydrogen ion back diffusion during the course of aspirin ulceration. Hiroshima J Med Sci. 1979 Mar;28(1):1–11. [PubMed] [Google Scholar]
- Orlando R. C. Esophageal epithelial defense against acid injury. J Clin Gastroenterol. 1991;13 (Suppl 2):S1–S5. [PubMed] [Google Scholar]
- Roland M., Berstad A., Liavåg I. Effect of carbacholine and urecholine on pentagastrin-stimulated gastric secretion in healthy subjects. Scand J Gastroenterol. 1975;10(4):357–362. [PubMed] [Google Scholar]
- Santucci L., Patoia L., Fiorucci S., Farroni F., Favero D., Morelli A. Oesophageal lesions during treatment with piroxicam. BMJ. 1990 Apr 14;300(6730):1018–1018. doi: 10.1136/bmj.300.6730.1018-b. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Semble E. L., Wu W. C., Castell D. O. Nonsteroidal antiinflammatory drugs and esophageal injury. Semin Arthritis Rheum. 1989 Oct;19(2):99–109. doi: 10.1016/0049-0172(89)90054-1. [DOI] [PubMed] [Google Scholar]
- Sontag S. J., Hirschowitz B. I., Holt S., Robinson M. G., Behar J., Berenson M. M., McCullough A., Ippoliti A. F., Richter J. E., Ahtaridis G. Two doses of omeprazole versus placebo in symptomatic erosive esophagitis: the U.S. Multicenter Study. Gastroenterology. 1992 Jan;102(1):109–118. doi: 10.1016/0016-5085(92)91790-b. [DOI] [PubMed] [Google Scholar]
- Sontag S. J., Robinson M., Roufail W., Hirschowitz B. I., Sabesin S. M., Wu W. C., Behar J., Peterson W. L., Kranz K. R., Tarnawski A. Daily omeprazole surpasses intermittent dosing in preventing relapse of oesophagitis: a US multi-centre double-blind study. Aliment Pharmacol Ther. 1997 Apr;11(2):373–380. doi: 10.1046/j.1365-2036.1997.141317000.x. [DOI] [PubMed] [Google Scholar]
- Taha A. S., Dahill S., Nakshabendi I., Lee F. D., Sturrock R. D., Russell R. I. Oesophageal histology in long term users of non-steroidal anti-inflammatory drugs. J Clin Pathol. 1994 Aug;47(8):705–708. doi: 10.1136/jcp.47.8.705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Walt R. P., Gomes M. D., Wood E. C., Logan L. H., Pounder R. E. Effect of daily oral omeprazole on 24 hour intragastric acidity. Br Med J (Clin Res Ed) 1983 Jul 2;287(6384):12–14. doi: 10.1136/bmj.287.6384.12. [DOI] [PMC free article] [PubMed] [Google Scholar]