

Abstract
Fatigue is the most commonly encountered symptom in patients with liver disease, and it has a significant impact on their quality of life. However, although some progress has been made with regard to the understanding of the processes which may generate fatigue in general, the underlying cause(s) of liver disease-associated fatigue remain incompletely understood. The present review describes recent advances which have been made in our ability to measure fatigue in patients with liver disease in the clinical setting, as well as in our understanding of potential pathways which are likely important in the pathogenesis of fatigue associated with liver disease. Specifically, experimental findings suggest that fatigue associated with liver disease likely occurs as a result of changes in neurotransmission within the brain. In conclusion, a reasonable approach to help guide in the management of the fatigued patient with liver disease is presented.
Keywords: Cholestasis, Fatigue, Hepatitis, Liver disease, Neurotransmitters, Therapy
Abstract
La fatigue est le principal symptôme chez les patients atteints d’une maladie hépatique, et elle a des conséquences considérables sur leur qualité de vie. Cependant, même si certains progrès ont été réalisés quant à notre compréhension des processus généraux susceptibles de produire de la fatigue, les causes sousjacentes de la fatigue associée à la maladie hépatique sont mal comprises. La présente analyse décrit les progrès récents accomplis dans notre capacité de mesurer la fatigue chez les patients atteints d’une maladie hépatique en milieu clinique, ainsi que dans notre compréhension des voies potentielles qui, selon toute probabilité, jouent un rôle important dans la pathogenèse de la fatigue associée à la maladie hépatique. Plus précisément, les observations expérimentales laissent supposer que la fatigue associée aux maladies hépatiques découle de modifications à la neurotransmission dans le cerveau. En conclusion, une démarche raisonnable pour orienter la prise en charge du patient atteint d’une maladie hépatique et de fatigue est présentée.
Fatigue is a complex symptom that encompasses a range of complaints including lethargy, malaise, lassitude and exhaustion. Chronic fatigue commonly occurs, affecting up to 20% of the population (1). Although the exact prevalence of fatigue in patients with chronic liver disease is somewhat variable in different studies and with different specific liver diseases, it is readily apparent that fatigue constitutes the most common complaint among this patient group (2–6). However, because of difficulties in defining and treating fatigue, this symptom is often overlooked or minimized by physicians caring for patients with liver disease. The prevalence of fatigue in patients with different forms of liver disease also appears to be quite variable. Specifically, cholestatic liver disease caused by primary biliary cirrhosis (PBC), primary sclerosing cholangitis or drugs is commonly associated with fatigue (2,3). In fact, fatigue in cholestatic patients can be the presenting symptom and occurs in 65% to 85% of patients (2,3,7,8). Moreover, fatigue in PBC is considered to be the worst symptom in approximately 50% of patients, and is disabling in approximately 25% (7). Fatigue also has a significant impact on the health-related quality of life (HRQOL) of PBC patients (7–9).
The prevalence of fatigue in hepatitic liver diseases is less clearly defined. Fatigue is an integral component of the clinical presentation of patients with autoimmune hepatitis, often paralleling hepatic inflammation as determined by serum alanine aminotransferase measurements or liver biopsy findings, and responding usually quite rapidly to the institution of immunosuppressive therapy (4,10,11). However, the overall prevalence of fatigue in patients with viral hepatitis is less clear. Acute presentations of viral hepatitis are often associated with feelings of fatigue or malaise, which gradually subside because the patient recovers clinically (eg, recovers from hepatitis A). However, the situation in patients with chronic viral hepatitis appears to be more controversial. Specifically, a significant proportion of patients with chronic hepatitis C who are followed in tertiary care centres, or who participate in clinical trials, complain of fatigue or decreased vitality, which has a direct negative impact on their HRQOL (5,6,12). However, this high prevalence of fatigue does not appear to hold for patients infected with hepatitis C who are unaware of their diagnosis (13,14). Moreover, the complaint of fatigue in hepatitis C patients does not appear to correlate with whether these patients are viremic (15). In contrast, patients chronically infected with hepatitis B appear to have HRQOL scores similar to those of healthy controls (12).
Recently, patients with hepatitis C have been reported to have subclinical findings of cognitive impairment and altered cerebral metabolism as reflected by magnetic resonance spectroscopy (16–18). The suggestion from these findings is that hepatitis C infection of the brain itself may lead to these changes (17,19). However, it is unclear whether these central changes observed in hepatitis C-infected patients are a direct result of the hepatitis C virus within the brain, are related to the complex behavioural, social and mental sequelae associated with carrying a diagnosis of chronic hepatitis C infection or are related to the mode of acquisition of their hepatitis C (eg, intravenous drug abuse).
Therefore, any discussion of the pathophysiology and management of fatigue in the context of liver disease must take these observations into account.
TYPES OF FATIGUE
In any discussion of fatigue, it is imperative to differentiate central from peripheral fatigue. Peripheral fatigue relates to neuromuscular dysfunction and occurs with muscle overutilization and associated metabolic changes, and is classically manifested clinically by weakness (20,21). This type of fatigue does not appear to be important in patients with liver disease in the absence of decompensated cirrhosis or liver failure. In contrast, central fatigue arises within the central nervous system (CNS) and is characterized by a difficulty in performing physical (and often mental) activities, which require self-motivation and responses to internal cues. Furthermore, central fatigue is often associated with a higher perceived effort when undertaking tasks (20). Therefore, by definition, central fatigue directly results from altered neurotransmission within the brain.
Typically, the complaint of central fatigue in the setting of any chronic disease, including liver diseases, does not correlate with traditional markers of disease activity or severity (20,21). Moreover, central fatigue is often associated with other neuropsychiatric complaints also thought to be secondary to altered neurotransmission within the CNS; namely depression and anxiety (20,21). This association of fatigue with depression and anxiety is commonly encountered in patients with cholestatic and hepatitic liver diseases (6–8,22).
Given that central fatigue arises from changes in neuro-transmitter systems within the brain, it is readily apparent that objective measurements of fatigue are problematic. Therefore, fatigue assessments in patients with liver disease have traditionally been performed using either general or specifically designed questionnaires (eg, Short Form-36 [12,15] versus Fatigue Impact Scale [23] or Fatigue Severity Scale [24]). By scoring a patient’s answers to a given set of questions concerning fatigue, these questionnaires allow for an objective quantification or score of fatigue to be made. Changes in these scores have been used to determine worsening or improving in fatigue with therapeutic interventions in patients with liver disease.
PATHOPHYSIOLOGY OF FATIGUE IN LIVER DISEASE
The pathogenesis of fatigue in general is poorly understood and this holds true for fatigue in the setting of liver disease (20,21,25). However, given that altered neurotransmission within the CNS drives central fatigue, and that central fatigue is the predominant issue in the setting of liver disease, any discussion of the possible etiology of fatigue in the context of liver disease must relate to these potential changes in neurotransmission within the brain (21,25,26). Therefore, the discussion of the pathophysiology of fatigue in liver disease must incorporate two main concepts:
How does the diseased or damaged liver ‘communicate’ with the brain to cause changes in neurotransmission?
What specific changes in neurotransmission occur within the brain as a result of this ‘communication’, and how do these changes give rise to the genesis of central fatigue?
Moreover, this discussion must also be placed in the context that fatigue in patients with liver disease is manifest in the setting of a diagnosis often holding an uncertain outcome and often associated with societal taboos. Therefore, the diagnosis of chronic liver disease encompasses complex interactions among biological, psychosocial and behavioural processes, which can all significantly affect the clinical expression of fatigue in a given patient.
As outlined previously, the ultimate cause of central fatigue in patients with liver disease must entail alterations in neurotransmitter pathways within the brain. The specific neurotransmitter pathways that have received the greatest clinical and experimental attention as potentially causing central fatigue include pathways that are important in behavioural activation, arousal and locomotor activity (25–28). Brain areas important in this regard include the basal ganglia, brainstem, reticular and limbic systems and higher cortical centres (20,25,26). The neurotransmitter systems that have been directly implicated in the genesis of central fatigue include the corticotropin-releasing hormone (CRH), serotonin, noradrenaline and other neurotransmitter systems.
CRH
CRH was initially identified as the factor released from the hypothalamus, which is the most potent activator of the hypothalamic-pituitary-adrenal axis. However, over the past three decades, it has become increasingly clear that CRH-containing nerve fibres are widely distributed throughout the CNS and are intimately involved in arousal and behavioural activation (27,29–31; Figure 1). These observations have led to the hypothesis that defective release of CRH within the brain may be important in the development of central fatigue (31–33). In an animal model of cholestatic liver disease, behaviours and physiological responses consistent with defective central CRH release have been documented (34–36). In addition, rats with experimental cholestasis demonstrate reduced hypothalamic CRH levels and increased CRH type 1 receptor expression, as well as enhanced sensitivity to the behavioural activating effects of centrally infused CRH (36); these findings are consistent with defective central CRH release playing an important role in cholestasis-associated fatigue. Moreover, clinical observations in patients with PBC also support this suggestion. Specifically, PBC patients demonstrate augmented adrenocorticotropic hormone release after intravenous CRH infusion, consistent with an upregulation of pituitary CRH receptors in these patients, possibly secondary to defective endogenenous CRH stimulation of their anterior pituitary glands (37). Of interest, defective central CRH release has also been implicated in central fatigue in patients with atypical depression and the chronic fatigue syndrome (26,32).
Figure 1.

Corticotropin-releasing hormone (CRH) acts in its traditional role to stimulate adrenocorticotropic hormone (ACTH) release from the anterior pituitary gland. However, CRH release from nerve fibres projecting to areas within the brain stimulates behavioural activation and arousal
Serotonin
Abnormal serotonergic neurotransmission has been commonly implicated in the development of altered behaviours including depression, anxiety and central fatigue (28). Serotonergic nerve fibres arise mainly within the dorsal raphe nucleus in the midbrain and project widely throughout the CNS (28,38,39). Of interest, the serotonin and CRH neurotransmitter systems are known to be intimately interrelated (38,40). Serotonin mediates its biological effects by activating a large number of receptor subtypes (41). However, the precise role played by serotonin in the generation of central fatigue remains unclear. It appears that serotonin released within the brain has a differential effect on the development of fatigue depending on whether exercise-induced fatigue or more classically defined central fatigue is being examined. Specifically, in rodents or athletes exercised to exhaustion, increased central serotonin levels appear to decrease exercise capacity (42,43). These observations suggest that increased central serotonin levels may contribute to central fatigue. However, the applicability of findings regarding serotonin in the setting of exercise to exhaustion appears to be less relevant to fatigue in the setting of liver disease. Patients with chronic fatigue syndrome exhibit findings on pharmacological challenge that are consistent with increased central serotonin sensitivity due to decreased serotonin release (44). These observations provided the impetus to use serotonin reuptake inhibitors to treat patients with chronic fatigue syndrome, albeit with mixed results (45).
The serotonin neurotransmitter system has been studied in an animal model of cholestatic liver disease and the findings are consistent with a possible role of serotonin in liver disease-associated fatigue (46,47). The 5-hydroxytryptamine 1A receptor subtype has been commonly linked to altered behaviours in humans and animals (48,49). The 5HT1A receptor exists as an autoreceptor situated on cell bodies of serotonergic nerves originating in the midbrain dorsal raphe nucleus (50; Figure 2). Activation of these cell body serotonin autoreceptors in the midbrain results in decreased serotonin release from the distal nerve terminals that project throughout the CNS (48–50). However, 5HT1A receptors also exist postsynaptically within the brain. Activation of postsynaptic 5HT1A receptors typically exerts an inhibiting influence on neurons where they are located (48). Therefore, systemic administrations of a 5HT1A receptor agonist results in a net decrease in serotonin neurotransmission at all postsynaptic serotonin receptors except those of the 5HT1A subtype (48). Experimental results in cholestatic rats are consistent with increased sensitivity and the number of 5HT1A midbrain autoreceptors coupled with normal 5HT1A postsynaptic receptors elsewhere within the CNS (46,47); these findings that would be expected to give rise to decreased central serotonin release as a potential contributor to central fatigue in cholestatic liver disease. In fact, this suggestion is supported by findings that the repeated administration of a 5HT1A receptor agonist, which desensitizes 5HT1A autoreceptors and increases central serotonin release into synapses where postsynaptic 5HT1A receptors are active, ameliorated fatigue-like behaviours in cholestatic rats (51). These observations suggest that the 5HT1A receptor may play an important role in the genesis of central fatigue in patients with liver disease.
Figure 2.

Serotonin-secreting nerves originate in the dorsal raphe nucleus within the midbrain and their axons project throughout the central nervous system. Activation of 5-hydroxytryptamine 1A (5HT1A) autoreceptors located on serotonin nerve cell bodies within the raphe nucleus results in a decrease in serotonin release from nerve terminals at the distal projection sites of these serotonergic nerves. ↓ Decrease
More recently, 5HT3 receptor antagonists have been reported to improve fatigue in patients with the chronic fatigue syndrome (52), as well as in a patient with hepatitis C-induced fatigue (53). Similar findings have been reported in preliminary experiments in cholestatic rats (54). Of note, in a recent clinical trial, the 5HT3 receptor antagonist ondansetron appeared to have a limited effect on fatigue in PBC patients, although the results of this study are difficult to interpret due to possible patient unblinding and a significant placebo effect (55). Therefore, the role played by serotonin-activating central 5HT3 receptors in the genesis of liver disease-associated fatigue remains unclear.
Noradrenaline
Noradrenaline is a classical neurotransmitter important in behavioural activation, especially in the context of acute stress (56). More important, hypofunctioning of noradrenaline-containing nerve pathways within the brain has been implicated in the development of central fatigue (57). Specifically, reserpine, which depletes central calecholamine stores, is commonly associated with the development of fatigue and depression (58). Moreover, beta-blockers and alpha-2 agonists frequently cause fatigue (58). Unfortunately, the role of altered noradrenaline neurotransmission in liver disease-associated fatigue remains completely unknown. However, an obvious patient population that could be studied includes cirrhotic patients taking beta-blockers as variceal bleed prophylaxis (59).
Other neurotransmitters
Numerous other neurotransmitter systems have also been implicated in the control of locomotor activity and behavioural activation, including the dopaminergic and cannabinoid systems (60,61). However, no studies of the role of these neurotransmitter systems in liver disease-associated fatigue have been performed.
The obvious question that arises is, how do these alterations in central neurotransmission, which lead to fatigue, come about in the setting of liver disease? Although the answer to this question is still unclear, it likely involves specific communication pathways from the diseased liver to the brain, as well as nonspecific effects of liver disease acting in the context of a chronic stress for an individual (62).
Chronic stress can have profound behavioural effects (63). These changes in behaviour can include depression, anxiety and fatigue (63,64). Moreover, this effect can be caused by physical, psychological or a combination of stressors, and these stressors have been implicated in changes in central neurotransmitter systems (63,65,66). Of note, chronic stress in rodents can induce marked changes in neurotransmitter systems within the brain, which have been discussed earlier with regards to the genesis of central fatigue (65,66). Furthermore, chronic liver disease can be viewed as both a physical and a psychological stressor. Although the physical stress of chronic liver disease is often relatively mild in the absence of cirrhosis or liver failure, the psychological impact of carrying a diagnosis of liver disease can be substantial because it directly involves social and professional interactions, and feelings of self-worth and fear. Certainly this ‘indirect’ pathway that relates to disease-labelling may contribute significantly to the development of central fatigue in patients who are aware of their diagnosis (14,67–69). However, this does not account for the observation that a significant proportion of patients with liver disease presents to doctors specifically complaining of fatigue before a diagnosis of liver disease is made. Therefore, a ‘direct’ communication pathway between the liver and the brain appears to play an important role in fatigue genesis in the context of liver disease.
Traditionally, communication between the periphery (ie, outside the CNS) and the brain has been considered to involve two potential pathways: neural (ie, nerve projections; Figure 3) and/or humoral (ie, substances contained within the circulation; Figure 4) (70). In the setting of liver disease, either or both pathways may be activated.
Figure 3.
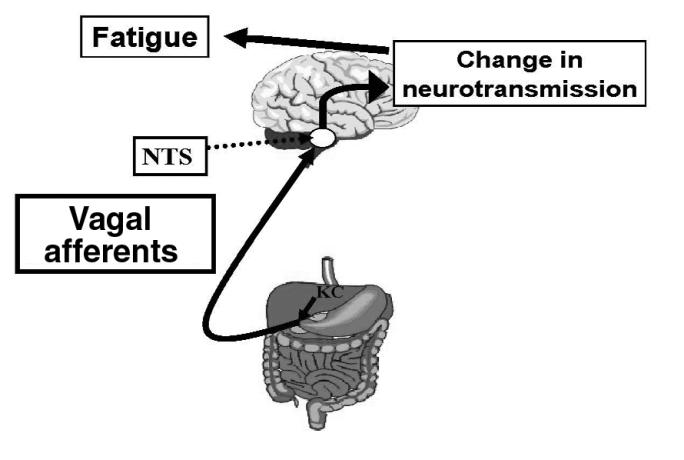
Neural transmission pathway for liver to brain signalling. Kupffer cells within the liver secrete proinflammatory mediators (eg, cytokines, prostaglandins) that activate vagal afferent nerves, which innervate the liver. Nerve impulses are then carried to the nucleus tractus solitarius (NTS) within the brainstem, which acts as a relay centre for the transmission of these impulses to areas throughout the brain. Stimulation of vagal afferent nerves can thereby result in alterations in neurotransmitter systems within the brain, which may give rise to central fatigue
Figure 4.

Humoral transmission pathway for liver to brain signalling. Substances released within the circulation in the setting of liver disease (eg, cytokines, including tumour necrosis factor-alpha [TNFα]) activate the cerebral endothelial cells that make up the blood-brain barrier. Activated cerebral endothelial cells then secrete secondary messengers (eg, nitric oxide, prostaglandin E2) into the brain parenchyma, which induce changes in central neurotransmitter systems, which give rise to central fatigue
The liver and peritoneum are richly innervated with afferent signals being carried to the brain in vagal and spinal nerve projections (71,72). Activation of these nerves during inflammation in rodents stimulates areas of the brain important in regulating behavioural arousal and results in the development of fatigue-like behaviours (73–75). Moreover, these effects can be abolished by subdiaphragmatic vagotomy (76). However, patients who have recurrent liver inflammation following liver transplantation and therefore after complete hepatic denervation (eg, hepatitic C, PBC) often continue to experience fatigue (77,78). These observations suggest that neural projections from the liver to the brain are less likely to contribute significantly to changes in CNS neurotransmitter systems that give rise to central fatigue in the setting of liver disease.
Communication between the diseased liver and the brain may also occur via mediators released into the circulation as a result of hepatic injury. In this regard, cytokines present within the circulation have received the greatest attention (79,80). Specifically, the liver contains the largest population of fixed macrophages in the body, which represents an important source of cytokines found in the circulation (79,80). Moreover, elevated circulating cytokine levels have commonly been documented in the setting of both cholestatic and hepatitic liver diseases (81–85). Furthermore, elevations in circulating cytokine levels, including interleukin-6, tumour necrosis factor-alpha and interferons, commonly induce fatigue and lethargy (86–90). In addition, elevated plasma endotoxin levels have been documented in patients with liver disease (91–93), and endotoxin administration to humans and animals results in elevated circulating cytokine levels as well as the generation of malaise and lethargy (94). In support of inflammatory mediators in the circulation causing changes in central neurotransmission and inducing fatigue, the intravenous administration of cytokines or endotoxin in rodents results in altered central neurotransmitter levels, including those implicated in the genesis of central fatigue (eg, CRH, serotonin; [95–97]). Furthermore, in support of the hypothesis that endotoxin can alter central neurotransmission to change behaviour, a recent report (98) suggested that gut-derived endotoxin can precipitate hepatic encephalopathy in cirrhotic patients.
An obvious question that arises concerns how cytokines, which are large proteins, gain access to the CNS. Two potential theories have been put forward to explain this observation. First, there are areas of the brain that are devoid of an intact blood-brain barrier, which represent potential areas where large molecules such as cytokines could gain access to the CNS (99). Second, the cerebral endothelial cells, which form the basis of the blood-brain barrier, express a number of cytokine receptors and can be stimulated by cytokines within the circulation to produce a variety of secondary messengers (eg, nitric oxide, prostaglandin E2), which can then be secreted into brain parenchynal structures (100–102). Moreover, both prostaglandin E2 and nitric oxide are capable of inducing changes in central neurotransmitter systems (79,80). In addition, circulating cytokines (via either of these mechanisms) can induce de novo synthesis and release of cytokines within the brain (from astroglia for example) (79,80). In support of the hypothesis that liver disease is associated with altered central cytokine responses, rats with experimental cholestatic liver disease exhibit increased sensitivity to the generation of fatigue-like behaviours compared with controls when interleukin-1-beta is administered centrally (103). These findings suggest that cytokines entering, or being produced within, the brain, in the setting of liver disease can induce fatigue when present at levels that are without effect in healthy patients.
MANAGEMENT OF FATIGUE IN PATIENTS WITH LIVER DISEASE
General approach
Management of central fatigue associated with liver disease is complicated and hampered by a general lack of understanding of fatigue in general. Therefore, specific therapies are currently not available. However, many patients can benefit from a systematic approach. An important first step in this process is to rule out causes of fatigue that may be separate from the patient’s liver disease. While meeting with a patient, specific questions should be asked with regard to symptoms of hypothyroidism, sleep patterns/behaviours, exercise, caffeine and alcohol ingestion, and life stresses. Moreover, a loss of motivation and pleasure in things that a patient would normally enjoy (ie, anhedonia), loss of interest in social activities, early morning awakenings, feelings of guilt and thoughts of suicide are important clues to the presence of depression and need to be directly addressed, and therapy instituted or psychiatric referral considered (20). In addition, a complete review of a patient’s prescription medications (eg, beta-blockers, benzodiazepines, etc) as well as over-the-counter medications and health supplements should be undertaken. Finally, simple laboratory tests should be performed to exclude other possible causes of fatigue (eg, thyroid-stimulating hormone, calcium, creatinine, blood urea nitrogen, electrolytes, fasting blood sugar and magnesium).
Modifying behavioural components to fatigue
Significant central fatigue warrants lifestyle changes, which may include rest periods and reduced workloads (104,105). However, the maintenance of physical activity is of paramount importance. The natural inclination of patients with central fatigue is to decrease physical activity. However, decreased physical activity over time will lead to cardiovascular and muscular deconditioning, which then makes physical activity even more difficult (104,105). Therefore, all patients need to be counselled with regard to maintaining an appropriate level of activity. In addition, an increase in activity should be attempted through the institution of a graded exercise program (106).
In many patients with liver disease and central fatigue, the degree and perpetuation of fatigue may be directly related to and influenced by a complex interaction of physiological, emotional, cognitive, behavioural and social factors (107). A patient’s thoughts and beliefs (ie, cognitions) may contribute significantly to the maintenance of certain illness behaviours, including fatigue (107,108). This concept has received the greatest attention in the setting of central fatigue related to chronic fatigue syndrome (107,108). The idea is that psychological processes not only drive deleterious behavioural patterns, but also directly increase the perception of fatigue (108). Moreover, cognitive behavioural therapy is the only therapy of proven efficacy for patients with chronic fatigue syndrome (109). Therefore, cognitive behaviour therapy needs to be examined as a potential therapeutic modality for fatigue in patients with liver disease. Subjective sleep disturbance is commonly associated with fatigue in patients with liver disease (8,110). Therefore, all fatigued liver disease patients need to be counselled with regard to proper sleep habits. However, any historical clues as to the presence of a specific sleep disorder (eg, sleep apnea) mandate the pursuit of formal sleep studies. In this vein, alcohol and caffeine should be limited. Moreover, any medications that may be contributing to fatigue should be discontinued if possible.
Pharmacological interventions
Specific pharmacological therapies directed at the physiological abnormalities that may underlie central fatigue in patients with liver disease are currently not available. Nonspecific CNS stimulants, including modafinil, have been used to treat central fatigue (111,112); however, their use in patients with liver disease and fatigue has not been reported but may warrant further investigation, especially for patients with severe fatigue. Some patients respond to nocturnal therapy with low-dose amitriptyline, especially if poor sleep patterns are possibly contributing.
CONCLUSIONS
Fatigue is the most common symptom reported by patients with liver disease. Although the underlying pathogenesis of fatigue in liver disease is still poorly defined, it appears to involve changes in central neurotransmission, which result from signalling between the diseased liver and the brain. A better understanding of the pathways and the neurotransmitter systems involved may provide directed specific therapies for liver disease-associated fatigue.
ACKNOWLEDGEMENTS
Mark G Swain is an Alberta Heritage Foundation for Medical Research Senior Scholar and a Canadian Institutes of Health Research Investigator
REFERENCES
- 1.Adams RD, Victor M, Ropper AH. Fatigue, asthenia, anxiety and depressive reactions. In: Adams RD, Victor M, Ropper AH, editors. Principles of Neurology. 6. New York: McGraw-Hill; 1997. pp. 497–507. [Google Scholar]
- 2.Kumar D, Tandon RK. Fatigue in cholestatic liver disease – a perplexing symptom. Postgrad Med J. 2002;78:404–7. doi: 10.1136/pmj.78.921.404. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 3.Milkiewicz P, Heathcote EJ. Fatigue in chronic cholestasis. Gut. 2004;53:475–7. doi: 10.1136/gut.2003.025155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Obermayer-Straub P, Strassburg CP, Manns MP. Autoimmune hepatitis. J Hepatol. 2000;32(Suppl 1):181–97. doi: 10.1016/s0168-8278(00)80425-0. [DOI] [PubMed] [Google Scholar]
- 5.Kenny-Walsh E Irish Hepatology Research Group. Clinical outcomes after hepatitis C infection from contaminated anti-D immune globulin. N Engl J Med. 1999;340:1228–33. doi: 10.1056/NEJM199904223401602. [DOI] [PubMed] [Google Scholar]
- 6.Poynard T, Cacoub P, Ratziu V, et al. Fatigue in patients with chronic hepatitis C. J Viral Hepat. 2002;9:295–303. doi: 10.1046/j.1365-2893.2002.00364.x. [DOI] [PubMed] [Google Scholar]
- 7.Huet PM, Deslauriers J, Tran A, Faucher C, Charbonneau J. Impact of fatigue on the quality of life in patients with primary biliary cirrhosis. Am J Gastroenterol. 2000;95:760–7. doi: 10.1111/j.1572-0241.2000.01857.x. [DOI] [PubMed] [Google Scholar]
- 8.Cauch-Dudek K, Abbey S, Stewart DE, Heathcote EJ. Fatigue in primary biliary cirrhosis. Gut. 1998;43:705–10. doi: 10.1136/gut.43.5.705. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Younossi ZM, Boparai N, Price LL, Kiwi ML, McCormick M, Guyatt G. Health-related quality of life in chronic liver disease: The impact of type and severity of liver disease. Am J Gastroenterol. 2001;96:2199–205. doi: 10.1111/j.1572-0241.2001.03956.x. [DOI] [PubMed] [Google Scholar]
- 10.Ferrari R, Pappas G, Agostinelli D, et al. Type 1 autoimmune hepatitis: Patters of clinical presentations and differential diagnosis of the ‘acute’ type. QJM. 2004;97:407–12. doi: 10.1093/qjmed/hch072. [DOI] [PubMed] [Google Scholar]
- 11.Czaja AJ, Freese DK. Diagnosis and treatment of autoimmune hepatitis. Hepatology. 2002;36:479–97. doi: 10.1053/jhep.2002.34944. [DOI] [PubMed] [Google Scholar]
- 12.Foster GR, Goldin RD, Thomas HC. Chronic hepatitis C virus infection causes a significant reduction in quality of life in the absence of cirrhosis. Hepatology. 1998;27:209–12. doi: 10.1002/hep.510270132. [DOI] [PubMed] [Google Scholar]
- 13.Wessely S, Pariante C. Fatigue, depression and chronic hepatitis C infection. Psychol Med. 2002;32:1–10. doi: 10.1017/s0033291701004615. [DOI] [PubMed] [Google Scholar]
- 14.Rodger AJ, Jolley D, Thompson SC, Lanigan A, Crofts N. The impact of diagnosis of hepatitis C virus on quality of life. Hepatology. 1999;30:1299–301. doi: 10.1002/hep.510300504. [DOI] [PubMed] [Google Scholar]
- 15.Coughlan B, Sheehan J, Hickey A, Crowe J. Psychological well-being and quality of life in women with an iatrogenic hepatitis C infection. Br J Health Psychol. 2002;7:105–16. doi: 10.1348/135910702169394. [DOI] [PubMed] [Google Scholar]
- 16.Kramer L, Bauer E, Funk G, et al. Subclinical impairment of brain function in chronic hepatitis C infection. J Hepatol. 2002;37:349–54. doi: 10.1016/s0168-8278(02)00172-1. [DOI] [PubMed] [Google Scholar]
- 17.Forton DM, Allsop JM, Main J, Foster GR, Thomas HC, Taylor-Robinson SD. Evidence for a cerebral effect of the hepatitis C virus. Lancet. 2001;358:38–9. doi: 10.1016/S0140-6736(00)05270-3. [DOI] [PubMed] [Google Scholar]
- 18.Weissenborn K, Krause J, Bokemeyer M, et al. Hepatitis C virus infection affects the brain-evidence from psychometric studies and magnetic resonance spectroscopy. J Hepatol. 2004;41:845–51. doi: 10.1016/j.jhep.2004.07.022. [DOI] [PubMed] [Google Scholar]
- 19.Morgello S. The nervous system and hepatitis C virus. Semin Liver Dis. 2005;25:118–21. doi: 10.1055/s-2005-864787. [DOI] [PubMed] [Google Scholar]
- 20.Chaudhuri A, Behan PO. Fatigue in neurological disorders. Lancet. 2004;363:978–88. doi: 10.1016/S0140-6736(04)15794-2. [DOI] [PubMed] [Google Scholar]
- 21.Swain MG. Fatigue in chronic disease. Clin Sci (Lond) 2000;99:1–8. [PubMed] [Google Scholar]
- 22.McDonald J, Jayasuriya R, Bindley P, Gonsalvez C, Gluseska S. Fatigue and psychological disorders in chronic hepatitis C. J Gastroenterol Hepatol. 2002;17:171–6. doi: 10.1046/j.1440-1746.2002.02669.x. [DOI] [PubMed] [Google Scholar]
- 23.Schwartz JE, Jandorf L, Krupp LB. The measurement of fatigue: A new instrument. J Psychosom Res. 1993;37:753–62. doi: 10.1016/0022-3999(93)90104-n. [DOI] [PubMed] [Google Scholar]
- 24.Fisk J, Ritvo PG, Ross L, Haase DA, Marrie TJ, Schlech WF. Measuring the functional impact of fatigue: Initial validation of the fatigue impact scale. Clin Infect Dis. 1994;18(Suppl 1):S79–83. doi: 10.1093/clinids/18.supplement_1.s79. [DOI] [PubMed] [Google Scholar]
- 25.Bearn J, Wessely S. Neurobiological aspects of the chronic fatigue syndrome. Eur J Clin Invest. 1994;24:79–90. doi: 10.1111/j.1365-2362.1994.tb00971.x. [DOI] [PubMed] [Google Scholar]
- 26.Crofford LJ, Demitrack MA. Evidence that abnormalities of central neurohormonal systems are key to understanding fibromyalgia and chronic fatigue syndrome. Rheum Dis Clin North Am. 1996;22:267–84. doi: 10.1016/s0889-857x(05)70272-6. [DOI] [PubMed] [Google Scholar]
- 27.Koob GF. Corticotropin-releasing factor, norepinephrine, and stress. Biol Psychiatry. 1999;46:1167–80. doi: 10.1016/s0006-3223(99)00164-x. [DOI] [PubMed] [Google Scholar]
- 28.Lucki I. The spectrum of behaviors influenced by serotonin. Biol Psychiatry. 1998;44:151–62. doi: 10.1016/s0006-3223(98)00139-5. [DOI] [PubMed] [Google Scholar]
- 29.Swanson LW, Sawchenko PE, Rivier J, Vale WW. Organization of ovine corticotropin-releasing factor immunoreactive cells and fibers in the rat brain: An immunohistological study. Neuroendocrinology. 1983;36:165–86. doi: 10.1159/000123454. [DOI] [PubMed] [Google Scholar]
- 30.Koob GF, Heinrichs SC, Pich EM, et al. The role of corticotropin-releasing factor in behavioural responses to stress. Ciba Found Symp. 1993;172:277–89. doi: 10.1002/9780470514368.ch14. [DOI] [PubMed] [Google Scholar]
- 31.Sutton RE, Koob GF, Le Moal M, Rivier J, Vale W. Corticotropin-releasing factor produces behavioural activation in rats. Nature. 1982;297:331–3. doi: 10.1038/297331a0. [DOI] [PubMed] [Google Scholar]
- 32.Gold PW, Chrousos GP. The endocrinology of melancholic and atypical depression: Relation to neurocircuitry and somatic consequences. Proc Assoc Am Phys. 1998;111:22–34. doi: 10.1046/j.1525-1381.1999.09423.x. [DOI] [PubMed] [Google Scholar]
- 33.Clauw DJ, Chrousos GP. Chronic pain and fatigue syndromes: Overlapping clinical and neuroendocrine features and potential pathogenic mechanisms. Neuroimmunomodulation. 1997;4:134–53. doi: 10.1159/000097332. [DOI] [PubMed] [Google Scholar]
- 34.Swain MG, Patchev V, Vergalla J, Chrousos G, Jones EA. Suppression of hypothalamic-pituitary-adrenal axis responsiveness to stress in a rat model of acute cholestasis. J Clin Invest. 1993;91:1903–8. doi: 10.1172/JCI116408. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Swain MG, Maric M. Defective corticotropin-releasing hormone mediated neuroendocrine and behavioral responses in cholestatic rats: Implications for cholestatic liver disease-related sickness behaviors. Hepatology. 1995;22:1560–4. [PubMed] [Google Scholar]
- 36.Burak KW, Le T, Swain MG. Increased sensitivity to the locomotor-activating effects of corticotropin-releasing hormone in cholestatic rats. Gastroenterology. 2002;122:681–8. doi: 10.1053/gast.2002.31878. [DOI] [PubMed] [Google Scholar]
- 37.Swain MG, Mogiakou MA, Bergassa NV, Chrousos GP. Facilitation of ACTH and cortisol responses to corticotropin-releasing hormone (CRH) in patients with primary biliary cirrhosis. Hepatology. 1994;20:A197. [Google Scholar]
- 38.Hanley NR, Van de Kar LD. Serotonin and the neuroendocrine regulation of the hypothalamic-pituitary-adrenal axis in health and disease. Vitam Horm. 2003;66:189–255. doi: 10.1016/s0083-6729(03)01006-9. [DOI] [PubMed] [Google Scholar]
- 39.Abrams JK, Johnson PL, Hollis JH, Lowry CA. Anatomic and functional topography of the dorsal raphe nucleus. Ann N Y Acad Sci. 2004;1018:46–57. doi: 10.1196/annals.1296.005. [DOI] [PubMed] [Google Scholar]
- 40.Buller KM. Neuroimmune stress responses: Reciprocal connections between the hypothalamus and the brainstem. Stress. 2003;6:11–7. doi: 10.1080/1025389031000092313. [DOI] [PubMed] [Google Scholar]
- 41.Roth BL. Multiple serotonin receptors: Clinical and experimental aspects. Ann Clin Psychiatry. 1994;6:67–78. doi: 10.3109/10401239409148985. [DOI] [PubMed] [Google Scholar]
- 42.Bailey SP, Davis JM, Ahlborn EN. Neuroendocrine and substrate responses to altered brain 5-HT activity during prolonged exercise to fatigue. J Appl Physiol. 1993;74:3006–12. doi: 10.1152/jappl.1993.74.6.3006. [DOI] [PubMed] [Google Scholar]
- 43.Wilson WM, Maughan RJ. Evidence for a possible role of 5-hydroxytryptamine in the genesis of fatigue in man: Administration of paroxetine, a 5-HT re-uptake inhibitor, reduces the capacity to perform prolonged exercise. Exp Physiol. 1992;77:921–4. doi: 10.1113/expphysiol.1992.sp003660. [DOI] [PubMed] [Google Scholar]
- 44.Bakheit AM, Behan PO, Dinan TG, Gray CE, O’Keane V. Possible upregulation of hypothalamic 5-hydroxytryptamine receptors in patients with postviral fatigue syndrome. BMJ. 1992;304:1010–2. doi: 10.1136/bmj.304.6833.1010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 45.Goldenberg D, Mayskiy M, Mossey C, Ruthazer R, Schmid C. A randomized, double-blind crossover trial of fluoxetine and amitriptyline in the treatment of fibromyalgia. Arthritis Rheum. 1996;39:1852–9. doi: 10.1002/art.1780391111. [DOI] [PubMed] [Google Scholar]
- 46.Burak KW, Le T, Swain MG. Increased midbrain 5-HT1A receptor number and responsiveness in cholestatic rats. Brain Res. 2001;892:376–9. doi: 10.1016/s0006-8993(00)03058-4. [DOI] [PubMed] [Google Scholar]
- 47.Celik T, Goren MZ, Cinar K, et al. Fatigue of cholestasis and the serotonergic neurotransmitter system in the rat. Hepatology. 2005;41:731–7. doi: 10.1002/hep.20617. [DOI] [PubMed] [Google Scholar]
- 48.Blier P, Ward NM. Is there a role for 5-HT1A agonists in the treatment of depression? Biol Psychiatry. 2003;53:193–203. doi: 10.1016/s0006-3223(02)01643-8. [DOI] [PubMed] [Google Scholar]
- 49.Rueter LE, Fornal CA, Jacobs BL. A critical review of 5-HT brain microdialysis and behavior. Rev Neurosci. 1997;8:117–37. doi: 10.1515/revneuro.1997.8.2.117. [DOI] [PubMed] [Google Scholar]
- 50.Riad M, Watkins KC, Doucet E, Hamon M, Descarries L. Agonist-induced internalization of serotonin-1a receptors in the dorsal raphe nucleus (autoreceptors) but not hippocampus (heteroreceptors) J Neurosci. 2001;21:8378–86. doi: 10.1523/JNEUROSCI.21-21-08378.2001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 51.Swain MG, Maric M. Improvement in cholestasis-associated fatigue with a serotonin receptor agonist using a novel rat model of fatigue assessment. Hepatology. 1997;25:291–4. doi: 10.1002/hep.510250206. [DOI] [PubMed] [Google Scholar]
- 52.Spath M, Welzel D, Farber L. Treatment of chronic fatigue syndrome with 5-HT3 receptor antagonists – preliminary results. Scand J Rheumatol Suppl. 2000;113:72–7. [PubMed] [Google Scholar]
- 53.Jones EA. Relief from profound fatigue associated with chronic liver disease by long-term ondansetron therapy. Lancet. 1999;354:397. doi: 10.1016/S0140-6736(99)02936-0. [DOI] [PubMed] [Google Scholar]
- 54.Swain MG, Le T, Ho W, Sharkey KA. Fatigue-like behavior is significantly improved by the 5-HT3 receptor antagonist tropisetron in cholestatic rats. Hepatology. 2004;40:A292. [Google Scholar]
- 55.Theal JJ, Toosi MN, Girlan L, et al. A randomized, controlled crossover trial of ondansetron in patients with primary biliary cirrhosis and fatigue. Hepatology. 2005;41:1305–12. doi: 10.1002/hep.20698. [DOI] [PubMed] [Google Scholar]
- 56.Berridge CW, Waterhouse BD. The locus coeruleus-noradrenergic system: Modulation of behavioral state and state-dependent cognitive processes. Brain Res Brain Res Rev. 2003;42:33–84. doi: 10.1016/s0165-0173(03)00143-7. [DOI] [PubMed] [Google Scholar]
- 57.Gold PW, Chrousos GP. The endocrinology of melancholic and atypical depression: Relation to neurocircuitry and somatic consequences. Proc Assoc Am Physicians. 1999;111:22–34. doi: 10.1046/j.1525-1381.1999.09423.x. [DOI] [PubMed] [Google Scholar]
- 58.Webster J, Koch HF. Aspects of tolerability of centrally acting antihypertensive drugs. J Cardiovasc Pharmacol. 1996;27(Suppl 3):S49–54. doi: 10.1097/00005344-199627003-00007. [DOI] [PubMed] [Google Scholar]
- 59.Vlachogiannakos J, Goulis J, Patch D, Burroughs AK. Review article: Primary prophylaxis for portal hypertensive bleeding in cirrhosis. Aliment Pharmacol Ther. 2000;14:851–60. doi: 10.1046/j.1365-2036.2000.00778.x. [DOI] [PubMed] [Google Scholar]
- 60.Tzschentke TM. Pharmacology and behavioral pharmacology of the mesocortical dopamine system. Prog Neurobiol. 2001;63:241–320. doi: 10.1016/s0301-0082(00)00033-2. [DOI] [PubMed] [Google Scholar]
- 61.Iversen L. Cannabis and the brain. Brain. 2003;126:1252–70. doi: 10.1093/brain/awg143. [DOI] [PubMed] [Google Scholar]
- 62.Shanks S, Harbuz MS, Jessop DS, Perks P, Moore PM, Lightman SL. Inflammatory disease as chronic stress. Ann N Y Acad Sci. 1998;840:599–607. doi: 10.1111/j.1749-6632.1998.tb09599.x. [DOI] [PubMed] [Google Scholar]
- 63.Chrousos GP, Gold PW. The concepts of stress and stress system disorders. Overview of physical and behavioral homeostasis. JAMA. 1992;267:1244–52. Erratum in 1992;268:200. [PubMed] [Google Scholar]
- 64.Korte SM, Koolhaas JM, Wingfield JC, McEwen BS. The Darwinian concept of stress: Benefits of allostasis and costs of allostatic load and the trade-offs in health and disease. Neurosci Biobehav Rev. 2005;29:3–38. doi: 10.1016/j.neubiorev.2004.08.009. [DOI] [PubMed] [Google Scholar]
- 65.Tsigos C, Chrousos GP. Hypothalamic-pituitary-adrenal axis, neuroendocrine factors and stress. J Psychosom Res. 2005;53:865–71. doi: 10.1016/s0022-3999(02)00429-4. [DOI] [PubMed] [Google Scholar]
- 66.McEwen BS. The neurobiology of stress: From serendipity to clinical relevance. Brain Res. 2000;886:172–89. doi: 10.1016/s0006-8993(00)02950-4. [DOI] [PubMed] [Google Scholar]
- 67.Cordoba J, Reyes J, Esteban JI, Hernandez JM. Labeling may be an important cause of reduced quality of life in chronic hepatitis C. Am J Gastroenterol. 2003;98:226–7. doi: 10.1111/j.1572-0241.2003.07195.x. [DOI] [PubMed] [Google Scholar]
- 68.Suurmeijer TP, Reuvekamp MF, Aldenkamp BP. Social functioning, psychological functioning, and quality of life in epilepsy. Epilepsia. 2001;42:1160–8. doi: 10.1046/j.1528-1157.2001.37000.x. [DOI] [PubMed] [Google Scholar]
- 69.Grassi L, Satriano J, Serra A, et al. Emotional stress, psychosocial variables and coping associated with hepatitis C virus and human immunodeficiency virus infections in intravenous drug users. Psychother Psychosom. 2002;71:342–9. doi: 10.1159/000065993. [DOI] [PubMed] [Google Scholar]
- 70.Blatteis CM. The afferent signalling of fever. J Physiol. 2000;526:470. [PubMed] [Google Scholar]
- 71.Adachi A. Projection of the hepatic vagal nerve in the medulla oblongata. J Auton Nerv Syst. 1984;10:287–93. doi: 10.1016/0165-1838(84)90026-2. [DOI] [PubMed] [Google Scholar]
- 72.Magni F, Carobi C. The afferent and preganglionic parasympathetic innervation of the rat liver, demonstrated by the retrograde transport of horseradish peroxidase. J Auton Nerv Syst. 1983;8:237–60. doi: 10.1016/0165-1838(83)90108-x. [DOI] [PubMed] [Google Scholar]
- 73.Wan W, Wetmore L, Sorensen CM, Greenberg AH, Nance DM. Neural and biochemical mediators of endotoxin and stress-induced c-fos expression in the rat brain. Brain Res Bull. 1994;34:7–14. doi: 10.1016/0361-9230(94)90179-1. [DOI] [PubMed] [Google Scholar]
- 74.Goehler LE, Gaykema RP, Hansen MK, Anderson K, Maier SF, Watkins LR. Vagal immune-to-brain communication: A visceral chemosensory pathway. Auton Neurosci. 2000;85:45–59. doi: 10.1016/S1566-0702(00)00219-8. [DOI] [PubMed] [Google Scholar]
- 75.Konsman JP, Luheshi GN, Bluthe RM, Dantzer R. The vagus nerve mediates behavioural depression, but not fever, in response to peripheral immune signals; a functional anatomical analysis. Eur J Neurosci. 2000;12:4434–46. doi: 10.1046/j.0953-816x.2000.01319.x. [DOI] [PubMed] [Google Scholar]
- 76.Gaykema RP, Dijkstra I, Tilder FJ. Subdiaphragmatic vagotomy supresses endotoxin-induced activation of the hypothalamic corticotropin-releasing hormone neurons and ACTH secretion. Endocrinology. 1995;136:4717–20. doi: 10.1210/endo.136.10.7664696. [DOI] [PubMed] [Google Scholar]
- 77.O’Carroll RE, Couston M, Cossar J, Masterton G, Hayes PC. Psychological outcome and quality of life following liver transplantation: A prospective, national, single-center study. Liver Transpl. 2003;9:712–20. doi: 10.1053/jlts.2003.50138. [DOI] [PubMed] [Google Scholar]
- 78.Belle SH, Porayko MK, Hoofnagle JH, Lake JR, Zetterman RK. Changes in quality of life after liver transplantation among adults. National Institute of Diabetes and Digestive and Kidney Diseases (NIDDK) Liver Transplantation Database (LTD) Liver Transpl Surg. 1997;3:93–104. doi: 10.1002/lt.500030201. [DOI] [PubMed] [Google Scholar]
- 79.Turnbull AV, Rivier CL. Regulation of the hypothalamic-pituitary-adrenal axis by cytokines: Actions and mechanisms of action. Physiol Rev. 1999;79:1–71. doi: 10.1152/physrev.1999.79.1.1. [DOI] [PubMed] [Google Scholar]
- 80.Licinio J, Wong ML. Pathways and mechanisms for cytokine signaling of the central nervous system. J Clin Invest. 1997;100:2941–7. doi: 10.1172/JCI119846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 81.Tilg H, Wilmer A, Vogel W, et al. Serum levels of cytokines in chronic liver diseases. Gastroenterology. 1992;103:264–74. doi: 10.1016/0016-5085(92)91122-k. [DOI] [PubMed] [Google Scholar]
- 82.Eriksson AS, Gretzer C, Wallerstedt S. Elevation of cytokines in peritoneal fluid and blood in patients with liver cirrhosis. Hepatogastroenterology. 2004;51:505–9. [PubMed] [Google Scholar]
- 83.Tilg H. Cytokines and liver diseases. Can J Gastroenterol. 2001;15:661–8. doi: 10.1155/2001/746736. [DOI] [PubMed] [Google Scholar]
- 84.Bemelmans MH, Gouma DJ, Greve JW, Buurman WA. Cytokines tumor necrosis factor and interleukin-6 in experimental biliary obstruction in mice. Hepatology. 1992;15:1132–6. doi: 10.1002/hep.1840150626. [DOI] [PubMed] [Google Scholar]
- 85.Mizuhara H, O’Neill E, Seki N, et al. T cell activation-associated hepatic injury: Mediation by tumor necrosis factors and protection by interleukin-6. J Exp Med. 1994;179:1529–37. doi: 10.1084/jem.179.5.1529. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 86.Vollmer-Conna U, Fazou C, Cameron B, et al. Production of pro-inflammatory cytokines correlates with the symptoms of acute sickness behaviour in humans. Psychol Med. 2004;34:1289–97. doi: 10.1017/s0033291704001953. [DOI] [PubMed] [Google Scholar]
- 87.Kerr JR, Tyrrell DA. Cytokines in parvovirus B19 infection as an aid to understanding chronic fatigue syndrome. Curr Pain Headache Rep. 2003;7:333–41. doi: 10.1007/s11916-003-0031-3. [DOI] [PubMed] [Google Scholar]
- 88.Mullington JM, Hinze-Selch D, Pollmacher TO. Mediators of inflammation and their interaction with sleep: Relevance for chronic fatigue syndrome and related conditions. Ann N Y Acad Sci. 2001;933:201–10. doi: 10.1111/j.1749-6632.2001.tb05825.x. [DOI] [PubMed] [Google Scholar]
- 89.Taylor JL, Grossberg SE. The effects of interferon-alpha on the production and action of other cytokines. Semin Oncol. 1998;25(Suppl 1):23–9. [PubMed] [Google Scholar]
- 90.Schuler M, Bruntsch U, Spath-Schwalbe E, et al. Lack of efficacy of recombinant human interleukin-6 in patients with advanced renal cell carcinoma: Results of a phase II study. Eur J Cancer. 1998;34:754–6. doi: 10.1016/s0959-8049(97)10089-2. [DOI] [PubMed] [Google Scholar]
- 91.Kaser A, Ludwiczek O, Waldenberger P, Jaschke W, Vogel W, Tily H. Endotoxin and its binding proteins in chronic liver disease: The effect of transjugular intrahepatic portosystemic shunting. Liver. 2002;22:380–7. doi: 10.1034/j.1600-0676.2002.01666.x. [DOI] [PubMed] [Google Scholar]
- 92.Caradonna L, Mastronardi ML, Magrone T, et al. Biological and clinical significance of endotoxemia in the course of hepatitis C virus infection. Curr Pharm Des. 2002;8:995–1005. doi: 10.2174/1381612024606983. [DOI] [PubMed] [Google Scholar]
- 93.Yamamoto Y, Sezai S, Sakurabayashi S, Hirano M, Kamisaka K, Oka H. A study of endotoxaemia in patients with primary biliary cirrhosis. J Int Med Res. 1994;22:95–9. doi: 10.1177/030006059402200205. [DOI] [PubMed] [Google Scholar]
- 94.Dantzer R. Cytokine-induced sickness behavior: Where do we stand? Brain Behav Immun. 2001;15:7–24. doi: 10.1006/brbi.2000.0613. [DOI] [PubMed] [Google Scholar]
- 95.Suda T, Tozawa F, Ushiyama T, Sumimoto T, Yamada M, Demura H. Interleukin-1 stimulates corticotropin-releasing factor gene expression in rat hypothalamus. Endocrinology. 1990;126:1223–8. doi: 10.1210/endo-126-2-1223. [DOI] [PubMed] [Google Scholar]
- 96.Linthorst AC, Reul JM. Brain neurotransmission during peripheral inflammation. Ann N Y Acad Sci. 1998;840:139–52. doi: 10.1111/j.1749-6632.1998.tb09558.x. [DOI] [PubMed] [Google Scholar]
- 97.Hayley S, Lacosta S, Merali Z, van Rooijen N, Anisman H. Central monoamine and plasma corticosterone charges induced by a bacterial endotoxin: Sensitization and cross-sensitization effects. Eur J Neurosci. 2001;13:1155–65. doi: 10.1046/j.0953-816x.2001.01496.x. [DOI] [PubMed] [Google Scholar]
- 98.Shawcross DL, Davies NA, Williams R, Jalan R. Systemic inflammatory response exacerbates the neuropsychological effects of induced hyperammonemia in cirrhosis. J Hepatol. 2004;40:247–54. doi: 10.1016/j.jhep.2003.10.016. [DOI] [PubMed] [Google Scholar]
- 99.McKinley MJ, McAllen RM, Davern P, et al. The sensory circumventricular organs of the mammalian brain. Adv Anat Embryol Cell Biol. 2003;172:III–Xii. 1–122. doi: 10.1007/978-3-642-55532-9. [DOI] [PubMed] [Google Scholar]
- 100.Vallieres L, Rivest S. Regulation of the genes encoding interleukin-6, its receptor, and gp130 in the rat brain in response to the immune activation lipopolysaccharide and proinflammatory cytokine interleukin-1beta. J Neurochem. 1997;69:1668–83. doi: 10.1046/j.1471-4159.1997.69041668.x. [DOI] [PubMed] [Google Scholar]
- 101.Van Dam AM, De Vries HE, Kuiper J, et al. Interleukin-1 receptors on rat brain endothelial cells: A role in neuroimmune interaction? FASEB J. 1996;10:351–6. doi: 10.1096/fasebj.10.2.8641570. [DOI] [PubMed] [Google Scholar]
- 102.Nadeau S, Rivest S. Effects of circulating tumor necrosis factor on the neuronal activity and expression of the genes encoding the tumor necrosis factor receptors (p55 and p75) in the rat brain: A view from the blood-brain barrier. Neuroscience. 1999;93:1449–64. doi: 10.1016/s0306-4522(99)00225-0. [DOI] [PubMed] [Google Scholar]
- 103.Swain MG, Beck P, Rioux K, Le T. Augmented interleukin-1beta-induced depression of locomotor activity in cholestatic rats. Hepatology. 1998;28:1561–5. doi: 10.1002/hep.510280616. [DOI] [PubMed] [Google Scholar]
- 104.Cook NF, Boore JR. Managing patients suffering from acute and chronic fatigue. Br J Nurs. 1997;6:811–5. doi: 10.12968/bjon.1997.6.14.811. [DOI] [PubMed] [Google Scholar]
- 105.Graydon JE, Bubela N, Irvine D, Vincent L. Fatigue-reducing strategies used by patients receiving treatment for cancer. Cancer Nurs. 1995;18:23–8. [PubMed] [Google Scholar]
- 106.Wearden AJ, Morriss RK, Mullis R, et al. Randomised, double-blind, placebo-controlled treatment trial of fluoxetine and graded exercise for chronic fatigue syndrome. Br J Psychiatry. 1998;172:485–90. doi: 10.1192/bjp.172.6.485. Erratum in 1998;173:89. [DOI] [PubMed] [Google Scholar]
- 107.Sharpe M. Cognitive behavior therapy for chronic fatigue syndrome: Efficacy and implications. Am J Med. 1998;105(Suppl 3A):104S–9S. doi: 10.1016/s0002-9343(98)00170-3. [DOI] [PubMed] [Google Scholar]
- 108.Fry AM, Martin M. Fatigue in the chronic fatigue syndrome: A cognitive phenomenon. J Psychosom Res. 1996;41:415–26. doi: 10.1016/s0022-3999(96)00190-0. [DOI] [PubMed] [Google Scholar]
- 109.Whiting P, Bagnall AM, Sowden AJ, Cornell JE, Mulrow CD, Ramirez G. Interventions for the treatment and management of chronic fatigue syndrome: A systematic review. JAMA. 2001;286:1360–8. doi: 10.1001/jama.286.11.1360. Erratum in 2002;287:1401. [DOI] [PubMed] [Google Scholar]
- 110.Cordoba J, Cabrera J, Lataif L, Penev P, Zee P, Blei AT. High prevalence of sleep disturbance in cirrhosis. Hepatology. 1998;27:339–45. doi: 10.1002/hep.510270204. [DOI] [PubMed] [Google Scholar]
- 111.Becker PM, Schwartz JR, Feldman NT, Hughes RJ. Effect of modafinil on fatigue, mood, and health-related quality of life in patients with narcolepsy. Psychopharmacology (Berl) 2004;171:133–9. doi: 10.1007/s00213-003-1508-9. [DOI] [PubMed] [Google Scholar]
- 112.Rammohan KW, Rosenberg JH, Lynn DJ, Blumenfeld AM, Pollak CP, Nagaraja HN. Efficacy and safety of modafinil (Provigil) for the treatment of fatigue in multiple sclerosis: A two center phase 2 study. J Neurol Neurosurg Psychiatry. 2002;72:179–83. doi: 10.1136/jnnp.72.2.179. [DOI] [PMC free article] [PubMed] [Google Scholar]