

Abstract
Isolated fractures of the trapezoid are rare. Of all of the fractures of the carpus, the most common is the scaphoid, which represents 68.2% of all carpal fractures (Papp, Orthop Clin N Am 38:251–60, 2007). In contrast, trapezoid fractures represent 0.4% of all carpal injuries. Because it is an infrequently fractured carpal bone, there is a wide variety of treatment plans, including rest, immobilization, and surgery (Green and Pederson, Green’s Operative Hand Surgery, Elsevier, Philadelphia, 759 pp, 2005). In this report, we describe a patient who presented with an isolated fracture of the trapezoid that was successfully treated with cast immobilization and had a full functional recovery.
Keywords: Trapezoid, Fracture, Carpal, Wrist, Hand surgery
Case Report
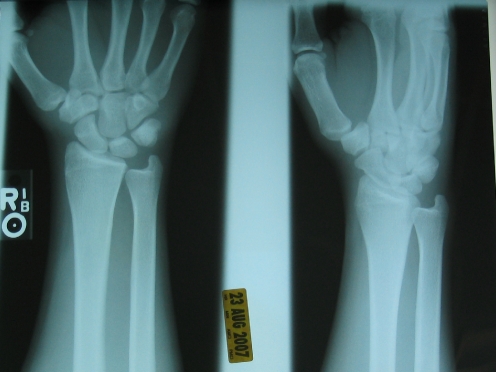
The patient was a 19-year-old right hand dominant male who presented to our facility 2 1/2 weeks after his injury. On the date of injury, the patient was roughhousing with a friend and, while trying to punch him, he hyperextended his right wrist and then heard a crack. He subsequently sought treatment from his primary care physician (PCP) 3 days later because of persistent pain and swelling. Three-view radiographs of the wrist did not show a fracture. The patient was given a wrist lacer splint for comfort.
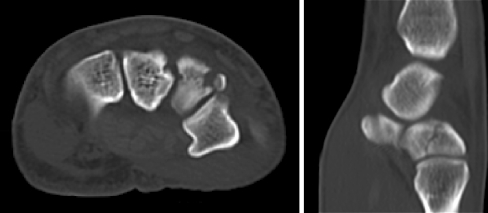
In a follow-up visit with his PCP, the patient continued to complain of wrist pain especially with range of motion. A computed tomography (CT) scan with 3-D reconstruction of the right wrist was obtained. It showed an isolated comminuted fracture of the trapezoid, and the patient was sent to the hand surgery clinic for consultation.
On physical examination of the affected right upper extremity, the patient had moderate swelling of the dorsal and volar surfaces of the wrist. There was tenderness to palpation at the base of the second metacarpal. Because of pain, the patient had limited wrist flexion, wrist extension, and radial–ulnar deviation. He had no crepitus or clicking on range of motion. He had full finger flexion and no extension lag. CT scan of the right wrist showed a nondisplaced proximal comminuted trapezoid bone fracture.

The patient was placed in a short arm cast for 6 weeks with the wrist in 20° of extension and the metacarpophalangeal and interphalangeal joints free and then progressed to a splint for the next 2 weeks. He also began hand therapy, which included passive and active range of motion.
After 8 weeks, the pain and swelling resolved completely and he recovered his range of motion. He was eventually able to return to his job in construction. He completed physical therapy with 68° of wrist extension on the right and 65° on the left. He had wrist flexion of 90° on both the right and left. Radial deviation was 35° on the right and 40° on the left. Ulnar deviation was 35° on both the right and left. He had an extremely symmetric wrist in terms of function between the injured and noninjured wrists. In a follow-up with the patient 8 months later, the patient stated that he remained pain-free and continued to be employed in construction.
Discussion
The trapezoid is the least commonly fractured carpal bone [8]. The anatomy of the trapezoid places it in a fairly protected position. Distally, it forms a stable, relatively immobile joint with the second metacarpal [4]. From this point, it is bound by strong ligaments to the trapezium radially, the capitate ulnarly, and the scaphoid proximally. Its shape is like a keystone, and it is two times wider dorsally than palmarly [2]. Gelberman and Gross showed that although the trapezoid has multiple sources of blood supply, it lacks internal anastamoses [3]. Osteonecrosis of the trapezoid has been reported; however, it is less common than osteonecrosis of the scaphoid [10].
Injury to the trapezoid can occur through axial force applied to the second metacarpal base. In our patient’s case, it appears that axial loading in addition to wrist hyperextension occurred when the patient delivered a punching blow. Fracture–subluxations are not uncommon. In these injuries, the force causes palmar flexion of the index metacarpal and displaces the trapezoid dorsally and proximally. Although closed reduction and percutaneous pinning can be attempted to reduce and fix these fracture–dislocations, open reduction and internal fixation may be necessary. Direct trauma to the metacarpal base, rather than axial compression, can also produce a trapezoid fracture.
Patients with trapezoid fractures complain of pain at the base of the second metacarpal. They may also complain of pain in the region of the snuffbox [5]. On physical exam, they can have wrist swelling and decreased range of motion of the wrist because of pain. Unfortunately, these fractures can be difficult to identify with plain radiography because of both overlapping bones which obscure the fracture line and the fragment size, as in our case. Such fragments are also rarely displaced because of the intercarpal and carpometacarpal ligaments that support them. Brismar found that zero of ten patients with a positive bone scan for a trapezoid fracture had evidence of the fracture on plain radiograph [1]. Waizenegger found that out of 84 patients with snuffbox pain and normal radiographs, six had fractures of the trapezium or trapezoid [11]. For this reason, special oblique and carpal tunnel views have been recommended. Bone scans, magnetic resonance imaging, and CT are useful adjuncts to attaining a definitive diagnosis and provide greater information regarding the nature of the fracture and can assist with the formulation of a treatment plan.
Because of the rarity of isolated trapezoid fractures, a standard treatment has not been established. There have been three other cases reported of truly isolated trapezoid fractures [5–7]. In addition, in the last two decades, there have been three additional case reports of trapezoid fracture as part of more global hand and wrist injuries [9, 12, 13]. Satisfactory treatment patterns have included cast immobilization, open reduction and internal fixation, and excision of smaller displaced fragments. Displacement of up to 2 mm has been successfully treated nonoperatively [5]. Nonunion of the trapezoid has been successfully treated with open reduction, internal fixation, bone grafting, and excision of the small comminuted fragments.
In summary, we treated a rare case of isolated fracture of the trapezoid with cast immobilization. Subsequent clinical visits showed resolution of pain and achievement of full recovery of wrist function and return to work.
References
- 1.Brismar J. Skeletal scintigraphy of the wrist in suggested scaphoid fracture. Acta Radiol 1988;29:101–7. [PubMed]
- 2.Cohen M. Fractures of the carpal bones. Hand Clin 1997;13(4):587–99. [PubMed]
- 3.Gelberman G. The vascularity of the wrist. Clin Orthop Relat Res 1986;202:40–9. [PubMed]
- 4.Green H, Pederson W. Green’s operative hand surgery. Philadelphia: Elsevier; 2005. 759 p.
- 5.Jeong GK, Lester B. Isolated fracture of the trapezoid. Am J Orthop 2001;30:228–30. [PubMed]
- 6.Miyawaki T, Kobayashi M, Matsuura S, Yanagawa H, Imai T, Kurihara K. Trapezoid bone fracture. Ann Plast Surg 2000;44:444–6. [DOI] [PubMed]
- 7.Nagumo A, Toh S, Tsubo K, Ishibashi Y, Sasaki T. An occult fracture of the trapezoid bone: a case report. J Bone Joint Surg Am 2002;84:1025–7. [DOI] [PubMed]
- 8.Papp S. Carpal bone fractures. Orthop Clin N Am 2007;38:251–60. [DOI] [PubMed]
- 9.Pruzansky M, Arnold L. Delayed union of fractures of the trapezoid and body of the hamate. Orthop Rev 1987;16(9):624–8. [PubMed]
- 10.Rhoades CE, Reckling FW. Palmar dislocation of the trapezoid. J Hand Surg 1983;8(1):85–8. [DOI] [PubMed]
- 11.Waizenegger M, Wastie ML, Barton J, Davis TRC. Scintigraphy in the evaluation of the “clinical” scaphoid fracture. J Hand Surg Br 1994;19B(6):750–3. [DOI] [PubMed]
- 12.Watanabe H, Hamada Y, Yamamoto Y. A case of old trapezoid fracture. Arch Orthop Trauma Surg 1999;119:356–7. [DOI] [PubMed]
- 13.Yasuwaki Y, Nagata Y. Fracture of the trapezoid bone: a case report. J Hand Surg Am 1994;19A(3):457–9. [DOI] [PubMed]