

Abstract
A 35-year-old man's vision had progressively deteriorated over a 3-month period. His left visual acuity was 5/20. Enhanced orbital computed tomographic (CT) scans revealed a fusiform dilatation of the ophthalmic artery in the left optic canal. Cerebral Angiography revealed a fusiform aneurysm on the left ophthalmic artery in the optic canal, measuring 6.2 × 4.6 mm in size. Four days after admission, visual acuity dropped to hand-motion. Endovascular treatment was chosen and a microcatheter was guided into the proximal segment of the ophthalmic artery. Using 4 detachable coils, parent artery occlusion was done. Three months after the intervention, the visual acuity in his left eye improved to 20/20. Dramatic recovery of visual acuity is exceptional with an ophthalmic artery trunk aneurysm. When an occlusion of the proximal ophthalmic artery is the only treatment option in such a situation, the endovascular occlusion of the proximal ophthalmic artery is quite feasible in the sense that it does not require any optic nerve manipulation.
Keywords: Detachable coil, Fusiform aneurysm, Intracanalicular portion, Ophthalmic artery trunk aneurysm
INTRODUCTION
"Ophthalmic artery aneurysm" usually refers to a carotid-ophthalmic junction aneurysm3). Due to its rarity, only a small number of true ophthalmic artery aneurysms have been reported. Intracanalicular ophthalmic artery aneurysms are even rarer, with only one previously reported case12).
Because the chance of rupture is not high9,12), the benign nature of an aneurysm with minor symptoms in this location has been previously noted2). However, since the ophthalmic artery trunk runs in intimate proximity to optic nerve, these aneurysms often create vision-related symptoms, which respond poorly to surgical treatments4,10,13). We report a case of a fusiform intracanalicular ophthalmic artery aneurysm presented with progressive visual loss, which recovered dramatically after coiling.
CASE REPORT
A 35-year-old man with a 3-month history of progressive visual loss was transferred to the neurosurgical department after an initial impression of retrobulbar optic neuropathy at a local clinic. He reported 2 minor traffic accidents, but past medical records and radiologic study results were not available. Visual acuity was 20/20 in the right eye and 5/200 in his left. A relative afferent pupillary defect of the left eye was noted. Ocular pressure was normal. Biomicroscopic and ophthalmoscipic examination revealed no remarkable abnormal findings. Fluorescein angiography did not show any leakage or delayed filling. Time to P1 of flash visual evoked potential was delayed to 159 ms in the left eye compared to 132 ms in the right eye. His visual field was not checkable due to his failing vision. An orbit magnetic resonance image (MRI) revealed a signal void in the left optic canal (Fig. 1A). MR angiography showed an aneurysm in the proximal portion of the left internal carotid artery (ICA) ophthalmic segment (Fig. 1B). An ophthalmic artery aneurysm was suspected. An orbital CT with enhancement revealed a fusiform dilatation of the ophthalmic artery in the left optic canal (Fig. 1C). A widened left optic canal with ethomoidal bony erosion was observed (Fig. 1C, D).
Fig. 1.

A : Axial T2-weighted magnetic resonance image demonstrating a signal void in the left optic canal (arrow). B : Magnetic resonance angiography revealing an aneurysm on the left ophthalmic artery trunk. C : Axial enhanced orbital computed tomographic scan showing a fusiform dilatation of the left ophthalmic artery with bony erosion of the ethmoidal wall (arrow). D : Coronal orbital computed tomography illustrating an enlarged left optic canal (arrow).
Digital subtraction cerebral angiography with left carotid injection showed a fusiform ophthalmic artery aneurysm in the intracanalicular segment, measuring 6.2 × 4.6 mm in size (Fig. 2A). External carotid artery (ECA) collateral from the infraorbital artery was well maintained. Four days after admission, his left visual acuity dropped to hand-motion status. The fusiform nature and the intracanalicular location of the ophthalmic artery aneurysm made a usual neck clipping procedure difficult. The only remaining option was the parent artery occlusion either by surgery or endovascular intervention. The effect of obliterating the parent artery by coil seemed equally effective as surgical occlusion. Since it does not require direct manipulation of optic nerve, endovascular treatment was chosen. A 6F sheath was inserted in the right femoral artery and a 6F guiding catheter was placed high to the left cervical ICA. Using a microcatheter (Excelsior 10, Boston Scientific), the proximal ophthalmic artery was selected (Fig. 2B).
Fig. 2.

A : Cerebral angiography of the left internal carotid artery depicting a fusiform aneurysm of the left ophthalmic artery trunk. Luminal irregularities are noted on proximal segments of left ophthalmic artery. B : The distal tip of a microcatheter is located just proximal to the aneurysm. C : Detached coils are visible on the proximal ophthalmic artery during the procedure. D : After the ophthalmic artery occlusion, the aneurysm is no longer filled and antegrade flow is not observed. E : Late arterial phase of left external carotid angiogram shows retrograde collateral flows which constitute choroidal crescent (arrow heads). Retrograde filling of the intraorbital ophthalmic artery is also noted (arrow).
With 4 platinum coils (GDC, Boston scientific), the proximal segment of the ophthalmic artery harboring a fusiform aneurym was obliterated (Fig. 2C). Postintervention angiography revealed complete occlusion of the left ophthalmic artery (Fig. 2D), and choroidal crescent supplied by the external carotid collaterals (Fig. 2E).
In following day, visual acuity of the left eye improved to finger-count status and the pupillary reflex was prompt. Four days later, his visual acuity increased to 20/25. Fluorescein angiography performed after 1 week demonstrated no delayed filling or ischemic change. Time to P1 of pattern reversal visual evoked potential was still delayed to 130 ms in the left eye compared to 100 ms in the right eye. Three months after the intervention, a control cerebral angiography was performed and showed a well-obliterated proximal ophthalmic artery (Fig. 3). After 2 years, MR angiography showed no evidence of recannalization or regrowth of the aneurysm. His vision was 20/20 in both eyes.
Fig. 3.
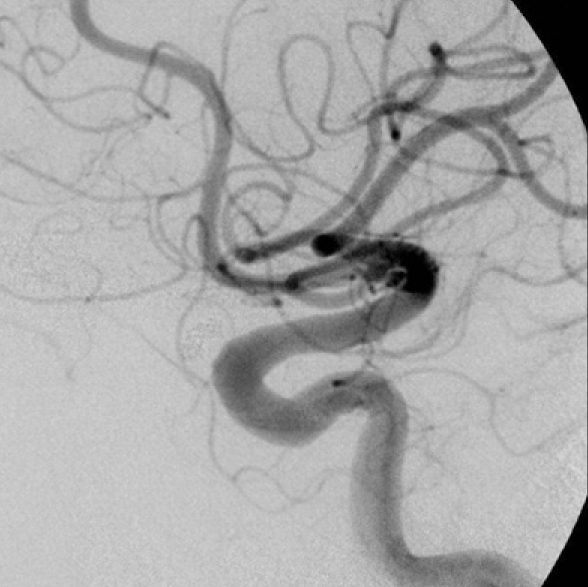
Three months after the intervention, cerebral angiography illustrates well-obliterated left ophthalmic artery.
DISCUSSION
The ophthalmic artery is composed of three segments; intracranial, intracanalicular and orbital segments11). Unlike usual ophthalmic artery aneurysms, which arise from the junction of the ICA trunk and ophthalmic artery, an ophthalmic artery trunk aneurysm is extremely rare10,14). There have been a small number of reported cases of intraorbital7,8,10,11,13,15) and intracranial5,7,14,16) segment aneurysms. However, only one case of intracanalicular segment aneurysms has been reported so far12).
Previously reported aneurysms in the intracranial and intraorbital segments have been often accompanied by arteriovenous fistula9), arteriovenous malformation9), moyamoya disease7), evident trauma1,13) or with aneurysms in different locations2,16). In the current case, luminal irregularities (Fig. 2A), the ectatic and stenotic segments on the proximal and distal portion of aneurysm (Fig. 2A) suggest common features of the dissecting aneurysm. Although the patient reported two previous traffic accidents, there was no evidence of skull fracture or deformed orbital structure caused by previous traumas. This aneurysm must have enlarged very slowly, slowly enough to create the total erosion of the ethmoidal wall and a widening of the optic canal (Fig. 1C, D).
The symptoms of a ruptured ophthalmic artery trunk aneurysm depend on its localization. When they rupture, intracranial segment aneurysms cause subarachoid hemorrhage (SAH)16,18), whereas intraorbital segment aneurysms may result in intraorbital bleeding10). However, the incidence of bleeding is known to be low, and the benign nature of this aneurysm has previously been commented on2,15). Most commonly, they present with eye-related symptoms, such as visual disturbance14,15), visual field defect14,15) and sometimes exophthalmos10,13). Visual disturbance is more likely to develop with an intracanalicular segment aneurysm12). In the optic canal, an aneurysm doesn't have enough space to expand, and the intracanalicular optic nerve is known to have a poor blood supply from the superior hypophyseal artery, not from the ophthalmic artery itself17). Visual disturbance associated with ophthalmic trunk aneurysms responds poorly to treatment. Once it starts, it is difficult to reverse. Of the treated ophthalmic artery trunk aneurysm cases where the initial symptom was visual disturbance4,9-15), postoperative visual function was better than the preoperative state in only one case9), where preoperative visual disturbance had been mild. Two reported cases showed similar postoperative visual acuity results to the preoperative state11,12). With these clinical characteristics, ophthalmic trunk aneurysm associated with the progressive visual disturbance should be treated urgently.
In the current case, the fusiform nature and intracanalicular location precluded the usual neck clipping procedure. The only remaining option was the parent artery occlusion either by surgery or endovascular intervention. There are numerous anastomoses between the external carotid and ophthalmic artery, and this collateral blood flow can prevent ocular ischemias after occlusion of the internal carotid and ophthalmic artery in 90% of cases6). However, surgical occlusion of the ophthalmic artery has not been so fruitful in previous reports. The location immediately near the optic nerve makes it difficult to ligate the pathology and unroofing the optic canal may cause additional damage to the nerve14). In a case with an intraorbital segment aneurysm reported by Ernemann et al.4), postoperative angiography showed a choroidal crescent supplied by the external carotid collaterals, but the patient's visual functions did not improve4). Ogawa et al.11) trapped and resected the intraorbital segment aneurysm. Four months after the surgery, visual acuity was still at finger-count status, even though a branch of the right external carotid artery fed the choroidal crescent. Piche et al.12) failed to accomplish occlusion of the proximal ophthalmic artery because of the adherence to the inferior aspect of the optic nerve. Later, they occluded the ophthalmic artery with endovascular detachable coils, which yielded a preoperative baseline visual acuity status12).
Upon reviewing the aforementioned previous reports, the recovery of visual acuity from hand-motion status is very exceptional. It is not easy to conclude which factors contributed to the reversal of the visual symptoms in the current case. It is believed that endovascular occlusion played a role, because this obviated the optic nerve manipulation.
CONCLUSION
We reported a case of a fusiform intracanalicular ophthalmic artery aneurysm presented with decreased visual acuity which improved completely after parent artery occlusion by coiling.
References
- 1.Beiran I, Dori D, Pikkel J, Goldsher D, Miller B. Recurrent retinal artery obstruction as a presenting symptom of ophthalmic artery aneurysm : a case report. Graefes Arch Clin Exp Ophthalmol. 1995;233:444–447. doi: 10.1007/BF00180950. [DOI] [PubMed] [Google Scholar]
- 2.Dehdashti AR, Safran AB, Martin JB, Rufenacht DA, de Tribolet N. Intraorbital ophthalmic artery aneurysm associated with basilar tip saccular aneurysm. Neuroradiology. 2002;44:600–603. doi: 10.1007/s00234-002-0786-y. [DOI] [PubMed] [Google Scholar]
- 3.Drake CG, Vanderlinden RG, Amacher AL. Carotid-ophthalmic aneurysms. J Neurosurg. 1968;29:24–31. doi: 10.3171/jns.1968.29.1.0024. [DOI] [PubMed] [Google Scholar]
- 4.Ernemann U, Freudenstein D, Pitz S, Naegele T. Intraorbital aneurysm of the ophthalmic artery : a rare cause of apex orbitae compression syndrome. Graefes Arch Clin Exp Ophthalmol. 2002;240:575–577. doi: 10.1007/s00417-002-0503-x. [DOI] [PubMed] [Google Scholar]
- 5.Jain KK. Saccular aneurysm of the ophthalmic artery. Am J Ophthalmol. 1970;69:997–998. doi: 10.1016/0002-9394(70)91045-7. [DOI] [PubMed] [Google Scholar]
- 6.Johnson HC, Walker AE. The angiographic diagnosis of spontaneous thrombosis of the internal and common carotid arteries. J Neurosurg. 1951;8:631–659. doi: 10.3171/jns.1951.8.6.0631. [DOI] [PubMed] [Google Scholar]
- 7.Kawaguchi S, Sakaki T, Okuno S, Uchiyama Y, Nishioka T. Peripheral ophthalmic artery aneurysm. Report of two cases. J Neurosurg. 2001;94:822–825. doi: 10.3171/jns.2001.94.5.0822. [DOI] [PubMed] [Google Scholar]
- 8.Kikuchi K, Kowada M. Case report : saccular aneurysm of the intraorbital ophthalmic artery. Br J Radiol. 1994;67:1134–1135. doi: 10.1259/0007-1285-67-803-1134. [DOI] [PubMed] [Google Scholar]
- 9.Kleinschmidt A, Sullivan TJ, Mitchell K. Intraorbital ophthalmic artery aneurysms. Clin Experiment Ophthalmol. 2004;32:112–114. doi: 10.1046/j.1442-9071.2004.00773.x. [DOI] [PubMed] [Google Scholar]
- 10.Meyerson L, Lazar SJ. Intraorbital aneurysm of the ophthalmic artery. Br J Ophthalmol. 1971;55:199–204. doi: 10.1136/bjo.55.3.199. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 11.Ogawa A, Tominaga T, Yoshimoto T, Kiyosawa M. Intraorbital ophthalmic artery aneurysm : case report. Neurosurgery. 1992;31:1102–1104. doi: 10.1227/00006123-199212000-00017. discussion 1104. [DOI] [PubMed] [Google Scholar]
- 12.Piche SL, Haw CS, Redekop GJ, Heran MK. Rare intracanalicular ophthalmic aneurysm : endovascular treatment and review of the literature. AJNR Am J Neuroradiol. 2005;26:1929–1931. [PMC free article] [PubMed] [Google Scholar]
- 13.Rahmat H, Abbassioun K, Amirjamshidi A. Pulsating unilateral exophthalmos due to traumatic aneurysm of the intraorbital ophthalmic artery. Case report. J Neurosurg. 1984;60:630–632. doi: 10.3171/jns.1984.60.3.0630. [DOI] [PubMed] [Google Scholar]
- 14.Raitta C. Ophthalmic artery aneurysm causing optic atrophy and enlargement of the optic foramen. Br J Ophthalmol. 1968;52:707–709. doi: 10.1136/bjo.52.9.707. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 15.Rubinstein MK, Wilson G, Levin DC. Intraorbital aneurysms of the ophthalmic artery. Report of a unique case and review of the literature. Arch Ophthalmol. 1968;80:42–44. doi: 10.1001/archopht.1968.00980050044007. [DOI] [PubMed] [Google Scholar]
- 16.Sato S, Suga S, Ohira T, Takayama H, Kawase T. Aneurysm of the ophthalmic artery trunk. Acta Neurochir (Wien) 1999;141:321–322. doi: 10.1007/s007010050304. [DOI] [PubMed] [Google Scholar]
- 17.van Overbeeke J, Sekhar L. Microanatomy of the blood supply to the optic nerve. Orbit. 2003;22:81–88. doi: 10.1076/orbi.22.2.81.14316. [DOI] [PubMed] [Google Scholar]
- 18.Yanaka K, Matsumaru Y, Kamezaki T, Nose T. Ruptured aneurysm of the ophthalmic artery trunk demonstrated by three-dimensional rotational angiography : case report. Neurosurgery. 2002;51:1066–1069. doi: 10.1097/00006123-200210000-00038. discussion 1069-1070. [DOI] [PubMed] [Google Scholar]