

Abstract
Background
The purpose of our study was to investigate the impact of distracting noise on the performance on a simulated orthopedic bone drilling skill when that noise blocks routine auditory feedback associated with the sounds of the drill.
Methods
Medical students (n = 11), intermediate residents (postgraduate years 3–5, n = 10) and surgeons (n = 8) each drilled 20 bicortical holes in a femur bone from a lamb: 10 holes without and 10 holes with the presence of distracting noise. We quantified surgical outcome in the form of plunge depth using computer-assisted objective methods.
Results
Novice participants plunged more than did the intermediate trainees and surgeons (p < 0.001). With the addition of distracting noise, the plunges of both intermediate residents and surgeons were affected.
Conclusion
Distracting noise impairs orthopedic bone drilling performance, and the ability to use drilling sounds to guide drilling motions is part of surgical expertise.
Abstract
Contexte
Nous voulions déterminer l'impact de la distraction sonore sur l'exécution d'une simulation de forage orthopédique dans un os lorsque le bruit bloque la rétroaction auditive habituelle associée au son de la perceuse.
Méthodes
Des étudiants en médecine (n = 11), des résidents de niveau intermédiaire (années postdoctorales 3 à 5, n = 10) et des chirurgiens (n = 8) ont foré 20 trous bicorticaux dans un os de fémur d'agneau : 10 trous sans distraction sonore et 10 en présence d'une distraction sonore. Pour quantifier le résultat chirurgical, nous avons mesuré la profondeur du trou au moyen de méthodes objectives assistées par ordinateur.
Résultats
Les participants novices ont percé un trou plus profond que les stagiaires de niveau intermédiaire et les chirurgiens (p < 0,001). L'ajout de la distraction sonore a eu un effet sur la profondeur du trou percé par les résidents de niveau intermédiaire et les chirurgiens.
Conclusion
La distraction sonore nuit à l'exécution du perçage orthopédique des os, et la capacité à utiliser les bruits de perçage pour guider les mouvements de perçage fait partie du savoir-faire chirurgical.
Sound levels in operating rooms are elevated.1–3 Commonly reported levels range from 66 dB during general surgery procedures4 to 83 dB during mastoidectomy5 to more than 140 dB in orthopedic surgery.3 Such elevated noise levels may not only present potential risks to patient health and safety,6–8 but may also have a detrimental effect on the technical performance of the surgeon.7,9
Moorthy and colleagues3 showed that high levels of noise did not adversely affect surgeons' performance of laparoscopic tasks. They cited the high levels of concentration required for performing this complex task as an explanation for their findings. Although this explanation is plausible, it conflicts with evidence that suggests performing psychomotor skills involving memory, 2-handed coordination,10 simple and complex reaction times, timed movements and proofreading skills11–13 are typically affected by distracting noise. The degree of this effect depends on 3 factors: the amount of auditory feedback required for optimal performance of the skill, the overall complexity of the skill and the participant's familiarity or expertise with the given skill.14
Orthopedic surgery often involves power tools and hard tissue, where surgeon–tissue interaction produces sounds that may be used to facilitate surgical performance. For example, drilling through a bicortical bone produces a drilling pitch that can be used to predict the density of the bone material. During drilling, the surgeon must be able to quickly cease any advancement of the drill when the full thickness of bone has been traversed to avoid potential injury to the underlying soft tissue structures such as nerves, arteries and veins. Because much of the bone's thickness is often concealed by soft tissue, visual information about when to stop the drilling action cannot often be used. Therefore, through practice, the surgeon must adapt to this challenging environment by relying on other sensory cues, such as auditory information in the form of drill pitch.
The primary purpose of our study was to test whether the orthopedic bone drilling skill depends partially on the availability of auditory information about the drilling pitch and whether this dependence changes as a function of expertise. However, before addressing this primary purpose it was important to establish construct validity of the measures employed. For this validation purpose we hypothesized that the computer-based measures of technical performance would be able to discern expert, intermediate and novice performance. After establishing the construct validity of the measures, we tested the primary purpose by comparing the performances of 2 groups of trainees, as well as experts, while they were drilling through a bicortical long bone with and without a masking noise, which we introduced to mask drilling sounds. We hypothesized that when compared with normal drilling conditions, the addition of a masking noise would affect expert performance to a greater degree than that of intermediate and novice trainees. Finally, we also hypothesized that we would be able to observe initial changes in performance for all groups as a function of familiarization with the bone model.
Methods
Participants
To address the 3 experimental hypotheses, we used control design with group (between-subject), noise (within-subject) and trial as factors. We stratified participants to each of the identified groups based on their training levels. The novice group comprised 11 first-year medical students (4 women, 7 men). The intermediate group comprised 10 male postgraduate orthopedic trainees (3 postgraduate year [PGY] 3, 6 PGY4, 1 PGY5). The expert group comprised 8 male university faculty members in orthopedic surgery. All participants were right-handed, as determined using Oldfield's questionnaire.15 All participants performed under control (no noise) and experimental (masking noise) conditions in this specific order. Before we began the study, each participant provided informed consent. The University of Toronto Research Ethics Board approved the ethics protocol for our study.
We recruited the novice participants from an undergraduate medical class using an email recruitment method. They were scheduled to participate in the study within a single week in the evenings. The intermediate and expert participants volunteered their time during an orthopedic skills course that was offered in the evening and did not contain drilling as one of the skills being practised. For all 3 groups, participation was voluntary, and the experiment was performed in a separate room away from the course.
A priori power calculations based on our earlier results16 indicated that the number of participants required to achieve a power greater than 0.80 and the expected 15-mm (standard deviation [SD] 8 mm) difference between the means under the 2 experimental sound conditions, an α of 0.05 (2-tailed) and a β of 0.20 was 8 participants per group.
Technique
Individual participants positioned themselves facing the experimental apparatus. If necessary, we provided a footstool for participants to achieve the most comfortable height for the skill. The bone model used was the femur of a lamb. It was secured by a custom-designed bone holder attached to a force sensor (200 Hz sampling frequency and 0.0025 N resolution, F/T Gamma; ATI Industrial Automation), which measured the reactive forces applied to the bone during the drilling. The bone was dissected and therefore free of soft tissue, but we positioned it on the bone holder so participants could not judge the depth of penetration based on visual cues about the bone thickness. We used an Optotrak 3-dimensional motion analysis system (200 Hz sampling frequency and 0.001 mm spatial resolution, Northern Digital Inc.) to monitor the drill movements. We affixed a position marker to the drill handle. We filtered all force and position profiles with a custom programmed 15 Hz dual pass Butterworth filter, which we used later to identify the magnitude of plunge depth.
We used 5 nitrogen-powered surgical drills (Series 4 Drill/Reamer, Model 5067 with 100 PSI pressure, equipped with a 3.5-mm Zimmer drill bit; Zimmer Inc.). We randomly assigned the drills to participants. Because they were reused, it was likely that there was variation in the sharpness of the drill bits. However, since the drills were randomly assigned to participants, it was assumed that there was no bias for any particular group.
Using the surgical drill, participants drilled 20 bicortical holes on a lamb femur, 10 under typical circumstances (no noise) and 10 while wearing headphones providing broadband noise at 85–90 dB to block the sound of the drill (masking noise). We instructed the participants to begin each drill with the drill bit held about 2 mm above the bone. We gave them no specific time restrictions, but we instructed them to be as precise and accurate as possible. For the purpose of this study, we defined broadband noise as a sound whose frequency spectrum had no dominant peaks. That is, in the frequency domain, a broadband noise has a continuous spectrum, meaning it is present at all frequencies in a given range and lacks a discernible pitch. We used this sound to mask any changes in the pitch produced by the drilling actions. We asked all participants to wear earplugs to mask any additional noise, ensuring their inability to hear the drilling sounds, and to avoid any possible discomfort. We conducted the study in an artificial laboratory setting that resembled real operating room sound conditions. The absence of noise is uncommon in real operating rooms, even when the surgeon prefers quiet, so we used active monitors, computers, background conversations and other equipment noise to control for this factor.
The order of the 2 noise conditions was consistent for all participants, with the no noise condition always preceding the masking noise condition. We selected this order for 2 reasons. First, all participants needed to hear the drilling sounds produced during drilling to form sensory-motor memories associating these drilling sounds with bone characteristics. Therefore, randomization of the noise conditions could have led to a scenario in which the appropriate mapping between drilling sounds and bone density did not take place before we masked these sounds. Second, based on the literature we expected that repetitive practice would lead to initial improvements in performance across trials,16 which could have confounded the effects of masking noise on performance. That is, any decrements in performance observed because of the masking noise could have been offset by learning effects.
Outcome measure
We considered the previously validated measure of plunge depth,16 defined as the displacement of the drill bit after drilling through the outer side of the bone, to be the most clinically relevant outcome measure. We calculated plunge depth as the difference between the instantaneous position of the marker on the drill when the force applied by the drill bit to the bone dropped toward zero (indicating that the drill had penetrated the final bone cortex) and the final lowest position of this marker before the drill bit was retrieved from the hole (change in drill bit movement direction).
Statistical analysis
We analyzed plunge depth using a mixed 3-way analysis of variance (ANOVA) with expertise (novice, intermediate and expert), noise condition (no noise, masking noise) and trial (1–10) as factors. In addition, we analyzed the effects significant at p < 0.05 using the Tukey post hoc method for the comparison of means.
Results
Before evaluating the effects of masking noise on surgical performance, we assessed the construct validity of the computer-based measurement methods. We hypothesized that our measures would be able to discern novice from intermediate and expert performers. In line with this hypothesis, the plunge depth discerned novice sfrom intermediates and experts (F2–26 = 16.74; p < 0.05); however, there were no differences between experts and intermediate trainees.
Next, we hypothesized that the experts would be affected by the addition of the masking noise to a greater extent than novice participants. This hypothesis was supported: the novice participants maintained their performance levels in the presence of masking noise, whereas the intermediate trainees and experts plunged more (F2–26 = 4.00; p < 0.05) under the masking noise condition compared with the normal auditory condition (see Fig. 1).
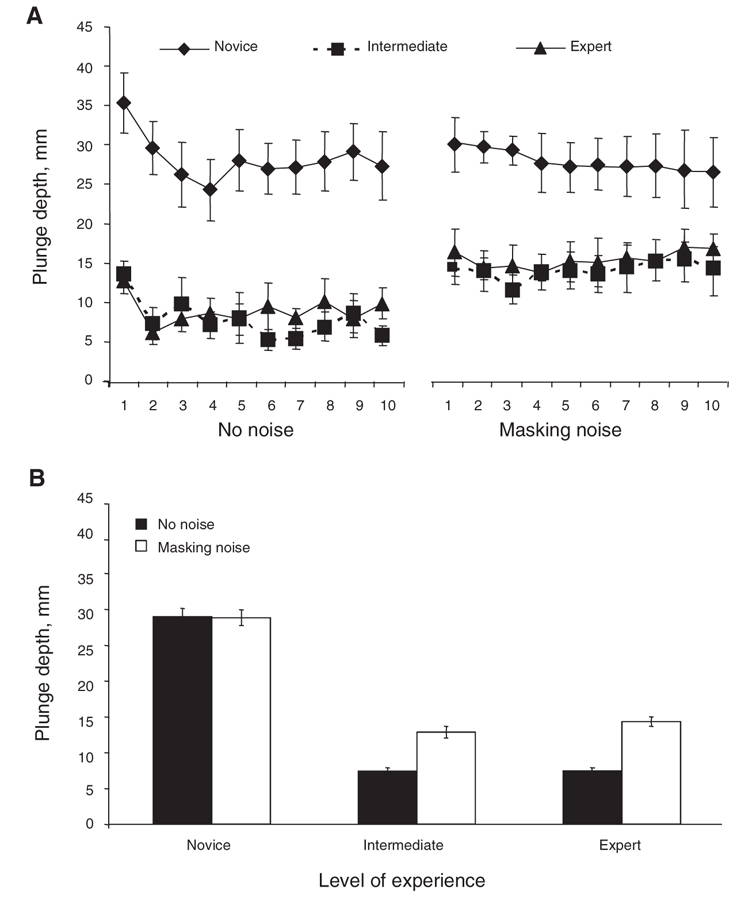
FIG. 1. (A) A summary of the amount of plunge as a function of expertise and noise condition for each of the 10 trials. (B) The graph shows plunge depth as a function of expertise and distracting noise. For the novices there was no difference between the no noise and masking noise conditions. For the intermediate trainees and experts, performance in the masking noise condition was worse than in the no noise condition.
Finally, we hypothesized that we would be able to detect changes in performance due to familiarization with the model. This hypothesis was not supported statistically (F9–234 = 1.31; p = 0.23) (Fig. 1). However, as seen in Figure 1, under normal auditory conditions, participants in all 3 groups underwent brief adaptation processes.
Discussion
The impetus for this study came from recent conflicting evidence in the psychomotor and surgical domains. Psychomotor literature shows that distracting noise can have adverse effects on performing various cognitive and motor skills,10–13 whereas the limited amount of research into the impact of distracting noise in a surgical environment shows no deterioration of surgical performance in the presence of distracting noise.8,12 Because noise levels in operating rooms are often high,1–5 their potential impact on technical surgical performance deserves more extensive research.3
In the present study, we showed that our measurement system can discern expert and intermediate from novice performance. This finding lends further support to the construct validity of our metrics.16 However, we were unable to demonstrate differences in the level of technical performances between intermediate trainees and experts, suggesting that at the intermediate trainee level, a plateau on the specific skill of drilling was reached. This indicates that basic orthopedic technical performance cannot be differentiated using the plunge measure above the intermediate level. However, surgical performance is multidimensional and comprises a variety of components such as technical skills, communication skills, leadership, and clinical judgment and knowledge, to name a few.17 In the present study, we investigated only the performance on the technical skill of drilling. Our finding that intermediate and expert technical performance on this skill did not differ is in agreement with the literature. Datta and colleagues18 demonstrated that when a range of trainees and experts were assessed on a 5-station technical skills examination, the performances of both senior trainees and expert surgeons did not differ. It has been suggested that trainees first become proficient at basic technical skills, and that further learning is more evident in the other aspects of surgical performance such as clinical judgment, knowledge and communication skills.
Our primary experimental hypothesis was also supported by our finding that, compared with no masking noise, the presence of high levels of masking noise resulted in the deterioration of technical performance on an orthopedic drilling skill, as evidenced by changes in plunge depth, among intermediate trainees and experts. The presence of masking noise did not affect the drilling performance of novices. Specifically, with the introduction of masking noise, experts and intermediate trainees plunged more, while the novices performed at the same level. Therefore, our results suggest skilled orthopedic performance is affected by the presence of masking noise.
Finally, our third hypothesis that we would observe changes in performance owing to familiarization with the model was not supported. We were not able to statistically document changes in performance as a function of practice for any of the 3 groups, which speaks to the sensitivity of the assessment tool. Rather, the adaptations that we observed can be attributed to learning by interacting with the novel bones. More specifically, we suggest that the initial improvements in performance represent 2 hypothetical processes. For the novice participants, we believe the longer and more profound learning curve (about 4 trials) represents the acquisition of the drilling skill. For the more experienced participants, we believe that the one-trial change in performance that we observed represents a warm-up effect where various sources of sensory information, including auditory information are associated with the characteristics of the bone.
Why were the novice, the intermediate and the expert performances affected differently by the presence of masking noise? The present data can be explained by considering the dual functions of sound. Sound, which is a physical property of the ambient environment, can be viewed as a source of performance-relevant sensory information or noninformative sensory information. Humans continuously gather all types of sensory information from the surrounding environment for the purpose of generating motor actions.19 In the process of learning, the most accurate and important sensory modalities for the success of a desired motor action are selected. Experts learn how to extract and use relevant sensory information such as sound to improve performance.16,20,21 The presence of masking noise, another form of sound, can mask auditory information that is crucial to performance.
Our findings complement those of previous investigations by Moorthy and colleagues.3,9 In one study,9 the participants (a group of laparoscopic surgeons) were asked to perform a laparoscopic suturing task without noise, with noise at 80–85 dB and with background music. They found the addition of noise did not interfere with performance. We suggest that during laparoscopic suturing, there is no inherent performance-enhancing, task-specific auditory information; therefore, their finding was not surprising. However, in performing an orthopedic drilling skill, the surgeon relies at least to some degree on sounds produced by the drill bit penetrating the bone to determine the density of the bone. Because the density of the bone changes as it is penetrated, the surgeon can determine the position of the drill within the layers by listening to the changes in the drill pitch. Our findings highlight the importance of auditory cues as a source of advanced information used by expert orthopedic surgeons to judge bone density, anticipate the changes in the density of the bone and thus achieve optimal performance (limited plunging). Collectively, these results suggest that expertise involves the acquired ability to use various sources of sensory information as part of an anticipatory motor control strategy,22 whereas novices are limited to the less effective online use of feedback for motor control.
Whether the demonstrated effect has any clinically negative consequences in the operating room is not clear. However, our results show surgical performance is a truly complex interaction of multisensory motor and cognitive integrations deserving more of our attention. Also, these results carry educational value because they highlight the use of auditory information during drilling as part of orthopedic surgical expertise. Therefore, new trainees should be made aware of this fact early in their training. For example, junior residents in orthopedic surgery may be instructed to minimize the amount of plunging when practising drilling on a bench model. However, our understanding of the control mechanisms of a drilling action underlying the observed plunge indicates that the residents should be instructed to pay attention to the sound generated when drilling, rather than told to minimize the amount of plunge.
Acknowledgments
This project was funded by separate Natural Science and Engineering Research Council of Canada discovery grants awarded to Heather Carnahan and Adam Dubrowski.
Podium presentations at the Wilson Centre Research Day, Oct. 28, 2004, Sunnybrook Health Sciences Centre, Toronto, Ont., and at the annual meeting of the Canadian Society for Psychomotor Learning and Sport Psychology, Oct. 15–17, 2004, Saskatoon, Sask.
Contributors: Ms. Praamsma and Drs. Carnahan and Dubrowski designed the study. Ms. Praamsma, Drs. Veillette and Dubrowski and Mr. Gonzalez acquired and analyzed the data, which Dr. Backstein also analyzed. Ms. Praamsma and Dr. Carnahan wrote the reviewed the article, which Drs. Backstein, Veillette and Dubrowski and Mr. Gonzalez also reviewed. All authors gave final approval for publication.
Competing interests: None declared.
Accepted for publication Jun. 27, 2007
Correspondence to: Dr. H. Carnahan, The Wilson Centre, 200 Elizabeth St., Eaton South 1ES 559, Toronto ON M5G 2C5; fax 416 340-3792; heather.carnahan@gmail.com
References
- 1.Dodenhoff RM. Noise in the orthopedic operating theatre. Ann R Coll Surg Engl 1995;77(Suppl):8-9. [PubMed]
- 2.Hodge B, Thompson JF. Noise pollution in the operating theatre. Lancet 1990;14: 891-4. [DOI] [PubMed]
- 3.Moorthy K, Munz Y, Undre S, et al. Objective evaluation of the effect of noise on the performance of a complex laparoscopic task. Surgery 2004;136:25-30. [DOI] [PubMed]
- 4.Liu EH, Tan S. Patients' perception of sound levels in the surgical suite. J Clin Anesth 2000;12:298-302. [DOI] [PubMed]
- 5.Love H. Noise exposure in the orthopedic operating theatre: a significant health hazard. ANZ J Surg 2003;73:836-8. [DOI] [PubMed]
- 6.Nott MR, West PD. Orthopedic theatre noise: a potential hazard to patients. Anaesthesia 2003;58:784-7. [DOI] [PubMed]
- 7.Ullah R, Bailie N, Crowther S, et al. Noise exposure in orthopedic practice: potential health risk. J Laryngol Otol 2004;118:413-6. [DOI] [PubMed]
- 8.Willett KM. Noise-induced hearing loss in orthopedic staff. J Bone Joint Surg Br 1991;73:113-5. [DOI] [PubMed]
- 9.Moorthy K, Munz Y, Dosis A, et al. The effect of stress-inducing conditions on the performance of a laparoscopic task. Surg Endosc 2003;17:1481-4. [DOI] [PubMed]
- 10.Bhattacharya SK, Roy A, Chatterjee SK. Comparison of motor-manual performance in quiet and noisy environments. Indian J Med Res 1978;68:306-11. [PubMed]
- 11.Landstrom U, Kjellberg A, Bystrom M. Acceptable levels of tonal and broadband repetitive and continuous sounds during the performance of non-auditory tasks. Percept Mot Skills 1995;81:803-16. [DOI] [PubMed]
- 12.Kjellberg A, Skoldstrom B. Noise annoyance during the performance of different non-auditory tasks. Percept Mot Skills 1991; 73:39-49. [DOI] [PubMed]
- 13.Persson Waye K, Bengtsson J, Kjellberg A, et al. Low frequency noise “pollution” interferes with performance. Noise Health 2001; 4:33-49. [PubMed]
- 14.van Gemmert AW, Van Galen GP. Stress, neuromotor noise, and human performance: a theoretical perspective. J Exp Psychol Hum Percept Perform 1997;23: 1299-313. [DOI] [PubMed]
- 15.Oldfield RC. The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia 1971;9:97-113. [DOI] [PubMed]
- 16.Dubrowski A, Backstein D. The contributions of kinesiology to surgical education. J Bone Joint Surg Am 2004;86:2778-81. [DOI] [PubMed]
- 17.Seymour NE, Gallagher AG, Roman SA, et al. Virtual reality training improves operating room performance: results of a randomized, double-blinded study. Ann Surg 2002;236:458-63. [DOI] [PMC free article] [PubMed]
- 18.Datta V, Bann S, Aggarwal R, et al. Technical skills examination for general surgical trainees. Br J Surg 2006;93:1139-46. [DOI] [PubMed]
- 19.Bhushan N, Shadmehr R. Computational nature of human adaptive control during learning of reaching movements in force fields. Biol Cybern 1999;81:39-60. [DOI] [PubMed]
- 20.Ernst MO, Banks MS. Humans integrate visual and haptic information in a statistically optimal fashion. Nature 2002;415: 429-33. [DOI] [PubMed]
- 21.Farrow D, Abernathy B. Do expertise and the degree of perception-action coupling affect natural anticipatory performance? Perception 2003;32:1127-39. [DOI] [PubMed]
- 22.Witney AG, Goodbody SJ, Wolpert DM. Learning and decay of prediction in object manipulation. J Neurophysiol 2000;84:334-43. [DOI] [PubMed]