

The isomorphic response of Koebner, also known as the Koebner phenomenon, is a well-recognized dermatologic manifestation first described in psoriasis. The isomorphic response occurs when a dermatologic disease develops at a site of normal-appearing skin that is injured in some manner.1
Chronic graft-versus-host disease (cGvHD) is a multisystem disorder that commonly affects the skin and may present with protean manifestations. Sclerotic cGvHD features are categorized as lichen sclerosus-like, morphea-like, or sclerosis involving the subcutaneous tissue and fascia.2 Morphea-like lesions of cGvHD are characterized by localized dyspigmented indurated plaques of skin thickening.
Report of Cases
A retrospective analysis was performed on 110 consecutive patients with a diagnosis of cGvHD of any organ system evaluated in a cross-sectional cGvHD study at the National Institutes of Health (NIH). Eighty-one patients had evidence of cutaneous cGvHD and 58 of these patients (72%) exhibited evidence of cutaneous sclerosis as defined by the NIH cGvHD Consensus Criteria.2 Eleven of 58 patients (19%) with cGvHD-associated sclerosis exhibited localized morphea-like lesions involving the lower abdomen (the “waistband” area), often in a striking linear distribution (Table 1, Figure 1A). Lesional skin biopsies were performed in six patients and all were consistent with sclerotic cGvHD. Six of 11 patients with waistband involvement were female and three of these six exhibited similar morphea-like lesions in the inframammary/lateral torso region (the “brassiere-band” area) (Figure 1B).
Table 1.
Characteristics of Patients with Morphea-like cGvHD Exhibiting an Isomorphic Response (continued on following page)
| Gender/Age | Primary diagnosis | Date of skin evaluation (days post transplant) | Type of allogeneic transplant | cGvHD other organ involvement | Type of cutaneous cGvHD | Current cGvHD treatment | Biopsy at site of isomorphic lesion | Location of isomorphic response |
|---|---|---|---|---|---|---|---|---|
| M/57 | CLL | Day +1611 | 6/6 NM related PBSCT | GI
Oral |
D/S/F | MMF 1500mg BID
Prednisone 25/0mg alternate days |
No | WB |
| M/56 | MM | Day +763 | 6/6 NM related PBSCT | None | D/S/F | None | Yes | WB |
| F/52 | MM | Day +541 | 6/6 NM related PBSCT | Oral
VV |
E/D | Clobetasol ointment 0.05% | No | BB
WB |
| F/39 | NHL | Day +1972 | 6/6 NM related PBSCT | Ocular
Oral VV |
E/D/S/F | ECP
Hydroxychloroquine 600mg QD Prednisone 35mg QOD Tacrolimus 1mg QAM; 0.5 mg QPM |
No | WB |
| F/20 | Precursor
B cell ALL |
Day +789 | 6/6 Myelo. related BMT | Ocular
Oral Pulmonary |
D/S | MMF 1500mg q12hrs
Prednisone 100 mg QD |
No | BB
WB |
| M/57 | MDS | Day +1647 | 6/6 Myelo. related PBSCT | Ocular
Oral |
E/D/S/F | ECP
MMF 1gm q12hrs Prednisone 20mg QOD Tacrolimus 4mg q12hrs |
No | WB |
| F/53 | MM | Day +2436 | 6/6 NM related PBSCT | Ocular
VV |
E/D | Prednisone 50/40mg alternate days | Yes | WB |
| M/36 | CML | Day +1203 | 6/6 Myelo. related BMT | Ocular
Oral |
E/D/S | MMF 500mg BID
Tacrolimus 2mg BID |
Yes | WB |
| M/40 | Precursor
B cell ALL |
Day +2835*
Day +1417** |
6/6 Myelo. unrelated BMT | GI
Hepatic Ocular Oral |
E/D/S/F | Prednisone 10mg QD
Tacrolimus 0.5 mg QD |
Yes | WB |
| F/46 | NHL | Day +944 | 6/6 NM related PBSCT | Ocular
Oral |
E/D/S/F | Prednisone 60/10mg alternate days
Sirolimus 1mg QD Tacrolimus 4mg QD |
Yes | BB
WB |
| F/49 | NHL | Day +1106 | 6/6 Myelo. related PBSCT | Ocular
Oral |
E/D/S/F | None | Yes | WB |
Abbreviations: ALL, acute lymphoblastic leukemia; BB, brassiere-band area; BMT, bone marrow transplant; CLL, chronic lymphocytic leukemia; CML, chronic myelogenous leukemia; ECP, extracorporeal photopheresis, MDS, myelodysplastic syndrome, MM, multiple myeloma, MMF, mycophenolate mofetil, Myelo, myeloablative, NHL, non-Hodgkin’s lymphoma, NM, non-myeloablative, PBSCT, peripheral blood stem cell transplant, VV, vulvovaginal, WB, waistband area.
Classification of cutaneous cGvHD: E, erythematous-type cGvHD; D, morphea-like sclerosis; S, subcutaneous sclerosis; F, fasciitis.
T-cell depleted 6/6 Myelo unrelated BMT
T-cell repleted 6/6 Myelo unrelated BMT (second transplant; same donor)
Figure 1.
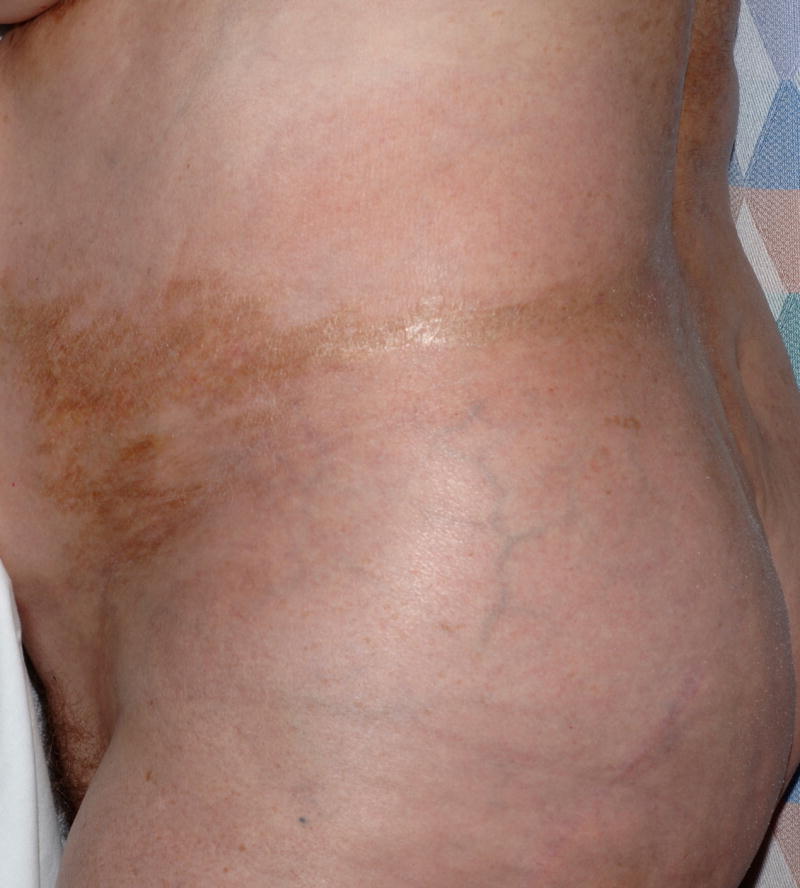

Extensive linear hyperpigmentation and skin fibrosis in the lower abdomen waistband area (A) and lateral torso brassiere-band area (B) in a patient with morphea-like cGvHD.
Comment
Chronic GvHD is an incompletely understood multi-system disorder with features of both alloimmunity and autoimmunity. We propose that the combination of irritation, friction, and pressure applied chronically to the waistband and brassiere-band areas of the torso is responsible for localization of cGvHD at these sites, consistent with an isomorphic response. The mechanism by which relatively minor external trauma triggers the complex immunological cascade that results in skin fibrosis is unclear. Interestingly, morphea and lichen sclerosus, two disorders which resemble cGvHD, are also associated with an isomorphic response,3 suggesting a common pathogenesis. Morphea-like cGvHD is characterized histologically by prominent dermal sclerosis, but apoptotic keratinocytes in the overlying epidermis suggestive of typical cGvHD may also be present. Local infiltration of T-cells is thought to initiate epithelial damage and propagate tissue injury through recruitment of natural killer (NK) cells, macrophages, and mast cells. Transforming growth factor-β and platelet derived growth factor have been implicated in the development of skin fibrosis in cGvHD.4 Recently, activating antibodies targeting the PDGF receptor were reported in a group of patients with extensive cGvHD, suggesting that targeted inhibition of PDGFR signaling with therapies such as imatinib may inhibit the fibrotic process associated with sclerotic cGvHD.5
Careful evaluation of the “high-risk” sites in the waistband area (and braissiere-band in females) may allow for early diagnosis of sclerotic cGvHD and appropriate intervention. Because it is not possible to predict which patients will develop sclerotic cGvHD, all patients at risk for cGvHD may wish to avoid excessively tight or binding garments that may irritate or apply significant pressure to the skin.
Acknowledgments
The study was supported in part by the Intramural Research Programs of the NIH, National Cancer Institute, Center for Cancer Research. Miss Patel was supported by the Clinical Research Training Program, a public-private partnership supported jointly by the NIH and Pfizer Inc. (via a grant to the Foundation for NIH from Pfizer Inc.), Bethesda, Maryland. Dr. Cowen had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Footnotes
Authorship responsibility and contributions: Miss Patel: Performed data analysis and wrote manuscript, Dr. Turner: Evaluated patients and edited manuscript, Dr. Pavletic: Evaluated patients and edited manuscript, Dr. Cowen: Evaluated patients, designed outline of submission, and edited manuscript; primary author responsible for scientific integrity of paper.
Conflict of Interest: The authors have no relevant financial disclosures or conflicts of interest to declare.
Contributor Information
Asha R. Patel, Email: patelas@mail.nih.gov.
Steven Z. Pavletic, Email: pavletis@mail.nih.gov.
Maria L. Turner, Email: mlturner@mail.nih.gov.
Edward W. Cowen, Email: cowene@mail.nih.gov.
References
- 1.Boyd AS, Neldner KH. The isomorphic response of Koebner. Int J Dermatol. 1990 Jul–Aug;29(6):401–10. doi: 10.1111/j.1365-4362.1990.tb03821.x. [DOI] [PubMed] [Google Scholar]
- 2.Filipovich AH, Weisdorf D, Pavletic S, et al. National Institutes of Health consensus development project on criteria for clinical trials in chronic graft-versus-host disease: I. Diagnosis and staging working group report. Biol Blood Marrow Transplant. 2005 Dec;11(12):945–56. doi: 10.1016/j.bbmt.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 3.Rubin AI, Stiller MJ. A listing of skin conditions exhibiting the koebner and pseudo-koebner phenomena with eliciting stimuli. J Cutan Med Surg. 2002 Jan-Feb;6(1):29–34. doi: 10.1007/s10227-001-0029-6. [DOI] [PubMed] [Google Scholar]
- 4.Ochs LA, Blazar BR, Roy J, Rest EB, Weisdorf DJ. Cytokine expression in human cutaneous chronic graft-versus-host disease. Bone Marrow Transplant. 1996 Jun;17(6):1085–92. [PubMed] [Google Scholar]
- 5.Svegliati S, Olivieri A, Campelli N, et al. Stimulatory autoantibodies to PDGF receptor in patients with extensive chronic graft-versus-host disease. Blood. 2007 Jul 1;110(1):237–41. doi: 10.1182/blood-2007-01-071043. [DOI] [PubMed] [Google Scholar]