

Abstract
Objective
This study examined the relationships between childhood and family background variables, including sexual and physical abuse, and subsequent alcohol abuse and psychological distress in adult lesbians.
Methodology
Structural equation modeling was used to evaluate relationships between childhood sexual and physical abuse and parenting variables and latent measures of lifetime alcohol abuse and psychological distress in a large community-based sample of lesbians.
Results
Childhood sexual abuse (CSA) directly predicted lifetime alcohol abuse, and childhood physical abuse (CPA) directly predicted lifetime psychological distress. In addition, CSA indirectly increased the risk of lifetime alcohol abuse through its negative effect on age at first heterosexual intercourse. Childhood physical abuse (CPA) had only indirect effects on lifetime alcohol abuse through its strong relationship to lifetime psychological distress. Parental drinking problems and parental strictness directly predicted lifetime psychological distress; parental drinking problems indirectly predicted lifetime alcohol abuse through the mediators of age of drinking onset and lifetime psychological distress. White lesbians, younger lesbians, and those with lower levels of education were at greatest risk of psychological distress.
Conclusion
While the cross-sectional design precludes causal conclusions, study findings—especially those related to CSA—are consistent with previous research on predominantly heterosexual women in the general population. Lesbians who experienced CSA were at heightened risk of lifetime alcohol abuse and those who experienced CPA were at heightened risk of lifetime psychological distress relative to lesbians without abuse histories. Given the dearth of research on childhood abuse and sexual orientation, studies are needed that examine the similarities and differences between lesbians’ and heterosexual women’s experiences of, and responses to, childhood abuse.
Introduction
Child abuse is an important public health concern that has a significant impact on both individuals and communities. In addition to the immediate threat of physical and psychological harm to a child, studies show that physical and sexual abuse in childhood are strongly associated with a number of later adverse mental health outcomes. The effects of childhood sexual abuse (which disproportionately affects girls and women) include substance use/abuse (Dube, Anda, Felitti, Edwards, & Croft, 2002; MacMillan et al., 2001; S. C. Wilsnack, Vogeltanz, Klassen, & Harris, 1997) and various forms of psychological distress, such as anxiety and depression (MacMillan et al., 2001). Research suggests that lesbians (and other sexual minority groups) may be at a heightened risk of childhood abuse (Balsam, Rothblum, & Beauchaine, 2005; Corliss, Cochran, & Mays, 2002; Tjaden, Thoeness, & Allison, 1999) and alcohol abuse (see Hughes, 2005, for review). Despite substantial empirical support for the association between childhood victimization and adverse mental health outcomes, the pathways that link these variables are unclear. This is particularly true for childhood physical abuse (CPA) as, to date, more research has focused on childhood sexual abuse (CSA) than on CPA. The purpose of this study was to examine the mechanisms by which childhood abuse may be related to alcohol abuse and psychological distress among adult lesbians.
Progress in understanding the links between childhood abuse and adverse mental health outcomes has also been hampered by a number of theoretical and methodological limitations of research in this area. Among the most important is that many studies assume a single causal pathway leading from childhood victimization to later substance abuse or other mental health problems. A related limitation is that many studies conceptualize experiences of childhood abuse as isolated events separate from the cultural, familial, and relational contexts in which they occur. Further, studies examining the long-term outcomes of childhood abuse often rely on samples of college students, patients in clinical treatment, or women recruited based on their abuse experiences. Thus, little is known about how cultural differences and life trajectories shape the later health consequences of childhood victimization among women in the general non-clinical population. In particular, very few studies have assessed the sexual orientation of study participants, and most researchers appear to assume that participants are heterosexual. The lack of attention to sexual orientation may represent an important research gap given accumulating evidence that lesbians are at heightened risk of both alcohol abuse and psychological distress.
Sexual orientation
Researchers are only beginning to consider sexual orientation as a significant focus of health research and an important demographic variable to include in studies of health. Like race/ethnicity and socioeconomic status, sexual orientation is a complex construct that is difficult to measure. Sexual orientation is most commonly described as including behavioral, affective (attraction or desire), and cognitive (identity) dimensions (Laumann, Gagnon, Michael, & Michaels, 1994). Although strongly correlated, these dimensions are not perfectly congruent. For example, women whose sex partners are primarily, or only, women may not identify as lesbian or bisexual. Similarly, women who identify as lesbian may have both female and male sexual partners or not be sexually active. For these reasons, the choice of sexual orientation definitions and measures should be guided by research purposes and goals. For example, in studies of sexually transmitted infections, sexual behavior is the obvious choice; studies that ask only about sexual identity may over- or under-estimate risk. However, in research on health concerns for which societal stigma, prejudice and discrimination are believed to play an important role, sexual identity may be especially relevant. Women were recruited for the CHLEW based on lesbian self-identity because we believe that lesbians’ heightened risk of drinking-related problems is largely a consequence of cultural and environmental factors associated with being part of a stigmatized and marginalized population group (Hughes, 2005; Hughes & Wilsnack, 1997).
Alcohol abuse and psychological distress
Lesbians’ heightened risk of alcohol abuse is supported by research using both non-probability (volunteer) samples and probability samples of women who self-identify as lesbian (Hughes, 2005). Even studies that find no difference between lesbian and heterosexual women in current drinking or drinking-related problems tend to report higher rates of alcoholism treatment or recovery among lesbians (Bloomfield, 1993; Hughes, Haas, Razzano, Cassidy, & Matthews, 2000; Hughes, Wilsnack, & Johnson, 2005), suggesting heightened lifetime risk. Researchers have begun to take advantage of the recent addition of questions about sexual orientation in several large national surveys to examine relationships between sexual orientation and alcohol use/abuse. For example, questions about gender of past sex partners (the sexual orientation question most commonly included) have permitted researchers to compare alcohol abuse indicators in women who report a history of same-sex partners with women who report only male sex partners (Cochran & Mays, 2000; Gilman et al., 2001). While samples defined on the basis of sexual behavior alone cannot be presumed to represent the population of women who identify as lesbian, data from these studies lend support to the prevailing assumption that lesbians are at heightened risk of alcohol abuse.
Research on psychological distress among lesbians has used similar sampling and study methods. Findings point to higher rates among lesbians of both lifetime depression (Cochran & Mays, 1994; Fergusson, Horwood, & Beautrais, 1999; Hughes et al., 2005; Matthews, Hughes, Razzano, Johnson, & Cassidy, 2002; Meyer, 2003; Oetjen & Rothblum, 2000) and recent (past year or current) depression (Cochran & Mays, 2000; Gilman et al., 2001; Oetjen & Rothblum, 2000). Although measures of anxiety are less often included in studies of mental health and sexual orientation, available findings suggest trends similar to those for depression (Cochran, Sullivan, & Mays, 2003; Gilman et al., 2001).
The primary goal of most research on lesbians’ mental health has been to estimate the prevalence of specific mental health problems or to evaluate lesbians’ risk of these problems relative to heterosexual women. Only a few studies have examined potential risk factors for lesbians’ mental health problems. The focus of these have studies varied, but as a whole, findings suggest that stress related to sexual orientation can likely explain only a portion of the difference in mental health risk between lesbians and heterosexual women. Recent reviews suggest that violence and victimization, including childhood sexual and physical abuse, may provide additional understanding of lesbians’ vulnerabilities to alcohol abuse and psychological distress (Hughes & Wilsnack, 1997).
Childhood sexual abuse and physical abuse
Large general population surveys of childhood abuse rarely ask about sexual orientation and studies of sexual minority groups have only occasionally assessed childhood abuse. Nevertheless, the available research has found that childhood sexual and physical abuse are as frequently, or more frequently, reported by lesbians compared to heterosexual women (e.g., Balsam et al., 2005; Corliss, Cochran, & Mays, 2002; Hughes et al., 2001; Saewyc, Bearinger, Blum, & Resnick, 1999; Tomeo, Templer, Anderson, & Kotler, 2001; Tjaden et al., 1999). Given the diversity of groups studied and the variety of ways that CSA and CPA were measured, the overall consistency of findings lends support to recent suggestions that lesbians (and other sexual minority groups) may be at heightened risk of childhood abuse (Balsam et al., 2005; Corliss et al., 2002; Tjaden et al., 1999).
Although the association between childhood victimization and subsequent substance abuse and psychological distress among women is well documented, it is not clear whether substance abuse resulting from childhood victimization increases the risk of other adverse consequences, (e.g., depression) or if such consequences come first and alcohol or other drug abuse follows in an effort to cope. Much of what is known about the sequelae of childhood abuse is from reports of women in treatment for substance abuse or psychological problems. In one of the few studies to explore the relationship between CSA and alcohol abuse among women in the general population, Wilsnack et al. (1997) found that CSA was strongly related to most drinking measures in their survey, including alcohol use in the past 30 days, intoxication, and number of problem consequences and symptoms of potential alcohol dependence in the past 12 months. Additionally, in longitudinal analyses, CSA predicted increased drinking and alcohol dependence symptoms over 10 years, controlling for baseline drinking levels (Wilsnack, Wilsnack, Kristjanson, & Harris, 1998). With regard to CPA, MacMillan et al. (2001) surveyed a large probability sample of Ontario residents (age 15 to 64 years) and found that both female and male respondents who reported CPA had significantly higher lifetime rates of alcohol abuse/dependence and anxiety disorders. In addition, among respondents who reported CPA, women, but not men, had significantly higher lifetime rates of major depression and illicit drug abuse/dependence.
The risk for adverse mental health outcomes among women who have experienced childhood victimization may differ for lesbians and heterosexual women (Balsam et al., 2005). The experience of being part of a stigmatized and marginalized minority group may contribute to different responses. Lesbians must learn to manage stigma and to cope in a world that is often hostile toward them. For some lesbians, this may increase their resilience and thus protect them, to varying degrees, when faced with other negative life experiences (Meyer, 2003). Conversely, other lesbians may be at a higher risk (than heterosexual women) of adverse mental health outcomes because the chronic stresses related to their minority status add to their overall psychological burden (Dohrenwend & Dohrenwend, 1969; Meyer, 2003). Because shame and secrecy often surround both CSA and early recognition of same-sex attraction, coming to terms with CSA may be particularly complex for some lesbians.
To develop effective mental health interventions it is important to know which groups of women are at greatest risk and which factors and processes put them at risk or protect them. The present analyses took advantage of a unique opportunity to address some of the current gaps in research on childhood victimization by examining relationships between childhood sexual abuse and physical abuse and adult mental health outcomes using data from the Chicago Health and Life Experiences of Women (CHLEW) study. The CHLEW includes a large, diverse sample of women who self-identify as lesbians, a population group that has received very little research attention. Further, the scope of questions included in the CHLEW allowed us to investigate the influence of childhood abuse experiences on both alcohol abuse and psychological distress while also assessing the impact of several other relevant background characteristics.
Methods
Sample recruitment and data collection
Because homosexuality continues to be highly stigmatized in the U.S., it is very difficult to estimate the prevalence of sexual minorities in a particular city or community. Existing estimates suggest that minority sexual orientation is relatively rare in the general population: from approximately 2% to 9% depending on how sexual orientation is defined (Laumann et al., 1994). Therefore, even large general population samples will have relatively small numbers of sexual minority women. Thus, a volunteer sample for the Chicago Health and Life Experiences of Women Study (CHLEW) was recruited using a broad range of recruitment sources and strategies, with strenuous efforts to maximize its representativeness by inclusion of a diverse group of participants. Women were eligible if they self-identified as lesbian, were 18 years old or older, and lived in the Chicago metropolitan area. The Chicago metropolitan area is in the Midwest region of the U.S. and includes 10 Illinois counties, 5 counties in Northwest Indiana, and one county in Wisconsin. The majority of CHLEW respondents, however, resided in Cook County, Illinois, where the city of Chicago is located.
We made a concerted effort to reach women who have been underrepresented in previous studies of lesbian health, including women of color, older lesbians, and lesbians of lower socioeconomic status. Interested women were asked to call the project office to complete a brief screening interview to determine eligibility (see Hughes et al., 2006 for more information about sample recruitment). We screened a total of 617 women; 553 of whom met our eligibility criteria. We interviewed 447 (80.8%) of these women. The major reasons that the remaining 106 (19.2%) were not interviewed included scheduling conflicts or screened respondents deciding that they did not want to participate (White women were slightly more likely than women of color to be screened but not participate: 51.9% vs. 48.1%). CHLEW participants represent a wide age range (18-83 years when first interviewed) and over half of them are racial/ethnic minority women.
Data were collected in 2000-2001 using face-to-face interviews conducted in private settings (usually the respondent’s home) by trained female interviewers. All interviewers received extensive training in general field interviewing techniques as well as study-specific training that included attention to potentially sensitive topics such as sexual orientation, substance use, sexual experiences, and childhood abuse experiences. Following a review of the study’s purpose and procedures, participants were asked to read and sign a detailed consent form approved by the University of Illinois at Chicago’s Institutional Review Board. Questions about sexual and physical abuse were asked near the end of the 90-minute interview that included many other areas of women’s lives and health. Participants received $35 in appreciation for their time.
Survey questionnaire
The interviews used a slightly adapted version of the interview questionnaire from the National Study of Health and Life Experiences of Women (NSHLEW), a 20-year longitudinal study of women’s drinking (e.g., Wilsnack, Wilsnack, & Klassen, 1984; Wilsnack et al., 1998). The Health and Life Experiences of Women questionnaire (HLEW) was designed in cooperation with the National Opinion Research Center. The nearly 400 questions permit assessment of the individual and combined effects of a large number of variables identified in previous theory and research as being associated with women’s drinking (e.g., family background characteristics, social roles, characteristics of close personal relationships, depression and anxiety, physical abuse and sexual abuse). Questions, indexes, and scales used in the initial (1981) HLEW were selected, whenever possible, from instruments that had been well validated in previous research; questions were added or adapted to make the questionnaire more sensitive to the special characteristics of women’s drinking. The HLEW was used to interview more than 1,600 women between 1981 and 2001, was extensively pretested prior to each wave of data collection and refined over time to retain variables with the greatest predictive value. Sexual orientation questions were developed in two focus groups. The Chicago version of the HLEW questionnaire, with the new sexual orientation questions and some changes in wording to make other questions more inclusive of lesbians’ experiences, was pretested in 1996 with 15 self-identified lesbians. A full-scale pilot of the questionnaire and interview protocol was conducted in 1997-1998 (Hughes, 2003; Hughes et al., 2001, 2005).
Sexual orientation
Respondents were screened for eligibility using the question: “Understanding that sexual identity is only one part of your identity, do you consider yourself to be lesbian, bisexual, heterosexual, transgender, or something else?” Because the experiences of women who self-identify as lesbian were of primary interest, women who identified as bisexual, heterosexual, or transgender in the telephone screening were excluded from the study. Despite this pre-study screening, in the subsequent interview 11 participants identified as bisexual, one identified as “queer,” and another refused to be labeled. These women were compared with the rest of the sample on demographic characteristics other than sexual orientation. No statistically significant differences were found, and they were included in the analyses.
Description of the sample
As reflected in Table 1, the study sample is much more diverse than those in previous lesbian health research. Women in the CHLEW ranged in age from 18 to 83 years (mean = 37.5 years). Fewer than one-half (47%) of the women identified as White, non-Hispanic White, 28% were Black non-Hispanic, 20% were Hispanic/Latina, and 5% were Asian/Pacific Islander, Native American, or bi- or multi-racial. Comparisons of respondents’ race/ethnicity with 2000 census data indicated that the sample closely reflected the distribution of the population in Cook County, Illinois where the vast majority of CHLEW participants lived (Chicago Fact Finder, 2003). In contrast to the general Cook County population, but similar to other lesbian samples, the respondents were well-educated overall; 56% had a bachelor’s degree or higher. The majority of respondents reported that they worked full-time at one job (54%) or multiple jobs (14%). Eleven percent worked part-time and 20% were not employed. Household income spanned a broad range. One-fourth of the sample had annual household incomes under $20,000, whereas 21% had incomes of $75,000 or more per year. Most (67%) respondents were in a committed relationship with a female partner, though 22% of these respondents did not live with their partner. Nearly one-third of the sample had one or more children and 19% had at least one child less than 18 years of age living with them at the time of the interview.
Table 1.
Demographic Characteristics of CHLEW Respondents (N=447)
| Total Sample (%) | |
|---|---|
| Age | |
| ≤ 30 | 32 |
| 31 – 40 yrs | 29 |
| 41 – 50 yrs | 23 |
| ≥ 51 | 16 |
| Mean age = (37.48) | |
| Race/Ethnicity | |
| White, non-Hispanic | 47 |
| Black, non-Hispanic | 28 |
| Hispanic | 20 |
| Other (bi/multi-racial) | 5 |
| Education Level | |
| High school or less | 14 |
| Some college | 30 |
| Bachelor’s degree | 26 |
| Graduate/Professional | 30 |
| Employment Status | |
| Work full-time for pay | 69 |
| Work part time for pay | 11 |
| Unemployed, looking | 10 |
| Unemployed, not looking | 10 |
| Annual Household Income | |
| Less than $20,000 | 25 |
| $20,000 – 39.999 | 26 |
| $40,000 – 74,999 | 27 |
| $75,000 or more | 21 |
| Relationship Status | |
| Living with partner, in a committed relationship | 45 |
| In committed relationship, not living with partner | 22 |
| Not in a committed relationship | 32 |
| Parental Status | |
| Any children (lifetime) | 31 |
| Any children at home | 19 |
Note. Because of rounding some categories do not equal 100
Measures
The primary focus of the analyses was on the relationships between childhood physical and sexual abuse and lifetime alcohol abuse and psychological distress. We also examined the influence of several important contextual background variables, including parental drinking problems, parental strictness, age of drinking onset, and age of first consensual sexual intercourse. Because psychological distress is a strong correlate of alcohol abuse in women (e.g., Grant & Harford, 1995), this variable was included as an independent predictor of alcohol abuse.
Latent variable measures: Alcohol abuse and psychological distress
Alcohol abuse
A latent variable representing lifetime alcohol abuse used four indicators: (a) the sum of eight adverse drinking consequences (e.g., driving while drunk or high from alcohol, starting arguments or fights with partner when drinking) and (b) the sum of five symptoms of potential alcohol dependence (e.g., blackouts, rapid drinking, inability to stop drinking before becoming intoxicated) as well as dichotomous measures of (c) whether the respondent had ever wondered if she was developing a drinking problem and (d) whether she had ever felt she ought to cut down on her drinking. The questions about adverse drinking consequences and alcohol dependence symptoms were drawn from national drinking surveys (e.g., Calahan, 1970; Polich & Orvis, 1979) and validated in the NSHLEW. The questions about self perceptions of drinking too much (feeling the need to cut down) and possibly having a drinking problem are also from the NSHLEW. In addition to having good face validity, they were moderately or strongly correlated with each of the other indicators in the latent measure of alcohol abuse.
Psychological distress
Psychological distress is a negative subjective state that most frequently manifests in two major, overlapping forms: depression and anxiety (Cho & Crittenden, 2006). A person who has one form of psychological distress tends to have the other, although not necessarily at the same time. Depression and anxiety indicators were used to construct the latent measure of lifetime psychological distress for this study. Lifetime experience of depression was measured by questions and diagnostic criteria of the National Institute of Mental Health Diagnostic Interview Schedule (Robins, Helzer, Croughan, & Ratcliff, 1981). Respondents were asked about a variety of symptoms (e.g., decreased appetite, problems with sleeping, thoughts of death). Persistence of three or more of these symptoms for at least 2 weeks, accompanied by feeling sad, blue, or depressed or by loss of interest or pleasure in things usually cared about, was defined as a depressive episode. The analyses reported here dichotomized lifetime depressive episodes into none versus one or more. Seven questions were used to measure anxiety: six 5-point Likert-type questions (e.g., worries a lot, can be tense, gets nervous easily) from the neuroticism scale of the Eysenck Personality Questionnaire (Eysenck & Eysenck, 1991) and a 5-point global question about anxiety, “How much has nervousness or anxiety interfered with your everyday life or activities?” The anxiety index had values ranging from 7 to 33 and was internally consistent (Cronbach’s alpha = .80). As anticipated, anxiety was weakly correlated with lifetime depression (r = .34, p < .001).
Childhood abuse variables
Childhood sexual abuse (CSA)
Women were classified as sexually abused based on their response to the question, “Do you feel that you were sexually abused when you were growing up?” This question was asked after a series of in-depth questions about a wide range of sexual experiences before age 18 that can be used to classify women’s experiences as CSA/non-CSA based on Wyatt’s (1985) definitions of intrafamilial and extrafamilial CSA. We decided to use the one-item self-perception question in these analyses because 12% (n = 53) of the cases had insufficient information to classify them according to Wyatt’s criteria, and because Wyatt’s definition is relatively inclusive and tends to define some experiences as CSA that are considered consensual by the respondent. In addition, all of the women whose experiences would be classified as CSA based on Wyatt’s criteria also reported self-perceived CSA. Nine women who reported self-perceived CSA could not be classified using Wyatt’s criteria because of insufficient information.
Childhood physical abuse (CPA)
Consistent with our measure of CSA, we used a one-item measure of self-perceived CPA. Questions in the interview first asked respondents if they had been physically hurt by a parent or other family member when they were growing up, and if so, how often. Respondents who reported that they were ever physically hurt were then asked, “Do you feel that you were physically abused by your parents or family members when you were growing up?”
Contextual variables
Several other contextual factors that have been associated with increased risk for child abuse and/or adverse mental health outcomes were also assessed. These included the respondent’s perceptions of whether her mother or her father had experienced drinking problems during the time that she was growing up (parental drinking problems; 0 = neither parent to 2 = both parents), as well as perceptions of parental strictness regarding sexual and nonsexual matters (0= neither parent perceived to be strict on either matter to 4=both parents strict on both matters). The respondent’s age when she first began to drink (age of drinking onset) was categorized as ≤ 10 years, 11-12, 13-14, 15-16, 17-18, 19-20, and 21 or older.
Age of first heterosexual intercourse (age of first sex) was categorized as 11-12, 13-14, 15-16, 17-18, 19-20, and 21 or older. We imputed age of first sex for women who reported the same age for the question “What was your age when you first had sexual intercourse after puberty?” and a later question about childhood sexual experiences which asked the respondent’s age when “someone had sexual intercourse with you, vaginal or anal.” Among women who reported the same age for both these experiences and who met Wyatt’s criteria for CSA (n=59) we did a conditional mean imputation looking first at the bivariate association between age of first sex and respondents’ age, income, education and race. All variables except income were significantly associated with age of first sex. Although we planned to do a three-way conditional mean imputation next, when all three variables were included in an ANOVA only race was independently associated with age of first sex. That is, race accounted for age and education differences and there were no significant interactions. Consequently, we did the conditional mean imputation using race only. Mean age at first sex was 16.8 years for non-Hispanic black lesbians, 18.3 years for Latina lesbians, and 19.3 years for non-Hispanic White women.
Consistent with the NSHLEW, we classified women who reported that they began drinking prior to age 15 as “early drinking onset” and those who reported heterosexual intercourse (other than CSA) prior to age 15 as “early heterosexual sex.”
Data analysis
After examining the bivariate associations, multivariate relationships were examined with covariance structure models (Hayduk, 1987). Covariance structure modeling can be used both to construct latent variable measures and to conduct path analyses. Eight cases that had missing data were omitted from these analyses: five with missing data for either CSA or CPA and three in which respondents reported being age 10 years or younger when they first had heterosexual intercourse.
The path model examined the effects of childhood abuse and background variables on lifetime risk of alcohol abuse and psychological distress. All potential direct effects of the childhood abuse (CSA, CPA) variables, background variables (parental drinking, parental strictness, age of onset of drinking and age of first sexual intercourse), and demographic variables (age, race and education) were examined, as well as the indirect paths by which the childhood abuse, demographic, and family variables (parental drinking problems and parental strictness) may have also influenced lifetime alcohol abuse and psychological distress through their effects on age at first sexual intercourse and age of drinking onset. Nonsignificant structural parameters were then eliminated and a final model was estimated. Path coefficients and model fit were estimated with Lisrel 8 using the full information maximum likelihood estimator (Joreskog & Sorbom, 1996).
Results
Frequencies of study variables
Childhood abuse was common in the CHLEW sample (Table 2). Nearly one-third of the respondents reported self-perceived CSA, and about one-fifth (22%) perceived themselves to have been physically abused. Thirty-two percent of the sample had at least one parent who had alcohol problems; 4% reported that both their parents had problems with alcohol. Fourteen percent of the sample said that both their parents were strict or very strict in both sexual and non-sexual matters; only 28% reported that neither parent was strict about either matter. One-fourth of lesbians in the sample began drinking alcohol before age 15 (early drinking onset), and 21% reported having had consensual heterosexual intercourse prior to age 15 (early sex). Excluding respondents who reported experiences of CSA involving intercourse and three who reported that they first had intercourse at age 10 or younger, 9% of the sample met study criteria for early sex.
Table 2.
Key Predictors and Outcome Frequencies a (N=447)
| Predictor Variables | (%)b | |
|---|---|---|
| Self-perceived childhood sexual abuse (CSA) | 31 | |
| Self-perceived childhood physical abuse (CPA) | 22 | |
| Parental drinking problems | ||
| Neither parent | 64 | |
| One parent | 32 | |
| Both parents | 4 | |
| Parental strictness | ||
| Neither parent strict | 28 | |
| At least one parent strict | 58 | |
| Both parents strict | 14 | |
| Early drinking onset (<15 yrs) | 25 | |
| Age of first sexual intercourse (<15 yrs) | 21 | |
|
| ||
| Outcome Variables | (%)b | |
|
| ||
| Lifetime Alcohol Abuse Indicators | ||
| Adverse drinking consequences | ||
| none | 32 | |
| 1 or more | 66 | |
| Alcohol dependence symptoms | ||
| none | 37 | |
| 1 or more | 62 | |
| Ever wondered if developing a drinking | 40 | |
| problem | ||
| Ever felt ought to cut down on drinking | 44 | |
| Lifetime Psychological Distress Indicators | ||
| DIS Depression | 57 | |
| Anxiety Index (Range = 7-33) | M=23.09 | SD=3.03 |
N’s vary slightly due to missing values
Some of the totals in the % column do not equal 100 because of rounding or missing data
The majority of the study respondents lifetime adverse drinking consequences (66%) and alcohol dependence symptoms (62%). Forty percent had wondered at some point in the past if they might be developing a drinking problem, and 44% reported feeling in the past that they should cut down on their drinking. Responses to these questions suggest potentially high rates of lifetime alcohol abuse. In addition, more than one-half (57%) of the study respondents reported lifetime depression. Scores on the anxiety index ranged from 7 to 33, with a mean of 23.09 (SD = 3.03).
Correlates of CSA and CPA
As indicated in the correlation matrix (Table 3), although the relationships were somewhat weak, both CSA and CPA were significantly correlated with parental drinking problems, lifetime depression, and lifetime alcohol dependence symptoms. Age of drinking onset was significantly associated with age of first heterosexual intercourse, alcohol problem consequences, and alcohol dependence symptoms. Age of first sex was significantly associated with alcohol problem consequences and alcohol dependence symptoms.
Table 3.
Bivariate Correlations among Study Variables
| Variable | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|
| 1. Childhood Sexual Abuse | .25*** | .10* | .05 | -.07 | -.10* | .07 | .12* | .14** | .05 |
| 2. Childhood Physical Abuse | --- | .16** | .09 | -.15** | -.08 | .12* | .10* | .16** | .08 |
| 3. Parental Drinking Problems | --- | -.11* | -.20*** | -.02 | .20*** | .21*** | .16*** | .17*** | |
| 4. Parental Strictness | --- | .12** | .03 | -.01 | -.04 | .03 | .07 | ||
| 5. Age of Drinking Onset | --- | .23*** | -.36*** | -.44*** | -.04 | -.03 | |||
| 6. Age of First Sexual Intercourse | --- | -.18*** | -.21*** | .01 | .07 | ||||
| 7. Alcohol Problem Consequences | --- | .64*** | .15** | ..06 | |||||
| 8. Alcohol Dependence Symptoms | --- | .13** | .14** | ||||||
| 9. Depression | --- | ..29*** | |||||||
| 10. Anxiety | --- |
p <.05
p <.01
p <.001
In bivariate analyses lesbians sexually abused in childhood were more likely than those without CSA to report lifetime alcohol dependence symptoms (70.8% vs. 58.8, p = .02) and lifetime depression (71.5% vs. 50.2%, p <. 001). Lesbians with CSA histories were also more likely than those without CSA to report early sex (64.2% vs. 37.5%, p < .001) and early onset of drinking (43.1% vs. 29.6%, p = .01). Lesbians who were physically abused in childhood were significantly more likely to report lifetime depression (71.9% vs. 52.3%, p = .001), early sex (59.8% vs. 41.4%, p =.001), and early onset of drinking (45.4% vs. 30.1%, p =.005).
Measurement model
As noted earlier, two variables served as indicators of lifetime psychological distress and four variables served as indicators of lifetime alcohol abuse (Table 4).
Table 4.
Measurement Model Components: Lifetime Alcohol Abuse and Psychological Distress* (N=439)
| Latent Variables
|
||||
|---|---|---|---|---|
| Observed Variables | Alcohol Abuse Estimate (SE) | Psychological Distress Estimate (SE) | ||
| Lifetime alcohol problem consequence | 1.00 | --- | ||
| Lifetime alcohol dependence symptoms | 1.27 | (0.09)*** | --- | |
| Ever wondered if developing a drinking problem | 0.67 | (0.06)*** | --- | |
| Ever felt ought to cut down on drinking | 0.47 | (0.05)*** | --- | |
| Lifetime depressive episode (DIS) | --- | 1.00 | ||
| Anxiety index | --- | 14.49 | (2.44)*** | |
Unstandardized coefficients
Structural model
Table 5 (with unstandardized coefficients) presents the estimated effects of the childhood predictors on lifetime psychological distress and on lifetime alcohol abuse. Several goodness-of-fit statistics indicate that the hypothesized model fit the data well [χ2 (55, N = 439) =56.2, p = .43, RMSEA = 0.0, 90% CI = 0.0-0.03]; GFI = 0.98; AGFI = 0.96; NFI = 0.97. As illustrated in Figure 1 (with standardized coefficients), all of the hypothesized direct paths were significant. The overall model accounted for 39% of the variance in lifetime alcohol abuse and 56% of the variance in lifetime psychological distress.
Table 5.
Structural Model Components: Lifetime Alcohol Abuse and Psychological Distress* (N=439)
| Mediators | Outcomes | |||||||
|---|---|---|---|---|---|---|---|---|
| Independent Variables | Age of Drinking Onset Estimate (SE) | Age First Intercourse Estimate (SE) | Psychological Distress Estimate (SE) | Alcohol Abuse Estimate (SE) | ||||
|
|
||||||||
| Parental drinking problems | -0.59 | (0.10)*** | 0.09 | (0.04)* | ||||
| Parental strictness | 0.03 | (0.02)* | ||||||
| Childhood physical abuse | 0.23 | (0.04)*** | ||||||
| Childhood sexual abuse | -0.11 | (0.06)* | 0.11 | (0.05)* | ||||
| Age of drinking onset | 0.04 | (0.02)* | -0.50 | (0.11)*** | ||||
| Age first intercourse | -0.19 | (0.04)*** | ||||||
| Psychological distress | 0.29 | (0.11)* | ||||||
| White | -0.18 | (0.07)* | 0.49 | (0.06)*** | 0.22 | (0.04)*** | ||
| Education | -0.08 | (0.03)*** | ||||||
| Age | 0.02 | (0.01)** | -0.01 | (0.00)*** | ||||
| R-Square | 0.13 | 0.14 | 0.56 | 0.39 | ||||
Model Goodness-of-Fit Statistics: X2 = 56.2, df = 55, ns; GFI = 0.98; AGFI = 0.96; NFI = 0.97; RMSEA = 0.0 (90% CI = 0.0 – 0.03); n =439.
p < .05
p < .01
p < .001
Figure 1. Covariance Structure Model: Lifetime Alcohol Abuse and Psychological Distress* (n = 439).
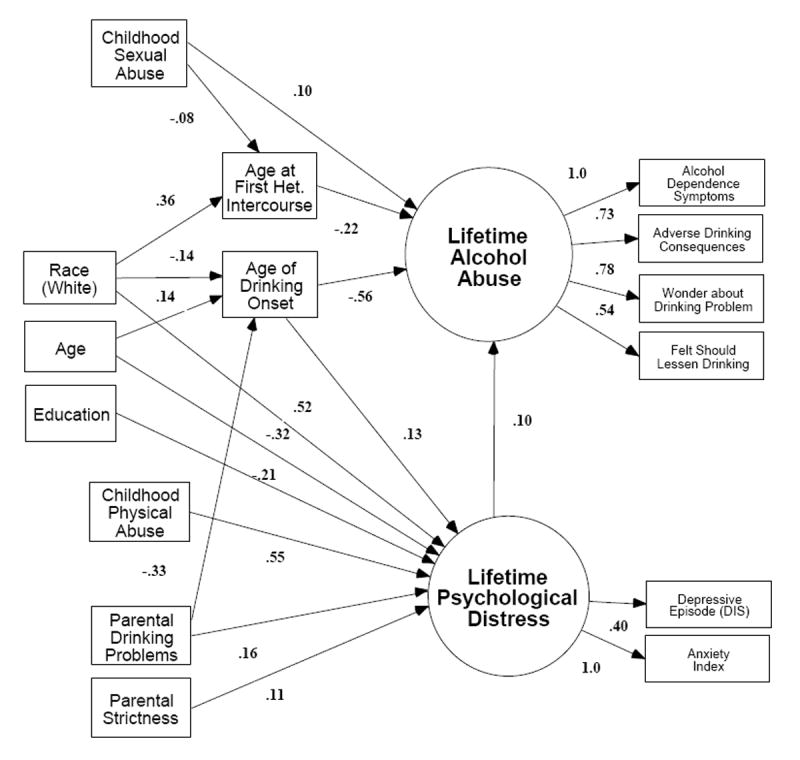
*Standardized Coefficients; Het. = Heterosexual; Race = White Respondents were compared with those from all other racial/ethnic groups
Childhood sexual and physical abuse
CSA directly predicted lifetime alcohol abuse (β = .10, p < .05), and CPA directly predicted lifetime psychological distress (β = .55, p < .001). In addition, CSA indirectly increased the risk of lifetime alcohol abuse through its negative effect on age of first sex.
Parental factors
Both parental drinking problems (β = .16, p < .05) and parental strictness (β = .11, p < .05) were directly related to lifetime psychological distress, which, in turn, was directly related to lifetime alcohol abuse (β = .10, p < .01). The parental drinking problems variable was directly related to younger age of drinking onset (β = -.33, p < .001) and indirectly to lifetime alcohol abuse.
Age of drinking onset and age of first heterosexual intercourse
Age of drinking onset, the strongest predictor of lifetime alcohol abuse (β = -.56, p < .001), mediated the effects of parental drinking problems on lifetime alcohol abuse and on lifetime psychological distress. Age of first sex partially mediated the effects of CSA on alcohol abuse.
Demographic variables
Although none of the three demographic variables in the model were directly associated with lifetime alcohol abuse, race, age, and education were each directly associated with lifetime psychological distress. White lesbians (β = .52, p < .001), younger lesbians (β = -.32, p < .001) and those with lower levels of education (β = -.21, p < .001) were at greater risk of lifetime psychological distress. Race indirectly influenced lifetime alcohol abuse. On the one hand, White lesbians tended to be younger than lesbians of color when they began drinking (β = -.14, p < .05)—which increased their risk of lifetime alcohol abuse. On the other hand, White lesbians were older when they first experienced heterosexual intercourse (β = .36, p < .001)—which decreased their risk of lifetime alcohol abuse. Age also indirectly influenced lifetime alcohol abuse: respondents who were older began drinking later (β = .14, p < .01), which was directly related to lower risk of lifetime alcohol abuse.
Psychological distress and alcohol abuse
CSA and lifetime psychological distress contributed equally to increased risk of lifetime alcohol abuse (β = .10, p < .05).
Discussion
In this study, lesbians who experienced CSA were at heightened risk of lifetime alcohol abuse and those who experienced CPA were at heightened risk of lifetime psychological distress relative to lesbians without abuse histories. Results concur with previous findings from general population samples of predominately heterosexual women, which suggest that childhood sexual abuse and physical abuse are associated with adverse mental health outcomes. Notably, the model accounted for 39% of the variation in lifetime alcohol abuse and more than one-half (56%) of the variation in lifetime psychological distress.
Findings also support previous research indicating that having a parent with alcohol problems is a strong predictor of adverse mental health outcomes (Dube et al., 2002; Widom, Ireland, & Glynn, 1995). The findings support the hypothesized indirect relationships between parental drinking problems and lifetime alcohol abuse through the effects of parental drinking problems on the age of drinking onset. Later onset of drinking has been shown to be an important protective factor against alcohol use disorders (Grant, Stinson, & Harford, 2001). Parental drinking problems, along with parental strictness, also predicted lifetime psychological distress but the contributions of these predictors were small compared with the influence of CPA on psychological distress.
Race and age had indirect effects on alcohol abuse via their influence on age of first sex and age of drinking onset. Consistent with recent results from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC) (Chen, Dufour, & Yi, 2004/05), White women and younger women in the CHLEW study reported earlier initiation of drinking, which was in turn associated with a higher risk of lifetime alcohol abuse. Although older when they began drinking, women of color reported earlier experience with heterosexual intercourse, a factor also associated with greater risk for lifetime alcohol abuse.
Race, age, and education were each directly associated with lifetime psychological distress: White participants, younger participants and those with lower levels of education were at greater risk. These findings are consistent with those of Kessler et al. (1994) who found that Black respondents in the National Comorbidity Study were less likely than White respondents to experience depression. Other studies (e.g., Plant & Sachs-Ericsson, 1994), however, have found that both Black and Hispanic respondents were more likely than White respondents to report depressive symptoms and depression.
Earlier heterosexual intercourse in this study was a direct predictor of lifetime alcohol abuse. Recent studies of sexual minority youth indicate that lesbians may engage in heterosexual intercourse at younger ages than their heterosexual counterparts (e.g., Saewyc et al., 1999). Potential reasons include “heterosexual immersion” as a strategy for responding to confusion or anxiety about same-sex attraction, and the risks associated with coming out (e.g., sexual minority teens are more likely than their peers to drop out of school and run away from, or be forced out of, their homes, and consequently are at risk of prostitution as a means of survival.) Researchers studying sexual-minority youth acknowledge the difficulty of determining which early sexual experiences were forced or consensual, and of disentangling the consequences of each. It is also difficult to determine the timing of early risk factors associated with CSA and alcohol abuse. Does CSA lead to early alcohol use, which then increases the likelihood of early consensual intercourse? Or (especially in the case of youth questioning their sexual orientation) does early sexual activity occur first and alcohol use follow as a way to deal with ambivalence about heterosexual sex? The co-occurrence of early onset of alcohol consumption and early engagement in heterosexual intercourse is common among adolescents (Jessor, Van den Bos, Vanderryn, Costa, & Turbin, 1995) and sexual abuse survivors (Finkelhor & Browne, 1985) and may be even more common among sexual-minority youth (Balsam et al., 2005; Saewyc et al., 1999).
It is possible that other variables not included in the current study could account for the association among the childhood abuse variables, lifetime alcohol abuse and psychological distress. For example, Tjaden and Thoennes (2000) found that women who had experienced CSA were more than twice as likely as women without CSA to be sexually assaulted in adulthood. In the same study, physical assault revictimization rates for women who had experienced CPA were twice as high as those of women who were not physically abused. These more proximal (unmeasured) experiences in adulthood might have accounted for some of the variance in the outcomes. Research using more complex models is needed to disentangle the influence of multiple traumas experienced at different developmental stages, as well as to evaluate the potential additive (or multiplicative) impact of multiple traumas experienced over the lifetime. In addition, the strong link between childhood abuse and posttraumatic stress found in previous studies (see Messman-Moore & Long, 2003) suggests that this factor may be another unmeasured influence on outcomes assessed in the current study.
Consistent with several recent studies of childhood abuse that have assessed sexual orientation (Balsam et al., 2005; Corliss et al., 2004; Tjaden et al., 1999; Tomeo et al., 2001), rates of CSA and CPA among lesbians in our sample were in the upper range of estimates for women in the general population. In addition, unlike studies of women in the general population (e.g., Wilsnack et al., 1997) reports of CSA did not differ by age group, nor did reports of CPA. High rates of childhood abuse in the present study may be explained, in part, by the method used (face-to-face interviews with a female interviewer) and the placement of the abuse questions in the interview (late in the interviews, after rapport and trust had been established). Higher rates of childhood abuse among lesbians may also be attributable to lesbians’ greater willingness to acknowledge and report these experiences. In coming to terms with their sexual orientation, lesbians likely spend a substantial amount of time in self-reflection and grappling with issues related to identity and authenticity. In addition, previous research indicates that the majority of lesbians have been in therapy or counseling at some point in their lives (see Hughes, 2005). This experience may increase lesbians’ comfort with acknowledging and disclosing both their minority sexual identity and other stigmatized statuses or experiences, such as childhood abuse.
In addition to the possibility that lesbians are more comfortable reporting childhood abuse experiences, some researchers have speculated that sexual-minority youth are, in fact, at greater risk of maltreatment when their sexual orientation is discovered or disclosed, or because of gender atypical appearance or behavior that may precede awareness of same-sex sexual orientation (Balsam et al., 2005; Tjaden et al., 1999). Discovery of a youth’s same-sex sexual orientation may lead to physical or sexual abuse by a family member, or to isolation from family and peers. Social isolation, in turn, can lead to behaviors (such as substance abuse and running away from home) that increase risk for sexual and physical victimization (Fergusson et al., 1999; Saewyc et al., 1999).
Whether or not lesbians are at higher risk of childhood abuse, it is possible that the impact of such abuse may differ from that experienced by heterosexual women. If so, such differences may have important implications for intervention and treatment. It is reasonable to assume that coming to terms with CSA may be complicated for lesbians. The transition from adolescence to adulthood is a critical developmental period when important health behaviors are adopted and attitudes and identity are formed. This transitional period is also characterized by rapid physical maturational changes that can be a source of embarrassment or discomfort. Such discomfort is likely intensified by sexual shame, confusion, and secrecy among adolescents who have experienced CSA (Finkelhor & Browne, 1985). Girls who are questioning their sexual orientation, or who identify as lesbian, must often navigate the transitional period of adolescence within an oppressive, if not overtly hostile, societal context and without the support of community, family, and peers. Some researchers argue that this context is an additional form of victimization (Balsam et al., 2005) which adds to shame, negative self-concept, and risk for self-destructive behaviors in survivors of CSA. Given that lesbians appear to be disproportionately represented among recipients of substance abuse and mental health services (Cochran & Mays, 2000; Cochran et al., 2003), clinicians and treatment programs must be prepared to address the needs of lesbian survivors of child abuse.
Adolescence is a critical point of intervention that may prevent later abuse-related disability. Such interventions may be especially important for sexual minority youth who have been abused and who consequently must come to terms with two stigmatized identities. Programs that provide outreach services to lesbians and other sexual-minority youth should be encouraged to incorporate strategies aimed at identifying individuals who live in abusive environments or who have histories of abuse. Access to mental health services provided by culturally sensitive and clinically skilled providers could reduce the human and economic costs associated with the adverse mental health consequences of childhood abuse.
In addition to the clinical implications, findings of the study suggest that more research is needed to examine the mental health impact of stigma associated with minority sexual orientation, as well as the potential cumulative impact of multiple stigmatized statuses, such as those experienced by lesbian survivors of CSA.
It is also important to recognize that many lesbians who have been victimized in childhood do not abuse alcohol or suffer from enduring psychological distress. Research on protective and resilience factors is imperative to understand more fully how lesbians cope with childhood abuse and multiple life stressors. Such information could provide important information about why some victims of childhood abuse do not turn to alcohol or other drugs as a means of dealing with these traumatic life experiences.
Strengths and limitations
This study’s limitations must be considered. First, the sample was selected using non-probability methods. However, even studies using probability samples typically over-represent White, middle-class, and well-educated lesbians, because these women tend to be most comfortable participating in research and disclosing their sexual orientation. While it can be argued that the current sample does not represent lesbians unwilling to disclose their sexual orientation, it does likely represent lesbians who are willing to disclose their sexual orientation (e.g., to health care providers). Furthermore, unlike most studies of lesbians, our sample is very diverse in terms of race/ethnicity and age, a factor that helps reduce some of the sample bias and enhances generalizability of the findings.
Limitations of several of the study measures should also be noted. Because the question about age of first heterosexual intercourse did not assess whether the experience was consensual it is possible that some of the respondents reported sexual experiences that would be classified as CSA. We were able to reduce the effects of this potential confounder by omitting women who reported the same age on this question in the CSA section and on a separate question about sexual intercourse elsewhere in the interview.
Some researchers have found that the number and type of questions about childhood abuse influence its reporting (e.g., Peters, Wyatt, & Finkelhor, 1986). Our use of single questions about self-perceived CSA and CPA may have underestimated the prevalence of these experiences. However, we chose to use these questions, in part, because findings from early research on stress and coping (e.g., Lazarus & Folkman, 1984), and more recent research on adult recollection of childhood abuse (e.g., Widom & Morris, 1997), suggest that the impact of childhood victimization on adult mental health outcomes is strongly related to the victims’ cognitive appraisal of the abuse events. Research should address further the most reliable and valid way to ask questions about childhood sexual and physical abuse.
Although this study used path analysis to test a time-ordered model, the data are cross-sectional, precluding any firm causal conclusions. Given the impossibility of manipulating the childhood abuse predictor variables, issues of causality cannot be easily resolved. Studies that examine a broad range of variables over time, however, would provide valuable longitudinal data about the effectiveness of various coping strategies and the persistence of mental health consequences that result from childhood abuse. Follow-up data collected with the CHLEW sample in 2004 will permit the examination of changes over time in alcohol abuse and psychological distress as well as the testing of predictive models that include a broader range of childhood and adult predictor variables.
Finally, the study is similar to most childhood sexual abuse research in its reliance on retrospective self-reports. Research has demonstrated that retrospective recall of childhood abuse is imperfect. Williams, Siegel, and Pomeroy (2000) found that of 129 women with documented histories of child sexual abuse, 38% did not remember the abuse 17 years later. Moreover, 16% of the women who currently remembered the abuse had periods when they did not remember it. Thus, it is possible that childhood abuse was underreported in our sample.
The current study also has a number of notable strengths. To our knowledge this is one of very few studies to examine the relationships between childhood abuse and mental health outcomes in a large sample of adult lesbians. The study used an instrument that has been well-validated in a large study of predominately heterosexual women. In addition, this study recruited a community-based sample of lesbians from a wide variety of sources. The sample is less subject to potential biases inherent in college or clinical samples, or in community samples recruited on the basis of past experience with childhood abuse. The use of standardized face-to-face interviews, conducted by trained interviewers, and analytic procedures that minimize measurement error are also strengths of the study.
As in heterosexual women, childhood victimization is a common experience of lesbians that has important and long-lasting effects on mental health and well-being. Clinicians who work with lesbians should routinely ask about experiences of victimization, as well as about past and current depression, drinking behavior and drinking-related problems. Adolescent and young adult lesbians who began drinking and who engaged in sexual activity at young ages may be at especially high risk for alcohol abuse and psychological distress. Lesbian survivors of childhood abuse need supportive environments in which they feel safe enough to disclose their sexual orientation and their victimization experiences. Clinicians who are able to provide such an environment have a unique opportunity to assist lesbian survivors in developing healthy, adaptive coping skills.
Acknowledgments
The authors wish to thank Frances Aranda, Wendy Bostwick, Kelly Martin, and Kelly Kinnison for assistance with the literature review, data analysis, and preparation of the manuscript. We also wish to thank the women who participated in the CHLEW study.
This study was supported by the National Institute of Alcohol Abuse and Alcoholism (NIAAA) AA00266 and AA13328 (T. Hughes, PI).
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Balsam K, Rothblum E, Beauchaine T. Victimization over the lifespan: Comparison of lesbian, gay, bisexual, and heterosexual siblings. Journal of Consulting and Clinical Psychology. 2005;73:477–487. doi: 10.1037/0022-006X.73.3.477. [DOI] [PubMed] [Google Scholar]
- Bloomfield K. A comparison of alcohol consumption between lesbians and heterosexual women in an urban population. Drug and Alcohol Dependence. 1993;33:257–269. doi: 10.1016/0376-8716(93)90112-4. [DOI] [PubMed] [Google Scholar]
- Calahan D. Problem drinkers: A national study. San Francisco, CA: Jossey-Bass; 1970. [Google Scholar]
- Chen CM, Dufour MC, Yi HY. Alcohol consumption among young adults ages 18–24 in the United States: Results from the 2001–2002 NESARC Survey. Alcohol Research & Health. 20042005;28:269–280. [Google Scholar]
- Chicago Fact Finder. Census Information Resource for Chicagoland Communities. 2003 Retrieved on March 24, 2005 from University of Notre Dames Institute for Latino Studies Website: http://www.nd.edu/~chifacts/chicago.html.
- Cho YI, Crittenden KS. The impact of adult roles on drinking among women in the United States. Substance Use & Misuse. 2006;41:17–34. doi: 10.1080/10826080500318574. [DOI] [PubMed] [Google Scholar]
- Cochran SD, Mays VM. Depressive distress among homosexually active African American men and women. American Journal of Psychiatry. 1994;151:524–529. doi: 10.1176/ajp.151.4.524. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cochran SD, Mays VM. Relation between psychiatric syndromes and behaviorally defined sexual orientation in a sample of the US population. American Journal of Epidemiology. 2000;151:516–523. doi: 10.1093/oxfordjournals.aje.a010238. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Cochran SD, Sullivan JG, Mays VM. Prevalence of mental disorders, psychological distress, and mental health services use among lesbian, gay, and bisexual adults in the United States. Journal of Consulting and Clinical Psychology. 2003;71:53–61. doi: 10.1037//0022-006x.71.1.53. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Corliss HL, Cochran SD, Mays VM. Reports of parental maltreatment during childhood in a United States population-based survey of homosexual, bisexual, and heterosexual adults. Child Abuse & Neglect. 2002;26:1165–1178. doi: 10.1016/s0145-2134(02)00385-x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Dohrenwend BP, Dohrenwend BS. Social status and psychological disorder: A causal inquiry. New York: Wiley; 1969. [Google Scholar]
- Dube SR, Anda RF, Felitti VJ, Edwards VJ, Croft JB. Adverse childhood experiences and personal alcohol abuse as an adult. Addictive Behaviors. 2002;27:713–725. doi: 10.1016/s0306-4603(01)00204-0. [DOI] [PubMed] [Google Scholar]
- Eysenck HJ, Eysenck BSG. Manual of the Eysenck Personality Scales. London: Hodder and Stoughton; 1991. [Google Scholar]
- Fergusson DM, Horwood LJ, Beautrais AL. Is sexual orientation related to mental health problems and suicidality in young people? Archives of General Psychiatry. 1999;56:876–880. doi: 10.1001/archpsyc.56.10.876. [DOI] [PubMed] [Google Scholar]
- Finkelhor D, Browne A. The traumatic impact of child sexual abuse: A conceptualization. American Journal of Orthopsychiatry. 1985;55:530–541. doi: 10.1111/j.1939-0025.1985.tb02703.x. [DOI] [PubMed] [Google Scholar]
- Gilman SE, Cochran SD, Mays VM, Hughes M, Ostrow D, Kessler RC. Risk of psychiatric disorders among individuals reporting same-sex sexual partners in the National Comorbidity Study. American Journal of Public Health. 2001;9:933–939. doi: 10.2105/ajph.91.6.933. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Grant BF, Harford TC. Comorbidity between DSM-IV alcohol use disorders and major depression: Results of a national survey. Drug and Alcohol Dependence. 1995;39:197–206. doi: 10.1016/0376-8716(95)01160-4. [DOI] [PubMed] [Google Scholar]
- Grant BF, Stinson FS, Harford TC. Age at onset of alcohol use and DSM-IV alcohol abuse and dependence: A 12-year follow-up. Journal of Substance Abuse. 2001;13:493–504. doi: 10.1016/s0899-3289(01)00096-7. [DOI] [PubMed] [Google Scholar]
- Hayduk LA. Structural equation modeling with LISREL: Essentials and advances. Baltimore: Johns Hopkins University Press; 1987. [Google Scholar]
- Hughes TL. Lesbians’ drinking patterns: Beyond the data. Substance Use & Misuse. 2003;38:1739–1758. doi: 10.1081/ja-120024239. [DOI] [PubMed] [Google Scholar]
- Hughes TL. Alcohol use and alcohol-related problems in lesbians and gay men. Annual Review of Nursing Research. 2005;23:283–325. [PubMed] [Google Scholar]
- Hughes TL, Haas AP, Razzano L, Cassidy R, Matthews A. Comparing lesbians’ and heterosexual women’s mental health: A multi-site survey. Journal of Gay and Lesbian Social Services. 2000;11:57–76. [Google Scholar]
- Hughes TL, Johnson T, Wilsnack SC. Sexual assault and alcohol abuse: A comparison of lesbians and heterosexual women. Journal of Substance Abuse. 2001;13:515–532. doi: 10.1016/s0899-3289(01)00095-5. [DOI] [PubMed] [Google Scholar]
- Hughes TL, Wilsnack SC. Use of alcohol among lesbians: Research and clinical implications. American Journal of Orthopsychiatry. 1997;67:20–36. doi: 10.1037/h0080208. [DOI] [PubMed] [Google Scholar]
- Hughes TL, Wilsnack SC, Johnson TP. Investigating lesbians’ mental health and alcohol use: What is an appropriate comparison group? In: Omoto A, Kurtzman H, editors. Sexual orientation and mental health: Examining identity and development in lesbian, gay, and bisexual people. Washington, D.C: American Psychological Association; 2005. pp. 167–184. [Google Scholar]
- Hughes TL, Wilsnack SC, Szalacha LA, Johnson T, Bostwick WB, Seymour R, Aranda F, Benson P, Kinnison KE. Age and race/ethnic differences in drinking and drinking-related problems in a community sample of lesbians. Journal of Studies on Alcohol. 2006;67:579–590. doi: 10.15288/jsa.2006.67.579. [DOI] [PubMed] [Google Scholar]
- Jessor R, Van den Bos J, Vanderryn J, Costa FM, Turbin M. Protective factors in adolescent problem behavior: Moderator effects and developmental change. Developmental Psychology. 1995;31:923–933. [Google Scholar]
- Joreskog KG, Sorbom D. LISREL 8: User’s reference guide. Chicago: Scientific Software International; 1996. [Google Scholar]
- Kessler RC, McGonagle KA, Zhao S, Nelson CB, Hughes M, Eshleman S, Wittchen H, Kendler KS. Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Archives of General Psychiatry. 1994;51:8–19. doi: 10.1001/archpsyc.1994.03950010008002. [DOI] [PubMed] [Google Scholar]
- Laumann EO, Gagnon JH, Michael RT, Michaels S. The social organization of sexuality: Sexual practices in the United States. Chicago, IL: University of Chicago Press; 1994. [Google Scholar]
- Lazarus RS, Folkman S. Stress, appraisal, and coping. New York: Springer; 1984. [Google Scholar]
- MacMillan HL, Fleming JE, Streiner DL, Lin E, Boyle MH, Jamieson E, Duku EK, Walsh CA, Wong MYY, Beardslee WR. Childhood abuse and lifetime psychopathology in a community sample. American Journal of Psychiatry. 2001;158:1878–1883. doi: 10.1176/appi.ajp.158.11.1878. [DOI] [PubMed] [Google Scholar]
- Matthews A, Hughes TL, Razzano L, Johnson T, Cassidy R. Prediction of depressive distress in a community sample of women: The role of sexual orientation. American Journal of Public Health. 2002;92:1131–1139. doi: 10.2105/ajph.92.7.1131. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Messman-Moore TL, Long PJ. The role of childhood sexual abuse sequelae in the sexual revictimization of women: An empirical review and theoretical reformulation. Clinical Psychology Review. 2003;23:537–571. doi: 10.1016/s0272-7358(02)00203-9. [DOI] [PubMed] [Google Scholar]
- Meyer IH. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychological Bulletin. 2003;129:674–697. doi: 10.1037/0033-2909.129.5.674. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Oetjen H, Rothblum E. When lesbians aren’t gay: Factors affecting depression among lesbians. Journal of Homosexuality. 2000;39:49–73. doi: 10.1300/J082v39n01_04. [DOI] [PubMed] [Google Scholar]
- Peters SD, Wyatt GE, Finkelhor D. Prevalence. In: Finkelhor D, editor. Sourcebook on child sexual abuse. Newbury Park, CA: Sage; 1986. pp. 15–59. [Google Scholar]
- Plant EA, Sachs-Ericsson N. Racial and ethnic differences in depression: The role of social support and meeting basic needs. Journal of Consulting and Clinical Psychology. 2004;72:41–52. doi: 10.1037/0022-006X.72.1.41. [DOI] [PubMed] [Google Scholar]
- Polich JM, Orvis BR. Alcohol problems: Patterns and prevalence in the U.S Air Force . Santa Monica, CA: Rand; 1979. p. R-2308-AF. [Google Scholar]
- Robins LN, Helzer JH, Croughan J, Ratcliff KS. The NIMH Diagnostic Interview Schedule: Its history, characteristics, and validity. Archives of General Psychiatry. 1981;38:381–389. doi: 10.1001/archpsyc.1981.01780290015001. [DOI] [PubMed] [Google Scholar]
- Saewyc EM, Bearinger LH, Blum RW, Resnick MD. Sexual intercourse, abuse and pregnancy among adolescent women: Does sexual orientation make a difference? Family Planning Perspectives. 1999;31:127–131. [PubMed] [Google Scholar]
- Tjaden P, Thoeness N. Full report of the prevalence, incidence, and consequences of violence against women. Washington, DC: US Department of Justice; 2000. Research Report No NCJ 183781. [Google Scholar]
- Tjaden P, Thoeness N, Allison CJ. Comparing violence over the life span in samples of same-sex and opposite-sex cohabitants. Violence and Victims. 1999;14:413–425. [PubMed] [Google Scholar]
- Tomeo ME, Templer DI, Anderson S, Kotler D. Comparative data of childhood and adolescent molestation in heterosexual and homosexual persons. Archives of Sexual Behavior. 2001;30:535–541. doi: 10.1023/a:1010243318426. [DOI] [PubMed] [Google Scholar]
- Widom CS, Ireland T, Glynn PJ. Alcohol abuse in abused and neglected children followed-up: Are they at increased risk? Journal of Studies on Alcohol. 1995;56:207–217. doi: 10.15288/jsa.1995.56.207. [DOI] [PubMed] [Google Scholar]
- Widom CS, Morris S. Accuracy of adult recollections of childhood victimization: Part 2. Childhood sexual abuse. Psychological Assessment. 1997;9:34–46. [Google Scholar]
- Williams LM, Siegel JA, Pomeroy JJ. Validity of women’s self-reports of documented child sexual abuse. In: Stone A, Turkkan JS, Bachrach CA, Jobe HS, Kurtzman HS, Cain VS, editors. The science of self-report: Implications for research and practice. Mahwah, NJ: Lawrence Earlbaum; 2000. pp. 211–226. [Google Scholar]
- Wilsnack RW, Wilsnack SC, Klassen AD. Women’s drinking and drinking problems: Patterns from a 1981 national survey. American Journal of Public Health. 1984;74:1231–1237. doi: 10.2105/ajph.74.11.1231. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Wilsnack RW, Wilsnack SC, Kristjanson AF, Harris TR. Ten-year prediction of women’s drinking behavior in a nationally representative sample. Women’s Health: Research on Gender, Behavior, and Policy. 1998;4:199–230. [PubMed] [Google Scholar]
- Wilsnack SC, Vogeltanz ND, Klassen AD, Harris TR. Childhood sexual abuse and women’s substance abuse: National survey findings. Journal of Studies on Alcohol. 1997;58:264–271. doi: 10.15288/jsa.1997.58.264. [DOI] [PubMed] [Google Scholar]
- Wyatt GE. The sexual abuse of Afro-American and White-American women in childhood. Child Abuse & Neglect. 1985;9:507–519. doi: 10.1016/0145-2134(85)90060-2. [DOI] [PubMed] [Google Scholar]