

Abstract
The Information-Motivation-Behavioural skills model (Fisher & Fisher, 1992) was used to predict condom use among adolescents residing in a court-ordered inpatient substance abuse treatment programme (N = 271; 181 male and 90 female, primarily of minority ethnicity). In a predictive structural equation model, demographic variables, HIV transmission knowledge, and motivational variables of pro-condom norms and attitudes, and perceived susceptibility predicted condom use skills and condom use self-efficacy. Along with the other variables in the model, condom skills and condom self-efficacy were hypothesized to predict condom use over a three-month period. It was found that condom skills were predicted by greater age, pro-condom attitudes and greater perceived susceptibility. Condom self-efficacy was predicted by gender, pro-condom norms and condom attitudes. Condom use was significantly predicted by pro-condom norms and stronger condom self-efficacy. Both condom skills and knowledge did not significantly predict condom use. Significant demographic predictors of condom use included greater age and gender. Results suggest that changing personal attitudes about condoms and reinforcing the power of pro-condom beliefs among significant others will encourage condom use among adolescents who are at high risk for HIV and other STDs.
Introduction
While the overall incidence of HIV has been declining in the USA, it has been growing at alarming rates for adolescents, particularly among adolescents who abuse alcohol and other drugs. The Centers for Disease Control and Prevention (2000) estimates that at least half of all new HIV infections occur among adolescents or young adults under age 25. Within a six-year period beginning in 1993, the number of adolescents with HIV increased by 34%, making AIDS one of the leading causes of death among persons 15 to 24 years of age (Jemmott & Jemmott, 2000; Kirby, 2000; Rotheram-Borus, 2000). Combined with high rates of STDs, increasingly earlier onset of sexual activity and high levels of unprotected sex make the design of effective HIV prevention strategies for adolescents among the most urgent challenges facing the scientific and treatment communities today (Kirby, 2000; Rotheram-Borus et al., 2000; Santelli et al., 2001). Unfortunately, previous adolescent HIV prevention approaches have been characterized as producing only modest effects (DiClemente, 1997; Jemmott & Jemmott, 2000; Rotheram-Borus, 2000).
Most importantly, there is a continued need for theory-based HIV risk reduction interventions for adolescents. The current study examined the usefulness of an intervention-oriented model of factors associated with HIV and STD preventive behaviours in a sample of sexually active, culturally diverse adolescents with major substance abuse problems. Specifically, we used Fisher and Fisher's Information-Motivation-Behavioral skills (IMB) model of HIV preventive behaviour change to examine risk reduction behaviors in at-risk adolescents (Fisher & Fisher, 1992; 2000). Using structural equation modeling, we tested associations among IMB constructs specifically designed to reflect condom use as predictors of condom use among sexually active adolescents in court-ordered substance use treatment.
The Information-Motivation-Behavioural skills (IMB) model was designed to predict AIDS preventive behaviour (Fisher & Fisher, 1992). The IMB model proposes that HIV preventive behaviour, such as condom use during sexual intercourse, is a function of HIV prevention information, HIV prevention motivation, and AIDS prevention behavioural skills (Fisher & Fisher, 1992; Fisher et al., 1994). Specifically, the model states that HIV prevention information and motivation work through prevention behavioural skills to influence risk reduction behaviours (Fisher & Fisher, 1992). Furthermore, information and motivation are independent constructs, such as when persons who are well informed about AIDS but may not be motivated to practise preventive behaviours and when individuals are motivated to practise preventive behaviours but may not be well informed. Information and motivation, however, may relate to the practice of behavioural skills relevant to risk behaviour change. In the IMB model, preventive behavioural skills represent a final common pathway for predicting complex preventive behaviours, such as condom use. It is common for studies to use measures of self-efficacy for performing a behaviour, that is confidence that one has in the ability to perform a specific behaviour under challenging conditions (e.g. Murphy et al., 2001). However, self-efficacy serves as a proxy to behavioural skills and may not be as predictive of condom use than a direct observational skills assessment. An important feature of the current study was therefore to include both measures of self-efficacy and direct observation of condom use proficiency skills as indicators of behavioural skills in our application of the IMB framework.
The constructs of the IMB model are generalizable as long as the constructs have content that is specific to the target population. The IMB model has been generalized to many diverse populations, including heterosexual university students, HIV-positive and HIV-negative men who have sex with men (Fisher et al., 1994), and heroin addicts (Bryan et al., 2000). This study tests the IMB model in substance-abusing adolescent offenders, a population at high risk for HIV infection. Our study hypothesized that information and motivation would predict both condom use self-efficacy and condom use proficiency skills and these indexes of condom use skills would predict the percentage of times that condoms were used during sexual intercourse among sexually active adolescents in court-ordered substance use treatment.
Methods
Participants
The sample (N = 271; 181 male and 90 female) was drawn from consecutive admissions to a court-ordered adolescent inpatient substance abuse treatment programme between 1998 and 2000. Participants were excluded from the study if they refused to provide informed assent (N = 72) and/or their parents (or legal guardians) refused to provide written consent for participation (N= 20). In addition, participants with no history of vaginal, anal or oral sex in the larger study from which these data were excluded from this current study. No participants suffered from severe cognitive or psychiatric impairments (e.g. psychosis) that would have compromised their ability to complete the assessment or caused them to be referred to other facilities and treatment. All adolescents were fluent in spoken English, having been in the public school system in which English is the language of instruction.
Participants were predominantly inner-city, low-income, ethnic or racial minorities who abused alcohol, marijuana, and/or non-injection 'crack' cocaine. Their average age was 15.7 years (SD = 1.07; range 12 to 18 years), and their average level of education was 8.7 years (SD = 1.3) with 29% African-American, 10% Non-Hispanic White, 3% Caribbean (non-Haitian), 9% Haitian, 2% Asian or Pacific Islander, 31% Hispanic (1% Mexican, 8% Puerto Rican, 22% Cuban) and 16% of other ethnic backgrounds. Eighty-seven per cent reported living with family members prior to being court-ordered for drug abuse treatment.
Assessment procedures
Measures included: (a) demographics questionnaire, (b) inventory measuring HIV transmission risk behaviours, preventive knowledge, motivation and behavioural skills, and (c) observational assessment of condom use proficiency skills. All assessment procedures were conducted by experienced interviewers, trained to create a process sensitive to gender and cultural issues. To avoid interviewer drift and other contaminating factors, interviewers received ongoing supervision from a clinical psychologist for the duration of the study. Assessment measures were administered orally to facilitate accurate reporting, full completion, and to compensate for any literacy difficulties. Assessments were administered one week after admission and with clearance from treatment staff that detoxification was adequately achieved. This was done to minimize the effect of detoxification or withdrawal factors on test performance and to maximize accuracy of responses.
To enhance the validity of self-report data, interviewers: (a) used key events and calendar timelines; (b) were trained to adopt a non-judgemental stance during interactions and to establish rapport and build trust; (c) employed multiple questions and probes to ensure that respondents understood the meaning of each item; and (d) would repeat or elaborate questions if a respondent showed any evidence of confusion. To ensure confidentiality, increase cooperation and facilitate accurate reporting, we conducted (1) the interviews in a confidential manner, in a room that allowed for privacy, and (2) told participants that their responses would not be shared with treatment staff. In addition, as suggested by Jemmott et al. 1992, efforts were made to motivate participants to respond accurately in order to reduce the likelihood that reports of sexual experiences would either be minimized or exaggerated. Participants were informed that their responses would be used to help improve HIV-prevention programmes for others like themselves in substance abuse treatment.
Measures
The latent variables described below were primarily based on responses to multi-item scales that were hypothesized to reflect key constructs of the IMB model. In the current study, responses are used as measured indicators of underlying latent variables. Single items represent some constructs. As recommended by Fisher and Fisher (1992), all measures included in the model were specified to an HIV risk reduction behaviour and keyed to an HIV-risk reduction behaviour, in this case condom use during vaginal and anal intercourse.
Demographics
Sociodemographic data, including age, level of education, ethnicity and information about family situations, was collected using the Adolescent Drug Abuse Diagnosis Questionnaire (ADAD; Friedman & Utada, 1989), which has been recommended by the Center for Substance Abuse Treatment (McLellan & Dembo, 1993) for use with drug-abusing adolescents. Gender and age were included in the latent variable IMB model as important controls in this adolescent sample.
IMB constructs
Information was quantified by the number of correct responses to 12 items from an 18-item true/false questionnaire adapted from St. Lawrence et al. 1995. Each of the 12 items were specific to condom use (e.g. condoms make intercourse completely safe), and sexual behaviour (e.g. anal sex is risky because it transmits HIV); while the six excluded items focus on possible transmission modes (e.g. sharing a drinking glass, or mosquito bites) unrelated to sexual activity. The number of correctly answered items served as a single score indicator of Information.
Motivation
Pro-condom norms were assessed with a measure of perceived social norms adapted from Jemmott et al. 1992, which assesses how important the approval of referents were in using condoms. Key referents included 'most people important to you', 'your most recent sex partner,' 'your parents,' and 'your friends'. Responses ranged from 1, extremely unimportant, to 5, extremely important. Adolescents who are more motivated to use condoms are assumed to value the approval and opinions of these key referents (Ajzen & Fishbein, 1980). Each of the four items assessing importance by different individuals was used as an indicator latent variable of pro-condom norms.
Condom attitudes were assessed as a second motivational indicator with ten items from the AIDS Risk Reduction Model (ARRM) Questionnaire Revised (ARRM-QR; Gibson et al, 1992). The ARRM-QR was developed to reliably and validly measure HIV-specific constructs hypothesized by the ARRM model (Catania et al., 1990) to be predictive of HIV risk behaviors. Typical items from the scale included 'A condom is not necessary if you know the person' and 'Condoms are messy'. The items were scored on a 1, disagree strongly, to 4, agree strongly, scale and were reverse-scored where appropriate so that higher scores indicated a more positive attitude towards use of condoms. To reduce the number of indicators, the ten items were combined randomly into three parcels used as measured indicators and were labeled condom attitudes 1, condom attitudes 2, and condom attitudes 3. Means of the combined items were used to keep them in the same comparable metric.
Perceived susceptibility was used as a third indicator of motivation and was assessed by one item from the ARRM-QR: 'Sooner or later I expect to catch the HIV infection or AIDS'. This item was scored 1, disagree strongly, to 4, agree strongly, and not reverse-scored. Therefore, a high score indicates more feelings of vulnerability or susceptibility to AIDS.
Behavioural skills
Condom self-efficacy, defined as confidence to adopt and maintain HIV-preventive behaviours, specifically condom use (Bandura, 1997), was used as an indicator of condom use behavioural skills. Three items from the ARRM-QR were used to assess condom self-efficacy. Items included: 'It's hard to always use condoms', 'Safer sex is hard when you're really turned on to someone' and 'It's hard to use condoms if you feel you really know someone'. These items were scored 1, disagree strongly, to 4, agree strongly, and reverse-scored so that higher scores indicate greater self-efficacy.
Condom use proficiency skills were assessed as a second skills indicator of behavioural skills and were determined by rating the participant's ability to properly enact nine steps in correctly placing a condom on a penis model (adapted from Sorensen et al., 1991, Somlai et al, 1998). Participants were scored for the presence or absence of specific actions, including: opening the condom package without tearing the condom; pinching the tip of the condom to remove air; and the condom is rolled to the base of the penile model. This measure recorded observed actions and did not require subjective interpretations of response quality. Scores reflect the total number of correct steps.
Sexual risk behaviours
Sexual risk behaviours were assessed using a modified version of a sexual risk assessment instrument previously used in other research (Kalichman et al., 1996; Kelly et al., 1994). The sexual risk assessment included retrospective recall of numbers of sex partners, unprotected sex acts, and condom use during the previous three months. Percentage of unprotected sex acts (vaginal, oral and anal) was calculated and used as the dependent variable in this study. Based on focus groups and in-depth interviews, the research team added items to the survey and modified the language to be culturally sensitive to reflect the local terminology of the target population. In addition, a tabular, calendar-based format facilitated administration (i.e. a time-line follow-back procedure (Sobell & Sobell, 1980; 1995)) and promoted accurate recall. A three-month reporting period was chosen because recall has been shown to be most reliable up until three months (Kauth et al., 1991).
Data analyses
All analyses were performed using the EQS structural equation modeling (SEM) programme (Bentler, 2002). SEM compares a proposed hypothetical model explicating relationships in the data with a set of actual data. The closeness of the variance-covariance matrix implied by the hypothetical model to the empirical variance-covariance matrix is evaluated through various goodness of fit indices. The comparative fit index (CFI) and Robust CFI (RCFI), chi-square values (both Maximum Likelihood (ML χ2) and the adjusted Satorra-Bentler robust χ2 (S-B χ2), and the Root Mean Square Errors of Approximation (RMSEAs) were used as indicators of fit (Bentler, 2002; Bentler & Dudgeon, 1996; Hu & Bentler, 1999). The CFI and RCFI indicate the proportion of improvement in the overall fit of the hypothesized model relative to a null model in which all covariances between variables are zero. Values of 0.95 or greater are desirable for the CFI and RCFI (Hu & Bentler, 1999). Robust statistics are more appropriate when the data are multivariately kurtose. The RMSEA is helpful as an additional tool to evaluate fit because it indicates the size of the residuals. Values less than 0.06 indicate a relatively good fit between the hypothesized model and the observed data (Hu & Bentler, 1999).
The model presented here was guided by the IMB model (Fisher & Fisher, 1992). The model simultaneously examines whether information and motivation are significant predictors of skills and sexual self-efficacy, and whether skills and/or sexual self-efficacy in turn are predictors of percentage of unprotected sex in the past three months. Demographics were included for important controls in predicting risk reduction behavioural skills.
Results
Results showed that both male and female sexually active adolescents in this sample presented relatively high rates of risk behaviours for HIV and other STDs. The average percentage of condom-protected sex in the past three months was 66%. Eighty-one per cent reported less than 100% condom use in the past three months, and 34% reported never using a condom. The means, standard deviations and ranges for each IMB variable appear in Table 1. The mean knowledge test score was nine (SD = 2.12) out of a possible 12 correct responses. Motivation indicators of pro-condom norms and condom attitudes were generally high, and perceived susceptibility was low. The indicators of condom self-efficacy were not as high as those reported for the motivational constructs of pro-condom norms and condom attitudes. As measured by the number of correct steps demonstrated on the objective condom skills task, the average participant only performed about half of the nine steps correctly (mean = 4.6, mode = 4). Only 2% (n = 6) correctly performed all nine of the condom skills task steps, and two-thirds failed to correctly perform at least six of the steps. The most prevalent incorrect responses were pinching the tip of the condom and removing from the base (71%), failing to hold the condom at the base and withdraw after ejaculation (67%), removing air from the condom prior to putting it on (51%), and leaving space at the tip of the condom for ejaculation (42%).
Table 1.
Descriptive statistics and factor loadings of measured variables in the confirmatory factor analysis
| Variable | Range | Mean | SD | Factor loading* |
|---|---|---|---|---|
| Age in years | 12–18 | 15.68 | 1.19 | NA** |
| Gender (1 = male, 2 = female) | 1–2 | 1.33 | 0.47 | NA |
| Knowledge | 1–12 | 9.00 | 2.12 | NA |
| Pro-Condom Norms | ||||
| Important people | 1–5 | 4.16 | 1.14 | 0.61 |
| Sex partner | 1–5 | 4.18 | 1.09 | 0.51 |
| Parents | 1–5 | 4.31 | 1.16 | 0.49 |
| Friends | 1–5 | 3.49 | 1.39 | 0.62 |
| Condom Attitude | ||||
| Condom Attitude 1 | 1–4 | 3.35 | 0.67 | 0.67 |
| Condom Attitude 2 | 1–4 | 3.45 | 0.56 | 0.27 |
| Condom Attitude 3 | 1–4 | 3.17 | 0.63 | 0.61 |
| Perceived Susceptibility | 1–4 | 1.32 | 0.69 | NA |
| Condom Self-Efficacy | ||||
| Hard to always use (R)*** | 1–4 | 3.11 | 1.00 | 0.57 |
| Hard to use when turned on (R) | 1–4 | 2.57 | 1.16 | 0.59 |
| Hard to use if know person (R) | 1–4 | 2.75 | 1.10 | 0.49 |
| Condom skill | (0–9) | 4.68 | 2.10 | NA |
| Three-month unprotected sex (%) | (0–100) | 44% | 39 | NA |
Estimation of the IMB model
A preliminary confirmatory factor model estimated the factor structure and relationships among all of the latent variables and the demographic variables. Table 1 reports the factor loadings of the hypothesized factor structure. All factor loadings were significant (p ≤ 0.001). Fit indexes were also in the acceptable range: ML χ2 = 98.0, 73 df; CFI = 0.95, RMSEA = 0.03. Robust statistics were somewhat better: S-B χ2 = 92.1, 73 df; RCFI = 0.96, RMSEA = 0.03. The standardized kurtosis estimate was 6.0, which indicates that the Robust solution may be more reliable in this model. However, both methods indicated a well-fitting structure.
Table 2 reports the bivariate correlations among constructs of the model without any directionality of influence among them. Older adolescents demonstrated significantly better condom skills, but also reported significantly more unprotected sexual encounters. The girls reported more positive condom attitudes and more condom use self-efficacy. More knowledge was significantly associated with more positive condom attitudes, less perceived susceptibility, and greater condom skills, but also was associated with more unprotected sex. Pro-condom norms were significantly associated with positive condom attitudes, greater condom use self-efficacy, and less unprotected sex.
Table 2.
Correlations among constructs in IMB model.
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
|---|---|---|---|---|---|---|---|---|
| 1. Knowledge | — | |||||||
| 2. Pro-condom norms | −0.13 | — | ||||||
| 3. Condom attitudes | 0.40*** | 0.29*** | — | |||||
| 4. Perceived susceptibility | −0.14** | −0.04 | − 0.26*** | — | ||||
| 5. Condom skills | 0.15* | 0.08 | 0.24*** | 0.04 | — | |||
| 6. Condom self-efficacy | 0.10 | 0.32*** | 0.64*** | −0.14 | 0.08 | |||
| 7. Three-month unprotected sex | 0.15** | − 0.22*** | −0.21** | −0.01 | 0.05 | −0.26*** | — | |
| 8. Age | 0.08 | −0.12 | −0.02 | −0.01 | 0.15** | −0.10 | 0.15** | — |
| 9. Female gender | 0.10 | 0.08 | 0.24*** | −0.05 | 0.03 | 0.33*** | 0.07 | −0.15* |
All factor loadings significant, p ≤ 0 .001.
NA = Not applicable, single-item indicator.
(R) = reverse-scored.
Favourable condom attitudes were significantly associated with each IMB variable except age, including negative associations with perceived susceptibility and unprotected sex. Condom attitudes were positively associated with the variables already reported above, and also with the objective measure of condom skills, and condom use self-efficacy. It is also noteworthy that the association of condom attitudes with other constructs was higher among the girls. Greater condom use self-efficacy was associated with less unprotected sex.
The final predictive IMB structural equation model is presented in Figure 1 after model trimming; through use of procedures suggested by MacCallum (1986), non-significant paths were gradually dropped until only significant ones remained. Measured variables are in rectangles and the multiply indicated latent variables are in ovals. Fit indexes were acceptable: ML χ2 = 117.8, 91 df; CFI = 0.94, RMSEA = 0.033. Robust statistics were better: S-B χ2 = 112.2, 91 df; RCFI = 0.95, RMSEA = 0.02.
Fig. 1.
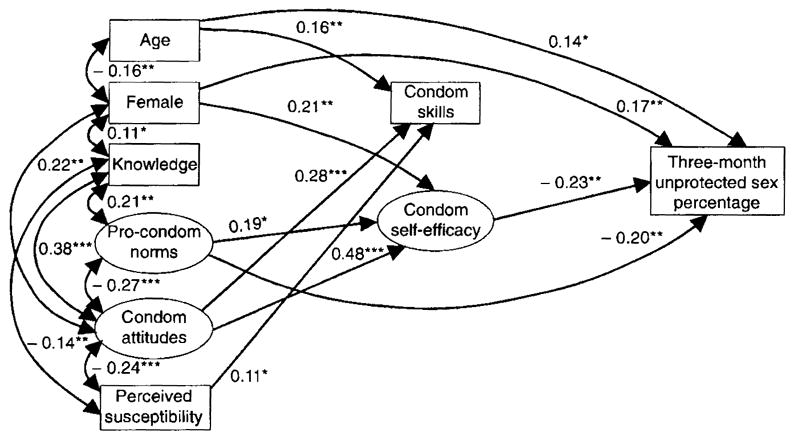
Significant regression paths in IMB model predicting three-month unprotected sex percentage among 271 inpatient adolescents with substance abuse problems. Ovals represent latent variables, rectangles represent single-item indicators. Lines with single arrows represent regression paths, double-headed arrows represent significant correlations between the predictors. Regression coefficients are standardized (*=p ≤ 0.0 5, **=p ≤ 0.01, ***=p ≤ 0.001).
Greater condom skills were predicted by age, condom attitudes and greater perceived susceptibility. Condom use self-efficacy was predicted by female gender, pro-condom norms and condom attitudes. Significant predictors of more unprotected sex included both age and female gender. Less unprotected sex was predicted by pro-condom norms and more condom self-efficacy. In addition, although positive condom attitudes were not a significant direct predictor of less unprotected sex, they were a significant indirect predictor, exerting influence through condom use self-efficacy (p ≤ 0.05). In addition, although female gender was a positive direct predictor of reporting more unprotected sex, its indirect effect as mediated through greater condom use self-efficacy was negative (p ≤ 0.05).
Discussion
The current study finding are likely to have important theoretical and practical implications for refining HIV and STD risk reduction interventions for adolescents. However, these implications may be constrained by several methodological limitations. Our study, like others in the field of HIV and STD risk and prevention, relied heavily on self-report behavioural instruments. Due to the sensitivity of sexual and substance use issues that we assessed, social desirability, privacy concerns and potential embarrassment may have lead to concealment of behaviours and therefore under-reporting. Although our study included a measure of direct observation for condom use proficiency skills, the possible effects of self-report biases on all other measures must be considered. In addition, the current study was conducted with adolescents residing in a court-ordered substance use inpatient treatment facility in an AIDS epicentre. Therefore, the study findings may have limited generalizability to other adolescent populations. Finally, our findings are based on a relatively small sample size, suggesting the need for further studies to replicate the observed associations. Despite these study limitations, the current findings are likely to offer new information regarding HIV and other STD risks and the use of the IMB model in predicting risk reduction behaviours in adolescents.
Consistent with the IMB model, indicators of motivation for reducing risks were significantly associated with risk reduction behavioural skills. In addition, motivational indicators, specifically pro-condom social norms and pro-condom attitudes, exerted direct and indirect effects, respectively, on the proportion of sexual episodes in which condoms were used. Also as predicted by the IMB model, a significant relationship was observed between an indicator of condom use behavioural skills, condom use self-efficacy and condom use. However, counter to our expectations, no associations were found between condom use-related knowledge, our indicator of information in the IMB model, and motivational factors, behavioural skills or condom use. The lack of effects of condom knowledge on condom use were not surprising, given previous research showing that information about risks and risk-reducing behaviours is often insufficient to change risk behaviour (Fishbein et al, 1994). Although of public health value, information or knowledge of condom use appears insufficient in predicting condom use.
An important theoretical finding in the current study was the contrasting effects of condom proficiency skills assessed by direct observation versus condom use self-efficacy assessed by self-report. There were robust associations among condom use self-efficacy, condom attitudes, pro-condom norms and condom use. These associations were consistent with those predicted by the IMB model. In contrast, condom-use skills assessed by direct observation were not significantly associated with condom use per se. Condom proficiency skill tasks are commonly used in HIV risk-reduction intervention outcome studies and have appeared superior to self-report measures because they are likely to be less susceptible to demand characteristics and other sources of response bias (Kelly et al., 1994; Malow et al., 1998; Somlai et al., 1998). Unfortunately, our study findings do not support using objectively assessed condom application skills as predictors of condom use, even in the context of our use of cross-sectional data that could maximize our sensitivity to detect such a relationship. Self-efficacy measures therefore represent a less expensive means of assessing condom use skills in the IMB framework in terms of staff time, training and participant burden without compromising results. In summary, the potential reactive practice effects of direct observation skills assessments do not appear to be offset by any value in advantages in predicting condom use. Our findings therefore caution against relying on objective measures of condom use proficiency skills as a marker for condom skills in the IMB framework or more generally as a predictor of condom use.
The current study also found that participant age and gender influenced the observed associations between IMB constructs and condom use, as well as exerting their own independent effects on condom use. Perhaps of greatest interest were the effects of gender on condom use self-efficacy and condom use. Female participants displayed more knowledge, were somewhat younger and reported strong pro-condom attitudes, yet in the structural equation model were less likely to have used condoms. This result may demonstrate a power imbalance in that, despite their desire to use a condom, girls acquiesce to their male partner's desire for unprotected sex. Also, since the study was conducted among heavy substance abusers, it is likely that many female participants may have been engaged in trading sex for drugs, a circumstance in which they have little power or control. Gender-power relations have been shown important in explaining risk and protective behaviours in adolescents and adults (Wingood & DiClemente, 2000). Our findings once again suggest the potential importance of gender in relation to HIV risk reduction and strongly suggest that predictors of risk be interpreted in the context of gender and that risk reduction interventions be tailored for gender relevance and to address relationship power issues.
Our study findings also have important implications for designing HIV risk reduction interventions for at-risk adolescents. First, as noted above, we failed to find significant associations among condom knowledge and indicators of motivation to use condoms, condom skills or condom use. One possible reason for this lack of association was the relatively high scores on the condom knowledge scale, which restricted the variability of our measure and its predictive value in our analyses. However, we observed considerable variability in condom use despite these high levels of condom knowledge and therefore conclude that condom knowledge alone is insufficient to predict condom use. In contrast, motivational factors, including condom attitudes and pro-social norms, were important predictors in our model. Because motivational influences such as attitudes and perceived norms are targets for cognitive and behavioural interventions, these associations have direct relevance for refining behavioural interventions. For example, techniques for enhancing motivation, such as using motivational interviewing strategies (Miller & Rollnick, 1991) to reduce risk behaviours, have become increasingly popular in interventions for adults at risk for HIV and other STDs (Carey et al., 1997; Kalichman et al., 1999). Motivation-enhancing techniques seem indicated in interventions for adolescents and should be tested in future research. In contrast, the lack of robust associations between perceived susceptibility and condom use suggests that risk sensitization or increased threat techniques may offer limited effects on risk reduction behaviours. Finally, intervention strategies that build condom use self-efficacy, that is, confidence in the ability to use condoms under challenging conditions, appear important in increasing condom use (Murphy et al., 2001). Condom use proficiency skills training is one approach to building self-efficacy and reducing risks for condom slippage and breakage, even if proficiency skills per se do not necessarily predict condom use. Research is needed to test the effects of IMB constructs on HIV risk reduction intervention outcomes as well as the effectiveness of interventions grounded in the IMB model. Given the immediate risks posed to adolescents who use alcohol and other drugs, developing and testing of such interventions should be given high priority.
Acknowledgments
This work was funded in part by grants RO1 DAI 1875 from NIDA and RO1 AA11752 from NIAAA awarded to Dr Malow, and DA 01070–28 to Dr Stein.
References
- Ajzen I, Fishbein M. Understanding attitudes and predicting social behavior. Englewood Cliffs, NJ: Prentice Hall; 1980. [Google Scholar]
- Bandura A. Self-efficacy: the exercise of control. New York: Freeman; 1997. [Google Scholar]
- Bentler PM. EQS 6 structural equations program manual. Encino, CA: Multivariate Software, Inc; 2002. [Google Scholar]
- Bentler PM, Dudgeon P. Covariance structure analysis: Statistical practice, theory, and directions. Annual Review of Psychology. 1996;47:563–592. doi: 10.1146/annurev.psych.47.1.563. [DOI] [PubMed] [Google Scholar]
- Bryan AD, Fisher JD, Fisher WA, Murray DM. Understanding condom use among heroine addicts in methadone maintenance using the Information-Motivation-Behavioral Skills model. Substance Abuse and Misuse. 2000;35:451–471. doi: 10.3109/10826080009147468. [DOI] [PubMed] [Google Scholar]
- Carey MP, Maisto SA, Kalichman SC, Forsyth A, Wright I, Johnson BT. Enhancing motivation to reduce risk for HIV infection for economically disadvantaged urban women. Journal of Consulting and Clinical Psychology. 1997;65:531–541. doi: 10.1037//0022-006x.65.4.531. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Catania JA, Kegeles SM, Coates TJ. Towards an understanding of risk behavior: an AIDS risk reduction model (ARRM) Health Education Quarterly. 1990;17:53–72. doi: 10.1177/109019819001700107. [DOI] [PubMed] [Google Scholar]
- Centers For Disease Control and Prevention. Sexually transmitted disease surveillance. Atlanta, Georgia: US Department of Health and Human Services, CDC; 2000. [Google Scholar]
- DiClemente R. Look forward: future directions for prevention of HIV among adolescents. In: Sherr L, editor. AIDS and adolescents. New York: Harwood Academic; 1997. pp. 189–199. [Google Scholar]
- Fishbein M, Middlestadt S, Hitchcock P. Using information to change sexually transmitted disease-related behaviors: an analysis based on theory of reasoned action. In: DiClemente R, Peterson J, editors. Preventing AIDS: theories, methods, and behavioral interventions. New York: Plenum Press; 1994. pp. 61–77. [Google Scholar]
- Fisher JD, Fisher WA. Changing AIDS-risk behavior. Psychological Bulletin. 1992;111:455–474. doi: 10.1037/0033-2909.111.3.455. [DOI] [PubMed] [Google Scholar]
- Fisher JD, Fisher WA. Theoretical approaches to individual-level change in HIV risk behavior. In: Peterson JL, DiClemente RJ, editors. Handbook of HIV prevention. New York: Kluwer Academic/Plenum Press; 2000. pp. 3–55. [Google Scholar]
- Fisher JD, Fisher WA, Malloy TE. Empirical tests of an information-motivation-behavioral skills model of AIDS-preventive behavior with gay men and heterosexual university students. Health Psychology. 1994;13:238–250. doi: 10.1037//0278-6133.13.3.238. [DOI] [PubMed] [Google Scholar]
- Friedman AS, Utada A. Adolescent drug abuse diagnosis. Philadelphia, PA: Belmont Center For Comprehensive Treatment; 1989. [Google Scholar]
- Gibson DR, Lovelle-Drache J, Young MT, Chesney M. HIV risk linked to psychopathology in IV drug users. International Conference on AIDS, Abstract POC 4691. 1992:1992. [Google Scholar]
- Hu LT, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Structural Equation Modeling. 1999;6:1–55. [Google Scholar]
- Jemmott J, Jemmott L. HIV behavioral interventions for adolescents in community settings. In: Peterson J, DiClemente R, editors. Handbook of HIV prevention. New York: Kluwer Academic/Plenum Press; 2000. pp. 103–127. [Google Scholar]
- Jemmott JB, Jemmott LS, Fong GT. Reductions in HIV risk-associated sexual behaviors among Black male adolescents: effects of an AIDS prevention intervention. American Journal of Public Health. 1992;82:372–377. doi: 10.2105/ajph.82.3.372. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kalichman SC, Cherry C, Brown-Sperling F. Effectiveness of a video-based motivational skills-building HIV risk reduction intervention for inner-city African-American men. Journal of Consulting and Clinical Psychology. 1999;67:959–966. doi: 10.1037//0022-006x.67.6.959. [DOI] [PubMed] [Google Scholar]
- Kalichman SC, Rompa D, Coley B. Experimental component analysis of a behavioral HIV-AIDS prevention intervention for inner-city women. Journal of Consulting and Clinical Psychology. 1996;64:687–693. doi: 10.1037//0022-006x.64.4.687. [DOI] [PubMed] [Google Scholar]
- Kauth MR, Lawrence JS, Kelly JA. Reliability of retrospective assessments of sexual HIV risk behavior: a comparison of biweekly, 3-month, and 12-month self reports. AIDS Education and Prevention. 1991;3:207–214. [PubMed] [Google Scholar]
- Kelly JA, Murphy DA, Washington CD, Wilson TS, Koob JJ, Davis DR, Ledezma G, Davantes B. The effects of HIV/AIDS intervention groups for high-risk women in urban clinics. American Journal of Public Health. 1994;84:1918–1922. doi: 10.2105/ajph.84.12.1918. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kirby D. School-based interventions to prevent unprotected sex and HIV among adolescents. In: Peterson J, DiClemente R, editors. Handbook of HIV prevention. New York: Kluwer Academic/Plenum Press; 2000. pp. 83–101. [Google Scholar]
- MacCallum R. Specification searches in covariance structure modeling. Psychological Bulletin. 1986;100:107–120. [Google Scholar]
- Malow R, Gustman S, Ziskind D, McMahon R, Lawrence J. Evaluating HIV prevention interventions among drug abusers: Validity issues. Journal of HIV/AIDS Prevention & Education for Adolescents and Children. 1998;2:21–40. [Google Scholar]
- McLellan T, Dembo R. Improvement Protocol (TIP) Volume 3: Screening and assessment of Alcohol and Other Drug (AOD) abusing adolescents. Treatment improvement protocol series. DHHS: Center for Substance Abuse Treatment. Washington, DC: US Department of Health and Human Services, Public Health Service; 1993. [Google Scholar]
- Miller WR, Rollnick S. Motivational interviewing: Preparing people to change addictive behavior. New York: Guilford Press; 1991. [Google Scholar]
- Murphy DA, Stein JA, Schlenger W, Maibach E The National Institute of Mental Health Multi-Site HIV Prevention Trial Group. Conceptualizing the multidimensional nature of self-efficacy: assessment of situational context and level of behavioral challenge to maintain safer sex. Health Psychology. 2001;20:281–290. [PubMed] [Google Scholar]
- Rotheram-Borus MJ. Expanding the range of interventions to reduce HIV among adolescents. AIDS. 2000;14(Suppl 1):33–40. doi: 10.1097/00002030-200006001-00005. [DOI] [PubMed] [Google Scholar]
- Santelli J, Robin L, Brener N, Lowry R. Timing of alcohol and other drug use and sexual risk behaviors among unmarried adolescents and young adults. Family Planning Perspectives. 2001;33:200–205. [PubMed] [Google Scholar]
- Sobell LC, Sobell MB. Convergent validity: an approach to increasing confidence in treatment outcome conclusions with alcohol and drug abusers. In: Sobell L, Sobell M, Ward E, editors. Evaluating alcohol and drug abuse treatment effectiveness: recent advances. New York: Pergamon Press; 1980. pp. 177–183. [Google Scholar]
- Sobell L, Sobell MB. NIAAA Treatment Handbook Series 4, Assessing alcohol problems: a guide for clinicians and researchers. 1995. Alcohol consumption measures; pp. 55–73. NIH publication no. 95-3745. [Google Scholar]
- Somlai A, Kelly J, McAuliffe T, Gudmundson J, Murphy D, Sikkema K, Hackl K. Role play assessments of sexual assertiveness skills: relationships with HIV/AIDS sexual risk behavior practices. AIDS and Behavior. 1998;2:319–328. [Google Scholar]
- Sorensen JL, London J, Morales E. Group counseling to prevent AIDS. In: Sorensen J, Wermuth D, Gibson K, Choi J, Guydish S, Batki S, editors. Preventing AIDS in drug users and their sexual partners. New York: Guilford Press; 1991. pp. 99–115. [Google Scholar]
- Lawrence JS, Jefferson KW, Alleyne E, Brasfield TL. Comparison of education versus behavioral skills training interventions in lowering sexual HIV-risk behavior of substance-dependent adolescents. Journal of Consulting and Clinical Psychology. 1995;63:154–157. doi: 10.1037//0022-006x.63.1.154. [DOI] [PubMed] [Google Scholar]
- Wingood G, DiClemete R. Application of the theory of gender and power to examine HIV-related exposures, risk factors, and effective interventions for women. Health Education and Behavior. 2000;27:539–565. doi: 10.1177/109019810002700502. [DOI] [PubMed] [Google Scholar]