

Abstract
We have completed a single ascending dose clinical study of the proposed chemopreventive agent 3, 3′-dindolylmethane (DIM). The study agent was nutritional-grade, absorption-enhanced BioResponse® 3, 3′-diindolylmethane (BR-DIM). We determined the safety, tolerability, and pharmacokinetics of single doses of BR-DIM in drug-free, non-smoking, healthy men and women. Groups of four subjects were enrolled for each dose level. After randomization, one subject in each group received placebo while three received active BR-DIM. Doses administered were 50, 100, 150, 200, and 300 mg, with the 300 mg dose repeated in an additional group. No BR-DIM-related adverse effects were reported at doses up to 200 mg. At the 300 mg dose, one of six subjects reported mild nausea and headache and one also reported vomiting. Only the latter effect was judged as probably related to study agent. Analysis of serial plasma samples showed that only one subject at the 50 mg dose had detectable concentrations of DIM. The single 100 mg dose of BR-DIM resulted in a mean Cmax of 32 ng/ml, and a mean AUC of 128 hr*ng/ml, and a single 200 mg dose produced a mean Cmax of 104 ng/ml and a mean AUC of 553 hr*ng/ml. The single 300 mg dose of BR-DIM resulted in a mean Cmax of 108 ng/ml and a mean AUC of 532 hr*ng/ml. We conclude that BR-DIM is well tolerated at single doses of up to 200 mg, and that increasing the dose to 300 mg did not result in an increase in Cmax.
Introduction
Cruciferous vegetables such as cabbage, broccoli, cauliflower and brussel sprouts contain several chemicals which have been shown to modulate carcinogenesis in animals (1-10) and humans (11, 12). Among these compounds is glucobrassicin (3-indolylmethyl glucosinolate). Glucobrassicin undergoes autolysis, forming indole-3-carbinol (I3C), indole-3-acetonitrile and 3,3′-diindolylmethane (DIM), a dimer of I3C. I3C has been shown to have pronounced chemopreventive effects against development of both spontaneous (4, 6) and chemically-induced (1-3, 5, 7-10) tumors in rats, mice, and trout. These chemopreventive effects of I3C were reported against tumor development in mammary gland (1, 4, 7), liver (2, 3), lung (5, 8), cervix (6, 9), and gastrointestinal tract (1). Our previous study of the tolerability, pharmacokinetics, and effects of oral I3C in humans demonstrated that the only detectable circulating product was DIM (13).
Our observations that no I3C was detectable in the plasma of women ingesting the compound, that DIM was the only I3C-derived compound detected (13), and that the ingestion of I3C elicited changes in drug and estrogen metabolism consistent with proposed chemoprevention mechanisms (14), when coupled with other reports supporting DIM as a major active chemopreventive agent derived from I3C (15-17), led to this study of DIM itself as a possible chemopreventive supplement. DIM, however, is poorly absorbed from the gastrointestinal tract. To address this potential problem, a formulation of DIM was administered that provides increased bioavailability of the compound, as shown by preliminary preclinical (18, 19) and clinical studies (17). We are studying Nutritional-grade BioResponse-DIM® (BR-DIM), the absorption-enhanced DIM formulation, in healthy men and women in a Phase I clinical trial. As reported here, we examined the safety and tolerability of single ascending doses of BR-DIM in drug-free men and women found healthy by medical histories, physical examinations and a battery of blood and urine tests. We also determined the pharmacokinetics of BR-DIM in these subjects. Based on the safety and tolerability of single doses of BR-DIM determined in this study, a separate protocol has been developed for a multiple-dose study of BR-DIM. In addition to studying the safety, tolerability and pharmacokinetics of single and multiple doses of BR-DIM, the follow-up protocol will evaluate the effects of BR-DIM on enzymes controlling the disposition of clinically used drugs, toxicants, and steroids.
Materials and Methods
Test compounds
3, 3′-Diindolylmethane (DIM); Nutritional-grade BioResponse-DIM® 150 Capsules (BR-DIM; 50 mg DIM per capsule [BioResponse, LLC, Boulder, CO]) and matching Placebo Capsules were supplied by the Division of Cancer Prevention, National Cancer Institute. BR-DIM is a patented oral formulation containing d-alpha-tocopheryl acid succinate, phosphatidylcholine, and silica microencapsulated in starch (20). This formulation exhibits higher bioavailability than does crystalline DIM (19).
Subjects and treatments
Men and women aged 22 to 58 who had negative results for tobacco use, based on urine cotinine, and for a drug screen, were enrolled. All enrolled subjects were free of acute, unstable, chronic or recurring medical conditions and with calculated BMI between 18 and 30. Characteristics of enrolled subjects are provided in Table 1. Strict vegetarians or individuals who ate more than 3 medium servings (1/2 cup each) of cruciferous vegetable per week were excluded. Those who stopped ingesting cruciferous vegetables ≥ 14 days and alcohol ≥ 7 days before starting this study were not excluded. Participants completed a brief diet questionnaire to assess these criteria. Caffeine- and grapefruit-containing foods and beverages were avoided by subjects for at least 48 hours before BR-DIM dosing. All subjects had blood and urine chemistries and complete blood cell counts within normal ranges, and all women had negative pregnancy tests prior to BR-DIM administration. All protocols, procedures, informed consent, and other forms were reviewed and approved by the Human Subjects Committee of the University of Kansas Medical Center.
Table 1. Subject Characteristics.
| Subject | Age | Sex | Weight (pounds) | Height (inches) | BMI | Study Drug Dose (mg) |
|---|---|---|---|---|---|---|
| 201 | 38 | Female | 157 | 62 | 28.8 | 50 |
| 202 | 55 | Female | 172 | 66 | 27.8 | 50 |
| 203 | 24 | Female | 159 | 68 | 24.2 | 50 (P) |
| 204 | 23 | Male | 166.5 | 74 | 21.4 | 50 |
| 206 | 23 | Male | 149 | 71 | 20.8 | 100 |
| 207 | 58 | Female | 144.5 | 65 | 24.1 | 100 |
| 208 | 23 | Male | 154.4 | 71 | 21.6 | 100 (P) |
| 209 | 25 | Female | 169 | 69 | 25.0 | 150 |
| 210 | 22 | Male | 139.4 | 72 | 19.0 | 100 |
| 211 | 25 | Male | 211.5 | 74 | 27.2 | 150 (P) |
| 212 | 25 | Male | 204 | 73 | 27.0 | 150 |
| 213 | 25 | Male | 128 | 70 | 18.4 | 150 |
| 215 | 24 | Female | 125 | 62 | 22.9 | 200 |
| 216 | 54 | Female | 131 | 64 | 22.5 | 200 (P) |
| 217 | 47 | Female | 111 | 64 | 19.1 | 200 |
| 218 | 25 | Male | 182.5 | 72 | 24.8 | 300 |
| 219 | 25 | Male | 225.5 | 78 | 26.1 | 200 |
| 220 | 30 | Female | 138.5 | 66 | 22.4 | 300 |
| 222 | 28 | Male | 184.5 | 73 | 24.4 | 300 |
| 223 | 24 | Female | 146 | 64 | 25.1 | 300 (P) |
| 225 | 28 | Male | 161 | 71 | 22.5 | 300 (P) |
| 226 | 44 | Male | 191 | 67 | 30.0 | 300 |
| 227 | 44 | Male | 167 | 71 | 23.3 | 300 |
| 228 | 44 | Female | 136 | 67 | 21.3 | 300 |
(P) = Placebo
Dosing and Sampling Procedures
Subjects, who had fasted overnight, had an intravenous catheter inserted and then were administered their oral dose of BR-DIM or matching placebo with 200 ml water. Fasting was continued for an additional two hrs to allow for absorption of DIM. Blood samples were collected into heparinized tubes immediately prior to and at 0.5, 1, 1.5, 2, 3, 4, 6, 8, 12, and 24 hrs after dosing for determination of plasma DIM concentrations. Samples were immediately placed in ice, and plasma was prepared within 30 min of sampling. Plasma samples were stored below -70° C, and analyzed within 4 months of acquisition. Subjects were observed and vital signs monitored during the first 12 hrs and at the 24 hr sampling time.
Plasma DIM Analysis
All samples were analyzed under contract at the School of Pharmacy, Texas Tech University-Health Sciences Center (Dallas, TX). The plasma samples were analyzed for DIM by LC-MS using a validated method (13), which involves the extraction of DIM from human plasma into diethyl ether. Indole-3-ethanol (I3E) was used as the internal standard. Separation was achieved by reverse phase HPLC. The mass spectrometer was operated in the selected ion recording (SIR) mode with ionization via positive ion electrospray. Ions with a m/z value of 130 Da (DIM), 162.1 Da (I3E parent ion, M+1), 247 Da (DIM parent ion, M+1) and 263 Da [hydroxylated DIM parent ion, (M+1)] were monitored.
Pharmacokinetic analysis
The data were analyzed using non-compartmental methods (WinNonlin, Version 5.1, SCI, Cary, North Carolina). Plasma concentration data were analyzed separately for each subject using this model-independent method of pharmacokinetic analysis in order to obtain area under the concentration-time curve up to the last measurable timepoint (AUC0-t), maximum plasma concentration (Cmax) and time to reach Cmax (Tmax). Additionally, plasma concentrations for each individual were analyzed to provide an estimate of the elimination half-life (t½) for the DIM. Area under the concentration time curve (AUC0-t) was calculated using the trapezoidal rule.
Results
We have completed dosing of subjects with single ascending doses of BR-DIM. There were 6 groups of 4 subjects each (3 DIM and 1 matching placebo in each group). Treatment groups received 50, 100, 150, 200 and 300 mg DIM, with a second group receiving the highest (300 mg) dose. All adverse events in these subjects are listed in Table 2. One subject reported headache and nausea and another became nauseated and vomited after receiving a 300 mg BR-DIM dose. In addition, one subject complained of nausea and headache, but was found after breaking the randomization code to have received placebo, rather than active BR-DIM. Two subjects, one receiving a 150 mg dose and the other a 200 mg dose of BR-DIM, complained of flatulence. All adverse events were classified as grade I, defined as mild, self-limiting, and not requiring treatment. Based on subject examination and on consideration of the time of onset and resolution of adverse effects relative to DIM administration, only the vomiting after the 300 mg dose was classified as probably related to DIM.
Table 2. Cumulative Listing of Adverse Events.
| Subject | Study Drug Dose (mg) | Event | Event Grade | Event Duration | Relatedness/Attribution |
|---|---|---|---|---|---|
| 210 | 100 | Headache | 1 | 1 day | Unlikely |
| 209 | 150 | Flatulence Menstrual Spotting |
1 | 2 days | Unlikely |
| 216 | Placebo | Blurred Vision Headache Dizziness Loss of Appetite Nausea Vomiting |
1 | 1 day | Possibly |
| 219 | 200 | Flatulence | 1 | 3 days | Possibly |
| 222 | 300 | Headache Nausea | 1 | 1 day | Possibly |
| 228 | 300 | Vomiting Nausea |
1 | 1 day 2 days |
Probably |
Serial plasma samples from all subjects were analyzed by LC-MS for DIM concentration and pharmacokinetic parameters were calculated. Mean plasma DIM concentrations over sampling time are shown for each dose group in Fig. 1. No subjects had detectable DIM in their pre-dose plasma, and all subject’s DIM plasma concentrations had dropped to below our limit of detection by the 12 hr time point for BR-DIM doses of 150 mg or less, and at 24 hrs for all doses.
Figure 1. Mean Plasma Concentration Profiles for Single Doses of BR-DIM.
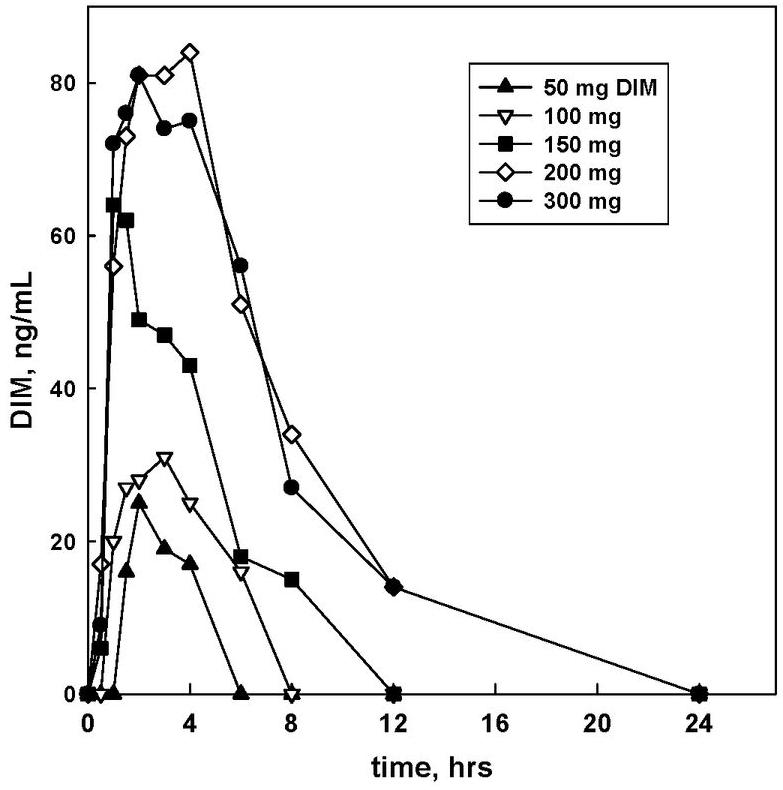
Values are the actual plasma concentrations of DIM for the single subject at the 50 mg BR-DIM dose with measurable plasma concentrations, and the mean values for all dosed subjects for the 100, 150, and 200 mg doses (n=3 per dose) and the 300 mg dose (n=6) of BR-DIM.
The pharmacokinetic parameters Cmax and tmax were determined for each subject by inspection, and AUC and t½ values were calculated for each individual subject. Mean values are reported for all doses except the 50 mg dose, where only one subject showed detectable DIM concentrations in plasma. These values are presented in Table 3, and their dose-dependence is presented in Fig. 2. The tmax and t1/2 values for DIM vary somewhat but show no trend as a function of BR-DIM dose. Cmax, however, increases in a linear fashion at least up to the 200 mg dose (Fig. 2A), and AUC is a linear function of dose throughout the dose range tested (Fig. 2B). These findings may be compared with our results for DIM in plasma obtained when the DIM precursor indole-3-carbinol (I3C) was administered orally to women (13), where both Cmax (Fig. 2C) and AUC (Fig. 2D) increased as a linear function of dose only at the lowest 2 doses of I3C, and then increased 8-12 times faster with increasing dose, compared to the relationship seen at the low doses.
Table 3. Single Dose Pharmacokinetic Parameters for BR-DIM.
| N | Dose, mg | tmax, hr | t1/2, hr | Cmax, ng/mL | AUC, hr*ng/mL |
|---|---|---|---|---|---|
| 1* | 50 | 2.0 | 3.5 | 25. | 62 |
| 3 | 100 | 2.7 ± 0.6 | 3.7 ± 1.2 | 32. ± 4 | 136 ± 8 |
| 3 | 150 | 1.8 ± 1.0 | 3.0 ± 0.6 | 79. ± 41. | 314 ± 249 |
| 3 | 200 | 2.5 ± 1.3 | 2.6 ± 0.7 | 104. ± 94. | 417 ± 441 |
| 6 | 300 | 2.2 ± 1.1 | 4.5 ± 1.4 | 108. ± 43. | 532 ± 289 |
Data are expressed as mean ± standard deviation.
Only one subject showed detectable DIM in plasma at this dose.
Figure 2. Dose-Dependency of DIM Pharmacokinetics following BR-DIM and I3C Administration.
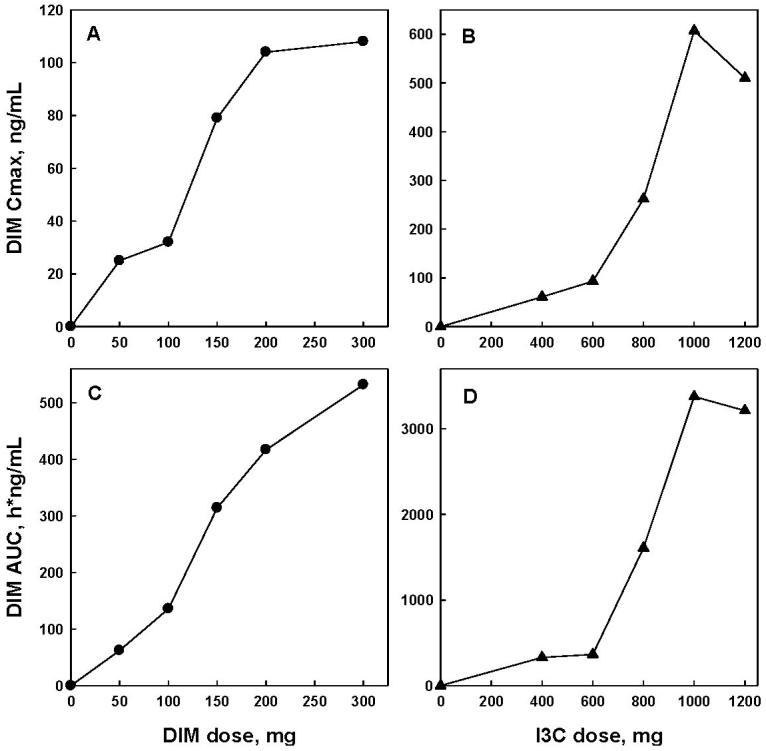
The observed Cmax and the calculated AUC for DIM from administration of different doses of BR-DIM (this study, Panels A and C, respectively) or from different doses of I3C (Ref. 13, Panels B and D, respectively). Values from subjects receiving BR-DIM (Panels A and C) are from a single subject at the 50 mg dose, and the mean values for 3 subjects at the 100, 150, and 200 mg doses and 6 subjects at the 300 mg dose. For subjects receiving I3C (Panels B and D), values shown are means of 4 subjects from the 400, 600, and 800 mg doses; 3 subjects at the 1000 mg dose, and 8 subjects at the 1200 mg dose.
When all plasma samples had been analyzed for DIM concentration and pharmacokinetic parameters calculated, all subjects were assessed for the relationship between Cmax and AUC for DIM and the occurrence of adverse effects. As shown in Fig. 3, no clear relationship or trend could be seen between either pharmacokinetic parameter and the incidence or severity of reported adverse effects. Even if the reported adverse effects from the subject receiving placebo are excluded, the remaining Cmax and AUC values appear clustered in the middle of the overall calculated ranges for these parameters. Subject 228, who exhibited the only adverse effect classified as probably related to BR-DIM, was found to have a Cmax of 82 ng/mL and an AUC of 272 h*ng/mL. Both of these values are exceeded in several subjects who reported no adverse effects. Whether this lack of correspondence between either AUC or Cmax for DIM with the occurrence of adverse effects is due to individual variability in susceptibility, or if it denotes that DIM did not actually cause those effects cannot be determined from our study.
Figure 3. Relationship Between DIM Plasma Concentrations and Adverse Events.
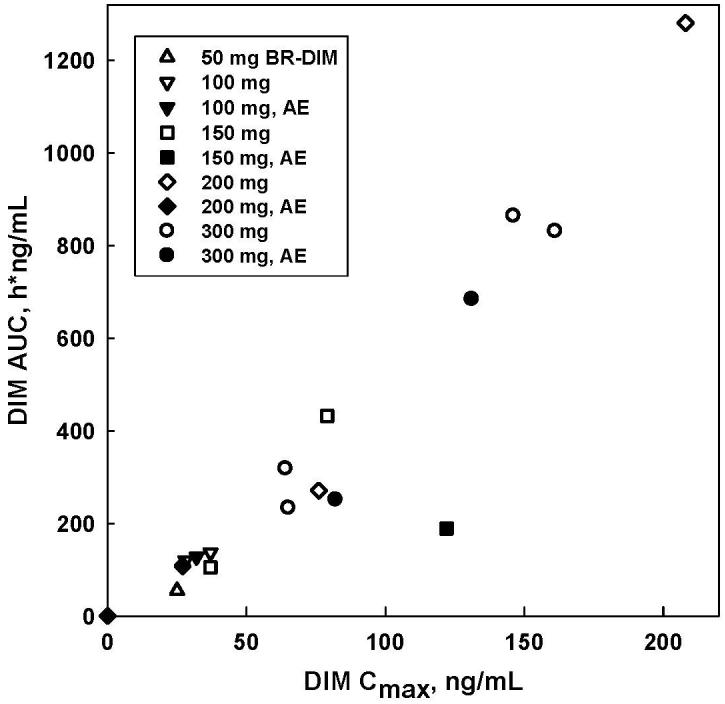
Points represent the Cmax and AUC for all subjects, with each subject’s dose of BR-DIM denoted as labeled. Filled symbols denote the 6 subjects reporting adverse effects, as listed in Table 2.
Discussion
Our results demonstrate that single doses of BR-DIM of up to 200 mg are well-tolerated by healthy subjects, and that even at a dose of 300 mg adverse effects were infrequent and of minimal severity. Although adverse effects were observed, several features suggest that these effects may not be caused by DIM. First, the time of onset and duration of some reported adverse effects are difficult to associate with the time of BR-DIM administration and its pharmacokinetics. Moreover, the incidence of adverse effects does not correlate with BR-DIM dose (Table 2). As shown in Fig. 3, the incidence of adverse effects also does not correlate with actual DIM exposure, based either on Cmax or on AUC. Finally, the most extensive range of adverse effects was from a subject who had received placebo, rather than active BR-DIM.
This tolerability of BR-DIM is consistent with the results of a pilot study in which nineteen post-menopausal women took BR-DIM (108 mg DIM daily) for thirty days (17). Of those subjects, one reported a rash that resolved with discontinuing the supplement and taking antihistamines, two reported increased hot flashes but continued to take the supplement, and one subject complained of nausea when BR-DIM was taken without food. BR-DIM also has been well-tolerated in our ongoing multiple-dose study. To date, fourteen healthy subjects have received twice-daily doses of either 100 mg or 200 mg BR-DIM for a four week period. This is a double-blind study, so no assignment by dose can be made prior to completion of all analyses, but adverse effects have not been reported by our subjects. The results of the pilot study in post-menopausal women (17), of our single ascending dose study reported here, and the preliminary findings of our current multiple-dose study with BR-DIM all support the tolerability of BR-DIM in this dose range.
Although most studies of the effects on I3C and related compounds on carcinogenesis in animal models have demonstrated chemopreventive effects (1-10), there have been reports of apparent tumor promotion by I3C in certain systems and at relatively high doses (21-23). A single report of tumor promotion by DIM, in an aflatoxin B1-initiated liver tumor model in trout, also has been published (24). A unifying feature of the studies showing tumor promotion by either I3C or DIM is the use of high doses of these supplements, and these doses appear to be associated with toxicity (25). These reports of possible tumor promoting activity for these indole derivatives is noteworthy, however the high doses employed in those studies and the associated toxicity both differ from the dosing regimens we have used and from our observations on tolerability and adverse effects reported here and in our current multiple dose study.
Examination and calculation of pharmacokinetic parameters for DIM from BR-DIM produce a tmax and t1/2 similar to those for DIM following ingestion of I3C (13). A comparison of Cmax and AUC values, however, shows that, when normalized to dose administered, BR-DIM produces 2-3 times higher values than does I3C. This could represent both the fractional conversion of I3C to DIM under acid conditions (26) and the lower bioavailability of DIM without the absorption-enhancing BR-DIM formulation.
Our inclusion and exclusion criteria were intended to minimize differences in general health, diet, social habits, and drug exposure as variables affecting DIM pharmacokinetics. Despite these restrictions, marked inter-individual variability in Cmax and AUC for DIM were noted (Table 2). When these values were compared among subjects at a given dose level no correlation or trend could be found with sex, age, or BMI. Normalizing Cmax and AUC to dose, expressed as mg/kg body weight, had minimal effects on the coefficient of variation for each dose group. Inter-individual variability in DIM metabolism might also contribute to the observed variability in pharmacokinetic parameters, however DIM metabolites have not been reported from in vivo studies. Staub et al. recently reported the formation of hydroxylated DIM sulfates by human breast cancer cells in culture (27), but the relevance of this finding to the intact organism is not known. It is noteworthy that Anderton et al. did not observe any DIM metabolites in either tissues or plasma of mice dosed with I3C (28) or DIM (19). The relative contributions to inter-individual variability in DIM pharmacokinetics of genetic variability and of additional dietary or environmental factors not addressed by our criteria cannot be assessed from this study.
Our pharmacokinetics data demonstrate a more linear dose-exposure relationship for BR-DIM, over the range from 50 mg to 300 mg, than was observed using the DIM precursor I3C (13). The mean Cmax for DIM is a linear function of BR-DIM up to the 200 mg dose (r2= 0.9552), and the mean AUC is a linear function of BR-DIM dose up to the 300 mg dose (r2= 0.9682). In contrast, DIM Cmax and AUC following ingestion of I3C deviated dramatically from linearity (Fig. 2). Such markedly dose-dependent pharmacokinetics presents a major challenge to standardization of dose and predictability of responses, thus the linearity of pharmacokinetics support BR-DIM as the more favored supplement for development as a chemopreventive agent.
The linearity of BR-DIM pharmacokinetics demonstrated here prompts a reexamination of our consideration of DIM pharmacokinetics when I3C, the precursor, is administered (13). We suggested that the increasing dose-normalized Cmax and AUC at increasing doses of I3C could represent a saturation of MDR1 and other efflux transporters in the enterocytes, thus increasing the net uptake of DIM. Given the increased linear range of Cmax and AUC with BR-DIM administration suggests that saturation of efflux is less likely. Rather, the superlinear increases observed with I3C may reflect increased DIM formation in a bimolecular reaction of I3C-derived reactants to produce DIM.
In our Phase 1 study of I3C we noted that DIM was the only detectable I3C-derived compound in plasma, and that no adverse effects were reported or observed at doses of 200 and 400 mg administered twice daily for 4 weeks (13, 14). The latter dose generated a Cmax of 69 ± 42 ng/mL and an AUC of 372 ± 180 h*ng/mL (13). These Cmax and AUC determined for DIM after four weeks of twice-daily 400 mg doses of I3C are only 13% higher than the corresponding values for a single dose of 400 mg, indicating no alteration in kinetics from the single dose case. This four week I3C treatment at 400 mg twice daily resulted in marked induction of CYP1A2, and in a doubling of the urinary 2-hydroxyestrone: 16α-hydroxyestrone ratio (14). Moreover, the change in the estrone hydroxylation ratio was obtained after four weeks at 200 mg I3C twice daily. Both of these changes elicited by I3C treatment fit with proposed mechanisms of chemoprevention by this agent, and if DIM is the active species eliciting these changes then we also have a target plasma concentration and AUC for chemoprevention. Our current findings with BR-DIM show that this target Cmax would be obtained at single dose of less than 150 mg, and that the target AUC would be achieved from a single dose between 150 and 200 mg. Based on this analysis, we are currently carrying out a multiple dose study with BR-DIM at doses of 100 mg and 200 mg administered twice daily. This study will assess the influence of BR-DIM on the activity of multiple hepatic enzymes including CYP1A2, CYP3A4, CYP2C9, and CYP2D6.
Acknowledgments
Grant support: Supported by NCI Contract N01-CN-35008.
References
- 1.Wattenberg LW, Loub WD. Inhibition of polycyclic aromatic hydrocarbon-induced neoplasia by naturally occurring indoles. Cancer Res. 1978;38:1410–1413. [PubMed] [Google Scholar]
- 2.Nixon JE, Hendricks JD, Pawlowski NE, et al. Inhibition of aflatoxin B1 carcinogenesis in rainbow trout by flavone and indole compounds. Carcinogenesis. 1984;5:615–619. doi: 10.1093/carcin/5.5.615. [DOI] [PubMed] [Google Scholar]
- 3.Fong AT, Hendricks JD, Dashwood RH, et al. Modulation of diethylnitrosamine-induced hepatocarcinogenesis and O6-ethylguanine formation in rainbow trout by indole-3-carbinol, α-naphthoflavone, and Aroclor 1254. Toxicol Appl Pharmacol. 1988;96:93–100. doi: 10.1016/0041-008x(88)90251-7. [DOI] [PubMed] [Google Scholar]
- 4.Bradlow HL, Michnovicz J, Telang NT, Osborne MP. Effects of dietary indole-3-carbinol on estradiol metabolism and spontaneous mammary tumors in mice. Carcinogenesis. 1991;12:1571–1574. doi: 10.1093/carcin/12.9.1571. [DOI] [PubMed] [Google Scholar]
- 5.Chung FL, Morse MA, Eklind KI, Xu Y. Inhibition of tobacco-specific nitrosamine-induced lung tumorigenesis by compounds derived from cruciferous vegetables and green tea. Ann NY Acad Sci. 1993;686:186–201. doi: 10.1111/j.1749-6632.1993.tb39174.x. [DOI] [PubMed] [Google Scholar]
- 6.Kojima T, Tanaka T, Mori H. Chemoprevention of spontaneous endometrial cancer in female donryu rats by dietary indole-3-carbinol. Cancer Res. 1994;54:1446–1449. [PubMed] [Google Scholar]
- 7.Grubbs CJ, Steele VE, Casebolt T, et al. Chemoprevention of chemically-induced mammary carcinogenesis by indole-3-carbinol. Anticancer Res. 1995;15:709–716. [PubMed] [Google Scholar]
- 8.El Bayoumy K, Upadhyaya P, Desai DH, et al. Effects of 1,4-phenylenebis (methylene)selenocyanate, phenethyl isothiocyanate, indole-3-carbinol, and d- limonene individually and in combination on the tumorigenicity of the tobacco-specific nitrosamine 4-(methylnitrosamino)-1-(3-pyridyl)-1-butanone in A/J mouse lung. Anticancer Res. 1996;16:2709–2712. [PubMed] [Google Scholar]
- 9.Jin L, Qi M, Chen D-Z, Anderson A, et al. Indole-3-carbinol prevents cervical cancer in human papilloma virus type 16 (HP V16) transgenic mice. Cancer Res. 1999;59:3991–3997. [PubMed] [Google Scholar]
- 10.Mori H, Sugie S, Rahman W, Suzui N. Chemoprevention of 2-amino-1-methyl-6-phenylimidazo[4,5]pyridine-induced mammary carcinogenesis in rats. Cancer Letters. 1999;143:195–198. doi: 10.1016/s0304-3835(99)00124-x. [DOI] [PubMed] [Google Scholar]
- 11.Verhoeven DTH, Goldbohm RA, van Poppel G, et al. Epidemiological studies on Brassica vegetables and cancer risk. Cancer Epidem. Biomarkers & Prev. 1996;5:733–748. [PubMed] [Google Scholar]
- 12.Keck A-S, Finley JW. Cruciferous vegetables: Cancer protective mechanisms of glucosinolate hydrolysis products and selenium. Integrative Cancer Therap. 2004;3:5–12. doi: 10.1177/1534735403261831. [DOI] [PubMed] [Google Scholar]
- 13.Reed GA, Arneson DW, Putnam W, III, et al. Single- and Multiple-Dose Administration of Indole-3-carbinol to Women: Pharmacokinetics Based on 3,3′-Diindolylmethane. Cancer Epidem. Biomarkers & Prev. 2006;15:2477–2481. doi: 10.1158/1055-9965.EPI-06-0396. [DOI] [PubMed] [Google Scholar]
- 14.Reed GA, Peterson KS, Smith HJ, et al. A phase I study of indole-3-carbinol in women: Tolerability and effects. Cancer Epidem. Biomarkers & Prev. 2005;14:1953–1960. doi: 10.1158/1055-9965.EPI-05-0121. [DOI] [PubMed] [Google Scholar]
- 15.Stresser DM, Bjeldanes LF, Bailey GS, Williams DE. The anti-carcinogen 3, 3′-diindolylmethane is an inhibitor of cytochrome P-450. J Biochem Toxicol. 1995;10:191–201. doi: 10.1002/jbt.2570100403. [DOI] [PubMed] [Google Scholar]
- 16.Le HT, Schaldach CM, Firestone GL, Bjeldanes LF. Plant-derived 3, 3′-diindolylmethane is a strong androgen antagonist in human prostate cancer cells. J Biol Chem. 2003;278:21136–21145. doi: 10.1074/jbc.M300588200. [DOI] [PubMed] [Google Scholar]
- 17.Dalessandri KM, Firestone GL, Fitch MD, et al. Pilot study: Effect of 3, 3′-diindolylmethane supplements on urinary hormone metabolites in postmenopausal women with a history of early-stage breast cancer. Nutrition and Cancer. 2004;50:161–167. doi: 10.1207/s15327914nc5002_5. [DOI] [PubMed] [Google Scholar]
- 18.Leibelt DA, Hedstrom OR, Fischer KA, et al. Evaluation of chronic dietary exposure to indole-3-carbinol and absorption-enhanced 3,3′-diindolylmethane in Sprague-Dawley rats. Toxicol Sci. 2003;74:10–21. doi: 10.1093/toxsci/kfg103. [DOI] [PubMed] [Google Scholar]
- 19.Anderton MJ, Manson MM, Verschoyle R, et al. Physiological modeling of formulated and crystalline 3, 3′-diindolylmethane pharmacokinetics following oral administration in mice. Drug Metab Dispos. 2004;32:632–638. doi: 10.1124/dmd.32.6.632. [DOI] [PubMed] [Google Scholar]
- 20.Zeligs MA, Jacobs IC. Compositions and methods of adjusting steroid hormone metabolism through phytochemicals. 6,086,915. U.S. patent. 2000
- 21.Kim DJ, Han BS, Ahn B, Hasegawa R, Shirai T, Ito N, Tsuda H. Enhancement by indole-3-carbinol of liver and thyroid gland neoplastic development in a rat medium-term multiorgan carcinogenesis model. Carcinogenesis. 1997;18:377–381. doi: 10.1093/carcin/18.2.377. [DOI] [PubMed] [Google Scholar]
- 22.Xu M, Orner GA, Bailey GS, Stoner GD, Horio DT, Dashwood RH. Post-initiation effects of chlorophyllin and indole-3-carbinol in rats given 1,2-dimethylhydrazine or 2-amino-3-methylimidazo[4, 5-f]quinoline. Carcinogenesis. 2001;22:309–314. doi: 10.1093/carcin/22.2.309. [DOI] [PubMed] [Google Scholar]
- 23.Yoshida M, Katashima S, Ando J, Tanaka T, Uematsu F, Nakae D, Maekawa A. Dietary indole-3-carbinol promotes endometrial adenocarcinoma development in rats initiated with N-ethyl-N’-nitro-N-nitrosoguanidine, with induction of cytochrome P450s in the liver and consequent modulation of estrogen metabolism. Carcinogenesis. 2004;25:2257–2264. doi: 10.1093/carcin/bgh225. [DOI] [PubMed] [Google Scholar]
- 24.Tilton SC, Hendricks JD, Orner GA, Pereira CB, Bailey GS, Williams DE. Gene expression analysis during tumor enhancement by the dietary phytochemical, 3, 3′-diindolylmethane, in rainbow trout. Carcinogenesis. 2007;28:1589–1598. doi: 10.1093/carcin/bgm017. [DOI] [PubMed] [Google Scholar]
- 25.Crowell JA, Page JG, Levine BS, Tomlinson MJ, Hebert CD. Indole-3-carbinol, but not its major digestive product 3, 3′-diindolylmethane, induces reversible hepatocyte hypertrophy and cytochromes P450. Toxicol Appl Pharmacol. 2006;211:115–123. doi: 10.1016/j.taap.2005.06.011. [DOI] [PubMed] [Google Scholar]
- 26.Grose KR, Bjeldanes LF. Oligomerization of indole-3-carbinol in aqueous acid. Chem Res Toxicol. 1992;5:188–193. doi: 10.1021/tx00026a007. [DOI] [PubMed] [Google Scholar]
- 27.Staub RE, Onisko B, Bjeldanes LF. Fate of 3, 3′-diindolylmethane in cultured MCF-7 human breast cancer cells. Chem Res Toxicol. 2006;19:436–442. doi: 10.1021/tx050325z. [DOI] [PubMed] [Google Scholar]
- 28.Anderton MJ, Manson MM, Verschoyle RD, et al. Pharmacokinetics and tissue disposition of indole-3-carbinol and its acid condensation products after oral administration to mice. Clin Cancer Res. 2004;10:5233–5241. doi: 10.1158/1078-0432.CCR-04-0163. [DOI] [PubMed] [Google Scholar]