

Abstract
The purpose of the present study was to describe the prevalence, patterns, and predictors of co-occurring modifiable cancer risk factors among African Americans seeking smoking cessation treatment, and to evaluate previously hypothesized models of the relationship between socioeconomic status and health behavior. Overweight/obesity, at-risk alcohol consumption, and insufficient physical activity were measured in 399 African American smokers. Analyses indicated that 92.8% of participants had at least one cancer risk factor in addition to smoking. Univariate ordinal logistic regression analyses revealed that female gender, unemployment, lower positive affect and greater negative affect were associated with having a greater number of cancer risk factors. Multivariate analyses yielded similar findings. A structural equation modeling approach indicated that stress/negative affect may function as one pathway linking socioeconomic status and modifiable cancer risk factors among African American smokers, and that gender has a direct effect on modifiable cancer risk factors. Thus, risk patterns identified within each gender group may guide the development of multiple risk factor interventions for African American smokers. Stress and negative affect may be an important treatment target within behavioral interventions for African American smokers of low socioeconomic status.
Keywords: Alcohol, Obesity, Physical Activity
Introduction
Lung cancer is the leading cause of cancer death in the United States, and the development of almost 90% of lung cancer cases is attributable to tobacco smoking.1 African Americans (AA) have the highest lung cancer incidence and mortality rates when compared to other racial/ethnic groups,2-4 despite reporting lower daily smoking rates and a later onset of smoking.3 Fernander et al.5 recently proposed a biopsychosocial model in which racial/ethnic differences in psychosocial factors, environmental variables, and the prevalence of modifiable risk factors are hypothesized to contribute to tobacco-related health disparities. Modifiable risk factors including poor nutrition/obesity, insufficient physical activity, and alcohol consumption have each been independently linked with cancer risk and/or mortality,6-8 and may confer additional risk in combination with smoking.9-10 While previous studies have indicated that smoking may be associated with having additional modifiable risk factors in primarily Caucasian samples,11-14 less is known about the patterns of modifiable cancer risk factors among AA smokers. Further, the influences of gender, socioeconomic status (SES), and psychosocial factors on the co-occurrence of modifiable risk factors in AAs remain to be explored. Information gained from studies of modifiable risk factors in AA smokers may be utilized to develop effective interventions aimed at attenuating cancer health disparities.
Preliminary evidence suggests that AA race/ethnicity may be associated with a higher prevalence of co-occurring modifiable risk factors. Specifically, two studies have indicated that AAs may have a greater number of risk factors than other racial/ethnic groups including Caucasians, Asians/Pacific Islanders, and Mexican Americans.15-16 Further, Murtaugh et al.17 reported that the majority of AA men and women who either smoked or were obese had at least one additional modifiable risk factor. However, the patterns and predictors of modifiable cancer risk factors remain to be identified among AAs who smoke and are at greater risk for the development of tobacco-related cancers and other diseases.
Gender is likely to influence the co-occurrence of certain modifiable cancer risk factors among AA smokers. Specifically, AA females have higher rates of obesity and insufficient physical activity (PA) than males,18-20 whereas hazardous drinking is more common among AA males.18 Thus, it is plausible that AA female smokers may have a greater number of co-occurring cancer risk factors when obesity, insufficient PA, and hazardous alcohol consumption are measured. It is notable that overweight/obesity and insufficient PA contribute to over four times as many deaths as alcohol consumption in the United States,21 suggesting that AA female smokers with co-occurring risk factors may be at high risk for serious health consequences.
Low SES is also associated with behavioral risk factors and negative health outcomes. Specifically, low SES has been linked with cancer development and mortality22-23 in addition to all-cause mortality.24 Low SES is associated with poorer perceived health and physical functioning,25-26 and low SES in childhood predicts the presence of modifiable risk factors in adulthood.27 Further, modifiable risk factors, including insufficient PA, hazardous alcohol consumption, tobacco use, and overweight/obesity, are more prevalent among adults of low SES.26,28 Notably, AA race/ethnicity and female gender are each associated with lower SES in the United States.29 Although SES is cross-sectionally and prospectively linked with health behaviors and outcomes, the pathways through which SES influences health behaviors and outcomes remain to be fully elucidated.
Researchers have hypothesized several pathways by which SES might influence disease development.30-31 Adler and Ostrove30 suggested that SES may influence health behavior and disease development through its influence on affect and cognition, the availability of environmental resources, exposure to carcinogens and pathogens, the physiological stress response, and the performance of health behaviors. In this model, one specific pathway between SES and health behaviors is through affect and cognition. Gallo and Matthews31 later hypothesized a similar pathway between SES and health behaviors that includes stress in addition to affect and cognition. In each of these models, low SES is associated with chronic stress and negative affect, which in turn negatively influence health behavior and increase the risk for disease.
There is some evidence that negative affect might function as one pathway between SES, health behaviors, and health outcomes. AAs and individuals of low SES report a greater number of stressful events than individuals who are Caucasian and/or of higher SES.32 Persistent economic hardship is associated with higher levels of depression,33 and lower SES is associated with depression among AAs specifically.34 Some research has indicated that negative affect may be associated with cancer risk, progression, and mortality due to stress-related dysregulation of Hypothalamic-Pituitary-Adrenal functioning and suppression of the immune system.35 Negative affect is also associated with behavioral factors that negatively influence cancer risk, such as non-adherence to medical recommendations,35 tobacco smoking,36-37 obesity,38 alcohol use disorders,39 and insufficient PA.40 Taken together, findings suggest that low SES may influence health behavior, at least in part, through its impact on negative affect and stress.
The purpose of present study was to identify the prevalence, patterns, and predictors of the co-occurrence of three modifiable cancer risk factors (i.e., overweight/obesity, insufficient PA, at-risk alcohol consumption) among treatment-seeking AA smokers, as these factors may contribute to disparities in the development of lung cancer and other tobacco-related diseases.5 In addition, demographic, socioeconomic, and psychosocial characteristics were examined as predictors of the co-occurrence of cancer risk factors. Finally, previously hypothesized models of the relationships among SES, affect, and the co-occurrence of modifiable cancer risk factors were evaluated.
Materials and Methods
Data for the current study were collected as part of a randomized clinical trial designed to determine the efficacy of a smoking cessation treatment that utilized palmtop computers and was targeted specifically at AA smokers. Participants were randomly assigned to either a standard smoking cessation treatment that included the nicotine patch, culturally sensitive self-help materials, and individual counseling, or the standard treatment in combination with treatment delivered via palmtop computer (Hewlett Packard iPAQ 1935 Pocket PC). All data used in the present study were collected prior to smoking cessation and treatment initiation.
Participants
Individuals were eligible to participate if they were AA, had been smoking five or more cigarettes per day for at least 12 months, had an expired carbon monoxide level of ≥ eight parts per million, planned to quit smoking within the next two weeks, possessed a functioning home telephone number, had a permanent home address, and were able to understand English at a sixth grade literacy level. Individuals were excluded from the study if they reported regular use of tobacco products other than cigarettes, were using pharmacological smoking cessation treatments other than the nicotine patches supplied by the study, reported that the nicotine patch was medically contraindicated, or were pregnant or lactating. Participant flow through the screening and enrollment process is depicted in Figure 1.
Figure 1.
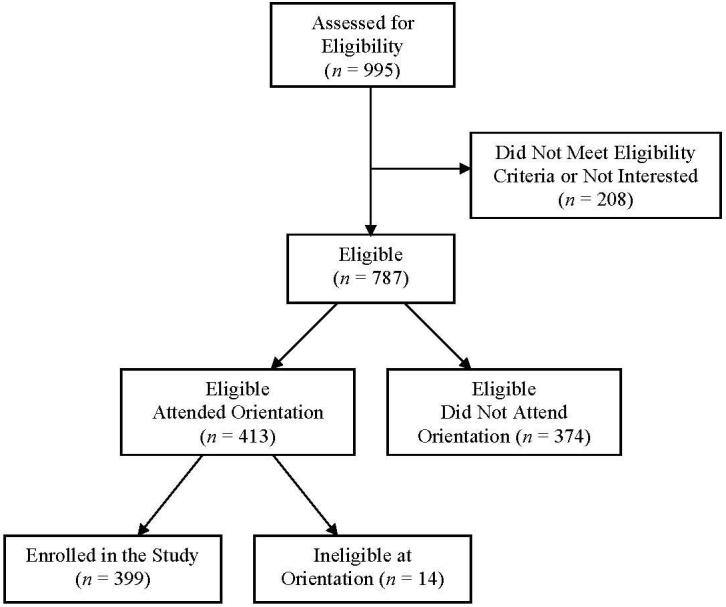
Flow of participants through screening and enrollment.
Measures
The Demographic Information Questionnaire is a self-report measure of demographic characteristics including age, gender, employment, education, and marital status.
The Tobacco History Questionnaire is a self-report measure of smoking characteristics, such as the number of years smoking and daily smoking rate. Participants who smoked < 20 cigarettes per day were considered light/moderate smokers and those who smoked ≥ 20 cigarettes per day were considered heavy smokers.
The Heaviness of Smoking Index (HSI) is a self-report measure that assesses level of nicotine dependence.41 The measure is calculated based on two items: 1) Self-reported cigarettes smoked per day, and 2) self-reported time until first cigarette of the day. Scores range from zero to six, with higher scores indicating greater dependence.
Overweight/Obesity Status was determined based on height and weight measurements, which were converted to body mass index (BMI; kg/m2). Participants with a BMI ≥ 25 were considered overweight/obese.
The International Physical Activity Questionnaire - Short Format (IPAQ) is a self-report questionnaire used to measure the amount of time spent in moderate activity, vigorous activity, and walking during the past seven days.42 Weekly minutes spent engaging in each type of activity were multiplied by the corresponding metabolic equivalent (MET) value, and MET minutes were summed to arrive at the total weekly MET minutes spent in PA. PA categories (low, moderate, high) were assigned based on total weekly MET minutes, the number of days per week engaged in PA, and the amount of time spent in each type of PA (see Guidelines for data processing and analysis of the IPAQ, 2005).43 Individuals were considered insufficiently active if they were categorized as having low activity during the previous week. The IPAQ short format has demonstrated good test-retest reliability (pooled Spearman reliability coefficient = .75), and reliability estimates have not been found to differ substantially whether the “last seven days” or the “usual week” were used as the reference period.42
The Patient Health Questionnaire (PHQ) - Alcohol Abuse/Dependence Scale is a self-report questionnaire used to indicate probable abuse or dependence on alcohol.44 The first item assesses current alcohol consumption, and any positive response on the subsequent items suggests probable alcohol abuse or dependence.
The Alcohol Quantity and Frequency Questionnaire is a self-report measure of average alcohol consumption on each day of the week over the last 30 days.45 Average daily alcohol consumption was summed to determine average weekly alcohol consumption. In addition, the measure assesses the number of binge drinking episodes (i.e., five or more drinks on one occasion) during the past three months.
At-Risk Drinking46 was confirmed if any of the following criteria were met: 1) participant was male and consumed an average of > 14 drinks per week, 2) participant was female and consumed an average of > seven drinks per week, 3) any individual who consumed ≥ five drinks on at least one occasion during the previous three months, or 4) any participant with probable alcohol abuse or dependence as indicated by the PHQ Alcohol Abuse/Dependence Scale.
The Total Number of Risk Factors was determined by summing the number of modifiable risk factors for which the specified criteria were met (i.e., overweight/obesity, insufficient physical activity, at-risk drinking in addition to smoking). Scores ranged from one to four risk factors. Participants who reported smoking as their sole risk factor were categorized as having one risk factor, while participants with all three risk factors in addition to smoking were categorized as having four risk factors.
The Patient Health Questionnaire (PHQ) - Major Depressive Disorder (MDD) is a self-report questionnaire used to indicate probable MDD.44 Responses on the questionnaire indicate a probable diagnosis of MDD when a participant 1) endorses little interest or pleasure in doing things on more than half the days during the past two weeks, and/or reports feeling down, depressed, or hopeless on more than half the days during the past two weeks, and 2) endorses five or more symptoms of MDD that were experienced on more than half the days during the past two weeks.
The Center for Epidemiological Studies Depression (CES-D) questionnaire was administered to measure depressive symptomatology.47 Scores of ≥ 16 indicate clinically significant distress.
The Positive and Negative Affect Schedule (PANAS) is a self-report measure on which participants rate the degree to which each of 20 adjectives reflects their mood during the past seven days.48 The measure utilizes a likert scale ranging from 1 (very slightly or not at all) to 5 (extremely), and is comprised of separate positive affect and negative affect subscales.
The Perceived Stress Scale - Short Version (PSS) is a self-rating scale of perceived stress level during the past week.49 Scores range from 0 to 16, with higher scores indicating higher perceived stress.
Procedure
The present study was approved by the Institutional Review Board of the University of Texas M. D. Anderson Cancer Center. Informed consent was obtained from all participants. All questionnaire and anthropometric data were collected prior to the quit date and treatment initiation of the larger smoking cessation study.
Analytic Plan
The present study focused on three modifiable disease risk factors (i.e., overweight/obesity, insufficient PA, and at-risk drinking) in addition to cigarette smoking. Each risk of the behavioral outcomes was dichotomized in order to reflect the cutpoint typically used to indicate when a behavior may warrant intervention (e.g., normal weight vs. overweight/obesity). This approach was believed to have greater clinical relevance, as individuals with clearly defined modifiable risk factors may be identified and targeted within treatment interventions. In addition, dichotomous outcomes allow for a description of the prevalence of each modifiable risk factor and may be summed to determine the prevalence of multiple risk factors.
Descriptive statistics were utilized to determine the prevalence of each risk factor, and to identify the frequencies of all combinations of risk factors. Ordinal logistic regression (OLR) analysis was utilized to identify characteristics that were associated with engaging in one, two, three, or all four of the measured cancer risk factors. OLR analysis was selected because of the ordered and categorical nature of the dependent variable.50 Demographic and socioeconomic variables including age, gender, education, employment status, marital status, and smoking level were tested as predictors of the total number of modifiable cancer risk factors, as were psychosocial variables including depression, perceived stress, negative affect, and positive affect. All predictor variables were tested for significance as univariate predictors of the total number of cancer risk factors, and each variable was additionally tested in separate multivariate models that included age, gender, education, employment status, marital status, and smoking level. All two-way interactions between predictor variables were subsequently tested. Finally, a structural equation model was tested using structural equation modeling software (Mplus Version 5.1).
Results
Participant Characteristics
A total of 399 AA smokers participated in the study, and 50.9% were female. Heavy smokers in the sample (58.8%) reported smoking an average of 27.23 (±11.70) cigarettes per day, while light/moderate smokers (41.2%) reported smoking an average of 11.05 (±3.22) cigarettes per day. Participants differed by gender on a variety of characteristics including weight status, PA, alcohol consumption, and the prevalence of probable MDD. See Table 1 for participant characteristics overall and by gender.
Table 1.
Participant characteristics overall and by gender group
| Males (n = 196) | Females (n = 203) | Total Sample (N = 399) | p | |
|---|---|---|---|---|
| Demographic Characteristics | ||||
| Age, years | 42.8 (±9.3) | 42.0 (±10.2) | 42.4 (±9.7) | .40a |
| ≤ High School Education (%) | 56.1 | 47.5 | 51.8 | .09b |
| Unemployment (%) | 60.4 | 60.3 | 60.4 | .98b |
| Single Marital Status (%) | 80.3 | 76.5 | 78.4 | .36b |
| Cigarette Smoking | ||||
| Years of Smoking | 22.5 (±10.6) | 20.6 (±10.9) | 21.5 (±10.8) | .08a |
| Cigarettes per Day | 21.3 (±13.5) | 19.8 (±10.7) | 20.6 (±12.2) | .22a |
| Heavy Smoking (%) | 60.7 | 56.9 | 58.8 | .44b |
| Heaviness of Smoking Index | 3.6 (±1.4) | 3.5 (±1.4) | 3.5 (±1.4) | .70a |
| Weight Status | ||||
| Body Mass Index | 27.5 (±6.0) | 31.2 (±8.0) | 29.4 (±7.3) | <.01a |
| Overweight/Obese (%) | 60.7 | 77.3 | 69.2 | <.01b |
| Physical Activity | ||||
| IPAQ Low Physical Activity (%) | 23.8 | 39.4 | 31.6 | <.01b |
| Alcohol Consumption | ||||
| Drinks per Week | 12.8 (±23.4) | 6.8 (±15.6) | 9.7 (±20.0) | <.01a |
| Binge Drinking Episodes (past 3 mos.) | 3.1 (±7.0) | 1.7 (±3.8) | 2.4 (±5.7) | .02a |
| PHQ Alcohol Abuse/Dependence (%) | 34.7 | 19.3 | 26.8 | <.01b |
| At-Risk Drinking (%) | 60.8 | 43.2 | 51.8 | <.01b |
| Negative/Positive Affect | ||||
| PHQ Major Depressive Disorder (%) | 14.4 | 22.8 | 18.6 | <.03b |
| CES-D | 16.3 (±11.2) | 17.3 (±12.2) | 16.8 (±11.7) | .41a |
| Perceived strees Scale | 6.3 (±3.1) | 6.4 (±3.1) | 6.3 (±3.1) | .79a |
| PANAS Negative Affect | 19.8 (±8.4) | 20.8 (±9.2) | 20.3 (±8.8) | .29a |
| PANAS Positive Affect | 33.1 (±8.3) | 32.2 (±9.0) | 32.6 (±8.7) | .25a |
Note: Means and standard deviations are presented unless specified. Bolded outcomes indicate p-values < .05. IPAQ = International Physical Activity Questionnaire, PHQ = Patient Health Questionnaire, CES-D = Center for Epidemiological
p-value based on ANOVA test for differences between gender groups.
p-value based on Chi-square test for differences between gender groups.
Risk Factor Prevalence
The mean number of modifiable cancer risk factors, including smoking, reported by participants was 2.51 (±.73). The total number of risk factors differed significantly by gender, F(1, 361) = 5.51, p = .02, such that females had more risk factors than males (2.60 vs. 2.42). Only 7.2% of participants reported smoking as their sole risk factor, while 6.9% reported all four risk factors. The distribution of the total number of risk factors differed significantly by gender, χ2(3) = 8.98, p = .03. Males were more likely than females to have only one risk factor, while females were more likely than males to have all four risk factors. See Figure 2 for the distribution of risk factors for the entire sample and by gender. The most prevalent combinations of risk factors among all participants were smoking and overweight/obesity (24.2%); smoking, overweight/obesity, and at-risk drinking (24.2%); smoking, overweight/obesity, and insufficient PA (13.8%); and smoking and at-risk drinking (13.5%). Smoking, overweight/obesity, and at-risk drinking was the most prevalent combination of behavioral risk factors among males (27.5%), while smoking and overweight/obesity was the most prevalent combination among females (27.6%).
Figure 2.

prevalence of having one to four modifiable cancer risk factors overall and by gender.
Univariate Analyses
Univariate OLR analysis revealed that gender was a significant predictor of the total number of modifiable cancer risk factors, χ2(1) = 4.04, p = .04. Specifically, male gender was associated with having fewer risk factors relative to females (see Table 2). Employment status was also significantly associated with the total number of cancer risk factors, χ2(1) = 4.39, p = .04, such that individuals who were unemployed had a greater number of risk factors relative to individuals who were employed. All measures of negative affect including the PHQ MDD, χ2(1) = 6.89, p < .01; CES-D, χ2(1) = 8.14, p < .01; PSS, χ2(1) = 10.56, p < .01; and PANAS negative affect, χ2(1) = 8.91, p < .01, were significantly associated with the total number of cancer risk factors, such that greater negative affect was associated with having a greater number of risk factors. Conversely, greater positive affect on the PANAS positive affect scale was associated with having fewer risk factors, χ2(1) = 8.69, p < .01. Smoking level approached significance as a univariate predictor variable, χ2(1) = 3.40, p = .07, such that light to moderate smokers (< 20 cigarettes per day) had a greater number of risk factors relative to heavier smokers (≥ 20 cigarettes per day). Age, education, and marital status were not significantly associated with the total number of risk factors in the univariate analyses.
Table 2.
Univariate and multivariate of the total number of modifiable cancer risk factors (1-4)
| Univariate | Multivariate* | |||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p | Odds Ratio (95% CI) | p | |
| Age | .98 (.97, 100) | .13 | .99 (.97, 101) | .17 |
| Gender | ||||
| Male | .67 (.45, .99) | .04 | .66 (.44, 98) | .04 |
| Female | 1.00 | - | 1.00 | - |
| Education | ||||
| ≤ High School | 1.31 (.88, 1.93) | .18 | 1.29 (.85, 1.95) | .23 |
| > High School | 1.00 | - | 1.00 | - |
| Employment Status | ||||
| Unemployed, Retired, Disabled | 1.53 (1.03, 2.30) | .04 | 1.46 (.96, 2.21) | .08 |
| Employed Full or Part-Time | 1.00 | 1.00 | ||
| Marital Status | ||||
| Single, Divorced, Seperated, Widowed | 1.24 (.77, 1.99) | .38 | 1.22 (.75, 1.98) | .42 |
| Married, Living with Sig. Other | 1.00 | - | 1.00 | - |
| Smoking Level | ||||
| Light/Moderate (< 20/day) | 1.46 (.98, 2.17) | .07 | 1.45 (.96, 2.18) | .08 |
| Heavy (≥ 20/day) | 1.00 | - | 1.00 | - |
| PHQ Depression | ||||
| Probable Major Depression | 1.96 (1.18, 3.25) | <.01 | 1.87 (1.10, 3.17) | .02 |
| Non-depressed | 1.00 | - | 1.00 | - |
| CES-D | 1.03 (1.01, 1.04) | <.01 | 1.03 (1.01, 1.05) | <.01 |
| Perceived Stress Scale | 1.11 (1.04, 1.19) | <.01 | 1.11 (1.04, 1.19) | <.01 |
| PANAS Negative Affect | 1.04 (1.01, 1.06) | <.01 | 1.04 (1.01, 1.06) | <.01 |
| PANAS Positive Affect | .97 (.94, .99) | <.01 | .97 (.94, .99) | <.01 |
Note: Bolded outcomes indicate p-values < .05. CI = Confidence Interval, PHQ = Patient Health Questionnaire, CES-D = Center for Epidemiological Studies-Depression, PANAS = Positive and Negative Affect Schedule
Age, gender, education, employment, matial status, and smoking level included in the model.
Multivariate Analyses
Multivariate models were tested with age, gender, education, employment status, marital status, and smoking level included in all analyses. Results indicated that gender remained a significant predictor of the total number of modifiable cancer risk factors, χ2(1) = 4.24, p = .04, such that male gender was associated with having fewer risk factors relative to individuals of female gender (see Table 2). All measures of negative affect including PHQ MDD, χ2(1) = 5.48, p = .02; CES-D, χ2(1) = 7.18, p < .01; PSS, χ2(1) = 8.95, p < .01; and PANAS negative affect, χ2(1) = 8.60, p < .01, remained significantly associated with the total number of risk factors, such that greater negative affect was associated with having more risk factors. Conversely, greater positive affect, as measured by the PANAS positive affect scale, was associated with having fewer risk factors, χ2(1) = 6.97, p < .01. Employment status approached significance as a predictor variable, χ2(1) = 3.13, p = .08, such that individuals who were unemployed had a greater number of risk factors than employed participants. Smoking level also approached significance as a predictor variable, χ2(1) = 3.18, p = .07, such that light to moderate smokers (< 20 cigarettes per day) had a greater number of risk factors relative to individuals who were heavy smokers (≥ 20 cigarettes per day). Age, education, and marital status were not significantly associated with the total number of cancer risk factors in the multivariate analyses. All two-way interactions were tested. However, few interactions were significant and no clear patterns among the significant interactions were observed. Therefore, these data will not be presented.
Structural Equation Modeling
A structural equation model was developed and tested in order to gain a better understanding of the interrelationships among key variables theorized to influence the likelihood of having co-occurring modifiable cancer risk factors. The first step in the process was to include all five variables related to affect (i.e., CES-D, PHQ MDD, PSS, PANAS negative affect, PANAS positive affect) as indicators of a latent construct. PANAS positive affect was ultimately removed from the model because it differed conceptually from the other indicators, and removing this indicator produced a model that was a better fit for the data. Multiple measures of negative and depressive affect were included a part of the latent variable in order to reduce the influence of measurement error, thus providing a stronger index of negative affect.51 Although all variables which comprise the negative affect latent variable are correlated, the magnitudes of the correlations do not suggest collinearity (i.e., ≥ .85).51-52 CES-D scores were significantly correlated with PANAS negative affect, r = .83, p = <.001, PSS, r = .71, p = <.001, and PHQ MDD scores, r = .55, p = <.001. PANAS negative affect scores were significantly correlated with scores on the PSS, r = .69, p = <.001, and PHQ MDD, r = .48, p = <.001, and PSS scores were significantly correlated with PHQ MDD scores, r = .44, p = <.001.
An initial model was developed in which gender, employment status, education, negative affect, positive affect, and the total number of risk factors were included. These particular variables were included in the model because they were either indicators of SES or significant predictors of the total number of cancer risk factors in the OLR analyses. Positive affect was subsequently removed because it was not significantly related to the total number of risk factors in the model. A pathway between gender and negative affect was initially included, but was ultimately removed because it was not significant. The inclusion of age, marital status, and smoking level did not improve the fit of the initial model; therefore these variables were not included in the final model. Variables included in the final model were gender, employment status, education, negative affect (latent variable), and the total number of cancer risk factors. PHQ MDD, an indicator of negative affect, was treated as a nominal variable, and the total number of risk factors was treated as an ordered categorical variable in the analyses, while all remaining variables were treated as continuous.
Maximum likelihood estimation for the final model yielded the following model fit values: χ2(17) = 38.445, p = .002; Root mean square error of approximation (RMSEA) = .056 (90% confidence interval: .033, .08); Comparative fit index (CFI) = .977; Tucker-Lewis index (TLI) = .966; and Standardized Root Mean Square Residual (SRMR) = .033. Overall, the model is a good fit for the data based on currently accepted model fit guidelines.51, 53 All paths in the final model are statistically significant at p < .001, with the exception of the path between gender and the total number of risk factors, p = .026. The standardized indirect effect of employment on the total number of cancer risk factors was -.037, p = .009, and the standardized indirect effect of education on the total number of cancer risk factors was -.046, p = .004. The final model including the standardized estimates of path coefficients is depicted in Figure 3.
Figure 3.

Model of the relationships among gender, socioeconomic status indicators, negative affect, and the total number of modifiable cancer risk factors. Note: PSS = perceived Stress Scale, NA = Negative Affect as measured by the positive and Negative Affect Schedule, CES-D = Center for Epidemiological Studies - Depression, MDD = Probable Major Depressive Disorder as measured by the patient Health Questionnaire.
Discussion
The present study generated several major findings. First, co-occurring modifiable cancer risk factors, especially overweight/obesity and at-risk drinking, are common among AAs seeking smoking cessation treatment. Only 7.2% of AA participants in the current study reported smoking as their sole risk factor, while 92.8% of the participants reported at least one modifiable cancer risk factor in addition to smoking. Second, AA females had a greater number of risk factors and exhibited different patterns of co-occurring risk factors than AA males. Third, greater negative affect was associated with having a greater number of risk factors, while positive affect was associated with having fewer risk factors. Finally, the findings of this study suggest that negative affect functions as one pathway linking SES and modifiable cancer risk factors among treatment-seeking AA smokers, which is consistent with current conceptual models.30-31
The results of this study indicate that those who are unemployed and/or have less education experience greater negative affect, which is in turn associated with having a greater number of modifiable cancer risk factors. Low SES is often associated with limited access to resources in combination with a greater frequency and severity of stressors, which consequently leads to higher levels of negative affect.32-34 Unfortunately, negative affect is associated with a variety of behaviors that are known to negatively influence health.35-40 This study provides support for the role of negative affect as described in the models developed by Adler and Ostrov30 and Gallo and Matthews,31 and contributes to an explanation of current health disparities among AAs and individuals of low SES. Few studies have focused on identifying the patterns of modifiable risk behaviors among AA smokers or the pathways linking SES and health behavior. Thus, the present study contributes to our understanding of potential influences on co-occurring modifiable cancer risk factors in AA smokers.
The patterns and prevalence of co-occurring cancer risk factors differed by gender. As expected, AA females had the highest rates of overweight/obesity and insufficient PA, while males had the highest rates of at-risk drinking. Additionally, a higher proportion of females than males had four concurrent cancer risk factors, while a greater number of males than females endorsed smoking as their sole risk factor. The most frequent combination of risk factors among females was smoking and overweight/obesity, while males were most likely to report concurrent smoking, overweight/obesity, and at-risk drinking. Although findings indicate that gender groups vary in the prevalence of cancer risk factors, overweight/obesity, at-risk drinking, and insufficient PA were common risk factors among smokers of each gender group.
Other predictors of the total number of cancer risk factors included employment status, negative affect, and positive affect. Age, education, marital status, and smoking level were not significant predictors. Although unemployment was associated with having a greater number of co-occurring risk factors in the univariate analyses, this relationship only approached significance in the multivariate analyses. Negative affect, measured in a variety of ways, was associated with having a greater number of co-occurring cancer risk factors, while positive affect was associated with having fewer risk factors in both the univariate and multivariate analyses.
Several strengths and limitations of the findings should be noted. The entirely AA sample provided an opportunity to obtain valuable information about the health behaviors of treatment-seeking AA smokers. However, the proposed model of SES and health behavior included only one pathway (i.e., negative affect) by which these variables were connected. Future research should focus on developing more comprehensive models that take into consideration other factors which are known to influence health behavior and disease risk, such as the neighborhood environment, access to health care, and biological variables. In addition, AA smokers who participated in the current study tended to be heavy smokers of low SES, and all were seeking smoking cessation treatment. As a result, they may differ from both the general population of AAs, as well as the AA population, with respect to the prevalence and type of modifiable risk factors. Compared with findings from nationally representative samples of AA smokers, AA smokers in the present study were more likely to be female, heavy smokers, unemployed, and of single marital status.54-55 Nevertheless, recent research has indicated that the characteristics of smokers who participate in smoking cessation treatment trials do not differ in a clinically meaningful way from the characteristics of smokers who do not participate.56 Another possible limitation is that participants may have underestimated their alcohol consumption due to poor recall or social desirability, although research indicates that self-reports of alcohol consumption are generally accurate.45 Finally, recent evidence suggests that the IPAQ may overestimate PA levels.57 It is also possible that self-reported physical activity levels during the past seven days did not accurately reflect the typical physical activity levels of some participants. Therefore, findings related to PA in the present study should be interpreted cautiously until they are replicated with additional PA measures.
The results of the current study highlight the role of education, employment, and negative affect in the co-occurrence of risk factors, and illustrate the need for interventions at multiple levels that target co-occurring cancer risk factors in AA smokers. For example, broad policy changes that impact employment and education could have downstream effects on cancer risk behaviors. Programs that increase the quality and quantity of education, as well as programs that reduce unemployment (e.g., job training) among individuals of low SES may increase access to higher paying employment of greater quality. This, in turn, may influence many other aspects of individuals’ lives (e.g., ability to afford residence in a safe neighborhood). Community-level interventions may influence health behavior by reducing or eliminating alcohol and tobacco advertising and increasing neighborhood walkability. The model tested in the current study suggests that one pathway through which these programs might influence cancer risk factors is their influence on reducing negative affect. Thus, individual-level interventions might target negative affect directly in order to facilitate change in cancer risk behaviors. Numerous other strategies for improving health that address poverty, education and job training, the availability of public transportation and housing, and the affordability and accessibility of healthy foods have been discussed in detail elsewhere.58
The findings also suggest that multiple risk factor interventions may be warranted among individuals who are seeking smoking cessation treatment. AA women, in particular, may benefit from smoking cessation interventions that address overweight/obesity and insufficient PA, whereas AA men may benefit from additional treatment that specifically targets at-risk drinking. The findings of the present study suggest that it may be beneficial to include adjunctive treatments for depression and negative affect, as well as coping skills training within existing smoking cessation interventions for those who are experiencing chronic stress related to low SES. The attenuation of negative affect may particularly important for individuals of low SES with multiple modifiable risk factors.
Addressing multiple risk factors in smoking cessation treatment is important because alcohol consumption, PA, and body weight may influence smoking cessation outcomes. Alcohol consumption has been associated with relapse following smoking cessation,59 and there is evidence that increased PA is linked with successful smoking cessation.60 Further, postcessation weight gain may lead to the development of overweight/obesity or exacerbate existing obesity-related health conditions. This is of particular concern given that AAs are at greater risk of excessive postcessation weight gain.61 Interventions addressing multiple cancer risk factors may improve smoking cessation rates and minimize the health consequences associated with alcohol use and postcessation changes in energy balance. Ultimately, it is hoped that multiple behavior change interventions will help to reduce the prevalence of cancer risk factors, and contribute to the elimination of cancer and other health disparities among AAs.
Acknowledgements
This research was supported by grants R01-CA094826 and R25T-CA57730 awarded by the National Cancer Institute, and grant K01-DP001120 awarded by the Centers for Disease Control and Prevention.
References
- 1.Levitz JS, Bradley TP, Golden AL. Overview of smoking and all cancers. Med Clin North Am. 2004 Nov;88(6):1655–75. doi: 10.1016/j.mcna.2004.07.005. [DOI] [PubMed] [Google Scholar]
- 2.Berger M, Lund MJ, Brawley OW. Racial disparities in lung cancer. Curr Probl Cancer. 2007 May-Jun;31(3):202–10. doi: 10.1016/j.currproblcancer.2007.02.002. [DOI] [PubMed] [Google Scholar]
- 3.Fagan P, Moolchan ET, Lawrence D, Fernander A, Ponder PK. Identifying health disparities across the tobacco continuum. Addiction. 2007 Oct;102(Suppl 2):5–29. doi: 10.1111/j.1360-0443.2007.01952.x. [DOI] [PubMed] [Google Scholar]
- 4.Flenaugh EL, Henriques-Forsythe MN. Lung cancer disparities in African Americans: health versus health care. Clin Chest Med. 2006 Sep;27(3):431–9. doi: 10.1016/j.ccm.2006.04.006. [DOI] [PubMed] [Google Scholar]
- 5.Fernander AF, Shavers VL, Hammons GJ. A biopsychosocial approach to examining tobacco-related health disparities among racially classified social groups. Addiction. 2007 Oct;102(Suppl 2):43–57. doi: 10.1111/j.1360-0443.2007.01954.x. [DOI] [PubMed] [Google Scholar]
- 6.Calle EE, Rodriguez C, Walker-Thurmond K, Thun MJ. Overweight, obesity, and mortality from cancer in a prospectively studied cohort of U.S. adults. N Engl J Med. 2003 Apr 24;348(17):1625–38. doi: 10.1056/NEJMoa021423. [DOI] [PubMed] [Google Scholar]
- 7.Lee I. Physical activity and cancer prevention - Data from epidemiologic studies. Med Sci Sports Exerc. 2003 Nov;35(11):1823–7. doi: 10.1249/01.MSS.0000093620.27893.23. [DOI] [PubMed] [Google Scholar]
- 8.Poschl G, Seitz HK. Alcohol and cancer. Alcohol Alcohol. 2004 May-Jun;39(3):155–65. doi: 10.1093/alcalc/agh057. [DOI] [PubMed] [Google Scholar]
- 9.Blot WJ, McLaughlin JK, Winn DM, et al. Smoking and drinking in relation to oral and pharyngeal cancer. Cancer Res. 1988 Jun 1;48(11):3282–7. [PubMed] [Google Scholar]
- 10.Marrero JA, Fontana RJ, Fu S, Conjeevaram HS, Su GL, Lok AS. Alcohol, tobacco, and obesity are synergistic risk factors for hepatocellular carcinoma. J Hepatol. 2005 Feb;42(2):218–24. doi: 10.1016/j.jhep.2004.10.005. [DOI] [PubMed] [Google Scholar]
- 11.Burke V, Milligan RAK, Beilin LJ, et al. Clustering of health-related behaviors among 18-year-old Australians. Prev Med. 1997 Sep-Oct;26(5 Pt 1):724–33. doi: 10.1006/pmed.1997.0198. [DOI] [PubMed] [Google Scholar]
- 12.Chiolero A, Wietlisbach V, Ruffieux C, Paccaud F, Cornuz J. Clustering of risk behaviors with cigarette consumption: a population-based survey. Prev Med. 2006 May;42(5):348–53. doi: 10.1016/j.ypmed.2006.01.011. [DOI] [PubMed] [Google Scholar]
- 13.Emmons KM, Marcus BH, Linnan L, Rossi JS, Abrams DB. Mechanisms in multiple risk factor interventions: smoking, physical activity, and dietary fat, intake among manufacturing workers. Prev Med. 1994 Jul;23(4):481–9. doi: 10.1006/pmed.1994.1066. [DOI] [PubMed] [Google Scholar]
- 14.Laaksonen M, Luoto R, Helakorpi S, Uutela A. Associations between health-related behaviors: A 7-year follow-up of adults. Prev Med. 2002 Feb;34(2):162–70. doi: 10.1006/pmed.2001.0965. [DOI] [PubMed] [Google Scholar]
- 15.Hahn RA, Teutsch SM, Franks AL, Chang M, Lloyd EE. The prevalence of risk factors among women in the United States by race and age, 1992-1994: opportunities for primary and secondary prevention. J Am Med Womens Assoc. 1998;53(2):96–107. [PubMed] [Google Scholar]
- 16.Sharma S, Malarcher AM, Giles WH, Myers G. Racial, ethnic and socioeconomic disparities in the clustering of cardiovascular disease risk factors. Ethn Dis. 2004;14(1):43–8. [PubMed] [Google Scholar]
- 17.Murtaugh KH, Borde-Perry WC, Campbell KL, Gidding SS, Falkner B. Obesity, smoking, and multiple cardiovascular disease risk factors in young adult African Americans. Ethn Dis. 2002;12(3):331–5. [PubMed] [Google Scholar]
- 18.Seale JP, Davis-Smith M, Okosun I. Ethnic and gender differences in lifestyle risk factors in a bi-ethnic primary care sample: prevalence and clinical implications. Ethn Dis. 2006;16(2):460–7. [PubMed] [Google Scholar]
- 19.Wang Y, Beydoun MA. The obesity epidemic in the United States - gender, age, socioeconomic, racial/ethnic, and geographic characteristics: a systematic review and meta-regression analysis. Epidemiol Rev. 2007;29:6–28. doi: 10.1093/epirev/mxm007. [DOI] [PubMed] [Google Scholar]
- 20.Whitt-Glover MC, Taylor WC, Heath GW, Macera CA. Self-reported physical activity among blacks: estimates from national surveys. Am J Prev Med. 2007 Nov;33(5):412–417. doi: 10.1016/j.amepre.2007.07.024. [DOI] [PubMed] [Google Scholar]
- 21.Mokdad AH, Marks JS, Stroup DF, Gerberding JL. Actual causes of death in the United States, 2000. JAMA. 2004 Mar 10;291(10):1238–45. doi: 10.1001/jama.291.10.1238. [DOI] [PubMed] [Google Scholar]
- 22.Chu KC, Miller BA, Springfield SA. Measures of racial/ethnic health disparities in cancer mortality rates and the influence of socioeconomic status. J Natl Med Assoc. 2007 Oct;99(10):1092–100. [PMC free article] [PubMed] [Google Scholar]
- 23.Ekberg-Aronsson M, Nilsson PM, Nilsson J, Pehrsson K, Lofdahl C. Socio-economic status and lung cancer risk including histologic subtyping - a longitudinal study. Lung Cancer. 2006 Jan;51(1):21–9. doi: 10.1016/j.lungcan.2005.08.014. [DOI] [PubMed] [Google Scholar]
- 24.Lantz PM, House JS, Lepkowski JM, Williams DR, Mero RP, Chen JC. Socioeconomic factors, health behaviors, and mortality. JAMA. 1998 Jun 3;279(21):1703–8. doi: 10.1001/jama.279.21.1703. [DOI] [PubMed] [Google Scholar]
- 25.Ross CE, Mirowsky J. Does employment affect health? J Health Soc Behav. 1995 Sep;36:230–243. [PubMed] [Google Scholar]
- 26.Ross CE, Mirowsky J. Refining the association between education and health: The effects of quantity, credential, and selectivity. Demography. 1999 Nov;36(4):445–60. [PubMed] [Google Scholar]
- 27.Melchior M, Moffitt TE, Milne BJ, Poulton R, Caspi A. Why do children from socioeconomically disadvantaged families suffer from poor health when they reach adulthood? A life-course study. Am J Epidemiol. 2007 Oct 15;166(8):966–74. doi: 10.1093/aje/kwm155. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Lynch JW, Kaplan GA, Salonen JT. Why do poor people behave poorly? Variation in adult health behaviors and psychosocial characteristics by stages of the socioeconomic life course. Soc Sci Med. 1997 Mar;44(6):809–19. doi: 10.1016/s0277-9536(96)00191-8. [DOI] [PubMed] [Google Scholar]
- 29.U.S. Census Bureau . Income, Poverty, and Health Insurance Coverage in the United States: 2006 (P60-233) U.S. Government Printing Office; Washington, DC: 2007. [Google Scholar]
- 30.Adler NA, Ostrove JM. Socioeconomic status and health: what we know and what we don’t. Ann N Y Acad Sci. 1999;986:3–15. doi: 10.1111/j.1749-6632.1999.tb08101.x. [DOI] [PubMed] [Google Scholar]
- 31.Gallo LC, Matthews KA. Understanding the association between socioeconomic status and physical health: do negative emotions play a role? Psychol Bull. 2003 Jan;129(1):10–51. doi: 10.1037/0033-2909.129.1.10. [DOI] [PubMed] [Google Scholar]
- 32.Hatch SL, Dohrenwend BP. Distribution of traumatic and other stressful life events by race/ethnicity, gender, SES, and age: a review of the research. Am J Community Psychol. 2007 Dec;40(34):313–32. doi: 10.1007/s10464-007-9134-z. [DOI] [PubMed] [Google Scholar]
- 33.Mirowsky J, Ross CE. Age and the effect of economic hardship on depression. J Health Soc Behav. 2001 Jun;42(2):132–50. [PubMed] [Google Scholar]
- 34.Lincoln KD, Chatters LM, Taylor RJ, Jackson JS. Profiles of depressive symptoms among African Americans and Carribbean Blacks. Soc Sci Med. 2007 Jul;65(2):200–13. doi: 10.1016/j.socscimed.2007.02.038. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Speigel D, Giese-Davis J. Depression and cancer: mechanisms and disease progression. Biol Psychiatry. 2003 Aug 1;54(3):269–82. doi: 10.1016/s0006-3223(03)00566-3. [DOI] [PubMed] [Google Scholar]
- 36.Glassman AH, Helzer JE, Covey LS, et al. Smoking, smoking cessation, and major depression. JAMA. 1990 Sep 26;264(12):1546–49. [PubMed] [Google Scholar]
- 37.Paperwalla KN, Levin TT, Weiner J, Saravay SM. Smoking and depression. Med Clin North Am. 2004 Nov;88(6):1483–94. doi: 10.1016/j.mcna.2004.06.007. [DOI] [PubMed] [Google Scholar]
- 38.Simon GE, Von Korff M, Saunders K, et al. Association between obesity and psychiatric disorders in the US adult population. Arch Gen Psychiatry. 2006 Jul;63(7):824–30. doi: 10.1001/archpsyc.63.7.824. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 39.Hasin DS, Goodwin RD, Stinson FS, Grant BF. Epidemiology of major depressive disorder. Arch Gen Psychiatry. 2005 Oct;62(10):1097–106. doi: 10.1001/archpsyc.62.10.1097. [DOI] [PubMed] [Google Scholar]
- 40.Goodwin RD. Association between physical activity and mental disorders among adults in the United States. Prev Med. 2003 Jun;36(6):698–703. doi: 10.1016/s0091-7435(03)00042-2. [DOI] [PubMed] [Google Scholar]
- 41.Heatherton TF, Kozlowski LT, Frecker RC, Rickert W, Robinson J. Measuring the heaviness of smoking: using self-reported time to first cigarette of the day and number of cigarettes smoked per day. Br J Addict. 1989 Jul;84(7):791–799. doi: 10.1111/j.1360-0443.1989.tb03059.x. [DOI] [PubMed] [Google Scholar]
- 42.Craig CL, Marshall AL, Sjostrom M, et al. International Physical Activity Questionnaire: 12-country reliability and validity. Med Sci Sports Exerc. 2003 Aug;35(8):1381–95. doi: 10.1249/01.MSS.0000078924.61453.FB. [DOI] [PubMed] [Google Scholar]
- 43. [cited 2008 Feb 18];Guidelines for data processing and analysis of the International Physical Activity Questionnaire (IPAQ) 2005 November; Available from: http://www.ipaq.ki.se/ipaq.htm.
- 44.Spitzer RL, Kroenke K, Williams JBW. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. JAMA. 1999 Nov 10;282(18):1737–44. doi: 10.1001/jama.282.18.1737. [DOI] [PubMed] [Google Scholar]
- 45.Sobell LC, Sobell MB. Alcohol consumption measures. In: Allen JP, Wilson VB, editors. Assessing alcohol problems: A guide for clinicians and researchers. 2nd ed. U.S. Department of Health and Human Services, National Institute on Alcohol Abuse and Alcoholism; Bethesda: 2003. pp. 75–99. NIH Publication No. 03-3745. [Google Scholar]
- 46.U.S. Department of Health and Human Services (USDHHS) Helping patients who drink too much: A clinician’s guide. May, 2007. NIH Publication No. 07-3769. [Google Scholar]
- 47.Radloff LS. The CES-D Scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1(3):385–401. [Google Scholar]
- 48.Watson D, Clark LA, Tellegan A. Development and validation of brief measures of positive and negative affect: the PANAS scales. Journal Pers Soc Psychol. 1988;54:1063–70. doi: 10.1037//0022-3514.54.6.1063. [DOI] [PubMed] [Google Scholar]
- 49.Cohen S, Kamarck T, Mermelstein R. A global measure of perceived stress. J Health Soc Behav. 1983 Dec;24:385–396. [PubMed] [Google Scholar]
- 50.Scott SC, Goldberg MS, Mayo NE. Statistical assessment of ordinal outcomes in comparative studies. J Clin Epidemiol. 1997 Jan;50(1):45–55. doi: 10.1016/s0895-4356(96)00312-5. [DOI] [PubMed] [Google Scholar]
- 51.Kline RB. Principles and practice of structural equation modeling. The Guilford Press; New York: 2005. [Google Scholar]
- 52.Brown TA. Confirmatory Factor Analysis. The Guilford Press; New York: 2006. [Google Scholar]
- 53.Hu L, Bentler PM. Cutoff criteria for fit indexes in covariance structure analysis: conventional criteria versus new alternatives. Struct Equation Model. 1999;6(1):1–55. [Google Scholar]
- 54.Carabello RS, Giovino GA, Pechacek TF, et al. Racial and ethnic differences in serum cotinine levels of cigarette smokers. JAMA. 1998 Jul;280(2):135–139. doi: 10.1001/jama.280.2.135. [DOI] [PubMed] [Google Scholar]
- 55.Novotny TE, Warner KE, Kendrick JS, Remington PL. Smoking by blacks and whites: socioeconomic and demographic differences. Am J Public Health. 1988 Sep;78(9):1187–1189. doi: 10.2105/ajph.78.9.1187. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 56.Graham AL, Papandonatos GD, DePue JD, et al. Lifetime characteristics of participants and non-participants in a smoking cessation trial: implications for external validity and public health impact. Ann Behav Med. doi: 10.1007/s12160-008-9031-1. in press. [DOI] [PubMed] [Google Scholar]
- 57.Fogelholm M, Malmberg J, Suni J, et al. International Physical Activity Questionnaire: Validity against fitness. Med Sci Sports Exerc. 2006 Apr;38(4):753–60. doi: 10.1249/01.mss.0000194075.16960.20. [DOI] [PubMed] [Google Scholar]
- 58.Tarlov AR. Public policy frameworks for improving population health. Ann N Y Acad Sci. 1999;896:281–93. doi: 10.1111/j.1749-6632.1999.tb08123.x. [DOI] [PubMed] [Google Scholar]
- 59.McClure JB, Wetter DW, de Moor C, Cinciripini PM, Gritz ER. The relation between alcohol consumption and smoking abstinence: Results from the Working Well Trial. Addict Behav. 2002 May-Jun;27(3):367–79. doi: 10.1016/s0306-4603(01)00177-0. [DOI] [PubMed] [Google Scholar]
- 60.Nagaya T, Yoshida H, Takahashi H, Kawai M. Cigarette smoking weakens exercise habits in healthy men. Nicotine Tob Res. 2007 Oct;9(10):1027–32. doi: 10.1080/14622200701591575. [DOI] [PubMed] [Google Scholar]
- 61.Filozof C, Fernandez Pinilla MC, Fernandez-Cruz A. Smoking cessation and weight gain. Obes Rev. 2004 May;5(2):95–103. doi: 10.1111/j.1467-789X.2004.00131.x. [DOI] [PubMed] [Google Scholar]