

Abstract
Purpose:
This health communication project measured the psychosocial influences of computer anxiety, computer confidence, and computer self-efficacy in older adults at six meal congregate sites. The adults completed a five-week education intervention, based on Bandura's self-efficacy model, designed to assist older adults in retrieving and evaluating health information resources on the Internet.
Methods:
One hundred thirty-seven participants, ages sixty-five and older, were randomized in a controlled, two-group, pre–post, repeated measures design. Participants in the intervention group received a two-hour training session, once a week for five weeks. The Computer Confidence Subscale and Computer Anxiety Subscale of the Computer Attitude Scale and the Computer Self-Efficacy Measure were administered to both groups at three time intervals: at baseline, completion of the five-week intervention, and six weeks after completion of the intervention. Data were analyzed using repeated measures analysis of variance.
Results:
Findings showed a reduction in computer anxiety and increases in computer confidence and computer self-efficacy in retrieving and evaluating online health information (P<0.001).
Discussion:
The study suggests an array of possibilities to engage older adults in the use of Internet health information resources to better contribute to their health, independence, safety, and wellness.
Highlights
Older adults residing in low socioeconomic communities are often deprived of access to health care information. “Partnering with Seniors for Better Health” is a health communication project targeted at bridging the digital divide in this population.
Older adults showed decreased anxiety, increased confidence, and increased self-efficacy in using the Internet, as well as an increased interest in consumer health information retrieval on MedlinePlus and the National Institutes of Health (NIH) NIHSeniorHealth websites.
Implications
An audience-appropriate intervention, coupled with Bandura's self-efficacy theory in computer training, can make older adults more knowledgeable about health information, services, and resources available to them.
More interventions and support services are necessary in underserved communities to eliminate health disparities in older adults.
Background
There has been an explosion of online health information resources targeted specifically to older adults since the adoption of new technologies for health communication. However, the quality of online information and the readability level of this information has always been a concern to many health care providers and consumers.
Many older adults have unique physical and motor difficulties and, to some extent, cognitive impairment. Because motor skill decreases in old age, a person may find clicking a mouse or scrolling down a page much more difficult than someone who is younger. Vision may also be affected when backgrounds are heavily patterned or a page uses fancy fonts. Although the usability of health websites for older adults have improved greatly in recent years, most websites on the Internet do have serious readability problems such as small font sizes, inappropriate instruction on how to use video streaming, and too many activities on a single web page [1].
Low health literacy among older adults also directly limits their access to critical information concerning their rights to health and health care, whether this information involves following instructions to care, learning about diseases, or learning about disease prevention and health promotion. Low health literacy has an impact on cognitive and linguistic abilities; hence, it influences a person's ability to navigate in a literate environment such as the Internet [2,3]. Most commercial health websites studied are in the ninth-to-twelfth grade readability range, which is far above the recommended reading level for providing information to the public [4]. The recommended reading level for health information is between sixth and eighth grades [5].
Changes have been made to improve web access for older adults. Some examples include addressing design issues by increasing font sizes to meet the aging vision of the older adults, incorporating video streaming into websites for those with literacy issues, and including Spanish and other languages to meet the needs of a culturally diverse senior population [6]. To ensure that older adults have access to high-quality health information through the Internet, older adults need to be introduced to credible health websites and be educated on how to evaluate the credibility of the information retrieved on the Internet [7].
Not every older American with lower income, with lower education, and from rural parts of the country owns a computer or has Internet access. About 2 million people aged 65 years and above reside in the state of Texas [8]. Texas is among the top ten states with the highest poverty rates for older adults, at 14.4% as compared to the national rate of 10.2% [8]. The Internet may be a powerful tool that promises to bring information to underserved populations such as people with disabilities, those living in remote areas, and those with socially stigmatized health conditions [9]. However, the extent to which technology and the Internet have penetrated to lower socioeconomic communities is still open to question. The Kaiser report notes that older Americans with an annual family income of less than $20,000 are less likely to be able to go online [10], because personal computers are priced too high for low-income populations [4,11]. These groups are largely excluded from the benefits of Internet health resources, producing a gap between older Americans who have the privilege of Internet access and those who do not.
Objective 11-1 of health communication for Healthy People 2010 also recognizes that lower socioeconomic older Americans have the least access to information, communication technologies, health care, and supporting social services in their communities. Hence, one of the objectives of Healthy People 2010 is to improve Internet access in the home, by addressing all the factors that make an Internet connection valuable, such as basic computer literacy, effective narrowing of the gap of the digital divide, and unequal distribution of technology and technical skills in society [12].
Understanding the factors that contribute to promoting certain health behaviors—such as computer confidence, computer anxiety, and computer self-efficacy with respect to health information retrieval and evaluation of web content—are important for establishing evidence-based practice, which, at this stage is still in its infancy.
The objective of the study reported here was to narrow the digital divide and unequal access to technology among older adults in lower socioeconomic communities by designing an intervention, based on Bandura's self-efficacy model, that would assist older adults in developing skills and competence in online consumer health information retrieval and evaluation. The study measured changes in three psychosocial influences—computer anxiety, computer confidence, and computer self-efficacy—among older adults, sixty-five and above, who participated in and completed a five-week education intervention in health information retrieval and evaluation on the Internet.
The following hypothesis was tested: Older adults, ages sixty-five and above, who complete a five-week education intervention in online health information retrieval at congregate meal sites will report lower computer anxiety, higher computer confidence, and higher computer self-efficacy at the end of the intervention and six weeks after the completion of the intervention as compared to older adults not in the program.
Review of the Literature
Intervention Studies
Few intervention studies to date have examined how older adults residing in lower socioeconomic communities use computers and Internet search systems to locate health-related information. One reason for the lack of studies may be the stereotypical expectation that older adults are generally less accepting of innovations and technology, resulting in fewer interventions designed for this population [9]. A community-based telephone survey conducted among sixty residents ages ranging between eighteen and sixty-five and older from an urban, low-income community in Chicago showed that twenty-five participants in the intervention group who received training and access to WebTV, a printer, and researcher support experienced positive health-related empowerment with in-home technology use as compared to the thirty-five participants who did not receive the intervention [13].
The outcome of a cross-sectional survey that measured computer and Internet access and use of Internet health information with low income, urban African American caregivers of pediatric outpatients reported that only 52% of the 206 participants had used the Internet for health information and agreed that it would be ideal if they had the opportunity to connect to the Internet and had access to health information on the Internet [14].
A pre–post study of sixty older adults who received a five-week Internet training program at public libraries and community centers in the greater Pittsburgh and Allegheny County region showed statistically significant changes in locus of control and health information seeking at a five-week follow-up after the completion of the intervention [15]. The study also showed that a year after receiving Internet training, twenty-one of the twenty-seven respondents reported using the Internet weekly or as needed to locate health information.
Psychosocial Influences
Computer Anxiety
Computer anxiety is a well-studied concept in the field of information technology, although there are conflicting theories with respect to its origin. Computer anxiety is defined as the fear or apprehension individuals feel when they use computers or when they consider the possibility of computer use [16–18]. Computer anxiety is characterized as an affective response, an emotional fear of potential negative outcomes, such as damaging the equipment or looking foolish [19]. A high level of computer anxiety has been negatively related to learning computer skills [20] and positively related to resisting the use of computers [21] and performing poorly on a task [22].
Computer Confidence
Computer confidence is defined as the ability to use or learn to use a computer [23]. Statements such as “I have a lot of confidence when it comes to working with computers” and “I am sure I could do work with computers” have been used to measure computer confidence. Computer confidence has also been shown to be inversely related to computer anxiety [24] and significantly related to computer utilization [25].
Computer Self-Efficacy
Computer self-efficacy has been identified as a key determinant of computer-related ability and use of computers [26]. The term is derived from the general concept of self-efficacy [27] and refers to individuals' perception of their ability to successfully perform a computing task and their intentions for future use of computers [28]. Zhang and Espinoza also reported that computer self-efficacy was positively related to enrolling in computer courses [29].
Theoretical Framework
The study is guided by Bandura's self-efficacy theory, a major component of Bandura's social learning theory [30]. Self-efficacy is a context-specific assessment of competence to perform a task in a given domain. Self-efficacy is the belief in “one's capability to organize and execute the courses of action required to manage prospective situations” [31]. Self-efficacy influences the choices an individual makes. The stronger the feelings of efficacy, the more effort and persistence a person will put forth in the face of obstacles and aversive experiences [30].
Model Specification
Figure 1 presents a theoretical model of computer training based on Bandura's self-efficacy theory. The model hypothesizes that a computer training experience that incorporates all four major components of efficacy expectations will positively influence computer confidence and lower anxiety toward computer use, leading to increased computer self-efficacy. Higher confidence and lower anxiety will positively and simultaneously affect one another. Higher confidence will positively lower anxiety toward computer use, and lower anxiety will positively increase confidence with computer use as shown. The model anticipates that both these variables will enhance the outcome expectation of computer self-efficacy because studies have suggested that anxiety and confidence essentially measure the same construct [23,32].
Figure 1.
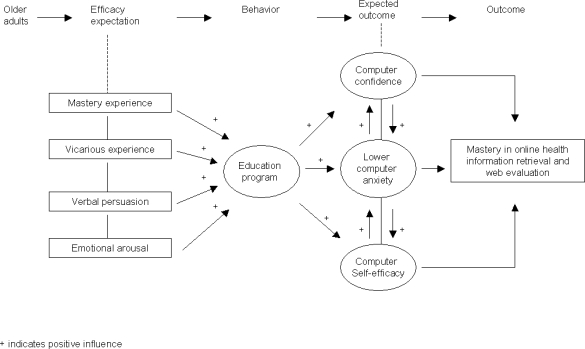
Hypothesized model of computer confidence and computer anxiety in the prediction of computer self-efficacy in a computer training program
The concept of self-efficacy is derived from four major sources of efficacy expectations: (1) mastery experiences, (2) vicarious experience, (3) verbal persuasion, and (4) emotional arousal. The most influential of these expectations is the interpreted result of one's performance, or “mastery experience” [33]. In the current study, performing a computer task would successfully raise mastery experience, while repeated failures would lower it. Accordingly, for example, when teaching how to evaluate the quality of a health website using standardized evaluation criteria, the instructor first performed the exercise in easily mastered steps, closely following the criteria taught in the course content. Participants then executed the modeled activity with appropriate guidance (participant modeling). Mistakes and failures were identified and corrected at this early stage until participants were able to perform the task confidently (performance exposure and desensitization). Working with an instructor allowed participants to engage in computer use with less anxiety and higher confidence. Reinforcement of course content, using case studies and handouts with exercises at every lesson in the intervention plan, provided supplementary practice on the learners' own time and allowed active participation in learning (self-instructed performance), hence reinforcing self-directed mastery experience.
The second source of efficacy expectations is the “vicarious experience” of the effects produced by the actions of others. This source of information is weaker than the interpreted results of mastery experiences, but when individuals are uncertain about their own abilities or have limited prior experience, they become more sensitive to the task at hand [30,33]. Therefore, achieving a vicarious experience of success provides a significant model that instills self-beliefs that can influence the course and direction an individual will take [30,33]. Accordingly, the intervention program was designed so that every participant had access to a computer in the classroom for adequate hands-on training. Live modeling with the instructor and observing other participants performing a computer activity with no adverse consequences was also provided to create self-efficacy through vicarious experience as the learners intensified and persisted in their efforts at learning a new skill.
Individuals can be led into believing that they can cope successfully through persuasive suggestions [30,33]. Although “verbal persuasion” is a weaker source of efficacy information than mastery and vicarious experiences, verbal persuasion plays a vital role in an individual's self-belief [30,33]. Verbal persuasions include suggestion, exhortation, self-instruction, and interpretive treatment. Conveying positive appraisals and social encouragement was part of the intervention: persuasions prompted participants to intensify their efforts in pursuing the accomplishment of a specific computer task and reaching higher self-efficacy belief [30,33]. Teaching strategies such as the use of questioning and repeated demonstration created opportunities for verbal exhortation.
“Emotional arousal,” the fourth source of efficacy expectations, includes responses such as anxiety, stress, fatigue, and mood change. Individuals have the ability to alter their own thoughts and actions [30,33]. Bandura theorizes that “people rely upon their state of physiological arousal in judging their anxiety and vulnerability to stress” [30]. Perceived self-efficacy in exercising control over stressors plays a central role in anxiety arousal [34]. When individuals believe they can exercise control over learning Internet searches on the computer, they do not conjure up disturbing thought patterns about computer use. On the contrary, when individuals believe they cannot manage the threat of computer and Internet use, they experience high anxiety arousal, dwelling on their own coping deficiencies. Attribution, relaxation, biofeedback, and symbolic desensitization and exposure can influence emotional arousal [30], thus enhancing optimism among older adults in computer training. The intervention program created a positive learning environment closely related to the practice of the real world to promote self-belief expectations and minimize aversive arousal leading to high anxiety and agitation [27].
Methodology
The research study utilized a randomized, controlled, repeated measures design with two groups to measure changes in the psychosocial influences of computer anxiety, computer confidence, and computer self-efficacy among older adults following a five-week structured program. The program, “Partnering with Seniors for Better Health,” introduced computer literacy and health information retrieval on the Internet. Adults in the program were compared to older adults who were not enrolled. The variables were measured at three time intervals: before the program, at the completion of the program, and six weeks following the completion of the program. The study eligibility criteria required that all participants: (1) read and understand English, (2) be able to identify the on switch button on the computer and hold a mouse to navigate the arrow on the screen, and (3) self-identify the ability to do simple typing on a keyboard.
Participants and Setting
Participants were older adults, sixty-five years and above, enrolled at congregate meal sites of the YWCA. The congregate meal sites were located in various senior or community centers, and in some instances churches, that provided meals and leisure activities for mobile adults in the greater Houston area. These lunches and organized activities were a form of social outlet for older adults who attended the congregate meal sites. The classes were conducted at a facility of the YWCA Houston. A computer lab was set up at the facility especially for this project. The sessions were taught using PowerPoint slides projected on a screen. Transportation to bring participants to the facility for classes was provided by the YWCA staff. Financial remuneration in the form of a gift card was given to participants who completed the study.
Instruments
The Computer Anxiety Subscale of the Computer Attitude Scale [23] is a ten-item Likert-type instrument measuring computer anxiety with responses ranging from “strongly agree” to “strongly disagree.” Higher scores on the scale reflect lower degree of anxiety. The Computer Confidence Subscale of the Computer Attitude Scale [23] is also a ten-item Likert-type instrument measuring computer confidence, with responses ranging from “strongly agree” to “strongly disagree.” Higher scores represent more confidence with computer use.
The Computer Self-Efficacy Measure [35] is five-item Likert scale measuring participants' levels of self-efficacy using the Internet to locate health information. This scale was modified with permission from the author to change all the items that were written in question format to statements for ease of use. For example, “How confident are you that you can learn to use ‘search tools’ to find information on the Internet?” was changed to “I am confident I can learn to use ‘search tools’ to find information on the Internet,” with responses ranging from “strongly agree” to “strongly disagree.” Higher scores represent higher feelings of self-efficacy toward using the Internet to search for information.
Content validity tests of the 3 instruments were conducted to ensure the measurements were appropriate for use with older adults. Experts consisting of health care professionals and community lay leaders who have experienced working with older adults were asked to participate in a validity survey. Nine of the 10 content and lay experts responded to the request. The content validity indexes for the 3 measurement scales fell between 0.93–1.0 for representativeness and 0.87–0.92 for clarity. The inter-rater agreement was acceptable at 0.8–1.0 for representativeness and 0.60–0.080 for clarity. Alpha coefficient reliabilities were 0.82, 0.72, and 0.83 for the Computer Anxiety Subscale, the Computer Confidence Subscale, and the Computer Self-Efficacy Measure.
Program: “Partnering with Seniors for Better Health”
The curriculum for “Partnering with Seniors for Better Health” consisted of two components: a computer literacy section that included instruction in correct mouse handling, basic Google search techniques, and methods of evaluating online health information. The second component introduced participants to consumer health information searches on MedlinePlus, the National Institutes of Health (NIH) NIHSeniorHealth, and Go Local. The program was taught by two instructors. The computer literacy instruction, Google search, and evaluation of health information on the web were taught by the principal investigator. The Internet health information searches were conducted by a consumer health librarian. The class was conducted once a week for five weeks, and each lesson lasted two hours with a fifteen-minute snack break in between. Training manuals were given to participants at each instructional session. As described earlier, methods designed to promote Bandura's self-efficacy expectations were incorporated into class activities. Reinforcing skills and conveying positive verbal and social encouragement were provided when participants solved problems as a group. Freebies were also given away at every session as incentives for helping and supporting one another as they learned together.
Data Collection Procedure
Permission to conduct the study was obtained from the Institutional Review Board at the Texas Woman's University and YWCA Houston. Participants, ages sixty-five and above, were enrolled in the study through distribution of flyers and sign-up sheets at six meal congregate sites. The investigator met with eligible participants to obtain signed informed consent, followed by administration of baseline measures consisting of the Computer Anxiety Subscale, Computer Confidence Subscale, and Computer Self-Efficacy Measure at each site. Eligible participants were assigned to either the intervention or wait-list control group according to their identification numbers, using randomized numbers generated on the computer. Participants in the intervention group attended the five-week education intervention.
The principal investigator met participants in person to administer posttest measurement of computer anxiety, computer confidence, and computer self-efficacy at the end of the five-week program and six weeks after the completion of the five-week program for both intervention and wait-list control groups. Program evaluation was obtained from participants in the intervention group at the completion of the last class session. Participants in the wait-list control group were offered the program after the termination of the research study.
Results
A total of 137 participants were recruited for the study from July 2007 to February 2008. Twenty-five participants dropped out of the study for various reasons. Some participants were relocated to other parts of the town due to a fire at one of the participating congregate meal sites, and others decided to opt out because they felt they had waited too long to take a class. A few moved away from the participating congregate meal sites for personal reasons. The attrition rate was at 18%.
Of the 112 multiethnic participants eligible for analysis, 72.0% were female. The mean age was at 74 years. Sixty-four percent of these participants' annual family incomes were below the $10,000 poverty line. All participants had at least some form of education ranging from less than high school to postgraduate degrees; only 21.4% of the participants had completed less than high school. Fifty percent of the participants had high school or some college or a technical degree. Of the participants, 70.5% had never used a computer before and almost 81.2% had never used or never had access to the Internet, even though 46% mentioned that they or a member of their family owned a computer. When participants were asked the reasons for not using a computer, 42.9% mentioned they did not have the opportunity to learn, while 25.0% of the older adults mentioned they did not have access to a computer. Similar questions were asked about Internet use. The findings showed that 71.4% of the older adults either did not have access to the Internet or they had no opportunity to learn how to get online. Of the 112 participants enrolled in the study, 70 believed that the Internet could be used to find medical information that would be useful in managing their health care, 3 participants responded negatively, and 39 participants were uncertain. Interestingly, almost 92% of the participants were not aware that computers and Internet access were available and accessible to the public at community centers and public libraries.
Computer Anxiety
The results of the repeated measures analysis of variance at baseline, at the completion of the 5-week training program, and 6 weeks after the completion of the program were analyzed with SPSS, version 16. A decrease in computer anxiety was noted after the completion of the program and maintained 6 weeks after the intervention (Figure 2). The results showed the means for computer anxiety at baseline (M = 26.13; SD = 5.77), at the completion of the 5-week training (M = 34.87; SD = 5.37), and 6 weeks after the training (M = 35.05; SD = 5.39) were significantly different F (2, 109) = 68.14, P<0.001). It is important to note that the larger the mean, the lower the anxiety toward computer use and information retrieval online.
Figure 2.

Computer anxiety score
Computer Confidence
Likewise, participants' confidence toward computer use and health information retrieval increased after the completion of the intervention and remained high 6 weeks after the intervention (Figure 3). The means for computer confidence at baseline (M = 28.26; SD = 5.40), at the completion of the 5-week training (M = 35.95, SD = 5.25), and 6 weeks after the completion of training (M = 36.10; SD = 5.18) indicated significant change over time (F (2, 109) = 56.21, P<0.001).
Figure 3.

Computer confidence scores
Computer Self-Efficacy
Perceptions of computer self-efficacy with respect to health information retrieval also increased after the completion of the intervention program and remained high 6 weeks after the completion of the program (Figure 4). Computer self-efficacy scores at baseline (M = 13.90; SD = 2.74), at the completion of the 5-week training (M = 17.76; SD = 2.58), and 6 weeks after the completion of the 5-week training (M = 17.87; SD = 2.63) showed a significant difference (F (2, 109) = 51.61, P<0.001).
Figure 4.

Computer self-efficacy scores
Participants who completed the intervention were also asked how they would evaluate the overall program content and instructional method and how they would use the information they had learned to manage their own health matters. More than half of the participants who completed the program agreed that the experience was an eye-opener, like “opening a Pandora's box” as one participant put it.
At the end of the intervention program, 95% of the participants reported they felt more confident exploring and evaluating health information online, planned on using the health information received on the Internet to manage their chronic illnesses, and had learned more about prescription drugs and Medicare benefits and would share this information with their friends and family members. Forty-five percent of the participants also reported more confidence in taking a collaborative role in their own health management, such as discussing and making important decisions about their health care needs with their physicians. Three participants mentioned that their physicians would not be interested in discussing Internet health information with them at a typical doctor's visit but stated they would try nonetheless. Incorporating time for hands-on practice was found to be useful, and almost 90% of the participants appreciated the various forms of social and verbal support from their peers and the trainers. Participants said they experienced less anxiety when learning a new skill as a group and felt less stress when instructors and peers worked together as a team.
The survey also asked participants to share with the researchers what they liked best or least about the MedlinePlus and NIHSeniorHealth websites. Sixty-five percent of the participants who completed the program reported that they liked MedlinePlus for its comprehensive content. The remaining 35% of the participants liked NIHSeniorHealth for its navigation features such as the ability to increase and decrease font size and background contrast and the short, one-page paragraph information on every content page. About 52% of the participants would prefer that MedlinePlus have similar features to those found in NIHSeniorHealth, such as the ability to increase font size and background contrast that were available in the latter. The prescription and supplement drug page of MedlinePlus had the most hits during the course of the program. Several participants also enjoyed Go Local Gulf Coast for locating local health information resources in their area.
Participants also agreed that they would prefer both that MedlinePlus and NIHSeniorHealth websites have translations to various languages besides Spanish, which was currently only available in MedlinePlus. Although MedlinePlus included a health information section that linked to multiple language sites, 15% of the participants who lived with non-English speaking relatives found consumer health information on the parent site more useful and hoped to be able to share it with family members who could not read or understand English and Spanish.
Participants were interviewed 6 weeks after the completion of the intervention. The results showed that 62% of the participants who had computers and Internet access in the home or had purchased a computer and subscribed to an Internet telephone line during the course of the program continued to use their computers to use Google to search for information and to use MedlinePlus to search for health information online. Most of the interviewed participants preferred to obtain a computer and an Internet line in the comfort of their homes than to use the public computers available in libraries and community centers. Only 1% of the participants who could not afford a computer drove to the nearest public library to use the Internet.
Discussion
The findings showed that participants in the intervention group had lower anxiety, higher confidence, and higher self-efficacy toward use of computers and toward health information searches on the Internet and that these changes persisted over time. No activity or booster session was given prior to the third interview six weeks after the completion of the intervention, yet the increase in scores was statistically significant and maintained six weeks after the completion of the five-week intervention.
Older adults are enthusiastic learners. The study observed that older adults needed very little encouragement to take on the task of learning new technology. They might take slightly longer to move and click the mouse, locate a letter on the keyboard, and read a paragraph on the web page, but they were persistent and refused to quit until they had mastered the task at hand. A combination of patience, perseverance, and peer-to-peer or instructor encouragement, whether with words or a pat on the shoulder, successfully reduced their stress and anxiety in learning and raised their self-efficacy and confidence while completing the program.
Older adults were grateful for the opportunity to learn to use computers and the Internet. As mentioned earlier, most of these adults did not have computers or Internet access in their homes. As such, the only contact time with a computer was during the five-week program. With their enthusiasm and newly developed quest for knowledge, a handful of these participants actually received free or hand-me-down computers from their families to be installed at their homes. Older adults were also able to obtain refurbished computers at a very low price from a local nonprofit organization that provides basic computer services to seniors and those with disabilities in the greater Houston area.
The study faced several challenges. Because this was an intervention study with participants randomized to the study and wait-list control groups, the researchers found it difficult to convince participants in the wait-list control group that they would be given the opportunity to take the program after the termination of the study. Participants in the wait-list control group were unhappy and frustrated with waiting so long in the process. Frequent on-sites visitations and telephone calls were made to participants in the wait-list control group to keep them aware of the progress of the study.
The study group participants also mentioned that the program did not have enough time for practice and exploration. The present study allowed a forty-five-minute practice period at the end of each lesson. The computer training program was conducted at a facility of one of the YWCA buildings. Transportation had to be arranged to bring the participants to the facility from the congregate meal sites. Classes were often not started on schedule because participants who required private transportation to the congregate meal sites often arrived too late for the YWCA transportation to bring them to the computer lab. Numerous negotiations and telephone calls were made to these private transportation services to bring participants to the congregate meal sites on time. Moreover, there was a stipulated time for participants to return to the congregate meal sites for lunch and for their private transportation to return them to their homes. Hence, practice times at the end of the lessons were often shortened to thirty minutes or less to accommodate the participants' stipulated lunch hours at the congregate meal sites.
Several study limitations were noted. The study was conducted in English. As a result, older adults who resided in the low socioeconomic community and could not speak or understand English were disqualified from the study. One of the goals of effective health communication is to get health information content out to the largest possible number of people in a target population [12]. Two recommendations from the authors are to develop programs in other languages and to have instructors who could speak more than one language in order to reach older adults of different races and ethnicities so that they, too, can enjoy the opportunity of health information and digital technology.
The current study documented positive differences in computer anxiety, computer confidence, and computer self-efficacy scores after a five-week intervention. The study, however, did not explore if such psychosocial changes led to more actual usage of Internet health information resources or whether the intervention impacted the lives of older adults in low socioeconomic communities in the long term. Moreover, even though the intervention focused on training in health information seeking and use, the study failed to provide sufficient information on the effect of the intervention on seniors' ability to evaluate health information online. Further study is recommended to explore how older adults use the Internet for health information matters after attending a health communication activity such as this and what role the activity plays in their lives and the lives of those around them.
Conclusion
The study was effective in providing the ideas and tools to carry out a health communication program among an urban, low socioeconomic community of older adults. Older adults who participated in the five-week program on retrieving and evaluating health information online increased their confidence and feelings of self-efficacy with respect to computer and Internet use and lowered their anxiety levels with respect to these activities. The study affirmed that feelings of self-efficacy did not necessarily decline in old age. The model also affirmed that a well-designed program, guided by Bandura's four major sources of efficacy expectations—mastery experiences, vicarious experience, verbal persuasion, and emotional arousal—can result in positive behavioral outcomes for study participants. Participants modeled and challenged one another to excel throughout the intervention study, providing encouragement and support to those who faced technical challenges.
Acknowledgments
The authors thank Adela Justice, co-instructor of the program, “Partnering with Seniors for Better Health,” who is also a consumer health librarian at the Houston Academy of Medicine-Texas Medical Center Library, for her assistance in planning and teaching the health information searches and retrieval on MedlinePlus, NIHSeniorHealth, and Go Local. The authors also thank the participants at the congregate meal sites, the staff of the YWCA Houston, and the staff of the Houston Academy of Medicine-Texas Medical Center Library for their full support of and collaboration in the success of the study. The authors are grateful to the following persons for granting permission to use and modify their materials and the measuring instruments used in this study for data collection: Robert Campbell for the Computer Self-Efficacy Measure Instrument and Clarice Gressard and Brenda Loyd for the Computer Anxiety Subscale and the Computer Confidence Subscale of the Computer Attitude Scale. This project is funded through a research grant by Sigma Theta Tau International Nursing Society, Beta Beta Houston, Texas.
Footnotes

This article has been approved for the Medical Library Association's Independent Reading Program <http://www.mlanet.org/education/irp/>.
Contributor Information
Adeline Chu, College of Nursing; Texas Woman's University, Institute of Health Sciences-Houston Center, 6700 Fannin, Houston, TX 77030. adeln@twu.edu.
Jeffrey Huber, School of Information and Library Science; Texas Woman's University, Institute of Health Sciences-Houston Center, 6700 Fannin, Houston, TX 77030. jhuber@twu.edu.
Beth Mastel-Smith, College of Nursing; Texas Woman's University, Institute of Health Sciences-Houston Center, 6700 Fannin, Houston, TX 77030. bmastelsmith@twu.edu.
Sandra Cesario, College of Nursing; Texas Woman's University, Institute of Health Sciences-Houston Center, 6700 Fannin, Houston, TX 77030. scesario@twu .edu.
References
- 1.Nahm E., Preece J., Resnick B., Mills M. Usability of health web sites for older adults: a preliminary study. Comput Inform Nurs. 2004 Nov–Dec;22(6):326–36. doi: 10.1097/00024665-200411000-00007. [DOI] [PubMed] [Google Scholar]
- 2.Baker D., Parker R., Williams M., Pitkin K., Parik N., Coates W., Imara M. The health experience of patients with low literacy. Arch Fam Med. 1996 Jun;5(6):329–34. doi: 10.1001/archfami.5.6.329. [DOI] [PubMed] [Google Scholar]
- 3.Parikh N.S., Parker R.M., Nurss J.R., Baker D.W., Williams M.V. Shame and health literacy: the unspoken connection. Patient Educ Couns. 1996 Jan;27(1):33–9. doi: 10.1016/0738-3991(95)00787-3. [DOI] [PubMed] [Google Scholar]
- 4.Birru M.S., Monaco V.M., Charles L., Drew H., Njie V., Bierria T., Detlefsen E., Steinman R.A. Internet usage by low-literacy adults seeking health information: an observational study. J Med Internet Res. 2004 Sep;6(3):e25. doi: 10.2196/jmir.6.3.e25. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Freda M.C. Issues in patient education. J Midwifery Womens Health. 2004 May–Jun;49(3):203–9. doi: 10.1016/j.jmwh.2004.01.003. [DOI] [PubMed] [Google Scholar]
- 6.Alpay L., Toussaint P., Ezendam N., Rövekamp T., Graafmans W., Westendorp R. Easing Internet access of health information for elderly users. Health Informatics J. 2004;10(3):185–94. [Google Scholar]
- 7.Bates B., Romina S., Ahmed R., Hopson D. The effect of source credibility on consumer's perceptions of the quality of health information on the Internet. Med Informat Internet Med. 2006 Mar;31(1):45–52. doi: 10.1080/14639230600552601. [DOI] [PubMed] [Google Scholar]
- 8.American Association of Retired Persons. National survey on consumer preparedness and e-commerce: a survey of computer users age 45 and above [Internet] Washington, DC: The Association; 2000 [cited 18 Jan 2008]. < http://assets.aarp.org/rgcenter/consume/ecommerce.pdf>. [Google Scholar]
- 9.Wagner L.S., Wagner T.H. The effect of age on the use of health and self-care information: confronting the stereotype. Gerontologist. 2003 Jun;43(3):318–24. doi: 10.1093/geront/43.3.318. [DOI] [PubMed] [Google Scholar]
- 10.Kaiser Family Foundation. E-health and the elderly: how seniors use the Internet for health—survey [Internet] Washington, DC: The Foundation; 2005 [cited 18 Jan 2008]. < http://www.kff.org/entmedia/upload/e-Health-and-the-Elderly-How-Seniors-Use-the-Internet-for-Health-Information-Key-Findings-From-a-National-Survey-of-Older-Americans-Survey-Report.pdf>. [Google Scholar]
- 11.Lai C., Arthur D., Chau W. Implication of Internet growth on enhancing health of disadvantaged groups in China: a global perspective. J Clin Nurs. 2004 Sep;13(6B):68–73. doi: 10.1111/j.1365-2702.2004.01046.x. [DOI] [PubMed] [Google Scholar]
- 12.Office of Disease Prevention and Health Promotion, Department of Health and Human Services. Healthy people 2010: 11 health communications [Internet] Bethesda, MD: The Department; 2006 [cited 18 Jan 2008]. < http://www.healthypeople.gov/document/HTML/Volume1/11HealthCom.htm>. [Google Scholar]
- 13.Masi C.M., Suarez-Balcazar Y., Cassey M.Z., Kinney L., Piotrowski Z.H. Internet access and empowerment: a community-based health initiative. J Gen Intern Med. 2003 Jul;18(7):525–30. doi: 10.1046/j.1525-1497.2003.20344.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Kind T., Huang Z.J., Farr D., Pomerantz K.L. Internet and computer access and use for health information in an underserved community. Ambul Pediatr. 2005 Mar–Apr;5(2):117–21. doi: 10.1367/A04-107R.1. [DOI] [PubMed] [Google Scholar]
- 15.Campbell R.J., Nolfi D.A. Teaching elderly adults to use the Internet to access health care information: before-after study. J Med Internet Res. 2005 Jun 30;7(2):e19. doi: 10.2196/jmir.7.2.e19. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Simonson M.R., Maurer M.M., Montag-Torardi M., Whitaker M. Development of a standardized test of computer literacy and a computer anxiety index. J Educ Com Res. 1987;3(2):231–47. [Google Scholar]
- 17.Maurer M.M. Development and validation of a measure of computer anxiety [master's thesis] Ames, IA: Iowa State University; 1983. [Google Scholar]
- 18.Chua S.L., Chen D., Wong A.F.L. Computer anxiety and its correlates: a meta-analysis. Computers Human Behav. 1999;15:609–23. [Google Scholar]
- 19.Hong K.S., Othman A.E.A., Nordin Z.S. Computer self-efficacy, computer anxiety and attitudes toward the Internet: a study among undergraduates in Unimas. EducTech Soc. 2005;8(4):205–19. [Google Scholar]
- 20.Harrington K.V., McElroy J.C., Morrow P.C. Computer anxiety and computer-based training: a laboratory experiment. J Edu Comput Res. 1990;6:343–58. [Google Scholar]
- 21.Torkzadeh G., Angula I.E. The concept and correlates of computer anxiety. Behav Inform Tech. 1992;11:99–108. [Google Scholar]
- 22.Heinssen R.K., Glass C.R., Knoght L.A. Assessing computer anxiety: development and validation of the computer anxiety rating scale. Comput Human Behav. 1987;3:49–59. [Google Scholar]
- 23.Gressard C.P., Loyd B.H. Validation studies of a new computer attitude scale. Assoc Edu Data Syst J. 1986;18(4):295–301. [Google Scholar]
- 24.Loyd B.H., Loyd D.H. The reliability and validity of an instrument for the assessment of computer attitudes. Edu Psy Meas. 1985;45(4):903–8. [Google Scholar]
- 25.Al-Khaldi M.A., Al-Jabri I.M. The relationship of attitudes to computer utilization: new evidence from a developing nation. Comput Human Behav. 1998;14(1):23–42. [Google Scholar]
- 26.Doll W., Torkzadeh G. A discrepancy model of end-user computing involvement. Manag Sci. 1989;35:1151–71. [Google Scholar]
- 27.Bandura A. Social foundations of thought and action: a social cognitive theory. Englewood Cliffs, NJ: Prentice-Hall; 1986. [Google Scholar]
- 28.Compeau D.R., Higgins C.A. Computer self-efficacy: development of a measure and initial test. MIS Q. 1995;19:189–211. [Google Scholar]
- 29.Zhang Y., Espinoza S. Relationships among computer self-efficacy, attitudes towards computers, and desirability of learning computing skills. J Res Tech Edu. 1998;30(4):420–36. [Google Scholar]
- 30.Bandura A. Social learning theory. Englewood Cliffs, NJ: Prentice-Hall; 1977. [Google Scholar]
- 31.Bandura A. Self-efficacy in changing society. New York, NY: Cambridge University Press; 1995. [Google Scholar]
- 32.Woodrow J.E.J. The development of computer-related attitudes of secondary students. J Edu Comput Res. 1994;11:307–38. [Google Scholar]
- 33.Pajares F. Current directions in self-efficacy research. In: Maehr M., Pintrich P.R., editors. Advances in motivation and achievement. Vol. 10. Greenwich, CT: JAI Press; 1995. pp. 1–49. [Google Scholar]
- 34.Bandura A. Self-efficacy. In: Ramachaudran V.S., editor. Encyclopedia of human behavior. Vol. 4. New York, NY: Academic Press; 1994. pp. 71–81. [Google Scholar]
- 35.Campbell R. Older women and the Internet. J Women Aging. 2004;16(1–2):161–74. doi: 10.1300/J074v16n01_11. [DOI] [PubMed] [Google Scholar]