

A 53-year-old postmenopausal woman presented at the emergency department shortly after an episode of intense emotional stress. She was experiencing angina-like chest pain. An electrocardiogram (ECG) showed ST-segment elevation in the anterolateral and inferior leads (Fig. 1). Immediate coronary angiography revealed normal coronary arteries.
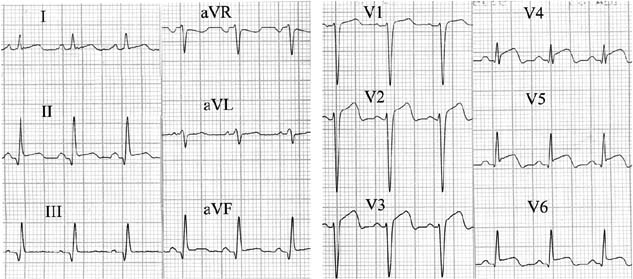
Fig. 1 Electrocardiogram shows ST-segment elevation in the anterolateral and inferior leads.
Two-dimensional echocardiography showed extensive mid-ventricular and apical akinesis and a large mural thrombus in the apex (Fig. 2) of the left ventricle (LV). Basal segments of the LV were hyperkinetic, generating a LV outflow tract (LVOT) gradient of 144 mmHg (Fig. 3). The LV ejection fraction (LVEF) was 0.32, in accordance with the Simpson rule.
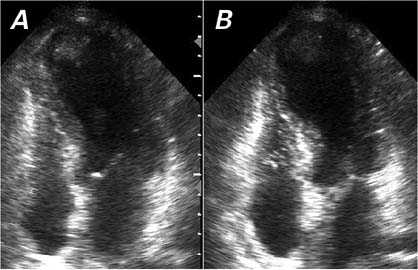
Fig. 2 A) End-diastolic and B) end-systolic 2-dimensional echocardiograms show left mid-ventricular and apical akinesis of the left ventricle, with a large mural thrombus in the apex.
Real-time motion image is available at www.texasheart.org/journal.
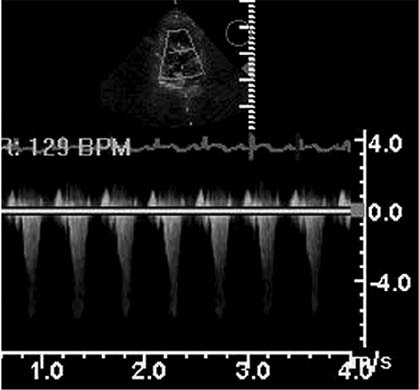
Fig. 3 Continuous-wave Doppler echocardiogram shows a high-velocity flow of 6.0 cm/sec at the left ventricular outflow tract, with a pressure gradient of 144 mmHg.
The following hormone levels were highly elevated in the urine: epinephrine, 8,720 (reference range, 0–190); norepinephrine, 7,650 (reference range, 0–620); and dopamine, 8,020 (reference range, 425–2,610). The cardiac enzymes were moderately elevated (peak creatine kinase, 1,690 U/L; and peak troponin I, 2.74 μg/L). Results of serum tests for viral infections were negative. Computed tomography revealed a cystic mass of the left adrenal gland (Fig. 4).

Fig. 4 Computed tomographic scan reveals a solitary cystic mass of the left adrenal gland.
The patient was treated with heparin (intravenous), aspirin, a diuretic, and an α-adrenergic blocker. Two weeks later, echocardiography showed normal LV regional systolic function (Fig. 5), absence of the mural thrombus, and no LVOT obstruction. The LVEF was 0.60. Histopathologic examination after surgery confirmed a diagnosis of pheochromocytoma (Fig. 6).
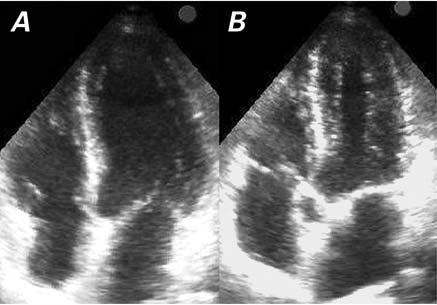
Fig. 5 A) End-diastolic and B) end-systolic 2-dimensional echocardiograms show normalization of the left ventricular systolic function and the absence of apical thrombus.
Real-time motion image is available at www.texasheart.org/journal.
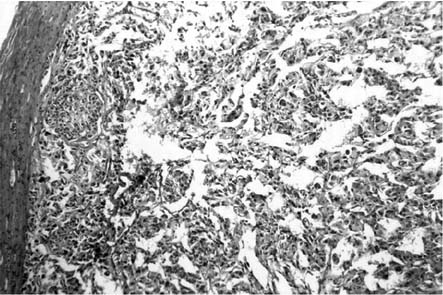
Fig. 6 Postoperative results of histopathologic examination confirm the diagnosis of pheochromocytoma (H & E, orig. ×200).
Comment
Transient LV apical ballooning, first described as takotsubo cardiomyopathy in 1990 by Sato and colleagues,1 is a syndrome characterized by a reversible balloon-like asynergy in the apical regions of the LV and excessive contraction in the basal regions. It may account for 1% to 2% of patients who present with an acute myocardial infarction2 and up to 1 in 30 cases of primary angioplasty in some institutions.3 Several pathophysiologic mechanisms of transient LV apical ballooning have been proposed, such as coronary vasospasm, abnormalities in coronary microvascular function, and direct catecholamine-mediated myocardial stunning.
Transient LV apical ballooning can be categorized as primary (takotsubo cardiomyopathy, idiopathic, or stress-related), or secondary to catecholamine-related entities (takotsubo-like), including adrenal4 or extra-adrenal5 pheochromocytoma-induced cardiomyopathy. For clinical diagnosis of transient LV apical ballooning, all 4 criteria proposed by Prasad2 (Mayo Clinic) should be present. For a diagnosis of primary transient LV apical ballooning, one of the criteria is the absence of a known catecholamine-mediated state.2,5,6
Transient LV apical ballooning syndrome has occasionally been associated with the development of LV mural thrombus.7 In addition, hemodynamically significant, dynamic LVOT obstruction has been observed in some patients.8
We present a case that encompasses all of the above-mentioned features of transient LV apical ballooning syndrome. This case, to our knowledge, is unique.
Supplementary Material
Footnotes
Address for reprints: Igor Mrdovic, PhD, Clinical Center of Serbia, Institute for Cardiovascular Diseases, Emergency Hospital, Coronary Care Unit A, Pasterova 2, 11000 Belgrade, Serbia. E-mail: igormrd@gmail.com
References
- 1.Sato, Tateishi H, Uchida T, et al. Takotsubo-type cardiomyopathy due to multivessel spasm. In: Kodama K, Haze K, Hon M, editors. Clinical aspect of myocardial injury: from ischemia to heart failure [in Japanese]. Tokyo; Kagakuhyouronsya Co.; 1990. p. 56–64.
- 2.Prasad A. Apical ballooning syndrome: an important differential diagnosis of acute myocardial infarction. Circulation 2007;115(5):e56–9. [DOI] [PubMed]
- 3.Iqbal MB, Moon JC, Buttmann OP, Shanahan P, Goadsby PJ, Holdright DR. Stress, emotion and the heart: Tako-tsubo cardiomyopathy. Postgrad Med J 2006;82:e29; doi:10.1136/pgmj.2006.051367. [DOI] [PMC free article] [PubMed]
- 4.Sanchez-Recalde A, Costero O, Oliver JM, Iborra C, Ruiz E, Sobrino JA. Images in cardiovascular medicine. Pheochromocytoma-related cardiomyopathy: inverted Takotsubo contractile pattern. Circulation 2006;113(17):e738–9. [DOI] [PubMed]
- 5.de Souza F, Altenburg Odebrecht Curi Gismondi R, Henriques Cunha Neto S, de Mattos MA. Tako-tsubo-like cardiomyopathy and extra-adrenal pheochromocytoma: case report and literature review. Clin Res Cardiol 2008;97(6):397–401. [DOI] [PubMed]
- 6.Bybee KA, Kara T, Prasad A, Lerman A, Barsness GW, Wright RS, Rihal CS. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med 2004;141(11): 858–65. [DOI] [PubMed]
- 7.Tibrewala AV, Moss BN, Cooper HA. A rare case of tako-tsubo cardiomyopathy complicated by a left ventricular thrombus. South Med J 2006;99(1):70–3. [DOI] [PubMed]
- 8.Penas-Lado M, Barriales-Villa R, Goicolea J. Transient left ventricular apical ballooning and outflow tract obstruction. J Am Coll Cardiol 2003;42(6):1143–4. [DOI] [PubMed]
Associated Data
This section collects any data citations, data availability statements, or supplementary materials included in this article.