

Abstract
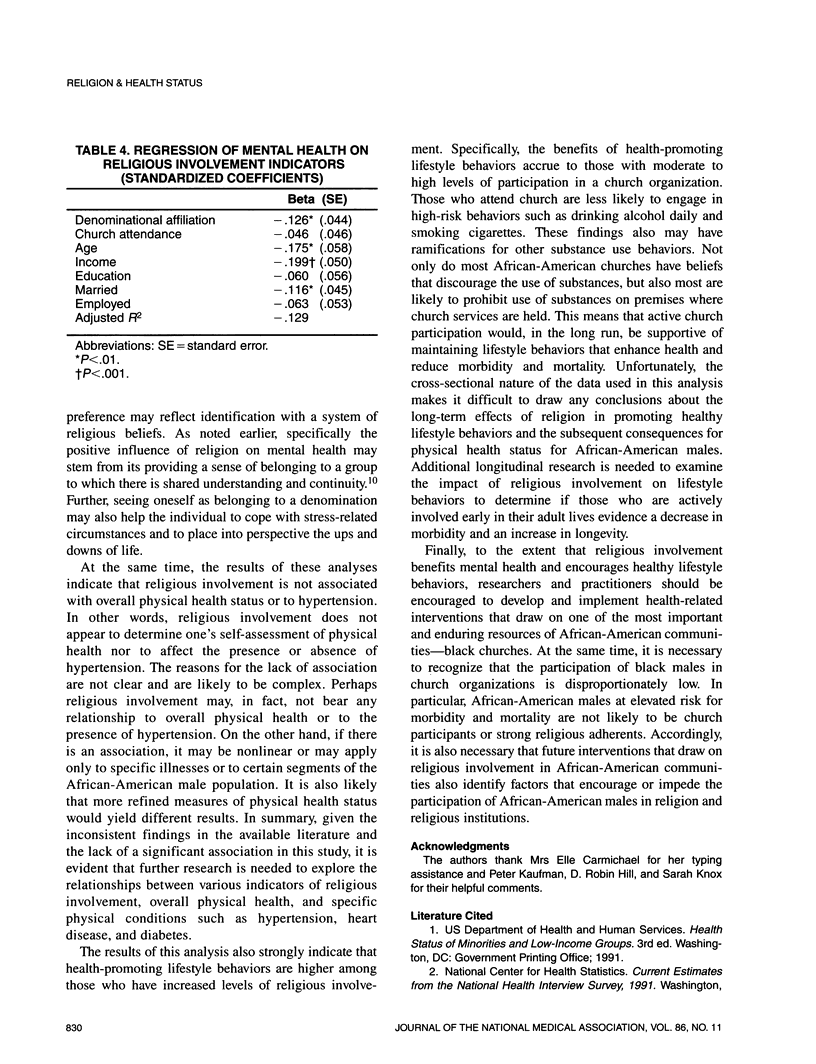
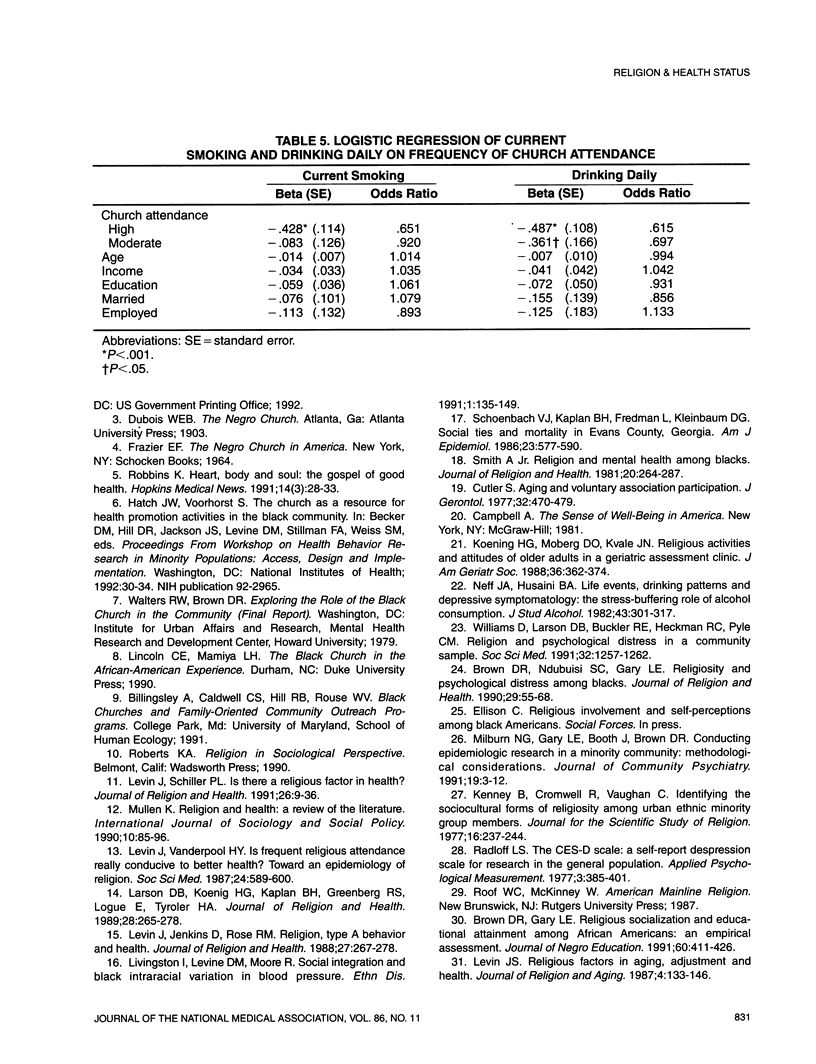
Previous studies document the importance of religious involvement in African-American communities. This study examines the extent to which religious involvement is associated with health status among African-American males. The data come from a community sample of 537 males residing in a major US urban area. Three indicators of religious involvement were used: denominational affiliation, frequency of church attendance, and overall religiosity. Measures of health status included a self-assessment of physical health, depressive symptoms, self-reported hypertension, cigarette smoking, and daily drinking of alcohol. The results show significant associations between selected indicators of religious involvement and measures of health status. Fewer depressive symptoms are associated with having a denominational affiliation, while no or low frequency of church attendance is associated with current smoking and daily drinking. Implications for health-related interventions with African-American males are discussed in light of these findings.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Cutler S. J. Aging and voluntary association participation. J Gerontol. 1977 Jul;32(4):470–479. doi: 10.1093/geronj/32.4.470. [DOI] [PubMed] [Google Scholar]
- Koenig H. G., Moberg D. O., Kvale J. N. Religious activities and attitudes of older adults in a geriatric assessment clinic. J Am Geriatr Soc. 1988 Apr;36(4):362–374. doi: 10.1111/j.1532-5415.1988.tb02365.x. [DOI] [PubMed] [Google Scholar]
- Levin J. S., Vanderpool H. Y. Is frequent religious attendance really conducive to better health? Toward an epidemiology of religion. Soc Sci Med. 1987;24(7):589–600. doi: 10.1016/0277-9536(87)90063-3. [DOI] [PubMed] [Google Scholar]
- Livingston I. L., Levine D. M., Moore R. D. Social integration and black intraracial variation in blood pressure. Ethn Dis. 1991 Spring;1(2):135–149. [PubMed] [Google Scholar]
- Neff J. A., Husaini B. A. Life events, drinking patterns and depressive symptomatology; the stress-buffering role of alcohol consumption. J Stud Alcohol. 1982 Mar;43(3):301–318. doi: 10.15288/jsa.1982.43.301. [DOI] [PubMed] [Google Scholar]
- Schoenbach V. J., Kaplan B. H., Fredman L., Kleinbaum D. G. Social ties and mortality in Evans County, Georgia. Am J Epidemiol. 1986 Apr;123(4):577–591. doi: 10.1093/oxfordjournals.aje.a114278. [DOI] [PubMed] [Google Scholar]
- Williams D. R., Larson D. B., Buckler R. E., Heckmann R. C., Pyle C. M. Religion and psychological distress in a community sample. Soc Sci Med. 1991;32(11):1257–1262. doi: 10.1016/0277-9536(91)90040-j. [DOI] [PubMed] [Google Scholar]