

Abstract
Submerged primary molars can be difficult to manage due to the developing dentition. Rarely in some severe cases, may the surgical interventions be required while ensuring the vital structures are protected. Therefore these cases require sophisticated imaging techniques in order to locate the vital structures.
In this case report, a 17 year old girl who had a retained and submerged deciduous molar which caused impaction of the second premolar and tipping of the first molar was presented. In addition, value of computed tomography (CT) for locating the vital anatomic structures was discussed.
In our case, CT has been supplied effective information about localization of the vital structures and amount of bone volume during the diagnosis and treatment planning period in addition to the routine dental radiographies.
Keywords: Submerged molars, Ankylosis, Impaction, Computed tomography
INTRODUCTION
The term “submerged” may be defined as teeth failing to erupt into a functional position and remaining under the occlusal plane. In the literature, “submerged” is often used synonymously with “ankylosed” and “infraoclusion”. Although the aetiology of submerged teeth is still unclear the following factors may affect a tooth to submerge.1–3
Ankylosis
Periodontal membrane disorders
Disturbed local metabolism
Local mechanical trauma
Local infection
Chemical or thermal irritation
Local failure of bone growth
Abnormal pressure of the tongue
Disturbance in normal hard tissue resorption and deposition
Systemic diseases (congenital syphilis, endocrine disorders etc.)
Heredity
Abnormal germ position and direction
Lack of space
The submerged primary teeth are complex clinical challenges and can be difficult to manage due to the developing dentition. There are four treatment options for impacted teeth. Observations (no treatment for a specific period); intervention (a brief period orthodontic therapy or the removal of teeth); relocation (repositioning of an impacted tooth surgically or orthodontically) and extraction (the removal of impacted tooth).4,5 Treatment may be complicated by the relationship of the teeth to the inferior alveolar nerve, which necessitates extensive bone removal and mental nerve transposition in the process of removing the submerged/impacted teeth. Early recognition and treatment of the submerge tooth might have prevented the need for such extensive surgery and morbidity at a later date.1,6
Rarely in some severe cases, may the surgical interventions be required while ensuring the vital structures such as inferior dental nerve are protected. Therefore these cases require sophisticated imaging techniques in order to locate the vital structures. CT has been suggested by the researchers in addition to the routine dental radiographies for these cases but very limited data is available in the literature.1,6–11
In this case report, a 17 year old girl who had a retained and submerged deciduous molar which caused impaction of the second premolar and tipping of the first molar was presented. In addition, value of computed tomography (CT) for locating the anatomic structure because of the potential trauma to the inferior alveolar nerve during surgical procedure was discussed.
CASE REPORT
Seventeen years-old Caucasian girl was presented to the clinics of the Department of Pedodontics, Faculty of Dentistry, Süleyman Demirel University for routine dental inspection. The medical history of the patient was insignificant. Clinical examination showed normal development of the dentition except for missing mandibular, right permanent second premolar and first molar. No sign of swelling, redness or discomfort was noted in the region. Only a small cusp of a tooth can be seen inside the gingiva (Figure 1).
Figure 1.

Intraoral view of the patient. Note that only a small cusp of right mandibular 1st molar can be seen.
Subsequent radiographic examination revealed an ankylosed second primary molar which caused impaction of the second premolar and tipping of the first molar. The second premolar which had a dilacerated root failed to erupt and was lying close to the lower border of the mandible (Figures 2 and 3). The tooth appeared to be in close proximity to the inferior alveolar canal as clearly seen in panoramic radiograph (Figure 2).
Figure 2.

Panoramic radiography of the patient.
Figure 3.
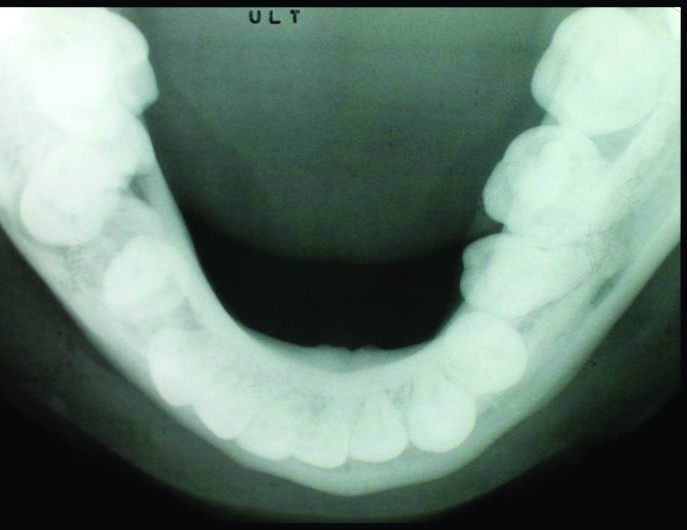
Occlusal radiography of the patient.
In order to assess the position of the inferior alveolar canal and the relationship between the canal and second premolar a coronal, CT was taken (Philips Tomoscan, Netherlands). CT scanning of the mandible consisted of 26 slices with a thickness of 3mm and 1mm slice gap. Relationship of inferior alveolar canal and impacted premolar can be observed in Figure 4. Furthermore the amount of bone volume of the involved section and symmetrical section (to compare the bone volume) calculated from the slices on post processing screen of the system. The bone volume was 8.46cm3 on the right side compared to 12.75cm3 on the opposing side which demonstrated that the structural weakness could arise, if molar, premolar and primary second molar were extracted. This could lead to long term problems such as potential pathological fracture of the mandible.
Figure 4.

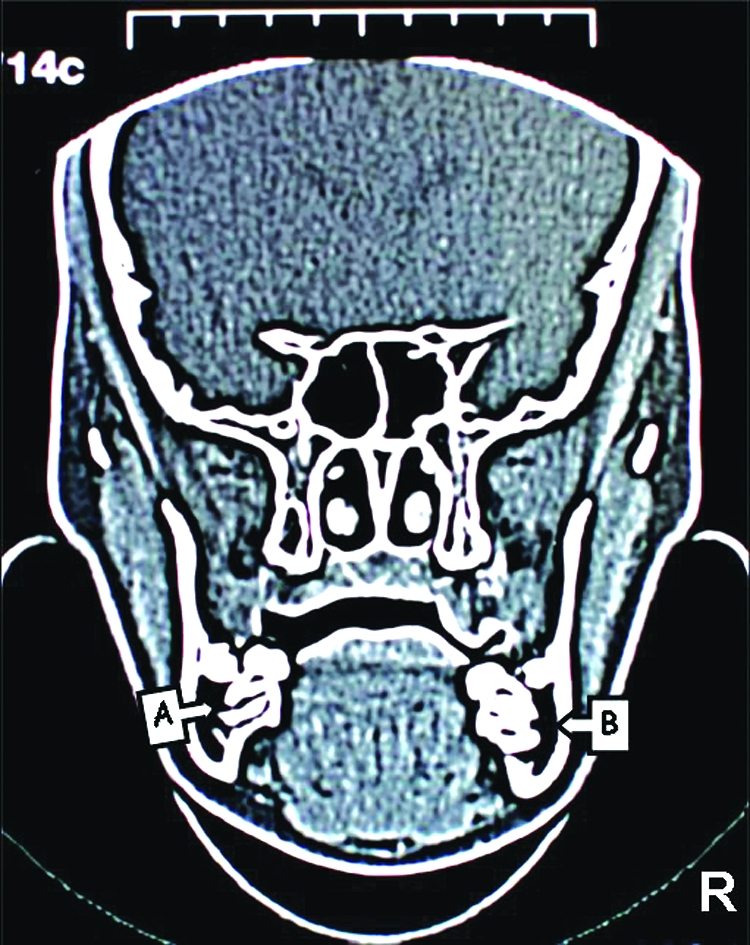
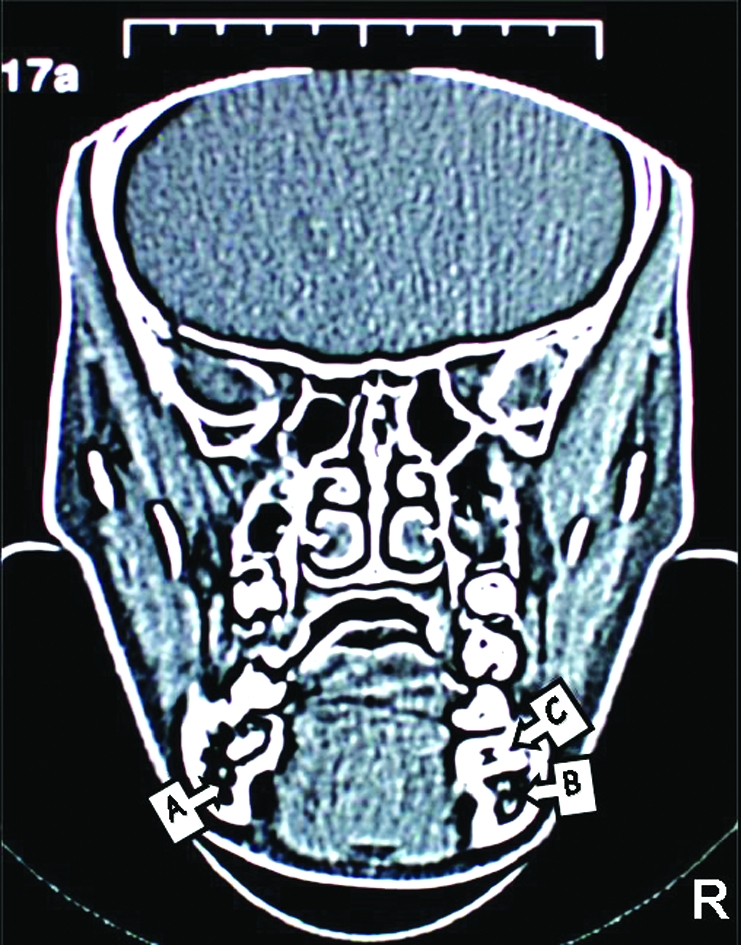
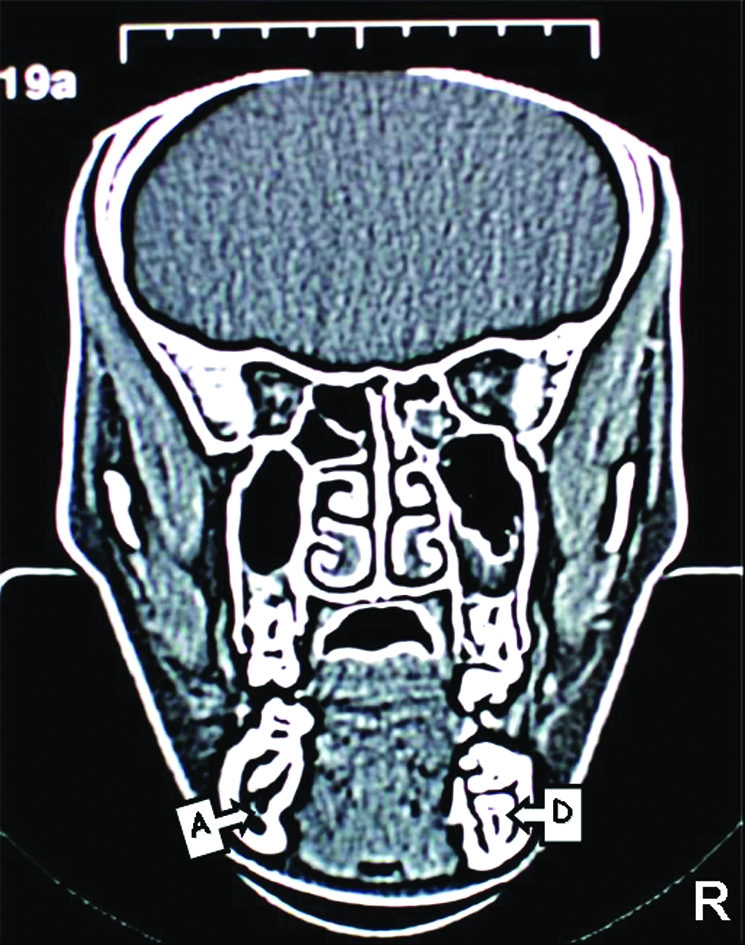
CT images of the patient. The position of right inferior dental canal can be seen clearly as a dark area but left inferior dental canal cannot be seen due to the impacted second premolar. (A; Right Mandibular Canal, B; Left Mandibular Canal, C; Tipped Right First Molar, D; Impacted Right Second
The patient and her parents have been informed about the possible complications (pathologic fracture of the mandible, paresthesia, hyperesthesia, anaesthesia, etc.) of removal of the involved teeth. Follow-up of the patient was agreed as the patient was unwilling to undergo surgical intervention.
DISCUSSION
Computed tomography (CT), is a medical imaging method employing tomography where digital geometry processing is used to generate a three-dimensional image of the internals of an object from a series of two-dimensional X-ray images taken around a single axis of rotation. CT produces a volume of data which can be manipulated, through a process in order to demonstrate various structures based on their ability to block the X-ray beam. In the head/neck/mouth area, CT scanning is used for surgical planning for craniofacial and dentofacial deformities and anomalies, evaluation of cysts and some tumors of the jaws/paranasal sinuses/nasal cavity/orbits, diagnosis of the causes of chronic sinusitis, and for planning of dental implant reconstruction. And also CT is useful in the setting of trauma for evaluating facial fractures. The advantages of CT are; (a) CT completely eliminates the superimposition of images of structures outside the area of interest. (b) Because of the inherent high-contrast resolution of CT, differences between tissues that differ in physical density by less than 1% can be distinguished. (c) Data from a single CT imaging procedure consisting of either multiple contiguous or one helical scan can be viewed as images in the axial, coronal, or sagittal planes, depending on the diagnostic task.12
CT scans do create low levels of ionizing radiation and radiation exposure from a CT scan is similar to, though higher than, that of a conventional x ray. The risk increases as numerous additional CT scans are performed. In some cases as in our case, a CT scan may still be done if the benefits greatly outweigh the risks.12,13
The exact physiological mechanisms involved in impaction have not been known yet. The degree of submergence and the age of the patient are important factors for consideration.4,14 Impaction of primary molars may cause several problems. If a submerging primary molar is retained too long, the second premolar may become displaced superiorly and the permanent first molar may migrate mesially as it erupts. However the curved root of the mandibular second premolar has formed after the impaction because the direction of the curvature was along the present outline of the mandible.1,4,6,15,16 The similar complications were observed in our case due to late diagnosis of the problem. The complexity of primary failure of eruption was illustrated by Wise et al17 which describes a case that was diagnosed and treated in the Orthodontic Clinics of University of Texas Health Science Centre, Houston. They stated that, despite comprehensive orthodontic treatment and third molar extractions, orthodontic force was not sufficient to bring the teeth into the desired plane of occlusion.
The spatial relationship between impacted and adjacent teeth has been examined using panoramic, occlusal, intraoral periapical radiographs and CT.1,6,8–11,18–23 CT has been shown to be superior to conventional radiographs in terms of visualization of the impacted teeth.1,10 The main rationale for using CT is to avoid injury to the inferior alveolar nerve which may occur during surgical procedure. Abrahms22 stated that CT procedures with multiplanar reconstructions provide a degree of precision but only bone or calcified structures are directly visible. Nasel et al7 proposed taking dental magnetic resonance images (MRI) for defining the location of the nerve.
In addition to the plain radiographies a CT was taken, due to the difficulties of locating the inferior alveolar neurovascular bundle in our case, which enabled us to determine the involved area more precisely for ensuring the vital structures are protected. The bone volume was calculated 8.46 cm3 on the right side and 12.75 cm3 on the opposing side from post processing screen of the system. This may imply extensive bone removal is required for extraction of the affected teeth which may predispose mandible to pathological fracture. Besides the possibility of eruption of second premolar was not considered in our case Premolar) as the tooth had curved root shape. Moreover, CT images revealed that mandibular nerve passes the impacted teeth in a very close proximity. Damage to the inferior alveolar nerve during the process of removal of the impacted teeth is highly likely. Previous reports documented that multiple impacted teeth were only observed with no surgical exposure or orthodontic traction due to the risk of extensive bone loss after surgical intervention.1,23
In conclusion; early treatment might have prevented these problems. Therefore, proper observation and early treatment for unerupted teeth are very important in patients with impacted teeth. In present case, in addition to the routine radiographies, CT provided effective information about localization of the inferior alveolar nerve and amount of bone volume during the diagnosis and treatment planning.
REFERENCES
- 1.Kitai N, Fujii Y, Murakami S, Takada K. Three-dimensional evaluation of rare case with multiple impacted teeth using CT. J Clin Pediatr Dent. 2003;27:117–121. doi: 10.17796/jcpd.27.2.kh4531177q42788m. [DOI] [PubMed] [Google Scholar]
- 2.Chen H-S, Lieu J-D. An unusual primary first molar impaction associated with a supernumerary tooth. Case report. Aust Dent J. 1993;38:277–279. doi: 10.1111/j.1834-7819.1993.tb05496.x. [DOI] [PubMed] [Google Scholar]
- 3.Douglass J, Tinanoff N. The etiology, prevalence, and sequelae of infrooclusion of primary molars. J Dent Child. 1991;58:481–483. [PubMed] [Google Scholar]
- 4.Suri L, Gagari E, Vastardis H. Delayed tooth eruption: Pathogenesis diagnosis and treatment. A literature review. Am J Orthod Dentofacial Orthop. 2004;126:432–445. doi: 10.1016/j.ajodo.2003.10.031. [DOI] [PubMed] [Google Scholar]
- 5.Frank CA. Treatment options for impacted teeth. JADA. 2000;131:623–632. doi: 10.14219/jada.archive.2000.0236. [DOI] [PubMed] [Google Scholar]
- 6.Cobourne MT, Brown JE, McDonald F. Analysis of the morbidity of submerged deciduous molars: The use of imaging techniques. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2002;93:98–102. doi: 10.1067/moe.2002.119245. [DOI] [PubMed] [Google Scholar]
- 7.Nasel CJO, Pretterlieber M, Gahleitner A, et al. Osteometry of the mandible performed using dental MR imaging. Am J Neuroradiol. 1999;20:1221–1227. [PMC free article] [PubMed] [Google Scholar]
- 8.Freisfeld M, Dahl IA, Jager A, Dresher D, Schuller H. X-ray diagnosis of impacted upper canines in panoramic radiographs and computed tomographs. J Orofac Orthop. 1999;60:177–184. doi: 10.1007/BF01365264. [DOI] [PubMed] [Google Scholar]
- 9.Preda L, La Fianza A, Di Maggio EM, et al. The use spiral computed tomography in the localization of impacted maxillary canines. Dentomaxillofac Radiol. 1997;26:236–241. doi: 10.1038/sj.dmfr.4600258. [DOI] [PubMed] [Google Scholar]
- 10.Krenmair G, Lenglinger FX, Traxler M. Imaging of unerupted and displaced teeth by cross-sectional CT scans. Int J Oral Maxillofac Surg. 1995;24:413–416. doi: 10.1016/s0901-5027(05)80470-9. [DOI] [PubMed] [Google Scholar]
- 11.Schmuth GP, Freisfeld M, Koster O, Schuller H. The application of computerized tomography (CT) in cases of impacted maxillary canines. Eur J Orthod. 1992;14:296–301. doi: 10.1093/ejo/14.4.296. [DOI] [PubMed] [Google Scholar]
- 12.Computed tomography. Wikipedia, The Free Encyclopedia. 2007 Sep 6; Retrieved 09:43, September 7,2007, from; http://en.wikipedia.org/w/index.php?title=Computed_tomography&oldid=156062111.
- 13.Frush DP, Donnelly LF, Rosen NS. Computed Tomography and Radiation Risks: What Pediatric Health Care Providers Should Know. Pediatrics. 2003;112:951–957. doi: 10.1542/peds.112.4.951. [DOI] [PubMed] [Google Scholar]
- 14.Schulze C. Developmental abnormalities of the teeth and jaws. In: Gorlin RJ, Goldman HM, editors. Thoma’s Oral Pathology. St. Louis: Mosby Company; 1970. pp. 152–53. [Google Scholar]
- 15.Ltyle JJ. Indications and contrindications for removal of the impacted tooth. Dent Clin North Am. 1979;23:333–336. [PubMed] [Google Scholar]
- 16.Altay N, Cengiz SB. Space-regaining treatment for a submerged primary molar: A case report. Int J Paediatr Dent. 2002;12:286–289. doi: 10.1046/j.1365-263x.2002.00374.x. [DOI] [PubMed] [Google Scholar]
- 17.Wise GE, Frazier-Bowers S, D’Souza RN. Cellular, molecular and genetic determinants of tooth eruption. Crit Rev Oral Biol Med. 2002;13:323–334. doi: 10.1177/154411130201300403. [DOI] [PubMed] [Google Scholar]
- 18.Aitasalo K, Lehtinen R, Oksala E. An orthopantomographic study of prevalence of impacted teeth. Int J Oral Surg. 1972;1:117–120. doi: 10.1016/s0300-9785(72)80001-2. [DOI] [PubMed] [Google Scholar]
- 19.Dachi SF, Howell FV. A survey 3874 routine full-mouth radiographs. A study of impacted teeth. Oral Surg. 1961;14:1165–1166. doi: 10.1016/0030-4220(61)90204-3. [DOI] [PubMed] [Google Scholar]
- 20.Sato K, Sugawara J, Mitani H, Kawamura H. Use of selectively colored stereolithography for diagnosis of impacted supernumerary teeth for a patient with cleidocranial dysplasia. Int J Adult Orthodon Orthognath Surg. 1998;13:163–167. [PubMed] [Google Scholar]
- 21.Kreiborg S, Jensen BL, Larsen P, Schleidt DT, Darvann T. Anomalies of craniofacial skeleton and teeth in cleidocranial dysplasia. J Craniofac Genet Dev Biol. 1999;19:75–79. [PubMed] [Google Scholar]
- 22.Abrahms JJ. Dental implants and multiplanar imaging of the jaw. In: Som PM, Curtin HD, editors. Head and neck imaging. 3. St Louis: Mosby; 1996. pp. 350–74. [Google Scholar]
- 23.Babu V, Nagesh KS, Diwakar NR. A rare case of hereditary multiple impacted normal and supernumerary teeth. J Clin Pediatr Dent. 1998;23:59–61. [PubMed] [Google Scholar]