

Abstract
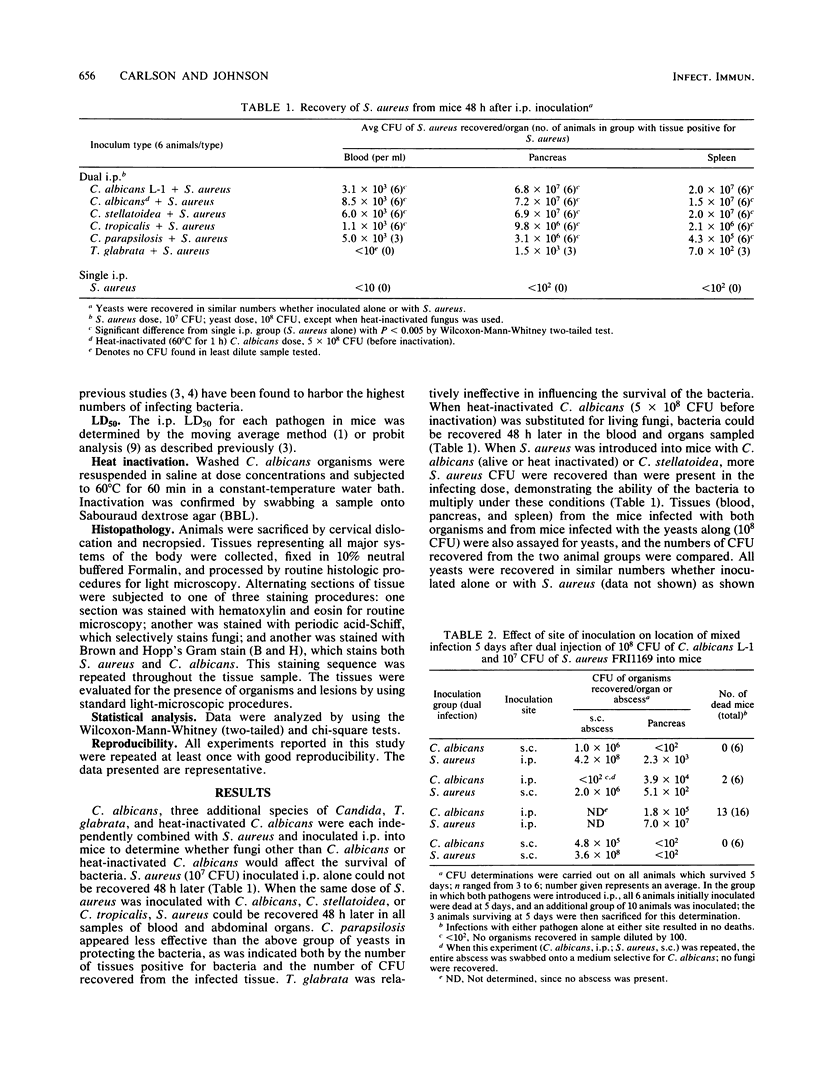
Candida albicans has been shown to stimulate infection in mice by a number of bacteria when both organisms are inoculated intraperitoneally (E. Carlson, Infect. Immun. 39:193-197, 1983). When subcutaneous and intraperitoneal inoculations were given with Staphylococcus aureus and C. albicans injected at opposite sites, mixed infection was established at the site of fungal inoculation but not at the site of the bacterial injection. Histopathologic evaluation of tissues for the presence of C. albicans and S. aureus after intraperitoneal inoculation of both showed fungal growth in the mesentery and omentum of the abdominal cavity. Cocci were numerous and always associated with the fungi, located within the fungal growth rather than at its periphery. It was concluded that this growth pattern in some way protected the bacteria and was the basis for the generalized fungal stimulation of the bacterial infections observed. In addition to C. albicans, Candida stellatoidea, Candida tropicalis, Candida parapsilosis, Torulopsis glabrata, and heat-inactivated C. albicans also demonstrated some ability to protect bacteria injected simultaneously, although C. parapsilosis and T. glabrata were less effective than the other yeasts in this respect.
Full text
PDF
Images in this article
Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- BENNETT B. M. Estimation of LD50 by moving averages. J Hyg (Lond) 1952 Jun;50(2):157–164. doi: 10.1017/s0022172400019513. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Berger M., Kirkpatrick C. H., Goldsmith P. K., Gallin J. I. IgE antibodies to Staphylococcus aureus and Candida albicans in patients with the syndrome of hyperimmunoglobulin E and recurrent infections. J Immunol. 1980 Dec;125(6):2437–2443. [PubMed] [Google Scholar]
- Carlson E. Effect of strain of Staphylococcus aureus on synergism with Candida albicans resulting in mouse mortality and morbidity. Infect Immun. 1983 Oct;42(1):285–292. doi: 10.1128/iai.42.1.285-292.1983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson E. Enhancement by Candida albicans of Staphylococcus aureus, Serratia marcescens, and Streptococcus faecalis in the establishment of infection in mice. Infect Immun. 1983 Jan;39(1):193–197. doi: 10.1128/iai.39.1.193-197.1983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carlson E. Synergistic effect of Candida albicans and Staphylococcus aureus on mouse mortality. Infect Immun. 1982 Dec;38(3):921–924. doi: 10.1128/iai.38.3.921-924.1982. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Chappler R. R., Maibach H. I., Conant M. A. Mucocutaneous candidiasis or mucocutaneous microbiosis? JAMA. 1978 Jan 30;239(5):428–429. [PubMed] [Google Scholar]
- DOBIAS B. SPECIFIC AND NONSPECIFIC IMMUNITY IN CANDIDA INFECTIONS. EXPERIMENTAL STUDIES OF THE ROLE OF CANDIDA CELL CONSTITUENTS AND REVIEW OF LITERATURE. Acta Med Scand. 1964;176:SUPPL 421–421:1+. [PubMed] [Google Scholar]
- JOSSE J. W., ZACKS S. I. Thymoma and pancytopenia; report of a case and review of the literature. N Engl J Med. 1958 Jul 17;259(3):113–117. doi: 10.1056/NEJM195807172590303. [DOI] [PubMed] [Google Scholar]
- KEENEY E. L. Candida asthma. Ann Intern Med. 1951 Jan;34(1):223–226. doi: 10.7326/0003-4819-34-1-223. [DOI] [PubMed] [Google Scholar]
- Klotz S. A., Drutz D. J., Harrison J. L., Huppert M. Adherence and penetration of vascular endothelium by Candida yeasts. Infect Immun. 1983 Oct;42(1):374–384. doi: 10.1128/iai.42.1.374-384.1983. [DOI] [PMC free article] [PubMed] [Google Scholar]
- MANKIEWICZ E., LIVAK M. Effect of Candida albicans on the evolution of experimental tuberculosis. Nature. 1960 Jul 16;187:250–251. doi: 10.1038/187250a0. [DOI] [PubMed] [Google Scholar]
- MARTIN C. M., GORDON R. S., MCCULLOUGH N. B. Acquired hypogammaglobulinemia in an adult; report of a case, with clinical and experimental studies. N Engl J Med. 1956 Mar 8;254(10):449–456. doi: 10.1056/NEJM195603082541002. [DOI] [PubMed] [Google Scholar]
- Morris C. A. Influence of oral contraceptives on the presence and persistence of Candida albicans and beta-haemolytic streptococci in the vagina. J Clin Pathol. 1969 Jul;22(4):488–491. doi: 10.1136/jcp.22.4.488. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Palestine R. F., Su W. P., Liesegang T. J. Late-onset chronic mucocutaneous and ocular candidiasis and malignant thymoma. Arch Dermatol. 1983 Jul;119(7):580–586. [PubMed] [Google Scholar]
- Staib F., Geier R. Proteolysis products of Candida albicans as a substratum for growth of staphylococcus aureus--a preliminary report. Zentralbl Bakteriol Orig A. 1971 Nov;218(3):374–375. [PubMed] [Google Scholar]
- Staib F., Grosse G., Mishra S. K. Staphylococcus aureus and Candida albicans infection (animal experiments). Zentralbl Bakteriol Orig A. 1976 May;234(4):450–461. [PubMed] [Google Scholar]
- Trier J. S., Bjorkman D. J. Esophageal, gastric, and intestinal candidiasis. Am J Med. 1984 Oct 30;77(4D):39–43. [PubMed] [Google Scholar]
- Wachs G. N. Monilial granuloma (Candida). Arch Dermatol. 1970 Jan;101(1):118–119. [PubMed] [Google Scholar]