

Abstract
Context:
In India, refractive errors are a major cause of treatable blindness. Population surveys in southern India have shown prevalence of high myopia to be 4.32-4.54%. Photodynamic therapy (PDT) for choroidal neovascularization (CNV) caused by pathologic myopia is beneficial.
Aims:
To report the 24 months outcome of PDT with verteporfin for subfoveal CNV caused by pathologic myopia in Indian eyes
Settings and Design:
Prospective case series
Materials and Methods:
Review of prospectively collected data of Indian patients with pathologic myopia and subfoveal CNV treated with verteporfin therapy between 2001 and 2005 using standard regimen for PDT.
Statistical Analysis Used:
Wilcoxon signed rank test was used to see the difference in the mean letter acuity at intervals compared to baseline. Kaplan Meier Survival analysis was done to estimate the success rate of verteporfin therapy for CNV caused by pathologic myopia.
Results:
Fifteen patients (15 eyes) treated with standard fluence PDT and who had completed 24 months follow-up were analyzed. The mean spherical equivalent was -13.36 ± 5.88 diopter. Five out of 15 eyes in six months, three out of 15 eyes at 12 months and four eyes out of 15 at 24 months had improved vision by > 10 letters. The mean number of treatment session was 2.2 in two years.
Conclusions:
PDT with verteporfin for subfoveal CNV caused by pathologic myopia in Indian eyes is effective.
Keywords: Choroidal neovascularization, pathologic myopia, photodynamic therapy, subfoveal, verteporfin
Choroidal neovascularization (CNV) with chorioretinal atrophy is the most common cause of poor vision in patients with pathologic myopia.1 In India, refractive errors are a major cause of treatable blindness. Population surveys in southern India have shown prevalence of high myopia to be 4.32-4.54%.2-4 Pathologic myopia is also common in Asian countries like Singapore (prevalence of 9%5). This is high compared to a prevalence of 2% in the United States.6
Pathologic myopia is associated with progressive stretching and thinning of the posterior pole and choroid with loss of choriocapillaries. The elongation of the globe causes vascular alterations, breaks in Bruch′s membrane (lacquer cracks) with increased risk of CNV.7 Photodynamic therapy (PDT) uses photosensitive verteporfin which selectively collects in proliferating endothelial cells within the target CNV and on activation, cytotoxic reactive oxygen intermediates damage the cellular proteins and cause microvascular thrombosis without a direct thermal effect.8
The natural course of the disease without treatment is unfortunately poor but better visual outcomes have been reported with PDT, compared to laser and submacular surgery.9-17 The VIP Study Group, a randomized controlled trial for treatment of pathological myopia using verteporfin recommended PDT.18 Complications of treatment19 and the cost, particularly in less developed countries should be borne in mind when treating these patients. The alternatives to PDT such as in anti-vascular endothelial growth factor (anti-VEGF) therapy20,21 and combination treatments22 are also promising.
We have reported earlier the one-year data in myopic patients.23 The present study reports on the outcome after a two-year follow-up of patients treated with verteporfin PDT for CNV caused by pathologic myopia in a tertiary care hospital in south India.
Materials and Methods
We reviewed the prospectively collected data of patients receiving PDT with verteporfin for subfoveal CNV secondary to pathologic myopia during the period from May 2001 to June 2005. All patients underwent ocular examination in each visit which included:
ETDRS letter acuity (best corrected) at 4 meters
Dilated slit-lamp biomicroscopy
Dilated fundus examination (+ 90 D and + 20 D)
Color fundus photograph
Fundus fluorescein angiography (FFA)
The inclusion and exclusion criteria and method of treatment were similar as published earlier.23 Briefly, the inclusion criteria were best corrected visual acuity ≥ 20/200; myopia ≥ 6 diopter; fundus changes characteristic of chorioretinal atrophy, lacquer cracks and posterior staphyloma and age ≥ 18 years. The exclusion criteria were history of previous macular laser, intraocular surgery in the last three months and other ocular disorders possibly causing CNV (viz. Angioid streaks and age-related macular degeneration).
Patients who completed at least 24 months follow-up were included in the study. The follow-up schedule was every three months. All the tests were repeated on each follow-up visit.
The primary outcome measure was visual outcome and secondary outcome was the number of retreatments. Improvement was defined as a gain of th > 10 ETDRS letters, deterioration as a loss of > 10 ETDRS letters and stabilization as < 10 letters gain or loss. Success was defined as improvement or stabilization of vision.
Wilcoxon signed rank test was used to see the difference in the mean letter acuity at intervals compared to the baseline. Kaplan Meier Survival analysis was done to estimate the success rate of verteporfin therapy for CNV caused by pathologic myopia.
Photodynamic therapy with verteporfin for CNV caused by pathologic myopia and the study protocol had been approved by the ethics committee of the institute in 2001.
Results
The age range of these 15 patients (eight male and seven female) was from 28 to 57 years (41 + 10.02). Right eye was affected in eight patients. The mean spherical equivalent was -13.46 + 5.88 diopter (range: -6.0 to -25.0 diopter). All patients completed at least 24 months follow-up.
At the baseline, four out of 15 eyes had visual acuity (VA) ≥ 20/40, six eyes out of 15 had between 20/50 and 20/80; and five eyes out of 15 had ≥ 20/200. At 24 months, four eyes out of 15 each had VA ≥ 20/40 and between 20/50 and 20/80 respectively, and seven eyes out of 15 had ≥ 20/200 [Figure 1].
Figure 1.
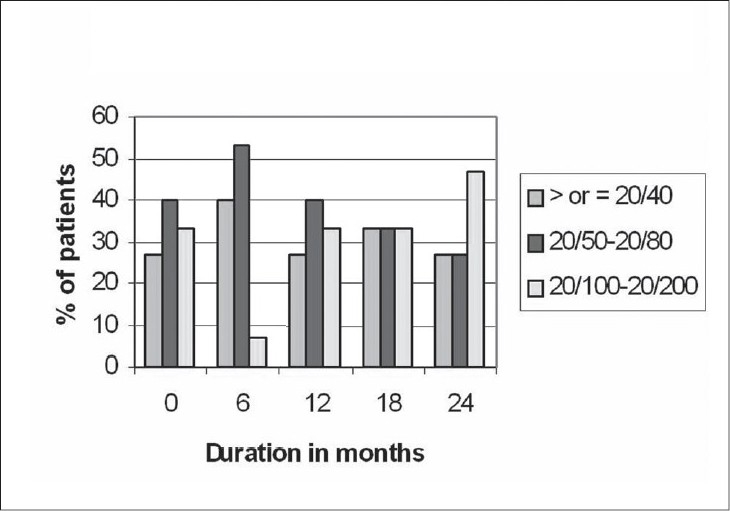
Snellen visual acuity at Month 0 (Baseline, Pre PDT) and every six months till the 24th month
[Figure 2] shows the trend of mean letter acuity over a period of 24 months. At six months, there was significant improvement in mean letter acuity (33.8 + 12.4) from baseline (27.4 + 15.2) (P=0.02), but there was no difference at 12 (P=0.3), 18 (P=0.9) and 24 months (P=0.95). Compared to improvement in letter acuity in the first six months, there was reduction in mean letter acuity at 18 (28.1 + 14.8) (P=0.02) and 24 months (27.3 + 14.3) (P=0.05).
Figure 2.
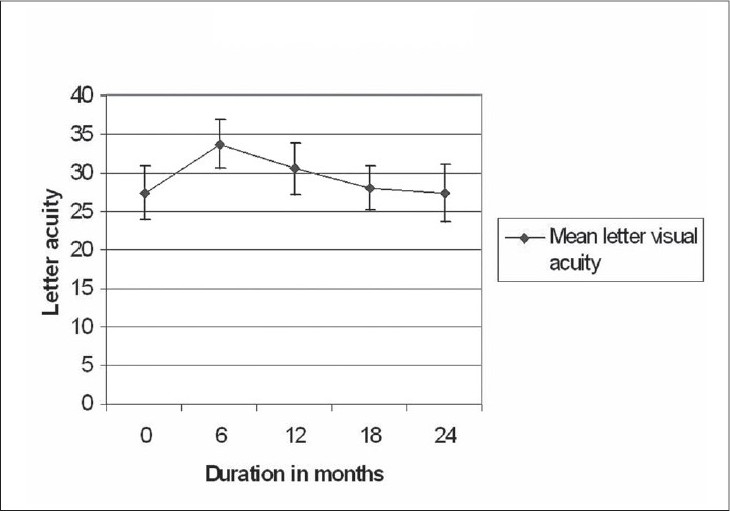
Trend of mean letter acuity over a period of 24 months
Five out of 15 eyes at six months, three out of 15 eyes at 12 and 18 months, and four out of 15 at 24 months follow-up gained ≥ 10 letters [Figure 3].
Figure 3.
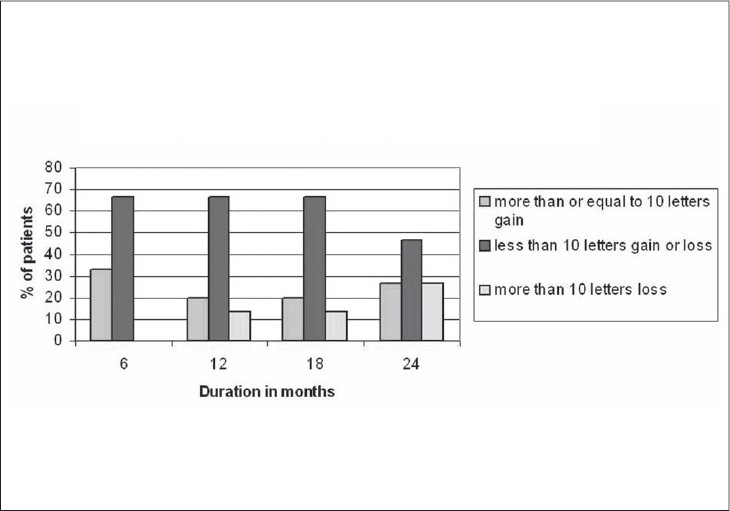
Percentage of eyes that gained or lost vision at the follow-up visits
Survival analysis showed a success rate of 100% at six months, 93.3% (SE=0.064) at 12 months and 73.3% (SE=0.114) at 24 months.
The mean number of PDT treatment session was 2.2 (Range: 1- 5, Mode: 2). It was 2.06 (range: 1-5) in the first year and 0.13 (range: 0 -2) in the second year. Retinal pigment epithelial collateral change was seen in five out of 15 eyes.
Discussion
Presence of subfoveal CNV is one of the major causes of decreased vision in pathologic myopia (5-10%) besides progression of myopic macular chorioretinal atrophy.23,24 Moreover, high myopia is common in the Asian population24,25 compared to the Caucasian population (2-4%).25 The VIP Study has shown the beneficial effect of PDT and demonstrated that verteporfin therapy improves the chance of stabilization (< 8 letters loss) or causes improvement of vision compared to either natural history or placebo at least at 24 months follow up.18
The present study has demonstrated that verteporfin therapy is beneficial in stabilization of vision at 24 months. Significant improvement of vision was seen at six months (P=0.02) from baseline but did not maintain till 24 months. Actually, a drop in visual acuity (VA) was seen after 12 months and the VA at 24 months was not significantly different from the baseline visual acuity. We have reported initial improvement of vision with verteporfin therapy in the first six months in neovascular age- related macular degeneration.26 Even though the mean visual acuity change at 24 months was not statistically significant, at least four out of 15 of eyes gained ≥ 10 letters and there was a success rate of 73.3% (S.E: 0.114) at the end of follow-up. The 24 months′ experience of a case series of 22 Asian Chinese eyes have also shown no statistical difference in mean best corrected visual acuity (P=0.5).11 Initial improvement of vision noted in the first three months did not sustain for two years. We had shown in our earlier report23 that eight of nine eyes had unchanged vision at the end of one year following PDT. The current report suggests that the trend is nearly similar and PDT stabilizes the vision in high myopic eyes with CNV.
In our study cohort, the mean number of treatment was 2.2 in 24 months and interestingly, 93.6% of the treatment (2.06) was required in the first year itself. This was almost similar to the report by Lam et al.,11 (mean treatment rate of 2.3) in 24 months. This may suggest that chances of recurrence of CNV needing treatment or requiring retreatment in the second year are minimal. The VIP study showed a higher mean treatment rate of 5.1 at 24 months in Caucasian eyes.18
Though PDT is helpful in stabilizing vision in pathologic myopia with CNV, currently there are other alternatives and options which were not available at the time of the study duration. While the anti-VEGF therapy has largely taken over as the primary treatment mode in subfoveal CNV, the role of PDT is still considered and tried the world over. Since the mechanism of actions is different, there could be a role for both PDT and anti-VEGF therapy in the future. Our study shows a limited role of PDT, and possibly today, combined with the anti-VEGF therapy could be more beneficial than PDT alone as shown in past.27
Thus, this study shows that verteporfin therapy in subfoveal CNV caused by pathologic myopia is equally effective in Indian eyes and compares well with the study in Asian Chinese eyes from Hong Kong. It may be possible that some ethnic variation may exist even amongst the Asian population. The ethnic variation between Asian and Caucasian population is not clearly known. This disparity may be due to more pigments in retinal pigmented epithelium providing a possible protective effect.11
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Avila MP, Weiter JJ, Jalkh AE, Trempe CL, Pruett RC, Schepens CL. Natural history of choroidal neovascularisation in degenerative myopia. Ophthalmology. 1984;91:1573–8. doi: 10.1016/s0161-6420(84)34116-1. [DOI] [PubMed] [Google Scholar]
- 2.Thulasiraj RD, Nirmalan PK, Ramakrishnan R, Krishnadas R, Manemakelai TK, Baburajan NP, et al. Blindness and vision impairment in a rural South Indian population: The Aravind Comprehensive Survey. Ophthalmology. 2003;110:1491–8. doi: 10.1016/S0161-6420(03)00565-7. [DOI] [PubMed] [Google Scholar]
- 3.Dandona R, Dandona L, Srinivas M, Giridhar P, McCarty CA, Rao GN. Population based assessment of refractive error in India: the Andhra Pradesh Eye Disease Study. Clin Exp Ophthalmol. 2002;30:84–93. doi: 10.1046/j.1442-6404.2002.00492.x. [DOI] [PubMed] [Google Scholar]
- 4.Raju P, Ramesh SV, Arvind H, George R, Baskaran M, Paul PG, et al. Prevalence of refractive errors in a rural southern Indian population. Invest Ophthalmol Vis Sci. 2004;45:4268–72. doi: 10.1167/iovs.04-0221. [DOI] [PubMed] [Google Scholar]
- 5.Wong TY, Foster PJ, Hee J, Nq TP, Tielsch JM, Chew SJ, et al. Prevalence and risk factors for refractive errors in adult Chinese in Singapore. Invest Ophthalmol Vis Sci. 2000;41:2486–94. [PubMed] [Google Scholar]
- 6.Sperduto RD, Seigel D, Roberts J, Rowland M. Prevalence of myopia in the United States. Arch Ophthalmol. 1983;101:405–7. doi: 10.1001/archopht.1983.01040010405011. [DOI] [PubMed] [Google Scholar]
- 7.Curtin B. The myopias: Basic science and clinical management. Philadelphia: Harper and Row; 1985. pp. 7–10. [Google Scholar]
- 8.Zhou C. Mechanisms of tumour necrosis induced by photodynamic therapy. J Photochem Photobiol B. 1989;3:299–318. doi: 10.1016/1011-1344(89)80035-1. [DOI] [PubMed] [Google Scholar]
- 9.Cohen SY, Bulik A, Dubois L, Quentel G. Photodynamic therapy for juxtafoveal choroidal neovascularisation in myopic eyes. Am J Ophthalmol. 2003;136:371–4. doi: 10.1016/s0002-9394(03)00201-0. [DOI] [PubMed] [Google Scholar]
- 10.Bandello F, Lanzetta P, Battaglia Parodi M, Ranam Poginuz D, Saviano S, Ravalico G. Photodynamic therapy of subfoveal recurrences after laser photocoagulation of extrafoveal choroidal neovascularization in pathologic myopia. Graefes Arch Clin Exp Ophthalmol. 2003;241:567–70. doi: 10.1007/s00417-003-0686-9. [DOI] [PubMed] [Google Scholar]
- 11.Lams DS, Chan WM, Liu DT, Fan DS, Lai WW, Chang KK. Photodynamic therapy with verteporfin for subfoveal choroidal neovascularisation of pathologic myopia in Chinese eyes: A prospective series of 1 and 2 year follow up. Br J Ophthalmol. 2004;88:1315–9. doi: 10.1136/bjo.2004.041624. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 12.Varano M, Parisi V, Tedeschi M, Sciamama M, Gallinaros G, Capaldo N, et al. Macular function after photodynamic therapy in myopic maculopathy: Psychophysical and electrophysiological evaluation. Invest Ophthalmol Vis Sci. 2005;46:1453–62. doi: 10.1167/iovs.04-0903. [DOI] [PubMed] [Google Scholar]
- 13.Tholen AM, Bernaosconi PP, Fierz AB, Messmer EP. Reading ability after photodynamic therapy for age related macular degeneration and high myopia. Ophthalmologie. 2003;100:28–32. doi: 10.1007/s00347-002-0681-2. [DOI] [PubMed] [Google Scholar]
- 14.Ruiz-Moreno JM, Montero JA. Visual acuity results after argon green laser photocoagulation of juxtafoveal choroidal neovascularization in highly myopic eyes: Long term results. Eur J Ophthalmol. 2002;12:117–22. doi: 10.1177/112067210201200207. [DOI] [PubMed] [Google Scholar]
- 15.Ruiz-Moreno JM, de la Vega C. Surgical removal of subfoveal choroidal neovascularisation in highly myopic patients. Br J Ophthalmol. 2001;85:1041–3. doi: 10.1136/bjo.85.9.1041. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Tabandeh H, Flynn HW, Jr, Scott IU, Lewis ML, Rosenfeld PJ, Rodriguez F, et al. Visual acuity outcomes of patients 50 years of age and older with high myopia and untreated choroidal neovascularisation. Ophthalmology. 1999;106:2063–7. doi: 10.1016/S0161-6420(99)90484-0. [DOI] [PubMed] [Google Scholar]
- 17.Ohno-Matsui K, Yoshida T. Myopic choroidal neovascularisation: Natural course and treatment. Curr Opin Ophthalmol. 2004;15:197–202. doi: 10.1097/01.icu.0000120709.35941.e9. [DOI] [PubMed] [Google Scholar]
- 18.Blinder KJ, Blumenkranz MS, Bressler NM, Bressler SB, Donato G, Lewis H, et al. Verteporfin therapy of subfoveal choroidal neovascularisation in pathologic myopia: 2 -year results of a randomized clinical trial-VIP report no. 3. Ophthalmology. 2003;110:667–73. doi: 10.1016/s0161-6420(02)01998-x. [DOI] [PubMed] [Google Scholar]
- 19.Ruiz-Moreno , Montero JO. Subretinal fibrosis after photodynamic therapy of subfoveal choroidal neovascular membrane in highly myopic eyes. Br J Ophthalmol. 2003;87:856–9. doi: 10.1136/bjo.87.7.856. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 20.Sakaquchi H, Ikuno Y, Gwui F, Kamei M, Sawa M, Tsujikawa M, et al. Intravitreal injection of Bevacizumab for choroidal neovascularisation caused by pathologic myopia. Br J Ophthalmol. 2006 Aug 16; doi: 10.1136/bjo.2006.099887. (Epub ahead of print) [DOI] [PMC free article] [PubMed] [Google Scholar]
- 21.Yamamoto I, Rogers AH, Reichel E, Yates PA, Duker JS. Intravitreal bevacizumab (Avastin) as treatment for subfoveal choroidal neovascularization secondary to pathologic myopia. Br J Ophthalmol. 2007;91:157–60. doi: 10.1136/bjo.2006.096776. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Marticorena J, Gomez-Ulla F, Fernandez M, Pazos B, Rodriguez-cid MJ, Sanchez-Salorio M. Combined photodynamic therapy and intravitreal triamcinolone acetonide for the treatment of myopic subfoveal choroidal neovascularisation. Am J Ophthalmol. 2006;142:335–7. doi: 10.1016/j.ajo.2006.03.003. [DOI] [PubMed] [Google Scholar]
- 23.Hussain N, Das T, Vashist U, Sumashri K. Verteporfin therapy for myopic choroidal neovascularisation in Indian eyes (one year results) Indian J Ophthalmol. 2004;52:227–31. [PubMed] [Google Scholar]
- 24.Yoshida T, Ohno-Matsui K, Yasuzumi K, Kojima A, Shimada N, Futagami S, et al. Myopic choroidal neovascularisation: Ten year follow up. Ophthalmology. 2003;110:1297–305. doi: 10.1016/S0161-6420(03)00461-5. [DOI] [PubMed] [Google Scholar]
- 25.Chan WM, Ohji M, Lai TY, Liu DT, Tano Y, Lam DS. Choroidal neovascularisation in pathological myopia: An update in management. Br J Ophthalmol. 2005;89:1522–8. doi: 10.1136/bjo.2005.074716. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 26.Hussain N, Das T, Khanna R, Sumasri K, Mohan Ram LS. Verteporfin therapy for Neovascular Age related macular degeneration in Indian eyes. Jpn J Ophthalmol. 2006;50:524–8. doi: 10.1007/s10384-006-0367-4. [DOI] [PubMed] [Google Scholar]
- 27.Hussain N, Das T, Rawal H, Kallukuri SB, Mohan Ram LS, Khanna R. Combination therapy of intravitreal triamcinolone and photodynamic therapy for neovascular age related macular degeneration. Indian J Ophthalmol. 2006;54:247–50. doi: 10.4103/0301-4738.27949. [DOI] [PubMed] [Google Scholar]