

Abstract
Background:
The northeastern region (NER) of India is geographically isolated and ethno-culturally different from the rest of the country. There is lacuna regarding the data on causes of blindness and severe visual impairment in children from this region.
Aim:
To determine the causes of severe visual impairment and blindness amongst children from schools for the blind in the four states of NER of India.
Design and Setting:
Survey of children attending special education schools for the blind in the NER.
Materials and Methods:
Blind and severely visually impaired children (best corrected visual acuity <20/200 in the better eye, aged up to 16 years) underwent visual acuity estimation, external ocular examination, retinoscopy and fundoscopy. Refraction and low vision workup was done where indicated. World Health Organization′s reporting form was used to code anatomical and etiological causes of visual loss.
Statistical Analysis:
Microsoft Excel Windows software with SPSS.
Results:
A total of 376 students were examined of whom 258 fulfilled the eligibility criteria. The major anatomical causes of visual loss amongst the 258 were congenital anomalies (anophthalmos, microphthalmos) 93 (36.1%); corneal conditions (scarring, vitamin A deficiency) 94 (36.7%); cataract or aphakia 28 (10.9%), retinal disorders 15 (5.8%) and optic atrophy 14 (5.3%). Nearly half of the children were blind from conditions which were either preventable or treatable (48.5%).
Conclusion:
Nearly half the childhood blindness in the NER states of India is avoidable and Vitamin A deficiency forms an important component unlike other Indian states. More research and multisectorial effort is needed to tackle congenital anomalies.
Keywords: Childhood blindness, corneal opacity, congenital anomalies, visual impairment
India has an estimated 320,000 blind children, more than any other country in the world.1 Even though this represents a small fraction of the total blindness, the control of blindness in children is one of the priority areas of the World Health Organization′s (WHO) ″Vision 2020: the right to sight″ program. This is a global initiative, which was launched by WHO in 1999 to eliminate avoidable blindness worldwide by the year 2020.2
Although blindness in children is relatively uncommon, this age group is also considered a priority as severe visual loss in children can affect their development, mobility, education, and employment opportunities. This has far- reaching implications on their quality of life and their affected families. In terms of the ′blind person years′ they form the maximum burden of blindness on the community, next only to cataract, the commonest cause of avoidable blindness.3 The prevalence of blindness in children ranges from approximately 0.3/1000 children in affluent regions to 1.5/1000 in the poorest communities. Globally there are estimated to be 1.4 million blind children, almost three-quarters of them live in developing countries.3
The population of India in 2001 was estimated to be 1.03 billion, approximately 420 million were children under 16 years of age (40.8%).4 India is a land of contrasts and there are huge differences amongst the 30 states that form the Union of India. The seven northeastern states are geographically isolated from the rest of the country and are different culturally, socially and economically. The people are predominantly of mongoloid race unlike the majority of Indians. Even though the central and state governments have taken efforts to develop these states, they remain at different stages of development. The topography is rugged and communication is difficult as compared to other states. Hence the childhood blindness pattern in these states may be different from that observed in other parts of the country.
Information on the major causes of blindness in children is required to design effective prevention of blindness programs.5 Reliable, population-based data on the causes of blindness in children are difficult to obtain in developing countries as registers of the blind do not exist, and very large sample sizes would be required for formal cross-sectional surveys. Alternative sources include the use of key informants, and examination of children identified as blind in community-based rehabilitation programs. Examination of children in special institution has increasingly been used to provide data on the causes of blindness in children, but possible sources of bias need to be borne in mind.
The standard reporting form for recording the causes of visual loss in children, developed by the International Centre for Eye Health, London for the WHO prevention of blindness program6 has been used in various states of India.7,8 But the northeastern states have not been covered so far.
The primary objectives of the present survey were to determine the causes of blindness in children in schools for the blind in northeast India, to assess the profile of causes of blindness by analyzing the data by age group, and to compare the findings of this study with data obtained from other states of India. The survey includes four out of seven states of Northeast India viz. Assam, Manipur, Mizoram, and Tripura. Arunachal Pradesh and Nagaland have no school for blind children. Meghalaya has two schools for the blind but were not included in the survey due to some limitations.
Materials and Methods
The schools for blind children in the northeastern states were identified with the help of blindness control societies of each state. The required permission for screening of the children was obtained from the principal/headmaster of each school. The concerned authorities of each school were briefed about the aims and objectives of the study. The school authorities were requested to inform the parents of the children at the time of screening.
UNICEF defines childhood as 0 to 16 years inclusive. The WHO defines blindness as a corrected visual acuity in the better eye of less than 10/200, and severe visual impairment as corrected visual acuity in the better eye of less than 20/200 but equal to, or better than 10/200. The Indian definition has a best corrected visual acuity <20/200 in the better eye as blind.
An ophthalmologist and an optometrist from Sri Sankaradeva Nethralaya (SSN) in Guwahati, the region′s largest city, examined the children in the respective school premises. A local ophthalmologist was also involved in the process to provide assistance in order to overcome the language barrier. The relevant information was collected from the class teachers and parents (whenever possible). The study included all the students of the blind school irrespective of age. Brief demographic details, medical and family history of each child were recorded. The ophthalmologists from SSN carried out a detailed eye examination of each child.
Visual acuity was assessed in each eye using a Snellen tumbling ″E″ visual acuity test chart. The child who did not cooperate with the ″E″ chart, were assessed for the ability to fix and follow light. Near vision were assessed using figures equivalent to N. The visual status of children was recorded using WHO categories of visual impairment before and after refraction.
To categorize a child under low visual category, simple tests of functional vision were used. They were, the ability to navigate around two chairs set two meters apart unaided with a visual acuity of <20/60 to light perception; to recognize faces at a distance of three meters, and to recognize the shape of three two-cm symbols at any near distance. The children who failed to cooperate with these tests due to additional handicaps were judged on their visual behavior.
Refraction and low vision aid assessment were performed in all children who were able to perform the tests of functional vision by an optometrist.
Anterior segments of the eye were examined using a light and loupe magnifier and/or with a handheld slit-lamp. The posterior segment was examined using direct and indirect ophthalmoscope after dilatation of pupil.
The WHO prevention of blindness program′s (WHO/PBL) eye examination record for children with blindness and low vision was used to categorize the causes of blindness and to record the findings, using the definitions in the coding instructions.6
The anatomical classification of causes of visual loss defined that part of the eye which had been damaged leading to visual loss (such as cornea, lens, retina, optic nerve, whole globe). Where two or more anatomical sites were involved the major site was selected, or where two sites contributed equally, the most treatable condition was selected. The etiological classification was divided into five categories depending on the time of onset of the condition leading to blindness (hereditary, intrauterine, perinatal, childhood and unknown). For each child, the need of optical, medical or surgical interventions was recorded and the visual prognosis was assessed. Children requiring further investigations and treatment procedures were referred to SSN or to contact the accompanying ophthalmologist for further management. The data were entered into a database and analyzed using SPSS for Windows.
Results
A total of 376 students were examined in 12 schools for the blind in the northeastern region (NER). The highest numbers of children examined were from the state of Assam with 174 (67.4 %) followed by Manipur 36 (14.0 %), Tripura 25 (9.7%), and Mizoram 23 (8.9 %). The list of the schools visited is given in Appendix 1. Twenty out of 376 (5.3%) students had undergone cataract surgery, while five (1.3%) had undergone glaucoma surgery and penetrating keratoplasties had been done in five (1.3%) children. Family history was found to be present in 38 out of 376 (10.1%) cases and a history of consanguineous marriage of the parents was recorded in 24 out of 376 (6.4%) of cases. Additional disability was found in 19 (5%) children only.
Of the 376, 260 were children less than 16 years of age. Two (0.8%) of the 260 had visual acuity of 20/200 to 20/80, 18 out of 260 (6.9 %) were severely visually impaired (SVI) and 240 out of 260 (92.3 %) were blind, having visual acuity <10/200 in the better eye. Table 1 shows the children examined from each state. Data on causes were analyzed for the 258 children who were severely visually impaired or blind after refraction (<20/200 in the better eye), blind by Indian standards.
Table 1.
State and gender-wise distribution of severely visually impaired and blind children in northeastern states of India
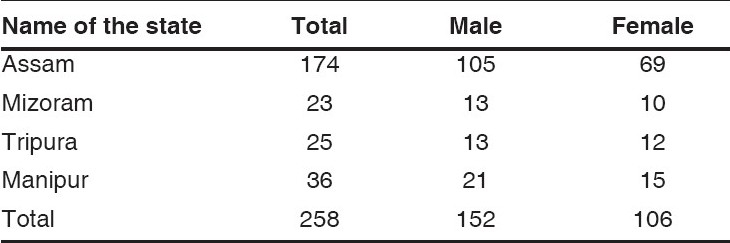
Among the children examined, 152 out of 258 (58.9 %) were males and 106 out of 258 (41.1 %) were females. There were 97 out of 376 (25.8%) students with functional low vision.
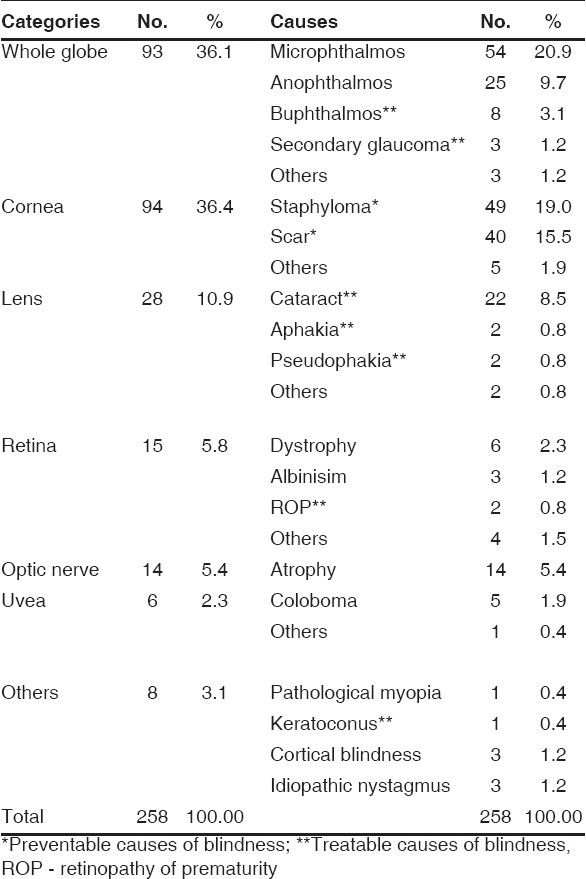
The whole globe 93 (36.1%), cornea 94 (36.4%), lens 28 (10.9%), retina 15 (5.8%) optic nerve 14 (5.4%) and uvea six (2.3%) were found to be the most frequently affected sites of abnormality [Table 2]. The globe appeared normal in one child with high pathological myopia, in one child with keratoconus, in three children with cortical blindness and three with idiopathic nystagmus.
Table 2.
Classification based on anatomical disorder of children with severe visual impairment and blindness
The etiological classification was based on the time of onset of the insult leading to visual loss, and the findings are shown in Table 3. Hereditary factors were identified in 18 (7%) cases, in which there was a positive family history of another similarly affected individual or well recognized or proved genetic/chromosomal disorders according to WHO/PBL eye examination record coding instructions. Postnatal causes were responsible for visual loss in 99 (38.4%) children, vitamin A deficiency being the single commonest cause 62 (24.0%) followed by measles 20 (7.8%).
Table 3.
Classification based on etiology of the vision loss in children with blindness

In 134 (51.9%) children the underlying cause remained undetermined; among them the abnormality had been present since birth in 95 (36.8%) children, and cataract and glaucoma of unknown cause were responsible for blindness in 26 (10.1%) and seven (2.7%) children, respectively.
One hundred and twenty-five (48.5%) children had potentially avoidable cause of blindness: preventable causes in 91 (35.3 %) children, and treatable causes in 34 (13.2%) children. Vitamin A deficiency and measles combined together was the major preventable cause of visual loss (31.8%), and cataract (10.1%) and glaucoma (2.7%) were the main treatable causes.
Discussion
There are some biases inherent in any study of children in schools for the blind. Children with multiple disabilities, preschool age children, those who have died, those from lower socioeconomic groups, and those from rural communities are likely to be under-represented in schools for the blind compared with population-based studies. In the present study, only 5% children had an additional disability, which is similar to a survey done in Maharashtra8 and Delhi,9 as children with multiple disabilities are often refused entry to schools for the blind in India.
Amongst children attending schools for the blind, corneal blindness was the most common cause of SVI and blindness (36.4%) and the major preventable cause identified. It was difficult to distinguish the different infectious causes of corneal blindness (such as ophthalmia neonatorum) without a good history. However, Vitamin A deficiency (VAD) is likely to have been an important contributing factor in many cases leading to keratomalacia and then to blindness. As VAD is associated with a high mortality rate, the children in schools for the blind represent only the survivors of a much larger problem. Vitamin A deficiency is known to vary markedly between regions.7 A history of measles (which can precipitate acute VAD) was also found in some cases (7.8%) of corneal blindness and this would be preventable by immunization. The high incidence of VAD-related blindness is, however, a cause of concern. It is an easily preventable cause of blindness and VAD as a cause of blindness in children has decreased in the more prosperous states like Maharashtra in west India.8 Congenital abnormalities of the globe (microphthalmos, anophthalmos and coloboma) were responsible for 30.6% of SVI and blindness. This is slightly higher than the results of the blind school study in Delhi in north India (27.4%),9 Karnataka (28.7%) and Tamil Nadu in south India (20.6%)7, but comparable to results from Maharashtra in west India (35%).8
The proportion of disease attributed to genetic factors in this study 18 (7%) is lower than the results from schools for the blind in south India (23%).10 The low proportion of genetic disease is likely to be related to the absence of consanguineous marriage in most of the NER. Research is needed to identify the causes of microphthalmos, anophthalmos and other anomalies of the globe in children.
The importance of hereditary factors (7%) and childhood factors (38.4%) contrasts with the small contribution from perinatal (three, 1.2%) and intrauterine factors (four, 1.6%). However, this study may underestimate the importance of both genetic and intrauterine factors, as in 36.8% of children the abnormality had been present since birth but the etiology could not be determined. The presence of a large proportion of children with visual loss of undetermined etiology is consistent with results from other studies using similar methods and reflects the limited investigations available and the lack of examination of family members in many cases.
A study of schools for the blind in south India had identified retinal dystrophies (including albinism) as the most common single cause of SVI and blindness, accounting for 26.1%.11 In our study retinal dystrophies accounted for only six (2.34%). Causes of SVI and blindness, which require specialist ophthalmic interventions, were cataract/aphakia 28 (10.8%) and buphthalmos/glaucoma 8 (3.7%).
To develop control programs to prevent childhood blindness, it is necessary to identify important avoidable causes in each country and monitor the changing patterns of childhood severely visually impaired or blind in different regions of the country over time. At least half, 125 (48.5%) of the children, were blind from potentially preventable or treatable conditions. Preventable causes 91 (35.3%) included VAD and measles 32 (31.8%), trauma and traditional harmful practices (TMP) 5 (1.9%), autosomal dominant conditions 2 (0.8%), and TORCH infection 2(0.8%). These findings suggest the importance of primary prevention, for example, high measles immunization coverage, promotion of breast feeding, health and nutrition education, and continued programs for the control of VAD through child survival programs. Easy availability of first aid and antibiotic eye drops would decrease the incidence of blinding corneal ulcers due to trauma.
Treatable causes of blindness 34 (13.2%) included cataract 26(10.1%), glaucoma seven (2.7%), and retinopathy of prematurity one (0.4%). Congenital cataract was the most important treatable cause of childhood blindness for which early diagnosis and referral, surgery by an experienced ophthalmologist, and long-term follow-up and management of aphakia and amblyopia are essential. There is a need to expand specialist pediatric ophthalmic services in the northeast, and it has been recommended that there should be one well-equipped child eye care center for every 10 million total population. It is important to begin to develop screening for retinopathy of prematurity as that is an increasing problem in countries with improving and expanding neonatal intensive care. Only one case was seen in this series, but a similar study from Delhi, the national capital that had better healthcare facilities, had more retinopathy of prematurity.9
Those with aphakia, microphthalmos, coloboma, pathological myopia, keratoconus and albinism were most likely to benefit from spectacles and/or low-vision aids. The provision of low- vision services (by a low-vision team) are extremely necessary for SVI and blind children to maximize their residual vision and subsequent improvement of quality of life.
The study also demonstrates the need for mandatory ophthalmic evaluation, refraction and assessment for low- vision devices prior to admission to schools for the blind because 24 (6.4%) students were classified as not blind, or SVI after refraction and another 13.6% students had potentially treatable disease. This evaluation should be repeated every two-three years.
Integrated education has been initiated in the state but the number of children integrated is still low. An alternative would be to encourage low-vision classes with print education in the blind schools alongside Braille classes, but this would require investment in teaching materials.
The pattern of childhood blindness in the northeastern states reveals the diversity of the region. Preventable causes like Vitamin A deficiency and corneal blindness are still common but newer challenges like congenital anomalies and retinopathy of prematurity are also seen. An integrated approach is needed to tackle this problem.
Acknowledgments
The authors are grateful to the State Blindness Control Societies of Assam, Mizoram, Manipur and Tripura for extending much needed help in the survey. We thank all the Principals/ Headmasters of schools for the blind and the children for their valuable help and consent.
We thank Dr. Jayanta Baruah, Nogaon, Dr. Narayan Bodoloi, Jorhat, Dr. R. K. Phukan, Lakhimpur, Dr. Yima Singh, Imphal, Dr. Manik Das, Agartala, Dr. Ramsanga and Dr. Nupuii for their valuable contribution to this survey.
We also thank Mr. Ratan Kalita, Mr. Amal Sarma, Mr. Jadu Das and Mr. Pranb Nath of Sri Sankaradeva Nethralaya for their contribution with the analysis of the data collected. Dr. Kuldeep Dole and Vasudha Raut of H.V.Desai Eye Hospital for reviewing the manuscript.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Gilbert C, Rahi J, Quinn G. Visual impairment and blindness in children. In: Johnson , Minassian , Weale , West , editors. Epidemiology of eye disease. 2nd ed. UK: Arnold Publishers; 2003. [Google Scholar]
- 2.World Health Organization. Global initiative for the elimination of avoidable blindness. Geneva: WHO; 1997. [Google Scholar]
- 3.Rahi JS, Gilbert CE, Foster A, Minassian D. Measuring the burden of childhood blindness. Br J Ophthalmol. 1999;83:387–8. doi: 10.1136/bjo.83.4.387. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Census of India 2001. India: Registrar General and Census Commissioner; 2001. [Google Scholar]
- 5.Dandona L, Gilbert CE, Rahi JS, Rao GN. Planning to reduce childhood blindness in India. Indian J Ophthalmol. 1998;46:117–22. [PubMed] [Google Scholar]
- 6.Gilbert C, Foster A, Negrel AD, Thylefors B. Childhood blindness: A new form for recording causes of visual loss in children. WHO Bull. 1993;71:485–9. [PMC free article] [PubMed] [Google Scholar]
- 7.Rahi JS, Sripathi S, Gilbert CE, Foster A. Childhood blindness due to vitamin A deficiency in India: Regional variations. Arch Dis Child. 1995;72:330–3. doi: 10.1136/adc.72.4.330. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Gogate P, Deshpande M, Sudrik S, Kishore H, Taras S, Gilbert C. Changing pattern of childhood blindness in Maharashtra, India. Br J Ophthalmol. 2007;91:8–12. doi: 10.1136/bjo.2006.094433. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Titiyal JS, Pal N, Murthy GV, Gupta SK, Tandon R, Vajpayee RB, et al. Causes and temporal trends of blindness and severe visual impairment in children in schools for the blind in North India. Br J Ophthalmol. 2003;87:941–5. doi: 10.1136/bjo.87.8.941. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 10.Rahi JS, Sripathi S, Gilbert CE, Foster A. The importance of prenatal factors in childhood blindness in India. Dev Med Child Neurol. 1997;39:449–55. doi: 10.1111/j.1469-8749.1997.tb07464.x. [DOI] [PubMed] [Google Scholar]
- 11.Hornby SJ, Adolph S, Gothwal VK, Gilbert CE, Dandona L, Foster A. Evaluation of children in six blind schools of Andhra Pradesh. Indian J Ophthalmol. 2000;48:195–200. [PubMed] [Google Scholar]