

Abstract
Purpose
Facial nerve injury can occur in the regions ranging from the cerebral cortex to the motor end plate in the face, and from many causes including trauma, viral infection, and idiopathic factors. Facial nerve paralysis in children, however, may differ from that in adults. We, therefore, evaluated its etiology and recovery rate in children and adults.
Materials and Methods
We retrospectively evaluated the records of 975 patients, ranging in age from 0 to 88 years, who displayed facial palsy at Kyung Hee Medical Center between January 1986 and July 2005.
Results
The most frequent causes of facial palsy in adults were Bell's palsy (54.9%), infection (26.8%), trauma (5.9%), iatrogenic (2.0%), and tumors (1.8%), whereas the most frequent causes of facial palsy in children were Bell's palsy (66.2%), infection (14.6%), trauma (13.4%), birth trauma (3.2%), and leukemia (1.3%). Recovery rates in adults were 91.4% for Bell's palsy, 89.0% for infection, and 64.3% for trauma, whereas recovery rates in children were 93.1% for Bell's palsy, 90.9% for infection, and 42.9% for trauma.
Conclusion
These results show that causes of facial palsy are similar in adults and children, and recovery rates in adults and children are not significantly different.
Keywords: Facial palsy, adult, children, causes, recovery
INTRODUCTION
Facial nerve paralysis is relatively rare, with an annual incidence of approximately 30 per 100,000 individuals in a population. Facial nerve paralysis has various causes, ranging from head injury to idiopathic Bell's palsy, and may occur as a result of injury to the central or peripheral nervous system.1 Since peripherally traveling facial nerves that run along the inside of the facial canal in the intratemporal bones are relatively long, they are at greater risk of injury compared with other cranial nerves. Facial nerve paralysis may induce facial asymmetry, leading to a loss of balanced appearance and function, which may have a deleterious effect on a patient's psychology and social life. Therefore, physicians treating patients with facial nerve paralysis are most frequently asked "what is the probability of improvement?" and "how much improvement will occur?"
Age is a prognostic factor in patients with facial nerve paralysis. For example, age is inversely related to recovery rate2,3 in adults with Bell's palsy. There have been few comparisons, however, regarding the causality and treatment outcomes in adults and children with facial nerve paralysis. We, therefore, assessed the causes and recovery rates in children and adults with facial nerve paralysis.
MATERIALS AND METHODS
The patient cohort consisted of 975 patients with facial nerve paralysis being treated at Kyung Hee Medical Center between January 1986 to December 2005. From their medical records, we retrospectively evaluated their age and sex, the cause of facial nerve paralysis, treatment methods, and recovery rate.
Patients were divided into 6 groups according to their age: 0 - 15 years, 16 - 30 years, 31 - 45 years, 46 - 60 years, 61 - 75 years, and older than 76 years. Patients aged 0 - 15 years were considered children, and those 16 years and older were considered adults. Patients without central nervous system diseases, otologic diseases, and cerebellopontine diseases were determined by medical history as well as by physical examination, and brain or temporal bone MRI. All patients were treated with bed rest, oral corticosteroids, peripheral vasodilators, and physical therapy. Adults were administered 80 mg/day oral prednisolone for the first 4 days, and doseages were tapered to 60 mg/day on days 5 and 6, 40 mg/day on days 7 and 8, 20 mg/day on days 9 and 10, and 10 mg/day on day 11. Children, adolescents, and light-weight adults were administered 1 mg/kg predinosolone for the first 4 days, followed by proportional tapering over the next 7 days.
The degree of facial nerve paralysis was evaluated based on the House-Brackmann classification method. Recovery was evaluated in patients who were followed up for longer than 6 months, with grades I and II recovery defined as satisfactory.
Statistical comparison was performed by the chi-square test, using SPSS for Windows (version 11.5, SPSS Inc., Chicago, IL, USA). A p < 0.05 was considered statistically significant.
RESULTS
Age and sex distribution
Of 975 patients, 447 (45.85%) were males and 528 were females (54.15%). The patients ranged in age from 0 to 88 years, with a mean age of 42.1 ± 21.5 years. Of these 975 patients, 157 (16.1%) were aged 0 - 15 years, 151 (15.5%) were 16 - 30 years old, 200 (20.5%) were 31 - 45 years old, 239 (24.5%) were 46 - 60 years old, 188 (19.3%) were 61 - 75 years old, and 40 (4.1%) were 76 years old or older (Fig. 1). The mean age of the 818 adults was 48.6 ± 16.9 years; 47.7 ± 17.1 years for men and 49.4 ± 16.6 years for women. The mean age of the 157 children was 8.2 ± 4.8 years; 8.0 ± 4.6 years for boys and 8.3 ± 5.0 years for girls.
Fig. 1.
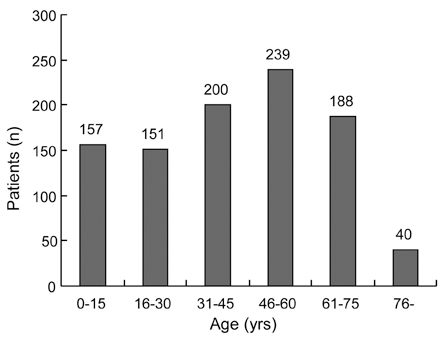
Number of patients, distributed by age.
Distribution of causality (Table 1)
Table 1.
Cause of Facial Palsy in Adults and Children

The most common cause of facial paralysis in adults was Bell's palsy (449 patients, 54.9%); followed by infection, including herpes zoster oticus, otitis media, otitis media with cholesteatoma, and tuberculosis lymphadenitis (219 patients, 26.8%). Traumatic causes, such as temporal bone fracture, cerebral contusion, facial injury, basal skull fracture, and epidural hemorrhage accounted for 5.9%, or 49 patients. Iatrogenic causes such as mastoidectomy and parotidectomy made up for 2% of the population (17 patients). Tumors such as pinealoma, meningioma, acoustic neuroma, parotid tumor, pontine glioma, malignant lymphoma, and lung cancer metastases accounted for 1.8% of the population (15 patients); and other causes, such as diabetes mellitus neuropathy, Guillain-Barre syndrome, cerebral infarction, leukemia, posterior communicating artery aneurysm, and trigeminal neuropathy accounted for 8.4% (69 patients).
The most common causes of facial paralysis in children was Bell's palsy (104 patients, 66.2%), followed by infection, including herpes zoster oticus and otitis media (23 patients, 14.6%), then traumatic causes such as temporal bone fracture, facial injury, and cerebral contusion (21 patients, 13.4%), and other causes, such as birth trauma, leukemia, facial burn, and postoperation of brachial cleft cyst (9 patients, 5.7%).
The rates of Bell's palsy (p = 0.009) and trauma (p = 0.001) were significantly higher in children than in adults, whereas the rate of infection was significantly higher in adults than in children (p = 0.001).
Overall, Bell's palsy was the most prevalent cause of facial paralysis (553 patients, 56.7%), followed by infection (242 patients, 24.8%), trauma (70 patients, 7.2%), and iatrogenic causes (18 patients, 1.8%).
Relationship between treatment and causality (Table 2)
Table 2.
Treatments Methods according to Causes in Adults and Children

S, steroid; A, antibiotics; V, antiviral agent.
All patients were treated with bed rest, oral steroids, peripheral vasodilators, and physical therapy. Medical treatments consisted of steroid monotherapy and combinations of steroids with antiviral agents or antibiotics. Surgical treatments consisted of facial nerve decompression, nerve graft, mastoidectomy, temporalis muscle transfer, and tumor resection.
Of 449 adults with Bell's palsy, 360 received steroid monotherapy; 83 received combinations of steroids and antiviral agents, 3 were treated with a combination of steroids and facial nerve decompression, temporalis muscle transfer, one patient with herpes zoster oticus was treated with a combination of steroids, antiviral agents and facial nerve decompression, and the remaining 173 were treated with a combinations of steroids and anti-viral agents. The most common treatment of adults with infectious causes of facial paralysis consisted of combinations of steroids and antibiotics; 3 patients with otitis media and cholesteatoma were treated with facial nerve decompression and mastoidectomy, and 21 were treated with mastoidectomy alone. Of patients with otitis media, 3 were treated with facial nerve decompression and mastoidectomy, and 9 were treated with mastoidectomy alone. Facial nerve decompression was performed in 3 patients with temporal bone fractures, and patients with facial paralysis caused by tumors underwent tumor resection.
Of children with Bell's palsy cases, 92 were treated with steroid monotherapy, and 12 were treated with acupuncture at the Department of Oriental Medicine. Children with herpes zoster oticus were treated with combinations of steroids and anti-viral agents. Eight children with otitis media were treated with combinations of steroids and antibiotics, and 1 was treated with a combination of steroids, antibiotics and myringotomy. Four children with temporal bone fractures were treated with steroid monotherapy, 3 were treated with steroids and facial nerve decompression, and 1 was treated with steroids and nerve graft. In addition, 2 neonates diagnosed with Bell's palsy and 5 patients with birth trauma were observed without other treatment.
Recovery rate
Of the 975 patients, 657 were followed up for longer than 6 months, with 577 patients showing satisfactory recovery, yielding an overall recovery rate of 87.8%.
Recovery rate according to gender
Overall recovery rates for male patients were 85.5% (247 of 289), 84.6% for adults (193 of 228) and 88.5% for children (54 of 61). Overall recovery rates for female patients were 89.7% (330 of 368), 90.2% for adults (268 of 297) and 87.3% for children (62 of 71).
Recovery rate according to age (Fig. 2)
Fig. 2.
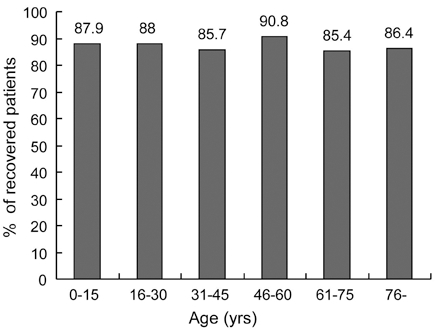
Percentage of recovered patients according to age.
Recovery rates were 87.9% in children aged 0 - 15 years (116 of 132) and 87.8% in adults aged 16 years and older (461 of 525) (p = 0.983). When adult patients were evaluated by age, the recovery rates were 88.0% in those aged 16 - 30 years (110 of 125), 85.7% in those aged 31 - 45 years (120 of 140), 90.8% in those aged 46 - 60 years (129 of 142), 85.4% in those aged 61 - 75 years (82 of 96) and 86.4% in those aged 76 years and older (19 of 22).
Recovery rate according to cause (Table 3)
Table 3.
Recovery Rate according to Causes in Adults and Children

Bell's palsy
Of 403 patients with Bell's palsy, 370 (91.8%) recovered, 275 of 301 adults (91.4%) and 95 of 102 children (93.1%) (p = 0.619). In adults aged 16 - 30, 31 - 45, 46 - 60, 61 - 75, and 76 years and older, the recovery rates were 95.5% (64 of 67), 91.0% (71 of 78), 91.1% (82 of 90), 89.0% (49 of 55), and 81.8% (9 of 11), respectively (Fig. 3).
Fig. 3.
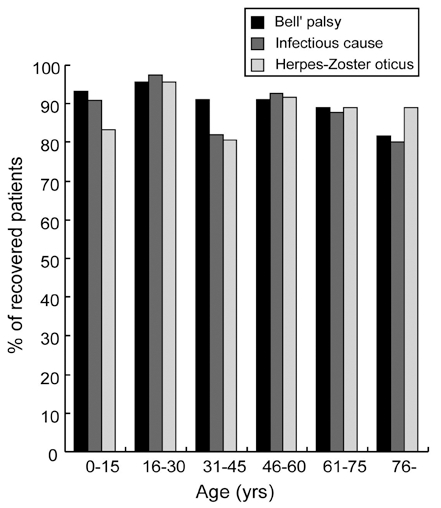
Percentage of patients who recovered from Bell's palsy, infectious causes and herpes zoster oticus according to age.
Trauma
Of 42 patients with traumatic causes of facial paralysis, 24 (57.1%) recovered; 18 of 28 adults (64.3%) and 6 of 14 children (42.8%).
Temporal bone fracture
Of 11 adults with temporal bone fracture, 7 (63.6%) recovered, compared with 2 of 6 children (33.3%).
Cerebral contusion
Of 9 adults with cerebral contusion, 7 (77.8%) recovered, compared with 4 of 8 children (50%).
Others
Four of 6 adults with facial injury (66.6%) recovered, but none of 2 adults with basal skull fracture (0%).
Infection
Of 183 patients with infectious causes of facial paralysis, 163 (89.0%) recovered; 153 of 172 adults (88.9%) and 10 of 11 children (90.9%). In adults aged 16 - 30, 31 - 45, 46 - 60, 61 - 75, and 76 years and older, the recovery rates were 97.3% (36 of 37), 82.0% (41 of 50), 92.8% (39 of 42), 87.8% (29 of 33), and 80.0% (8 of 10), respectively (Fig. 4).
Herpes zoster oticus
Of 141 patients with herpes zoster oticus, 124 (87.9%) recovered; 119 of 135 adults (88.1%), and 5 of 6 children (83.3%) (p = 0.723). In adults aged 16 - 30, 31 - 45, 46 - 60, 61 -75, and 76 years and older, the recovery rates were 95.5% (21 of 22), 80.5% (33 of 41), 91.7% (33 of 36), 88.9% (24 of 27), and 88.9% (8 of 9), respectively (Fig. 5).
Otitis media
Of 17 adults with otitis media, 15 (88.2%) recovered, as did 19 of 20 adults with otitis media with cholesteatoma (95.0%), and all 5 children with otitis media.
Others
In adults, 7 of 9 with iatrogenic causes of facial paralysis (77.8%), 1 of 4 with tumors (25.0%), 7 of 11 with cerebral infarctions (63.6%), 0 of 1 with diabetic neuropathy and 1 of 1 with trigeminal neuropathy (100%) recovered, as did all 5 children with facial paralysis caused by birth trauma (100%).
DISCUSSION
Since facial nerves have a long intracranial course and pass through the narrow bony canal within the intratemporal bone, they are more readily injured by middle ear or temporal bone surgery, trauma, infection, and compression caused by tumors in or within the vicinity of nerves. Moreover, facial nerve paralysis may develop secondarily as a result of systemic diseases, or, although rarely, may accompany congenital anomalies. In an analysis of 2,165 patients with facial nerve paralysis, Bell's palsy was the most prevalent cause, followed by incidence of trauma and herpes zoster cephalicus.4 In a second analysis of 161 patients with facial nerve paralysis, the causes were in order of decreasing frequency Bell's palsy, trauma, and chronic otitis media.5 In our overall patient population, the cause of facial paralysis was in the order of Bell's palsy, infection, and trauma. In adults, the order was Bell's palsy, infections, such as herpes zoster oticus, otitis media, otitis media with cholesteatoma, and tuberculosis lymphadenitis, and trauma such as temporal bone fracture, cerebral contusion, facial injury, basal skull fracture, and epidural hemorrhage. The order in children was similar to that in adults: Bell's palsy, infection including herpes zoster cephalicus and acute otitis media, and trauma, including cerebral concussion, temporal bone fracture, and facial injury. The incidence of facial paralysis caused by trauma was significantly higher in children than adults. This may have arisen for various reasons. First, children suffer more severe injuries caused by falls, traffic accidents, and other causes than adults. This is supported by the observation that 10 out of 14 children were H-B grade V, whereas 12 out of 28 adults were H-B grade V. Second, the incidence of facial paralysis due to infection was significantly higher in adults than in children. Finally, there were fewer children in the study than adults.
Numerous studies conducted on factors influencing the prognosis of facial nerve palsy showed younger age,6-8 initial paralysis lower than HB grade III,6-9 and normal responses on nerve excitability tests6,9 and in stapedial reflex,9,10 were associated with good prognosis.
As age increases, so does vascular degeneration, which leads to a decrease in peripheral blood supply. These conditions may cause Bell's palsy, with recovery from facial nerve paralysis shown to decrease with increasing age of patients.11 Other studies6-8 found that age is a prognostic factor in patients with facial nerve paralysis. However we found that recovery rate in patients with Bell's palsy was not related to age, with no statistically significant difference between children and adults (p = 0.983).
Recovery rates have been shown to depend on the cause of facial nerve paralysis, with one study showing complete recovery in 64% of patients with Bell's palsy, 55.4% of patients with herpes zoster oticus, 78% of patients with otitis media, and 43% of patients with temporal bone fracture.12 In contrast, others3 have reported that the recovery rate in patients with Bell's palsy was higher than that in patients with herpes zoster oticus. We found, however, that the recovery rate in Bell's palsy patients (91.8%) did not differ significantly from that in patients with herpes zoster oticus (p = 0.171).
Another important prognostic factor is electroneurography, with satisfactory recovery observed in 98% of patients with scores higher than 25% on the healthy side when electroneurography was performed within 10 days of onset.13 Although electroneurography is an objective recording method for facial nerve paralysis as well as being a useful test for assessing the ratio of axons without Wallerian's degeneration, it cannot accurately predict prognosis of patients with facial nerve paralysis caused by herpes zoster oticus.14
Various methods have been used to treat facial nerve paralysis, depending on causality. Spontaneous recovery, however, has been observed in 85% of patients with Bell's palsy, with 71% showing complete recovery (grade I), and another 13% showing satisfactory recovery (grade II).15 Oral steroids are a preferred treatment for patients with Bell's palsy, although it produces mixed results. For example, a retrospective assessment found that prednisone effectively prevented nerve degeneration,16 whereas a prospective, double blind trial found that steroids had no effect when started within 2 days of the disease onset.17 Since the etiology of Bell's palsy is thought to include viral infection,18 the combination of steroids and the antiviral agent acyclovir has been used to treat this condition. Patients treated with steroids and acyclovir had a higher recovery rate than those treated with steroids alone; 92% vs. 76% in one trial,19 and 96.5% vs. 89.7% in another.20 We found that the recovery rate with steroid monotherapy was 85.1%, whereas that with steroid and acyclovir was 92.5%, although the difference was not statistically significant.
Even in studies reporting that more than 80% of Bell's palsy patients achieve complete recovery, approximately 16% of patients do not achieve even satisfactory recovery.21
Surgical methods have, therefore, been utilized to correct incompletely recovered facial nerve paralysis, including methods such as cross-facial nerve grafts with the hypoglossal or spinal accessory nerve, nerve cross-over using the phrenic nerve, or muscle transfer using the temporalis or masseter muscle.22,23 Recently, the suprascapular nerve has been used for extracranial facial nerve reinnervation.24 In addition, non-invasive methods or Botulinum toxin A may resolve the excessive tension at the opposite side of the paralyzed face, as well as other diverse methods have been attempted.
Another important treatment method is physical therapy. Thus, in addition to drug treatments, all of our patients were referred for physical therapy to the Department of Rehabilitation Medicine. For these patients, physical therapy primarily consisted of neuromuscular retraining of the paralyzed nerve.25 Through electrical stimulation, EMG feedback, and facial expression exercises, this physical therapy regimen enables patients to understand facial exercises and paralysis and to induce natural face movements. These exercises can help prevent the atrophy and contracture of the facial muscles and maintain facial symmetry. The development of synkinesis in patients with facial nerve paralysis can be reduced by neuromuscular retraining.26 In addition, in our department, pamphlets on facial expression exercise were distributed to all facial nerve paralysis patients. Thus, after discharge from the hospital, patients can be trained to move each facial muscle while watching themselves in a mirror.
The facial expression program performed in our department27 consisted of training the expression of each facial muscle, with frowning induced by moving the frontalis muscle, forming waveforms between the eye brows by moving the corrugator supercilii muscle, making wrinkles by moving the procerus muscle, protruding the lips by moving the orbicularis oris muscle, smiling widely by moving the zygomaticus major muscle, protruding the lower lip by moving the mentalis muscle, lowering both ends of the mouth by moving the depressor anguli oris muscle, and filling the mouth with air and exhaling by moving the buccinator muscle. Patients with residual Bell's paralysis who performed such facial muscle exercises showed improvements in their level of paralysis.28
Patients with facial nerve paralysis caused by herpes zoster otitis were treated with acyclovir (800 mg, 5 times daily) and prednisone (60 mg daily for 3 - 5 days). Injections of 100 mg of hydrocortisone and intravenous administration of 5 mg/kg acyclovir every 8 hors for 7 days were shown to induce recovery in 82.6% of patients.29
Due to the disposition of our country, most adults were treated with acupuncture, compared with only 12% of children with Bell's palsy. Acupuncture has been reported to stimulate the central nerve system by secreting chemical substances to the muscles, spinal cord, and the brain. Moreover, acupuncture has been reported to conduct electromagnetic signals and to change involuntary body functions.30
Surgical methods are required for patients in whom paralysis developed immediately after trauma or as the result of chronic otitis media or acute mastoiditis. These surgical methods can include facial nerve decompression, end-to-end anastomosis, nerve graft anastomosis, and nerve cross anastomosis, while several of our patients were treated also with temporalis muscle transfer, mastoidectomy, myringotomy, or tumor resection.
In conclusion, facial nerve paralysis in both adults and children is caused by Bell's palsy, infection, and trauma in decreasing order. In contrast to previous studies, we did not observe a statistically significant difference in recovery rate between adults and children.
Footnotes
This research was supported by the Program of Kyung Hee University for the Young Researcher in Medical Science(KHU-1491).
References
- 1.Kim IS, Shin SH, Kim J, Lee WS, Lee HK. Correlation between MRI and operative findings in Bell's palsy and Ramsay Hunt syndrome. Yonsei Med J. 2007;48:963–968. doi: 10.3349/ymj.2007.48.6.963. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Danielidis V, Skevas S, Van Cauwenberge P, Vinck B. A comparative study of age and degree of facial nerve recovery in patients with Bell's palsy. Eur Arch Otorhinolaryngol. 1999;256:520–522. doi: 10.1007/s004050050203. [DOI] [PubMed] [Google Scholar]
- 3.Ikeda M, Abiko Y, Kukimoto N, Omori H, Nakazato H, Ikeda K. Clinical factors that influence the prognosis of facial nerve paralysis and the magnitudes of influence. Laryngoscope. 2005;115:855–860. doi: 10.1097/01.MLG.0000157694.57872.82. [DOI] [PubMed] [Google Scholar]
- 4.May M. Differential diagnosis by history, physical findings, and laboratory results: clinical-pathologica Correlation. In: May M, editor. The facial nerve. New York: Thieme Inc; 1986. pp. 181–216. [Google Scholar]
- 5.Kim JS, Kim LS. Diagnosis and treatment of peripheral facial nerve paralysis. Seoul symposium. 1985;1:153–206. [Google Scholar]
- 6.Kerbavaz RJ, Hilsinger RL, Jr, Adour KK. The facial paralysis prognostic index. Otolaryngol Head Neck Surg. 1983;91:284–289. doi: 10.1177/019459988309100315. [DOI] [PubMed] [Google Scholar]
- 7.Smith IM, Heath JP, Murray JA, Cull RE. Idiopathic facial(Bell's) palsy: a clinical survey of prognostic factors. Clin Otolaryngol Allied Sci. 1988;13:17–23. doi: 10.1111/j.1365-2273.1988.tb00276.x. [DOI] [PubMed] [Google Scholar]
- 8.Ko JY, Sheen TS, Hsu MM. Herpes zoster oticus treated with acyclovir and prednisolone: clinical manifestations and analysis of prognostic factors. Clin Otolaryngol Allied Sci. 2000;25:139–142. doi: 10.1046/j.1365-2273.2000.00336.x. [DOI] [PubMed] [Google Scholar]
- 9.Gavilán C, Gavilán J, Rashad M, Gavilán M. Discriminant analysis in predicting prognosis of Bell's palsy. Acta Otolaryngol. 1988;106:276–280. doi: 10.3109/00016488809106436. [DOI] [PubMed] [Google Scholar]
- 10.Hydén D, Sandstedt P, Odkvist LM. Prognosis in Bell's palsy based on symptoms, signs and laboratory data. Acta Otolaryngol. 1982;93:407–414. doi: 10.3109/00016488209130898. [DOI] [PubMed] [Google Scholar]
- 11.Devriese PP, Schumacher T, Scheide A, de Jongh RH, Houtkooper JM. Incidence, prognosis and recovery of Bell's palsy. A survey of about 1000 patients (1974-1983) Clin Otolaryngol Allied Sci. 1990;15:15–27. doi: 10.1111/j.1365-2273.1990.tb00427.x. [DOI] [PubMed] [Google Scholar]
- 12.Kim HN, Chang SO, Lee WS. Facial nerve symposium. Seoul: Ilji Munwha Printing Co; 1995. Basic and clinical management; pp. 129–175. [Google Scholar]
- 13.May M, Shambaugh GE. Facial nerve paralysis. In: Paparella MM, Shumrick DA, Gluckman JL, Meyerhoff WL, editors. Otolaryngology. 3rd ed. Philadelphia: W.B. Saunders; 1991. p. 1106. [Google Scholar]
- 14.Lee DH, Chae YS, Park YS, Yeo SW. Prognostic value of electroneurography in Bell's palsy and Ramsay-Hunt's syndrome. Clin Otolaryngol. 2006;31:144–148. doi: 10.1111/j.1749-4486.2006.01165.x. [DOI] [PubMed] [Google Scholar]
- 15.Peitersen E. Bell's palsy: The spontaneous course of 2,500 peripheral facial nerve palsies of different etiologies. Acta Otolaryngol Suppl. 2002;549:4–30. [PubMed] [Google Scholar]
- 16.Adour KK, Wingerd J, Bell DN, Manning JJ, Hurley JP. Prednisone treatment for idiopathic facial paralysis (Bell's Palsy) N Engl J Med. 1972;287:1268–1272. doi: 10.1056/NEJM197212212872503. [DOI] [PubMed] [Google Scholar]
- 17.May M, Wette R, Hardin WB, Jr, Sullivan J. The use of steroids in Bell's palsy: a prospective controlled study. Laryngoscope. 1976;86:1111–1122. doi: 10.1288/00005537-197608000-00003. [DOI] [PubMed] [Google Scholar]
- 18.Furuta Y, Fukuda S, Chida E, Takasu T, Ohtani F, Inuyama Y, et al. Reactivation of herpes simplex virus type I in patients with Bell's palsy. J Med Virol. 1998;54:162–166. doi: 10.1002/(sici)1096-9071(199803)54:3<162::aid-jmv3>3.0.co;2-3. [DOI] [PubMed] [Google Scholar]
- 19.Adour KK, Ruboyianes JM, Von Doersten GP, Byl FM, Trent CS, Quesenberry CP, Jr, et al. Bell's palsy treatment acyclovir and prednisone compared with prednisone alone: a double-blind, randomized, controlled trial. Ann Otol Rhinol Laryngol. 1996;105:371–378. doi: 10.1177/000348949610500508. [DOI] [PubMed] [Google Scholar]
- 20.Hato N, Matsumoto S, Kisaki H, Takahashi H, Wakisaka H, Honda N, et al. Efficacy of early treatment of Bell's palsy with oral acyclovir and prednisolone. Otol Neurotol. 2003;24:948–951. doi: 10.1097/00129492-200311000-00022. [DOI] [PubMed] [Google Scholar]
- 21.Peitersen E. Natural history of Bell's palsy. Acta Otolaryngol Suppl. 1992;492:122–124. doi: 10.3109/00016489209136829. [DOI] [PubMed] [Google Scholar]
- 22.Julian GG, Hoffmann JF, Shelton C. Sugical rehabilitation of facial nerve paralysis. Otolaryngol Clin North Am. 1997;30:701–726. [PubMed] [Google Scholar]
- 23.Hoffman WY. Reanimation of the paralyzed face. Otolaryngol Clin North Am. 1992;25:649–667. [PubMed] [Google Scholar]
- 24.Tubbs RS, Louis RG, Jr, Wartmann CT, Loukas M, Shoja MM, Ardalan MR, et al. Suprascapular nerve as a donor for extracranial facial nerve reanimation procedures: a cadaveric feasibility study. J Neurosurg. 2008;108:145–148. doi: 10.3171/JNS/2008/108/01/0145. [DOI] [PubMed] [Google Scholar]
- 25.Balliet R. Facial paralysis and other neuromuscular dysfunctions of the peripheral nervous system. In: Payton OD, editor. Manual of physical therapy. New York, NY: Churchill Livingstone; 1989. p. 175. [Google Scholar]
- 26.Brach JS, VanSwearingen JM, Lenert J, Johnson PC. Facial neuromuscular retraining for oral synkinesis. Plast Reconstr Surg. 1997;99:1922–1931. doi: 10.1097/00006534-199706000-00017. discussion 1932-3. [DOI] [PubMed] [Google Scholar]
- 27.Ahn KH. Rehabilitation of Bell's Palsy. In: Kim HN, Chang SO, Lee WS, editors. Facial nerve symposium. Basic and clinical management. Seoul: Ilji Munwha Printing Co.; 1995. pp. 212–229. [Google Scholar]
- 28.Cederwall E, Olseń MF, Hanner P, Fogdestam I. Evaluation of a physiotherapeutic treatment intervention in "Bell's" facial palsy. Physiother Theory Pract. 2006;22:43–52. doi: 10.1080/09593980500422529. [DOI] [PubMed] [Google Scholar]
- 29.Uri N, Greenberg E, Kitzes-Cohen R, Doweck I. Acyclovir in the treatment of Ramsay Hunt syndrome. Otolaryngol Head Neck Surg. 2003;129:379–381. doi: 10.1016/s0194-5998(03)01305-6. [DOI] [PubMed] [Google Scholar]
- 30.Maslov B, Roje-Bedeković M, Miškov S, Demarin V. Acupuncture treatment in facial palsy-clinical observations. Acta Clin Croat. 2002;43:275–279. [Google Scholar]