

Abstract
Purpose
Goggles are frequently worn in the sport of swimming and are designed to form a seal around the periorbital tissue orbit. The resultant pressure on the eye may have the potential to affect intraocular pressure and blood flow of the optic nerve head. This study evaluates the influence of wearing swimming goggles on intraocular pressure (IOP) and blood flow of the ocular nerve head (ONH) in normal subjects.
Materials and Methods
Thirty healthy participants took part in this study. The IOP of each participant was measured using a Goldmann tonometer. Measurements were taken immediately before putting on swimming goggles, at 5, 10, 30, and 60 minutes after putting on swimming goggles, and then immediately after taking off the goggles. Blood flow of the ONH was measured using the Heidelberg retinal flowmeter.
Results
The average IOP before, during and after wearing the swimming goggles were 11.88 ± 2.82 mmHg, 14.20 ± 2.81mmHg and 11.78 ± 2.89 mmHg, respectively. The IOP increased immediately after putting on the goggles (p < 0.05) and then returned to normal values immediately after removal (p > 0.05). Blood flow of the ONH was 336.60 ± 89.07 Arbitrary Units (AU) before and 319.18 ± 96.02 AU after the goggles were worn (p < 0.05).
Conclusion
A small but significant IOP elevation was observed immediately after the swimming goggles were put on. This elevated IOP was maintained while the goggles were kept on, and then returned to normal levels as soon as they were taken off. Blood flow of the ONH did not change significantly throughout the experiment. These facts should be considered for safety concerns, especially in advanced glaucoma patients.
Keywords: Swimming goggles, intraocular pressure, blood flow of optic nerve head
Elevation of intraocular pressure is an important risk factor in the progression of glaucoma. Swimming goggles induce pressure around the periocular area and might have an influence on the intraocular pressure (IOP). Swimmers who wear goggles are exposed to this pressure, and several patients in our clinic have asked whether this could have an influence on the progression of glaucoma. We are unaware of any previous reports discussing the relationship between goggles and an IOP elevation. In this study, we evaluated whether swimming goggles have an influence on the IOP as well as on the blood flow of the optic nerve head (ONH).1
MATERIALS AND METHODS
We obtained informed consent from each participant, and our study was approved by the Institutional Review Board. The study was comprised of 30 eyes from 30 healthy volunteers (18 male, 12 female). One eye of each patient was selected randomly for the analysis. The average age of the subjects was 27.4 years (26 - 32). The criteria for this study required a completely normal ophthalmic examination after pupil dilation with a best-corrected vision ≥ 20/25, IOP < 20 mmHg and no family history of glaucoma. IOP was measured in all patients before the goggles were applied, at 5, 10, 30 and 60 minutes after the goggles were put on, and then immediately after the goggles were removed. Blood flow of the ONH was measured immediately before and after the goggles were worn. As shown in Fig. 1, the lenses of the goggles were removed to allow the measurement of the IOP. The IOP was measured at each time-point by one examiner (CWS) three times, and the readings were averaged. A Heidelberg retinal flowmeter (HRF) (Heidelberg Engineering GmbH, Heidelberg, Germany) was used to measure the blood flow of the ONH. One examiner measured all the patients, and then the data was analyzed using an Automatic Full-Field Perfusion Image Analyzer (AFFPIA) program, which calculated the 'average flow'.2,3 Arbitrary units (AU) were used in the HRF software to measure blood flow, volume and velocity measurements. The conventional method to measure blood flow in the ONH, which uses a sampling technique in a 10 × 10 pixel frame, can show a fluctuation according to the selection of the pixels. In this case to analyze the blood flow, the AFFPIA uses two circles with one just inside the margin of the optic disc and the other just outside the optic pit, ensuring precision in the measurements.
Fig. 1.

Swimming goggles with anterior part of lens removed to measure IOP while wearing them.
The difference between IOP before and after wearing swimming goggles was analyzed using repeated measurements and Analysis of Variance(ANOVA) with Bonferroni correction. The statistical significance was set at p < 0.05.
RESULTS
The IOP before the swimming goggles were worn was 11.88 ± 2.82 mmHg (mean ± SD; n=30). The IOP increased by 2.32 mmHg (p < 0.05) to 14.20 ± 2.82 mmHg (mean ± SD; n=30) immediately after the goggles were put on. Over the 60 minutes while the goggles were worn, the average IOP was 14.63 ± 2.92 mmHg (mean ± SD; n=30) at five minutes, 14.72 ± 2.94 mmHg (mean ± SD; n=30) at 10 minutes, 14.60 ± 2.78 mmHg (mean ± SD; n=30) at 30 minutes and 14.51 ± 2.82 mmHg (mean ± SD; n=30) at 60 minutes (p < 0.05). The IOP decreased to 11.78 ± 2.89 mmHg (mean ± SD; n=30) immediately after the goggles were taken off(Fig. 2). The HRF showed an average flow of 336.60 ± 89.07 AU (mean ± SD; n=30) before the goggles were put on, and decreased to 319.18 ± 96.02 AU (mean ± SD; n=30) immediately after they were taken off. However, the difference between these two values did not show statistical significance (p =0.58).
Fig. 2.
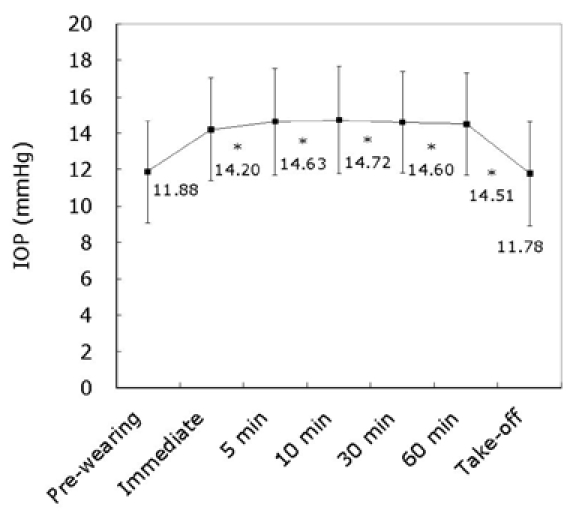
Mean IOP (mean ± SD) change before and while the goggles were worn, and after they were removed(Repeated measures of ANOVA with Bonferroni correction, *p < 0.05).
DISCUSSION
Various activities in everyday life have been reported to increase intraocular pressure. Playing the trumpet has been reported to elevate the IOP by 20 mmHg,4 the Sirsasana posture in yoga has been shown to induce IOP to rise up to 15.8 mmHg,5 and the necktie has been shown to be responsible for a 1.58 mmHg rise in IOP.6,7 In this study, swimming goggles resulted in a 2.4 mmHg increase in IOP. This rise may not be as high as that of musicians playing the trumpet or yoga practitioners in the Sirsasana posture, but it is greater than the IOP rise caused by neckties. Although this increase in IOP may not have a significant effect on normal participants, any elevation of IOP, such as that caused by the wearing of swimming goggles, may be detrimental to patients with advanced glaucoma.8 The IOP elevation was observed immediately after the goggles were put on, and this elevation returned to a normal level immediately after they were removed. Although the decrease in IOP immediately after removing the goggles did not have statistical significance, it does imply that the change in IOP is a result of direct pressure on the periorbital tissue.
This preliminary study has been performed in normal subjects who are much younger than the average glaucoma patient, so further studies in glaucomatous subjects are necessary. Also, this study simulates only partial effects of the swimming goggles because the anterior section of the lens was removed. The vacuum pressure inside the chamber formed in each eye by the goggles should also be considered.
This study used one common type of swimming goggles, and so a different goggle design which has less pressure around periorbital tissue could have a different effect on IOP. Therefore, advanced glaucoma patients who use swimming goggles regularly should be carefully monitored, or should use specially-designed swimming goggles that produce minimal pressure around the eyelid.
References
- 1.Sato EA, Ohtake Y, Shinoda K, Mashima Y, Kimura I. Decreased blood flow at neuroretinal rim of optic nerve head corresponds with visual field deficit in eyes with normal-tension glaucoma. Graefes Arch Clin Exp Ophthalmol. 2006;244:795–801. doi: 10.1007/s00417-005-0177-2. [DOI] [PubMed] [Google Scholar]
- 2.Boehm AG, Pillunat LE, Koeller U, Katz B, Schicketanz C, Klemm M, et al. Regional distribution of optic nerve head blood flow. Graefes Arch Clin Exp Ophthalmol. 1999;237:484–488. doi: 10.1007/s004170050266. [DOI] [PubMed] [Google Scholar]
- 3.Logan JF, Rankin SJ, Jackson AJ. Retinal blood flow measurements and neuroretinal rim damage in glaucoma. Br J Ophthalmol. 2004;88:1049–1054. doi: 10.1136/bjo.2003.034884. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 4.Schuman JS, Massicotte EC, Connolly S, Hertzmark E, Mukherji B, Kunen MZ. Increased intraocular pressure and visual field defects in high resistance wind insrutment players. Ophthalmology. 2000;107:127–133. doi: 10.1016/s0161-6420(99)00015-9. [DOI] [PubMed] [Google Scholar]
- 5.Baskaran M, Raman K, Ramani v, Roy J, Vijaya L, Badrinath SS. Intraocular pressure changes and ocular biometry during sirsasana (headstand posture) in yoga practitioners. Ophthalmology. 2006;113:1327–1332. doi: 10.1016/j.ophtha.2006.02.063. [DOI] [PubMed] [Google Scholar]
- 6.Talty P, O'Brien PD. Does extended wear of a tight necktie cause raised intraocular pressure? J Glaucoma. 2005;14:508–510. doi: 10.1097/01.ijg.0000185435.08051.cb. [DOI] [PubMed] [Google Scholar]
- 7.Teng C, Gurses-Ozden R, Liebmann JM, Tello C, Ritch R. Effect of a tight necktie on intraocular pressure. Br J Ophthalmol . 2003;87:946–948. doi: 10.1136/bjo.87.8.946. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.The Advanced Glaucoma Intervention Study (AGIS) 7. The relationship between control of intraocular pressure and visual field deterioration. The AGIS Investigators. Am J Ophthalmol. 2000;130:429–440. doi: 10.1016/s0002-9394(00)00538-9. [DOI] [PubMed] [Google Scholar]