

Abstract
Purpose
The short-term safety and efficacy of zoledronic acid for the treatment of skeletal metastasis was evaluated in patients with hormone-refractory prostate cancer.
Patients and Methods
A total of 19 hormone-refractory prostate cancer patients with bone metastases were enrolled. All patients received up to six infusions of zoledronic acid (4 mg, given intravenously over 15 minutes, every 3 - 4 weeks). Safety was assessed by monitoring a`dverse events and serum creatinine levels. Efficacy was assessed by monitoring skeletal-related events, brief pain inventory score, quality of life score, type of pain medication, and analgesic score. Mean age of patients was 67.3 years (46 - 86 years), mean time from diagnosis of bone metastases was 27.6 months (0 - 117 months), and mean time from diagnosis of hormone-refractory disease was 7.5 months (0 - 26 months).
Results
There was no clinically significant change in serum creatinine levels. Eleven adverse events (musculoskeletal disorders and systemic disorders) in 8 patients were classed as having a possible relationship to study drug. Fifteen patients completed six courses of zoledronic acid infusion. There were no significant changes in the brief pain inventory composite scores, quality of life questionnaire scores or analgesic score. No new skeletal-related events developed during the treatment period.
Conclusion
Zoledronic acid administered in this study as a 15-minute infusion demonstrated an acceptable and well-known safety profile in patients with refractory prostate cancer with bone metastases. However, prospective placebo-controlled clinical trials are required to elucidate the efficacy of zoledronic acid.
Keywords: Prostatic neoplasms, neoplasm metastasis, zoledronic acid
INTRODUCTION
Every year, half a million men are diagnosed with prostate cancer worldwide and more than two hundred thousand die of this disease.1 The majority of patients (65 - 75%) with advanced prostate cancer characteristically develop bone metastases to the spine, pelvis and ribs, and most of these patients experience skeletal-related events (SREs), such as pathological bone fractures, spinal cord compression or debilitating bone pain.2 Therefore, the occurrence of SREs is one of the most important factors that can impact on a patient's quality of life.
The older a patient is at prostate cancer diagnosis, the more likely hormone therapy and bone metastases will contribute to bone loss leading to SREs. In the US, bone loss is prevalent among 1.5 million men aged over 65 years.3 In addition, approximately 33% of all hip fractures occur in men, and the mortality rate due to hip fractures in men is known to be twofold greater than that in women.4 Sometimes patients with prostate cancer have pre-existing osteopenia and bone loss before the start of hormone therapy,5,6 which places them at greater risk of developing SREs and bone loss due to primary hormone therapy.4 Long-term androgen deprivation therapy (ADT) confers a significant decrease in bone mineral density (BMD),4 due to a decrease in the conversion of androgen to estrogen; estrogen plays a vital role in inhibiting bone resorption and sustaining BMD.7,8 Morote et al.9 observed significant bone loss in up to half the number of patients treated with ADT for more than 5 years, and duration of ADT correlated with a decline in BMD and an increase in the relative risk of hip fractures.
Although medical advances in the treatment of advanced prostate cancer have prolonged life expectancy, most patients may develop bone metastases resulting in significant skeletal complications.2 Moreover, the relatively long survival time when compared to other malignancies may increase the incidence of SREs, which significantly reduce quality of life in patients with prostate cancer.10
Zoledronic acid is a third generation bisphosphonate containing a heterocyclic imidazole group on the side chain. It is 40 to 850 times more potent than pamidronate, a pyrophosphate derivative that used to be the sole agent available to treat skeletal complications related to cancer. In Europe and the US it is the only drug approved for prostate cancer with bone metastases and is used for the relief of bone pain associated with cancer metastasized to bone, as well as hypercalcemia of malignancy. Zoledronic acid is the most potent inhibitor of bone resorption among the bisphosphonates available to date.11-13
This study, the first of its kind in Korea, has been conducted to evaluate the short-term safety and efficacy of zoledronic acid in patients with hormone-refractory prostate cancer with bone metastases.
PATIENTS AND METHODS
Patients
Patients aged ≥ 18 years with histologically confirmed prostate cancer refractory to hormone therapy with bone metastases were enrolled. Hormone-refractory prostate cancer was defined as presence of biochemical or clinical progression despite serum testosterone levels closer to castration levels, and evidence of persistent progression after discontinuation of anti-androgen agents for at least 4 weeks. Patients were also required to have ≥ 1 bone lesions associated with prostate cancer, bone metastases as assessed by simple bone radiography or bone scan, and Eastern Cooperative Oncology Group (ECOG) performance status score of ≤ 2. The Institutional Review Board at each participating hospital approved the study protocol and patients signed a written consent form.
Exclusion criteria included patients with abnormal renal function (serum creatinine levels 1.5 times greater than the upper normal limit or creatinine clearance < 60 mL/min), corrected serum calcium concentration < 8.0 mg/dL (< 2.0 mmol/L) or ≥ 12 mg/dL (≥ 3.00 mmol/L), clinical symptoms of brain metastasis, or a history of allergy to zoledronic acid or other bisphosphonates. Patients were also excluded if they had received any other investigational study drugs within 30 days prior to the first infusion of zoledronic acid, had received radiation therapy to bone within 3 months before the first infusion of zoledronic acid, or had received a bisphosphonate for the treatment of other diseases such as osteoporosis within 2 years before the start of the study.
Study design
This was a prospective, multi-centre, open-label study. Enrolled patients received up to six infusions of zoledronic acid (4 mg, diluted in 100 mL calcium-free solution e.g. 0.9% w/v sodium chloride), as a 15-minute infusion every 3 - 4 weeks. All patients were given a calcium supplement (500 - 600 mg) and multi-vitamins containing vitamin D (400 - 500 IU) once daily.
Safety assessments
To evaluate kidney function, serum creatinine levels were measured prior to each infusion. Serum creatinine levels were measured pre- and post-dose. Adverse events (AEs) were monitored throughout the study and were evaluated according to incidence and severity. Any follow-up action taken to treat AEs was recorded by the treating physician. The severity of an AE was assessed based on Common Terminology Criteria for Adverse Events (National Cancer Institute v3.0) using a grading scale of 0 (no adverse event), to 5 (death related to an adverse event),14 and relationship to the study drug.
Efficacy assessments
Pain assessments
Bone pain was assessed using the brief pain inventory (BPI) short form.15 A composite pain score was used, calculated as a mean of the scores for questions 3, 4, 5 and 6. Changes in the composite pain scores pre- and post-treatment were determined and statistical analysis performed using a linear mixed model.
Skeletal-related events (SREs)
SREs were defined as pathological bone fractures, spinal cord compression, surgery or radiotherapy to bone, or hypercalcemia. New cases of pathological bone fractures involving bones other than vertebrae that were secondary to minor injury were detected by patient's self-report and confirmed by radiography. Radiography was mandatory at the screening visit and the final visit, and was also performed whenever clinically indicated. Hypercalcemia was defined as a corrected serum calcium level of ≥ 12 mg/dL (≥ 3.00 mmol/L), or a corrected serum calcium level < 12 mg/dL (< 3.00 mmol/L) with the presence of symptoms, or a need for treatment other than hydration. SREs were evaluated at each visit.
Quality of life assessments
The Functional Assessment of Cancer Therapy-General (FACT-G) questionnaire was administered at screening, at the fourth infusion of zoledronic acid and at the final visit.16 Quality of life scores representing four questionnaire subscales were evaluated, as well as changes in scores for each subscale. Quality of life scores at the fourth infusion of study drug and at the final visit were compared with those at screening using a paired t-test. The higher FACT-G scores the better the patient's quality of life.
Analgesic scores
Analgesic use was recorded pre- and post-zoledronic acid infusion (at screening, at each infusion, and at the final visit). Analgesic scores were classified into four categories of analgesics, 'minor analgesics (eg, aspirin or acetaminophen)' (score 1), 'tranquilizers' (score 2), 'mild opioids (eg, oxycodone)' (score 3), and 'strong opioids (eg, morphine)' (score 4).17 An analgesic score of '0' was assigned when no analgesic was administered, and a higher score obtained when two or more categories of analgesics were administered. At each visit analgesic scores were calculated by determining analgesics used since the last visit. A non-parametric, paired 2-sample Wilcoxon analysis was used to analyze changes in analgesic scores before and after treatment. The statistical analyses in this study were performed using SAS Version 8.0.
RESULTS
A total of 19 patients were eligible for the study. All patients received at least one dose of zoledronic acid and were included in the safety analysis. Fifteen (78.9 %) patients who completed the study were included in the efficacy analysis. Four patients were excluded from the efficacy analysis for the following reasons: withdrawal of informed consent (2 patients); study protocol violation (1 patient); and adverse event, Grade 3 myalgia related to study drug (1 patient).
Mean age of patients was 67.3 ± 9.6 years (range 46.3-85.6 years), the duration of prostate cancer (time from diagnosis of prostate cancer to first infusion of zoledronic acid) was 32.6 ± 24.6 months (range 7 - 117 months), and the duration of bone metastases (time from diagnosis of bone metastases to the first infusion of zoledronic acid) was 27.6 ± 26.5 months (range 0 - 117 months). The time from diagnosis of hormone refractory prostate cancer to the first infusion of zoledronic acid was 7.5 ± 9.1 months (range 0 - 26 months). During the study, 10 (52.6%) patients received ADT and 9 (47.4%) patients received ADT in conjunction with cytotoxic chemotherapy. Mean number of zoledronic acid infusions administered was 5.3 ± 1.5 (range 1 - 6).
Safety analysis
Changes in serum creatinine levels from screening to final visit increased by < 0.5 mg/dL in 18 (94.7%) patients. For one patient serum creatinine was elevated by 0.5 - 1.0 mg/dl after completion of the study, but returned to within the normal range during follow-up.
The 11 AEs with a possible relationship to study drug occurred in 8 (42.1%) patients. No AEs were recorded with a 'probable' or 'definite' relationship to study drug. These AEs included musculoskeletal disorders, such as arthralgia, myalgia or back pain (9 AEs, grades 1, 2, and 3 in 6 patients), and systemic disorders, such as fever or malaise (2 AEs, grade 2 in 2 patients). Of these 8 patients, permanent discontinuation of study drug was required for 1 patient (Grade 3 myalgia), 3 patients were managed with concomitant medication, and no intervention was required for the other 4 patients.
Efficacy analysis
Efficacy was assessed in 15 patients who completed the study. There was no statistically significant difference between the composite pain scores at screening and at each infusion. Among patients who had a composite pain score > 0 at the first infusion of zoledronic acid, there was a trend towards a decrease in pain after the third infusion (Fig. 1), but this was not statistically significant.
Fig. 1.
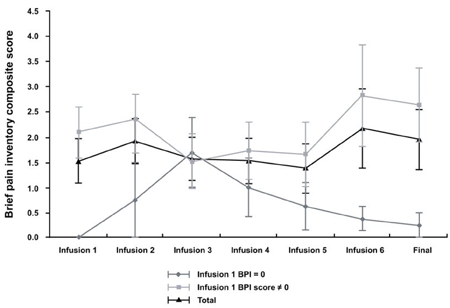
Change of brief pain inventory composite scores.
SREs prior to zoledronic acid infusion were reported in 3 (20.0%) patients, but none of the patients developed new SREs.
There was a trend towards a decrease in FACT-G overall scores but this was not statistically significant. When subscales at the first infusion of zoledronic acid were compared with those at the final infusion, physical (p = 0.042) and functional (p = 0.017) subscales showed a statistically significant decrease. Changes in social or familial and the emotional subscales were not statistically significant (Table 1).
Table 1.
Functional Assessment of Cancer Therapy-General (FACT-G) Scores

SD, standard deviation.
The proportion of patients using analgesics increased from 26.3% at screening to 35.1% during follow-up, but there was a trend towards a decrease in the use of narcotic analgesics (Table 2). When analgesic scores at the time of screening were compared with those at each infusion, there was no significant difference. For patients who had scores > 0 at the time of screening, there was a trend towards a decrease in analgesic score after the second infusion, but this was not statistically significant (Fig. 2).
Table 2.
The Type of Pain Medication Administered During Treatment

Fig. 2.
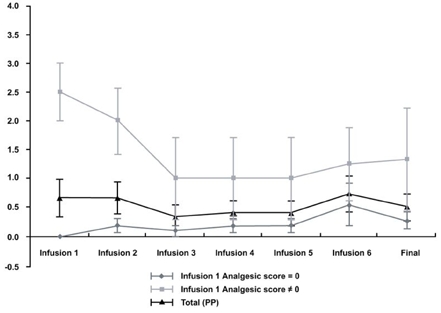
Change of mean analgesic scores.
DISCUSSION
Bone lesions in patients with prostate cancer and bone metastases are characterized by osteoblastic lesions but are also associated with osteolytic activity resulting in a drastic decline in bone remodeling and significant bone loss.18 Escalated osteoclast activity combined with osteoblastic lesions justify the use of bisphosphonates, which are potent inhibitors of osteoclasts.19
Previous studies have demonstrated that bisphosphonates such as etidronate, clodronate and pamidronate provide a decrease in bone pain, and in the use of analgesics for patients with hormone-refractory prostate cancer and bone metastases.20 However, these studies were not placebo-controlled, and because of the transient effects of the bisphosphonates, no firm conclusions could be drawn. Moreover, controlled studies with clodronate and pamidronate have not been able to demonstrate a statistically significant decrease in pain, or in the use of analgesics.20
Conversely, a large placebo-controlled study evaluating the efficacy of zoledronic acid in patients with hormone-refractory prostate cancer and bone metastases demonstrated that the treatment group had a significant decrease in bone pain and SREs, such as pathological bone fractures, spinal cord compression and bone radiotherapy compared with the placebo group.21 BPI composite pain scores increased in both the placebo and treatment groups, but this increase was significantly less in the treatment group, and its effect was sustained for up to 24 months.19 SREs occurred in 38% of patients in the treatment group and 49% in the placebo group with a significant decrease of 22%. The median time to the onset of SREs was 321 days in the placebo group and 488 days in the treatment group indicating a delay of nearly 5 months in the onset of SREs for patients who received zoledronic acid. Zoledronic acid was, therefore, considered to play an important role in stabilizing bones by delaying accumulation of unstable bones.11-13,22,23
Safety analyses in cancer patients with bone metastases have demonstrated the stability of zoledronic acid in blood and urine, with no significant changes in estimated creatinine clearance.24,25 Our study also showed that any change in serum creatinine level occurred within an acceptable range, with no clinical impact. A 15-minute intravenous infusion of 4 mg zoledronic acid is superior in terms of safety and efficacy, and supplementation with calcium and vitamin D is recommended.10,26,27 All patients in our study were supplemented with calcium and vitamin D, and no side effects due to hypocalcemia were recorded.
Adverse events occurred in 14 (73.7%) patients. The majority (64.9%) of AEs were mild. Eleven AEs in 8 (42.1%) patients were classed as having a 'possible' relationship to zoledronic acid. The most common AEs related to zoledronic acid are known to be fatigue, anemia, myalgia, fever and edema on the lower extremities.26 During the study, 9 AEs (musculoskeletal disorders), such as arthralgia, myalgia or back pain and 2 AEs (systemic disorders), such as fever or malaise were recorded. Meanwhile, the long-term side-effect and possible complications, such as osteonecrosis of jaw, have not been fully evaluated in this study.28
The composite pain scores measured by BPI questionnaire, and quality of life assessments (FACT-G questionnaire) did not show statistically significant changes, but there was a trend towards a decrease in the use of narcotic analgesics. There was, however, no significant difference in analgesic scores. A subgroup analysis of patients with an analgesic score and pain score > 0 at the time of screening, showed a trend towards improvement for later infusions. However, given the study limitations, such as small patient number, an uncontrolled study design and short follow-up period, these efficacy results need to be confirmed with more robust studies. This first prospective study evaluating the safety of zoledronic acid in patients with hormone-refractory prostate cancer in Korea is, however, noteworthy in providing preliminary safety information.
The 3rd International Consultation on Prostate Cancer developed a prostate cancer treatment algorithm that supports the use of zoledronic acid at first evidence of bone metastases.29 Although still controversial, it has been noted that zoledronic acid stabilizes bones through an increase in BMD as well as a delay of a mean time to the onset of SREs, and prevents bone loss in patients receiving ADT.30 However, further studies are needed to determine whether early administration of zoledronic acid enhances the effects of ADT or increases the survival rate in prostate cancer patients with metastases. Promising results, examining these issues, are anticipated from a large clinical study currently underway.
In conclusion, Zoledronic acid, administered as a 15-minute intravenous infusion in this study demonstrated an acceptable and well-known safety profile in patients with hormone refractory prostate cancer with bone metastases. However, a large, prospective, controlled study is necessary to substantiate the efficacy of zoledronic acid in the prevention of SREs, alleviation of pain and improvement in quality of life.
Table 3.
Functional Assessment of Cancer Therapy-General (FACT-G) Scores

SD, standard deviation.
Table 4.
The Type of Pain Medication Administered During Treatment

Table 5.
Mean Analgesic Scores on Each Infusion Period

Footnotes
This clinical trial was sponsored by Novartis Korea. The authors conducted the trial under an agreement with Novartis Korea, and do not have any other affiliations with Novartis Korea.
References
- 1.Ferlay J, Bray F, Pisani P, Parkin DM. GLOBOCAN 2000: cancer incidence, mortality and prevalence worldwide. version 1.0. Lyon: IARC Press; 2001. (IARC Cancer Base no. 5). [Google Scholar]
- 2.Coleman RE. Metastatic bone disease: clinical features, pathophysiology and treatment strategies. Cancer Treat Rev. 2001;27:165–176. doi: 10.1053/ctrv.2000.0210. [DOI] [PubMed] [Google Scholar]
- 3.Siddiqui NA, Shetty KR, Duthie EH., Jr Osteoporosis in older men: discovering when and how to treat it. Geriatrics. 1999;54:20–22. 27–28, 30. passim. [PubMed] [Google Scholar]
- 4.Smith MR. Diagnosis and management of treatment-related osteoporosis in men with prostate carcinoma. Cancer. 2003;97(3 Suppl):789–795. doi: 10.1002/cncr.11149. [DOI] [PubMed] [Google Scholar]
- 5.Smith MR, McGovern FJ, Fallon MA, Schoenfeld D, Kantoff PW, Finkelstein JS. Low bone mineral density in hormone-naïve men with prostate carcinoma. Cancer. 2001;91:2238–2245. [PubMed] [Google Scholar]
- 6.Wei JT, Gross M, Jaffe CA, Gravlin K, Lahaie M, Faerber GJ, et al. Androgen deprivation therapy for prostate cancer results in significant loss of bone density. Urology. 1999;54:607–611. doi: 10.1016/s0090-4295(99)00301-5. [DOI] [PubMed] [Google Scholar]
- 7.Khosla S, Melton LJ, 3rd, Atkinson EJ, O'Fallon WM. Relationship of serum sex steroid levels to longitudinal changes in bone density in young versus elderly men. J Clin Endocrinol Metab. 2001;86:3555–3561. doi: 10.1210/jcem.86.8.7736. [DOI] [PubMed] [Google Scholar]
- 8.Smith MR. Treatment-related osteoporosis in men with prostate cancer. Clin Cancer Res. 2006;12:6315S–6319S. doi: 10.1158/1078-0432.CCR-06-0846. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Morote J, Martinez E, Trilla E, Esquena S, Abascal JM, Encabo G, et al. Osteoporosis during continuous androgen deprivation: influence of the modality and length of treatment. Eur Urol. 2003;44:661–665. doi: 10.1016/s0302-2838(03)00379-8. [DOI] [PubMed] [Google Scholar]
- 10.Weinfurt KP, Li Y, Castel LD, Saad F, Timbie JW, Glendenning GA, et al. The significance of skeletal-related events for the health-related quality of life of patients with metastatic prostate cancer. Ann Oncol. 2005;16:579–584. doi: 10.1093/annonc/mdi122. [DOI] [PubMed] [Google Scholar]
- 11.Cheer SM, Noble S. Zoledronic acid. Drugs. 2001;61:799–806. doi: 10.2165/00003495-200161060-00010. [DOI] [PubMed] [Google Scholar]
- 12.Gucalp R, Ritch P, Wiernik PH, Sarma PR, Keller A, Richman SP, et al. Comparative study of pamidronate disodium and etidronate disodium in the treatment of cancer-related hypercalcemia. J Clin Oncol. 1992;10:134–142. doi: 10.1200/JCO.1992.10.1.134. [DOI] [PubMed] [Google Scholar]
- 13.Ralston SH, Gallacher SJ, Patel U, Dryburgh FJ, Fraser WD, Cowan RA, et al. Comparison of three intravenous bisphosphonates in cancer-associated hypercalcaemia. Lancet. 1989;2:1180–1182. doi: 10.1016/s0140-6736(89)91791-1. [DOI] [PubMed] [Google Scholar]
- 14.Cancer Therapy Evaluation Program, Common Terminology Criteria for Adverse Events, Version 3.0. DCTC, NCI, NIH, DHHS; 2003. Mar 31, ( http://ctep.cancer.gov) Publish Date: August 9, 2006. [Google Scholar]
- 15.Cleeland CS, Ryan KM. Pain assessment: global use of the Brief Pain Inventory. Ann Acad Med Singapore. 1994;23:129–138. [PubMed] [Google Scholar]
- 16.Cella DF, Tulsky DS, Gray G, Sarafian B, Linn E, Bonomi A, et al. The Functional Assessment of Cancer Therapy scale: development and validation of the general measure. J Clin Oncol. 1993;11:570–579. doi: 10.1200/JCO.1993.11.3.570. [DOI] [PubMed] [Google Scholar]
- 17.Tong D, Gillick L, Hendrickson FR. The palliation of symptomatic osseous metastases: final results of the Study by the Radiation Therapy Oncology Group. Cancer. 1982;50:893–899. doi: 10.1002/1097-0142(19820901)50:5<893::aid-cncr2820500515>3.0.co;2-y. [DOI] [PubMed] [Google Scholar]
- 18.Mundy GR. Metastasis to bone: causes, consequences and therapeutic opportunities. Nat Rev Cancer. 2002;2:584–593. doi: 10.1038/nrc867. [DOI] [PubMed] [Google Scholar]
- 19.Saad F. Preventing bone complications in patients with prostate cancer: the emerging role of zoledronic acid. Eur Urol Suppl. 2004;3:25–33. [Google Scholar]
- 20.Saad F, Karakiewicz P, Perrotte P. The role of bisphosphonates in hormone-refractory prostate cancer. World J Urol. 2005;23:14–18. doi: 10.1007/s00345-004-0472-2. [DOI] [PubMed] [Google Scholar]
- 21.Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L, et al. Long-term efficacy of zoledronic acid for the prevention of skeletal complications in patients with metastatic hormone-refractory prostate cancer. J Natl Cancer Inst. 2004;96:879–882. doi: 10.1093/jnci/djh141. [DOI] [PubMed] [Google Scholar]
- 22.Body JJ. Clinical research update: zoledronate. Cancer. 1997;80(8 Suppl):1699–1701. doi: 10.1002/(sici)1097-0142(19971015)80:8+<1699::aid-cncr23>3.3.co;2-a. [DOI] [PubMed] [Google Scholar]
- 23.Lipton A, Berenson JR. Bisphosphonate treatment of lytic bone metastases. Drugs Aging. 1999;14:241–246. doi: 10.2165/00002512-199914040-00001. [DOI] [PubMed] [Google Scholar]
- 24.Chen T, Berenson J, Vescio R, Swift R, Gilchick A, Goodin S, et al. Pharmacokinetics and pharmacodynamics of zoledronic acid in cancer patients with bone metastases. J Clin Pharmacol. 2002;42:1228–1236. doi: 10.1177/009127002762491316. [DOI] [PubMed] [Google Scholar]
- 25.Guarneri V, Donati S, Nicolini M, Giovannelli S, D'Amico R, Conte PF. Renal safety and efficacy of i.v. bisphosphonates in patients with skeletal metastases treated for up to 10 Years. Oncologist. 2005;10:842–848. doi: 10.1634/theoncologist.10-10-842. [DOI] [PubMed] [Google Scholar]
- 26.Saad F, Gleason DM, Murray R, Tchekmedyian S, Venner P, Lacombe L, et al. A randomized, placebo-controlled trial of zoledronic acid in patients with hormone-refractory metastatic prostate carcinoma. J Natl Cancer Inst. 2002;94:1458–1468. doi: 10.1093/jnci/94.19.1458. [DOI] [PubMed] [Google Scholar]
- 27.Saad F, Olsson C, Schulman CC. Skeletal morbidity in men with prostate cancer: quality-of-life considerations throughout the continuum of care. Eur Urol. 2004;46:731–740. doi: 10.1016/j.eururo.2004.08.016. [DOI] [PubMed] [Google Scholar]
- 28.Migliorati CA, Siegel MA, Elting LS. Bisphosphonate-associated osteonecrosis: a long-term complication of bisphosphonate treatment. Lancet Oncol. 2006;7:508–514. doi: 10.1016/S1470-2045(06)70726-4. [DOI] [PubMed] [Google Scholar]
- 29.Carroll PR, Altwein J, Brawley O, Cockett A, Cooperberg M, Hirao Y, et al. Management of disseminated prostate cancer. In: Denis L, Bartsch G, Khoury S, Murai M, Partin A, editors. Prostate Cancer: 3rd International Consultation on Prostate Cancer-Paris. Paris: Health publications; 2003. pp. 251–284. [Google Scholar]
- 30.Ryan CW, Huo D, Demers LM, Beer TM, Lacerna LV. Zoledronic acid initiated during the first year of androgen deprivation therapy increases bone mineral density in patients with prostate cancer. J Urol. 2006;176:972–978. doi: 10.1016/j.juro.2006.04.078. [DOI] [PubMed] [Google Scholar]