

Abstract
The co-occurrence of conduct problems (CP) and depressive symptoms (DS) is an important topic in developmental psychopathology; however, research in this area is still in early stages. We used data from a school-based longitudinal sample of 2,453 adolescents with 5 waves from grade 6 to 9 to examine the prevalence, etiology, and consequences of the co-occurrence of CP and DS. General Growth Mixture Modeling (GGMM) was applied to obtain findings consistent with a developmental person-centered view. As hypothesized, a small proportion of boys (8.8%) and girls (3.7%) reported high in both CP and DS over time. Among the adolescents with the highest level of CP, only 6.3% boys and 6.0% girls experienced the highest level of DS. However, among those with the highest level of DS, 42.9% boys and 10.2% girls reported the highest level of CP, indicating increased risk of depressed boys for CP. Psychosocial and family factors were identified as vulnerable precursors to the co-occurrence of CP and DS, a finding in line with the multiple domain risk model for CP and the transactional model for DS. The study also found that adolescents with co-occurrence of CP and DS were more similar to those with ‘pure’ DS than those with ‘pure’ CP in academic adjustment at 9th grade.
The co-occurrence of adolescent conduct problems (CP) and depressive symptoms (DS) has been the focus in a number of studies (Beyers & Leober 2003; Capaldi, 1991, 1992; Capaldi & Stoolmiller 1999; Compton, et al. 2003; Harrington, Rutter & Fombonne, 1996; Lansford et al., 2006; Ruchkin, et al, 2006; Rutter, 1989; Wiesner, Kim, & Capaldi, 2005). A central thesis in these studies is how and why the two problem behaviors with qualitatively different symptoms are associated in adolescence. With CP and DS indicating externalizing and internalizing behavior problems, respectively, it is of theoretical and practical interest to examine the extent of co-occurrence of these two dimensions of problem behaviors. One interpretation is that noxious behavior such as bullying and destroying property cause social rejection, and in turn, leads to vulnerability to depression (Capaldi, 1991). Depression, however, does not seem a likely cause of CP. Another explanation is that CP and DS may share a similar etiology where the same precursors, such as childhood abuse, low social competences, low parent knowledge (Lansford et al., 2006), or high parent-child conflict (Rutter, 1989; Formosa, Gonzales & Aiken, 2000) lead to the emergence and maintenance of both CP and DS. Harrington, Rutter & Fombonne (1996) suggested another interpretation that depression may be heterogeneous and CP could be more likely to expresswith certain types of DS. Researchers are also interested in the consequences of the co-occurrence of CP and DS in adolescents. For example, Capaldi & Stoolmiller (1999) found that social and academic maladjustment were more likely to result in association with the co-occurrence of CP and DS. However, Harrington, Rutter & Fombonne (1996) reported that adolescents with comorbid CP and depression had lower risk of recurrence of major depression later compared with youths with ‘pure’ depression. A review of the literature shows that many important issues in this area are still in the early stages of research and previous studies are mostly based on at-risk, clinical, male-only, or cross-sectional samples. Findings from these studies are naturally limited by sample selection, design, and methodology. Longitudinal studies with non-clinical samples including both boys and girls on the co-occurrence of CP and DS are rare.
This study examined issues related to the co-occurrence of CP and DS in a school-based sample of 2,435 participants measured in 5 waves from grade 6 to 9. We applied General Growth Mixture Modeling (GGMM, Muthen, 2004) to identify subgroups with distinctive pathways of CP and DS during early adolescence. The conditional distributions of CP and DS were obtained from predicted memberships to identify adolescents with both high CP and DS. We sought to examine demographical, psychosocial, and parenting factors as precursors. Academic achievement at 9th grade was compared among the groups to determine the consequences of the co-occurrence of CP and DS. Because of the possible existence of population heterogeneity in the pathways of CP and DS, this person-centered approach is likely to capture the differential effects of vulnerable factors on subgroups. Gender difference in CP and DS has been consistently documented in literature and it was a major consideration in this study.
The tendency for CP and DS to co-occur among adolescents both in clinical and non-clinical samples has been reported in a number of studies. In a summary of literature review, Capaldi (1991) reported that approximately one-third of the children diagnosed as either conduct disorders or depressions might be diagnosed as having both syndromes. Among Capaldi's (1991) non-clinical sample of 203 at-risk boys, using the 70th percentile as the cutoff for CP and DS measures, about 13% of the boys were classified as high in both CP and DS. With a large sample from the Minnesota Twin Family Study, Marmorstein and Iacono (2003) documented that about 15% to 25% of youths with conduct disorder also had major depression, and approximately 15% to 35% depressed youths also had conduct disorder. In a more recent study on the prevalence of DS and its associated psychopathology, Ruchkin et al. (2006) reported that among an urban community sample of 1,343 adolescents from 14 to 17 years old, 13.1% boys and 17.9% girls had clinical levels of DS. Among those depressed boys and girls, 6.93% boys and 4.23% girls also had severe antisocial behaviors including starting a fist fight, participating in a gain fight, hurting someone badly or carrying a knife to school. In non-depressed adolescents, only 4.66% boys and 2.46% girls reported severe antisocial behaviors. Clearly, co-occurrence of CP and DS exists in both clinical and non-clinical adolescent populations with clinical populations having considerably higher prevalence than non-clinical populations.
Etiology of CP and DS
A great number of studies have examined the etiology that may contribute to the development of adolescent CP and DS; however most studies consider CP and DS as an isolated problem behavior rather than a co-occurring outcome. A few studies sought to identify the vulnerable or protective factors as shared precursors to the development of CP and DS. Probably the most comprehensive study on the co-occurrence of adolescent CP and DS was conducted by Capaldi and colleagues (Capaldi, 1991; Capaldi, 1992; Capaldi & Stoolmiller, 1999). This longitudinal study used an at-risk sample of approximately 200 boys in the Oregon Youth Study with data collected at 6th, 8th and 12th grade. The study examined the common etiology, developmental stability and consequences of the co-occurrence of CP and DS in youth. A failure model was proposed that noxious conduct would result in poor social and academic adjustment, and in turn, maladjustment would cause more depression in adolescents. The study reported that lower SES, parent substance use, parent antisocial behavior, parent depression and lower parent monitoring were significantly related to elevated CP and DS in adolescent boys. Both CP and DS were found stable into young adulthood with worse social adjustment as predicted.
Using a community sample of 585 children from kindergarten to 8th Grade, Lansford et al. (2006) examined risk and protective factors that may alter the trajectories of internalizing and externalizing problem behaviors. The study reported that being African American, being male, low social competence, low SES, low parent monitoring, and low parent knowledge were associated with higher levels of externalizing problems over time. Low social competence, low SES and low proactive parenting were found to be related to internalizing problems.
Certain family characteristics and parenting practices have also been identified as risk precursors that may lead to both high in adolescent CP and DS. Rutter (1989) concluded that CP and depression may share common determinants such as neglected and disorganized parenting. Campton et al. (2003) reported that family interaction styles such as coercion may contribute to both CP and DS in adolescents. Using a high-risk sample of 240 kindergarten children, Hollenstein, Stoolmiller and Synder (2004) found that rigidity in parent-child interaction may be associated with the development of both externalizing and internalizing behavior problems in children.
Association with deviate peers has been robustly related to the emergence and maintenance of child and adolescent CP (e.g., Moffitt, Rutter, & Silva, 2001; Synder, et al. 2005). A few studies have also identified that peer influence was related to adolescent depression (e.g., Allen, Porter & McFarland, 2006; Gutman & Sameroff, 2004). Using a longitudinal sample of 372 families, Gutmana & Sameroff (2004) found that although the multiple settings influencing adolescent depression were gender specific, peer variables were significant factors related to both male and female adolescents. Allen, Porter & McFarland (2006) used a lab-based assessment to examine the possible consequences of susceptibility to peer influences. The study concluded that susceptibility to peer influences from close friends was related to a broad range of behavior problems including both depression and externalizing behavior problems.
To better understand the etiology of the co-occurrence of CP and DS, we sought to adopt a developmental perspective (Cicchetti and Toth, 1998) considering the onset and maintenance of the co-occurring CP and DS in a broader developmental context. This transactional model integrates multiple diverse factors including biological, social and psychological variables with an emphasis on personal adaptation to the environment over the developmental process. Consistent with this perspective, a vulnerable factor needs to be examined simultaneously with the contextual features that may exist with the factor. Ciccehetti, Rogosch and Toth (1998) observed that offspring of depressed parents were at increased risk for behavior problems; however, the researchers observed that a substantial number of children with depressed caregivers showed no evidence of behavior dysfunction. A series of contextual risk features including social support, marital quality, and family conflict were identified and the study found that not all depressed families had equal amount of these contextual risks. The contextual risks were found to be significant mediators between maternal depression and child behavior problems.
In examining correlates of child CP, Greenberg, Speltz, Deklyen & Jones (2001) emphasized the multiple risk factor model based on the rationale that it was unlikely that any single risk factor was sufficient to predict child CP. The study evaluated four domains of possible correlates of child CP: vulnerable child characteristics, poor parenting practices, insecure attachment, and adverse family environment. It was found that when three or more domains were present, the clinical status of child CP was dramatically increased. However, no specific domain was found to be either necessary or sufficient for clinical case of child CP. Consistent with the multiple domain model for CP and the transactional model for DS, we sought to include a variety of factors to examine the etiology of co-occurrence of CP and DS. Based on the findings that CP or DS is not likely to be caused by a single precursor, we had no intention to identify a certain risk factor that was responsible for both CP and DS.
Consequences of Co-occurrence of Adolescent CP and DS
The consequences of co-occurrence in adolescent CP and DS have been examined by a number of studies (Capaldi, 1991; Capaldi & Stoolmiller, 1999; Harrington, Rutter & Fombonne, 1996; Marmorstein & Iacono, 2003). As hypothesized, Capaldi (1991) reported that the boys with elevated CP and DS showed poor academic adjustment compared to the boys with low CP and DS. However, from the same sample with follow-up measures at 12th grade, Capaldi and Stoolmiller (1999) reported that those boys with elevated CP and DS during early adolescence did not show increased difficulties in any one adverse outcome at 12th grade compared with boys with either CP only or DS only at 8th grade. It seems that over time, co-occurrence of CP and DS does not increase adverse consequences compared to those with ‘pure’ CP or ‘pure’ DS.
Similar finding was also reported by Harrington, Rutter and Formonne (1996). The study reported that youths who were higher in both CP and DS showed lower risk of recurrence of major depression at a later time compared to adolescents with only DS. Interpretation to this seemingly paradoxical finding was that the maladaptive functioning associated with one problem behavior may be attenuated by the presence of the other disorder. However, a recent study by Marmorstein and Iacono (2003) did not replicate this counterintuitive finding. Using a sample of adolescents with data from the Minnesota Twin Family Study, the researchers reported that the co-occurrence of conduct disorder and major depression was significantly associated with difficulties in a variety of important domains of functioning, including school success, substance dependence, peer relationship, and earlier age at first sexual intercourse. Clearly, further studies are needed to clarify controversial issues in this research area.
Hypotheses
We had multiple hypotheses in the present study. Based on consistent findings of gender differences in CP and DS (e.g., Ciccchetti & Toth, 1998; Cole et al. 1999), we first hypothesized that boys would report higher levels of CP, while girls would experience higher levels of DS during adolescence. Harrington, Rutter & Fombonne (1996) pointed out that the prevalence of depression as a syndrome in clinical samples would increase during adolescence but depression as a mood in epidemiological samples would reach a maximum level around age 14 and then decrease. Since we had a school-based, non-clinical sample, we expected that the trajectories for DS would be nonlinear for both boys and girls. The levels of CP were expected to correlate with the levels of DS; therefore we expected that the trajectories of CP would show similar shapes to the trajectories of DS.
The second hypothesis was related to the estimation of conditional distributions of CP and DS in population. We hypothesized that a majority of adolescents in a non-clinical sample would experience low levels of CP and DS over time. We also expected that the proportion of adolescents who had co-occuring CP and DS would be relatively larger for boys than for girls. We also expected that of adolescents who remained high over time on one problem, only a small proportion would remain high over time on the other problem.
In line with the multiple factor model (e.g., Greenburg et al., 1993) and the transactional model (Cicchetti & Toth, 1998), our third hypothesis was that a variety of factors measured at 6th grade would significantly differentiate the group high in both CP and DS from the other groups. Based on previous findings, we selected SES, problem peers, child social competence, parent-child conflict and parent knowledge to represent different domains as covariates. We expected that most of these covariates would be significant predictors, but would have different patterns for boys and girls. To replicate the findings that adolescents with higher CP and DS had poorest academic skills (e.g., Capaldi, 1991), we hypothesized that academic failure rate and average GPA at 9th grade would be significantly lower for adolescents with co-occurring CP and DS.
Methods
Participants
The 2,453 adolescents in the present study were from two cohorts participating in a school-based intervention program (the Going Places Program, Simons-Morton, et. al., 2005) targeting the prevention of adolescent substance use, aggression, and antisocial behavior. Participants were recruited from seven middle schools in a Maryland school district starting from the 1996 school years, and the schools were randomly assigned to treatment (3 schools) and control (4 schools) conditions. Participants in the treatment schools were exposed to the Going Places Program, which included parent education in the form of materials sent home, school environment improvement, and social skills curriculum consisted of 18 class sessions in sixth grade, 10 sessions in seventh grade, and 6 sessions in eighth grade. Participants responded to surveys 5 times at the beginning and end of 6th grade, and again in the spring of 7thgrade, and in the fall of 8th, and 9th grades. The questionnaires consisted of background, substance use, peer and parent influence variables and psycho-social measures including depression and conduct problems.
The original sample included 2,969 students (72% white, 18% black, and 10% others) eligible to participate in baseline assessment. Special education students with reading problems were not included because a pilot study showed that these students were not able to provide reliable data. Parent consent was obtained in sixth grade and again before the ninth grade follow-up. The 2,651 (87.8%) eligible students provided consent by their parents in the 6th grade. Of these, 9 became ineligible during the study by failing a grade and 110 were newly classified as special education, leaving a sample of 2,532, of whom 79 moved out of the school district or missed multiple assessments, leaving a final sample of 2,453. Compared with the final sample, participants lost to follow up were significantly more likely to be black, live with only one parent, and to report drinking. Missing values in major outcomes (CP and SD) at each wave are presented in Table 1 for boys and girls separately. The missing values were treated as missing at random and MPlus (version 3, Muthen & Muthen 1998-2004), which offers maximum likelihood estimation based on the data with missing outcome values through the iterative EM algorithm, was used to handle the missing values in subsequent data analyses.
Table 1. Means, Standard Deviations and Sample Sizes of Conduct Problems and Depressive Symptoms for Boys and Girls at Five Waves.
| Conduct Problems | Depressive Symptoms | |||
|---|---|---|---|---|
| Boys | Girls | Boys | Girls | |
| Fall, 6th Grade | 1.44 (1.49) | 0.63 (1.14)** | 4.14 (3.05) | 4.11(2.99) |
| N = | 1,012 | 1,193 | 991 | 1169 |
| Spring, 6th Grade | 1.63 (1.56) | 0.94 (1.34)** | 4.59 (3.40) | 4.82 (3.39) |
| N = | 1,029 | 1,241 | 1,024 | 1,236 |
| Spring, 7th Grade | 1.77 (1.57) | 1.10 (1.41)** | 4.75 (3.49) | 5.01 (3.40) |
| N = | 1,086 | 1,275 | 1,079 | 1,270 |
| Fall, 8th Grade | 1.64 (1.60) | 1.12 (1.44)** | 4.55 (3.33) | 4.89 (3.55)* |
| N = | 1,028 | 1,245 | 1,011 | 1,233 |
| Fall, 9th Grade | 1.44 (1.56) | 1.04 (1.42)** | 3.95 (3.35) | 4.47 (3.34)** |
| N = | 799 | 1,010 | 796 | 1,010 |
p < 0.05,
p < 0.01.
Procedures
Questionnaires were administered in class and during make-up sessions. Two trained proctors administered data collection in classes of less than 30 students each. As required by the school district, teachers remained to manage the classroom but they were not involved in the conduct of the survey. To protect confidentiality, students completed and turned in a cover page that included name, survey identification number, birth date, and homeroom teacher's name that was kept separate from the questionnaires. The returned questionnaires had only an identification number matching the one on the cover page. The study protocol was approved by the Institutional Review Board, National Institute of Child Health and Human Development.
Measures
Background Variables
Participants responded to the questionnaires with demographic and contextual items including gender, race, mother's education, attendance of free lunch program, family structure, school attended, etc.
Conduct Problems
Conduct problems were assessed by an index of items asking how often in the past year the youth had been in a physical fight, hurt someone in a physical fight, bullied or picked on someone younger or weaker, carried a weapon, stole something from a person or store, or marked something with graffiti. Each item was rated on a 4 point scale with 0 = zero occurrence, 1 = one to two times, 2 = three to five times, and 4 = six or more times in the past 12 months. Reponses to the items were summed across the items to obtain the measure of CP. The average internal reliability across 5 waves of measurement was α = 0.75 for boys and α = 0.74 for girls.
Depressive Symptoms
Depressive symptoms were assessed using a subscale from the Weinberger Adjustment Inventory (Weinberger, 1991). These six items assessed the respondent's level of DS through items such as “I feel so down and unhappy that nothing makes me feel much better,” and “I get into such a bad mood that I feel like just sitting around and doing nothing.” Response categories were never, some of the time, most of the time, or always. Higher scores indicate greater levels of depression. Internal reliability was α = 0.77 at first assessment in fall 6th grade.
Social Competence
Social competence was assessed with 9 items developed consistent with the conceptualization of Harter (1982). The items addressed issues such as communication, conflict resolution, and problem solving. Response choices allowed students to indicate if they perceived items to be much harder, a little harder, a little easier, or much easier for them compared to others in their grade (α = 0.79). Higher scores indicate higher levels of social competence.
Problem Peers
Problem behaving friends were assessed by asking how many of the respondent's five closest friends participated in each of the problem behaviors including smoking, drinking, bullying, being disrespectful to teachers, fighting, cheating, lying to parents, and marking property with graffiti. The average score was used to indicate Problem Peers. We excluded friends engaged in smoking and drinking in the average to be consistent with CP as a major outcome in present study.
Parent Variables
We employed extensive pilot testing and factor analytic procedures to develop reliable student report measures of perceived parenting behavior (Simons-Morton, et al., 1999). Parental Knowledge included six items that focused on how much the parent knows (knows almost nothing, knows a little, knows a lot) about the teen's friends, activities, interests, health habits, free time, and school (α = .76). Parent-Child Conflict was assessed with four items adapted from Robin and Foster (1989), which asked to report about the following (strongly agree, agree, disagree, or strongly disagree): I have a parent or guardian who is hard to get along with; often makes me angry; gets angry at me almost every day; easily loses his/her temper with me (alpha = .82).
GPA and Academic Failure
Participant's academic grading at 9th grade on four subjects: Math, Science, language Arts and Social Studies with each scored from 1 to 5 was obtained from school records. GPA at 9th grade was calculated with the average score from the four subjects (from 1 to 5) subtracted by one resulting a range from 0 to 4. Academic Failure was a dummy variable derived from the average score (from 1 to 5) with an average score less than 2.5 was defined as failure. The overall failure rate in the sample is 7.74% (10.1% for boys and 6.0% for girls). The definition of academic failure in this study is subjective that was created to compare gender and subgroups differences besides GPA.
Analysis
Descriptive statistics for CP and DS as major outcomes at each wave were calculated and charted to display the overall changes for boys and girls. Simple correlations for the covariates with CP and DS measured at baseline were presented to show the bivaraite relationship at the beginning of the study. The method of General Growth Mixture Modeling (GGMM, Muthen, 2004) was applied to address the major research hypotheses of the study. Prior to fitting the mixture models, unconditional latent growth curve models (LGC model without covariates, e.g., Curran, 2000) were estimated with 5 repeated measures of CP and DS for boys and girls separately. The purpose of fitting the unconditional LGC model was to determine the shape of the trajectories and the variance in the growth factors that would provide guidelines in subsequent analyses. The overall fit indices for LGC model included the Comparative Fit Index (CFI), the Tucker-Lewis Index (TLI) and the Root Mean Square Error of Approximation (RMSEA) provided by MPlus (Muthen & Muthen 1998-2004). Most researchers regard a model acceptable if CFI and TLI are greater than 0.9. A model with an RMSEA less than 0.05 is regarded as a ‘good’ fit and an RMSEA less than 0.08 is ‘acceptable’ (McDonald & Ho, 2002).
The second step in the analysis was to fit conditional parallel processing LGC models (Muthen and Curran, 1997) to evaluate the association of CP and DS trajectories. The covariates were included in the model to evaluate the relative effects on growth factors (intercepts and slopes, see Figure 2). For curvilinear models, we applied the method of estimating factor loading by freeing a few time scores in the parallel processing model (Bollen & Curran, 2006, p. 98). With only two growth factors specified (intercept and slope), this method facilitates the interpretation of path coefficients leading from the covariates to the growth factors, especially to the slopes. The conditional models for boys and girls were estimated in one multi-group model for statistical comparisons across gender. A major purpose of conducting this traditional variable-centered method was to evaluate the relation between the changes of CP and DS over time, which was indicated by the covariance between the two slopes. The intervention treatment was included in the model as a covariate to statistically control the effects, although previous evaluation of the Going Places program did not show significant treatment effects on the change of CP or DS (Simons-Morton, et al., 2005).
The final model for GGMM was based on the conditional parallel process LGC model by adding two latent categorical variable, one for CP heterogeneous subgroups and one for DS subgroups, and academic failure at 9th grade was specified as the distal outcome (see Figure 3). The model with the best number of subgroups was determined by the Bayesian Information Criteria (BIC) and AIC (Muthen 2004). A smaller value of BIC or AIC indicates a better fit model. The variances in the growth factors were permitted to vary across the trajectory groups in GGMM estimation. Graphs of observed trajectories were displayed to help understanding the changes and the variances in groups over time. MPlus version 3 (Muthen and Muthen, 2004) was used for modeling and handling the missing values that were assumed missing-at-random (MAR, Little and Ribin, 2002) with EM algorithm. The mixture modeling process was conducted for boys and girls separately.
Results
Developmental Pathways for CP and DS
Descriptive statistics for CP and DS at each wave and statistical comparisons between boys and girls are shown in Table 1. Based on observed means of CP and DS, trajectories showing levels of CP and DS for boys (N = 1,120) and girls (N = 1,333) are presented in Figure 1. As hypothesized, boys reported significantly (p < 0.01) higher level of CP at each time point relative to girls, but the difference began to narrow starting at spring 7th grade. CP increased for both boys and girls starting from the beginning of 6th grade to the end of 7th grade and then leveled off among girls and slightly declined among boys. As shown in Figure 1, the levels of SD at 6th grade were similar among boys and girls. It was after 6th grade that the difference in DS between boys and girls started to appear. For both boys and girls the levels of DS reached maximum around 7th grade followed by a decline to 9th grade. This finding replicates the report by Harrington, Rutter & Fombonne (1996) that in a non-clinical population, depression mood increases for both boys and girls until about 14 years old and followed by a decline thereafter. More recently Ge, Natsuaki and Conger (2006) also showed that the trajectories for adolescent SD were nonlinear with the maximum level of DS happened around 15 years old for girls. In summary, our hypothesis concerning the overall levels and the trajectory shapes of CP and DS are confirmed and the findings, in general, similar to findings reported in previous studies.
Figure 1.
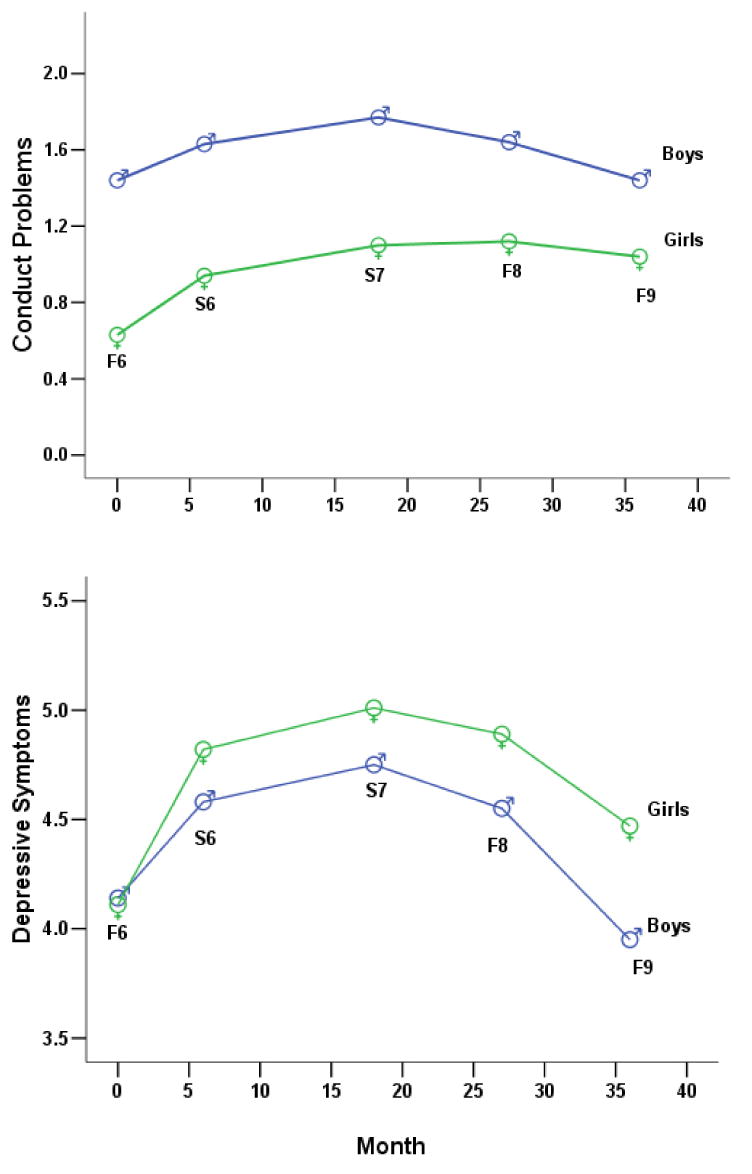
Developmental trajectories of conduct problems and depressive symptoms for boys (N = 1,120) and girls (N = 1,333) from Grade 6 to Grade 9
Results from Latent Growth Curve (LGC) modeling
Simple correlations between the covariates used in the LGC models and the major outcomes (CP and DS) at 6th grade are presented in Table 2. It can be seen from Table 2 that CP and DS are significantly correlated with r = 0.30 for both boys and girls indicating higher CP was associated with higher DS at baseline. CP was significantly associated with almost all covariates except for boys' SES. Although DS was significantly correlated with all covariates for boys, it only correlated with parent-child conflict (r = .36) and parent knowledge (r = -0.29) for girls, showing higher parent-child conflict and less parent knowledge are associated with higher DS for girls at baseline. It is not surprising that the interventin effect was not correlated with the covariates at baseline because the data were collected prior to the treatment program.
Table 2. Correlation matrix, Means and Standard Deviations of covariates and outcome variables for Boys (lower triangle matrix) and Girls (upper triangle matrix) measured at baseline.
| Variables | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 |
|---|---|---|---|---|---|---|---|---|
| 1 Conduct Problems | 1.00 | .30** | .11** | .44** | -.40** | .30** | -.33** | -.08** |
| 2 Depressive Symptoms | .30** | 1.00 | .03 | .21 | -.34 | .36** | -.29** | -.05 |
| 3 SES | .02 | .07* | 1.00 | .11** | -.09** | .14** | -.14** | -.03 |
| 4 Problem Peers | .45** | .22** | .07* | 1.00 | -.31** | .24** | -.01** | -.01 |
| 5 Social Competence | -.42** | -.32** | -.05 | -.37** | 1.00 | -.35** | .39** | .05 |
| 6 Parent Child Conflict | .27** | .26** | .13** | .27** | -.26** | 1.00 | -.40** | -.04 |
| 7 Parent Knowledge | -.24** | -.26** | -.12** | -.28** | .32** | -.31** | 1.00 | .06* |
| 8 Treatment Effect | -.01 | .04 | -.03 | -.03 | -.04 | -.13 | .04 | 1.00 |
|
|
||||||||
| Mean for Girls | .63 | 4.11 | .24 | 2.26 | 24.05 | 7.72 | 16.67 | 1.46 |
| Standard Deviation | 1.14 | 2.99 | .43 | 4.14 | 4.79 | 3.07 | 2.05 | .49 |
| Mean for Boys | 1.44 | 4.14 | .19 | 3.57 | 23.26 | 7.97 | 16.27 | 1.46 |
| Standard Deviation | 1.50 | 3.05 | .39 | 5.03 | 5.03 | 3.11 | 2.26 | .50 |
p < 0.05;
p < 0.01.
Unconditional LGC models were first fit for CP and DS to determine the shape of the trajectories and the variances in the growth factors. The four curvilinear trajectories shown in Figure 1 suggested a quadratic model. A quadratic model indeed fit significantly better than a linear model (p < 0.01) for boys and girls, respectively. The CFI and TLI are greater than 0.98 and the RMSEA is less than 0.04 in each of the four quadratic unconditional LGC models (CP for boys, CP for girls, DS for boys and DS for girls). Estimated variances in the intercepts, slopes and quadratic growth factors in the 4 fitted models are all significantly different from zero suggesting individual differences in the pathways of CP and DS. The significant differences in individual pathways justified the application of GGMM to identify heterogeneous subgroups in subsequent analyses.
Based on the fit of unconditional quadratic models, conditional parallel processing LGC models (Muthen & Curran, 1997; Muthen & Muthen, 2004, p.96) were estimated for boys and girls by incorporating the covariates into the model with paths from each covariate leading to the growth factors of CP and DS (see Figure 2). To apply the ‘estimating factor loading’ method to a quadratic model, three paths from the slopes to the five repeated measures were set free for estimation, with the first (time score = 0) and the last (time score = 3, indicating year) path kept fixed, as shown in figure 2. This multi-group parallel processing model for boys and girls fit well with CFI = 0.97, TLI = 0.96 and RMSEA = 0.037. The intercepts for CP and DS are significantly correlated with the unstandardized estimate = 0.28 (p < 0.01) for boys and 0.47 (p < 0.01) for girls, indicating positive association between CP and DS at the beginning of the study. However this path was not significantly different between boys and girls with χ2 (1) = 2.03, p > 0.05. A major interest in conducting this parallel processing model was the association between the two slopes. Figure 2 shows that the unstandardized estimate for this association was 0.08 (p < 0.01) for boys and 0.09 (p < 0.05) for girls indicating that the change of CP is positively related to the change in DS over time. However, the Chi-Square Difference Test did not show significant gender difference in this association with χ2 (1) = 0.44, p > 0.05.
Figure 2.

Path diagram for conditional parallel process LGC model for adolescent conduct problems and depressive symptoms from Grade 6 to Grade 9
Note: Unstandardized estimates are shown. The estimates on top are for girls and that at bottom are for boys.
The effects of covariates on the growth factors in this parallel processing model are summarized in Table 3. It should be noted that an effect of a covariate in this model are similar to that in a multiple regression where an effect is adjusted for other covariates in the model. We first evaluate the effects of covariates on the intercepts. Table 3 shows that more problem behaving peers, higher parent-child conflict, and lower social competence are related to higher CP and DS for both boys and girls at the base line. Higher parent knowledge was related to lower CP and DS for girls, but only related to lower DS for boys. SES showed no significant effects on the intercepts in the model.
Table 3. Effects of Covariates on Growth Factors for Conduct Problems and Depressive Symptoms Over Time for Boys (N = 1,120) and Girls (N = 1,333).
| Boys | Conduct Problems | Depressive Symptoms | ||
|---|---|---|---|---|
| Intercept | Slope | Intercept | Slope | |
| SES | -.157 | -.001 | .213 | -.051 |
| Problem Peers | .094** | .004 | .040* | -.001 |
| Social Competence | -.083** | -.005 | -.130** | .005 |
| Parent Child Conflict | .055** | -.002 | .144** | .024* |
| Parent Knowledge | -.018 | -.003 | -.155** | -.008 |
| Treatment Effect | -.094 | .000 | .192 | -.068 |
|
| ||||
| Girls | ||||
| SES | .068 | .035 | -.328 | .114* |
| Problem Peers | .085** | .011** | .048** | .012 |
| Social Competence | -.054** | -.004 | -.124** | -.005 |
| Parent Child Conflict | .038** | .008 | .224** | .022* |
| Parent Knowledge | -.059** | -.006 | -.153** | .025 |
| Treatment Effect | -.097 | .013 | -.181 | .031 |
p < .05.
p< .01. Standardized effects are shown.
Only a few covariates were found to have significant effects on slopes. Parent-child conflict was positively related to DS slope for both boys and girls showing higher parent-child conflict predicted an increase in DS over time. SES (coded 1 for free lunch and 0 for no free lunch) was related to DS slope for girls indicating that lower SES was associated with an increase in DS over time. Problem peers was significantly related to CP slope for girls suggesting that more problem friends at 6th grade predicted an increase in CP over time.
Results from General Growth Mixture Modeling (GGMM)
The GGMM was an extension of the conditional quadratic parallel processing model by adding two latent categorical variable (labeled ‘C1 and C2’ in the conceptual model diagram in Figure 3) and academic failure at 9th grade as a distal outcome. An important feather of the GGMM is to predict memberships for subgroups by capturing distinct pathways in the changes of CP and DS. The quadratic growth factor was specified in the model with the path loadings squared from the paths for the slope factor. Latent categorical variable C1 and C2 indicate heterogeneous subgroups in CP and DS, respectively, which are specified as correlated in the model. Each covariate leads directly to C1, C2, and Academic Failure that is also predicted by the two latent categorical variables. It should be noted that in GGMM analysis with MPlus, a missing value in outcome variables will be estimated with the EM algorithm, but a missing in a covariate will exclude the case from analysis. Due to missing values in the 6 covariates, the sample sizes in GGMM analysis were 916 boys and 1,104 girls.
Figure 3.

Path diagram for a general growth mixture model (GGMM) of concurrent changes in adolescent conduct problems and depression symptoms from Grade 6 to Grade 9
The first task in fitting the GGMM is to select a best fit model to decide the number of latent subgroups. We considered both BIC and AIC indices for this choice as described in Analysis section, with a smaller value of BIC or AIC indicating a relatively better fit model. The BIC and AIC indices for various models with different number of latent subgroups are presented in Table 4. The choice is clear by judging from BICs: the model with 4 latent subgroups in CP and 4 latent subgroups in DS is the best fit model for both boys and girls. The AIC value for this model is not the smallest, but models with 5 latent subgroups resulted in only a few memberships in one of the 5 subgroups. Therefore the GGMM with 4 latent CP subgroups and 4 latent DS subgroups was selected as the best fit model for boys and girls.
Table 4. Fit Indices for GGMM for Boys and Girls.
| Number of latent classes | Boys | Girls | |||
|---|---|---|---|---|---|
| CP | DS | BIC | AIC | BIC | AIC |
| 3 Classes | 4 Classes | 35386.4 | 34533.0 | 40296.4 | 39410.2 |
| 4 Classes | 3 Classes | 35272.0 | 34274.3 | 39386.5 | 38349.5 |
| 4 Classes | 4 Classes | 34988.6 | 33836.6 | 39342.9 | 38146.3 |
| 4 Classes | 5 Classes | 35069.0 | 33763.1 | 39648.6 | 38111.7 |
| 5 Classes | 4 Classes | 35006.3 | 33784.5 | 39396.3 | 37989.6 |
| 5 Classes | 5 Classes | 35406.2 | 34075.9 | 39350.2 | 37968.3 |
Note: BIC is Baysian information criterion and AIC is Akaike information Criterion. Smaller values of BIC and AIC indicate better fit of the model.
After obtaining group memberships for each participant from the GGMM analysis, the observed means of CP and DS were calculated to chart line graphs presented in Figure 4. The upper panel in Figure 4 shows the developmental pathways of CP for distinct subgroups for boys and girls separately. We can see from Figure 4 that the trajectory patterns are quite similar for boys and girls: adolescents in Subgroup 1 (G1 in Figure 4) reported lowest CP over time and Subgroup 4 (G4) started high in CP at 6th grade but followed by a decline to 9th grade. Adolescents in Subgroup 2 (G2) and Subgroup 3 (G3) reported medium levels of CP at 6th grade and in general kept in that level stably to 9th grade. We also can see that in the subgroups with the highest level of CP (Boys CP G4 and Girls CP G4), boys had a substantially bigger proportion (26%) than girls (9.1%). On the other hand in subgroups with the lowest level of CP (Boys CP G1 and Girls CP G1), girls had a bigger proportion (68.8%) than boys (41.3%). These results show that CP is relatively a more serious problem for boys than for girls.
Figure 4.
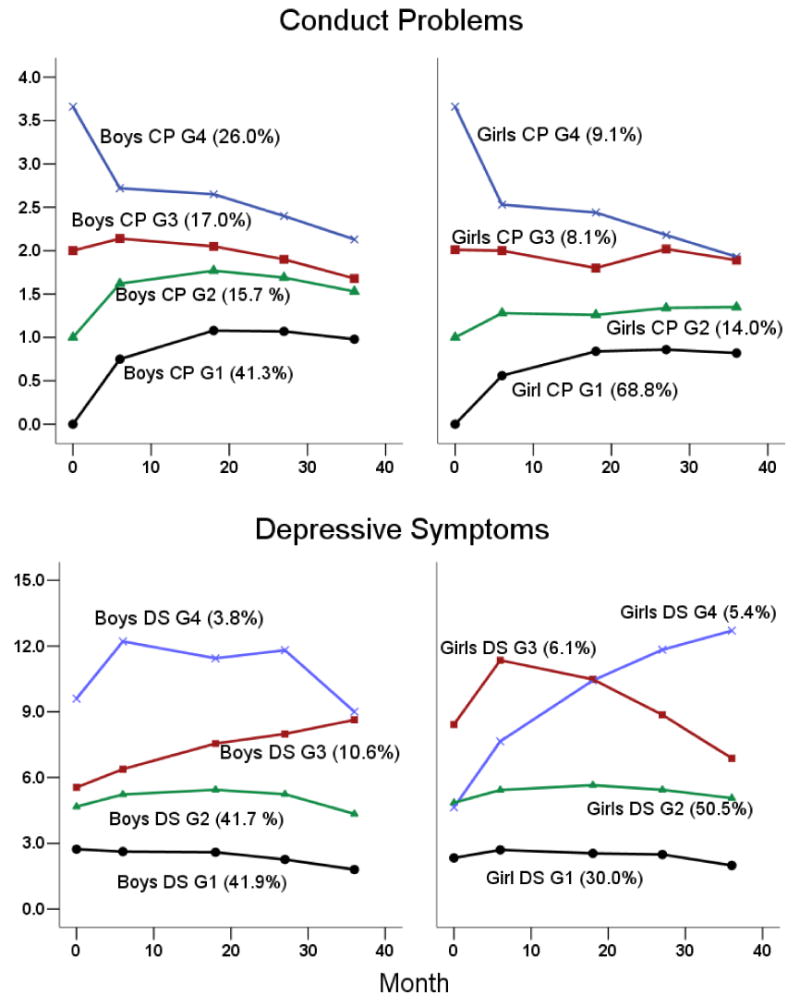
Line graphs for trajectories subgroups of conduct problems and depressive symptoms for boys and girls
The lower panel in Figure 4 shows the DS trajectories for subgroups predicted by GGMM. The trajectory patterns are also somewhat similar across gender, except that there was a distinct girl subgroup (Girls G4, 5.4%) that had low DS at 6th grade but the level of DS dramatically increased over time. There was a similar boy subgroup (Boys DS G3, 10.6%) with straight increase in DS over time, but the level of DS was never higher than the level for Boys DS G4 (G4, 3.8%). For both boys and girls there was a subgroup (Boys DS G1, 41.9% and Girls DS G1 30%) that reported almost free of DS over time. There was also a subgroup for boys and girls respectively (Boys DS G2, 41.7% and Girls DS G2, 50.5%) that experienced limited but stable DS over time. Only a small proportion of boys (Boys G4, 3.8%) experienced the highest level of DS over time. About 6.1% of the girls (Girls DS G3) had highest level of DS at 6th and 7th grade but the level of DS declined to 9th grade.
GGMM analysis estimated the effects of covariates on differentiating subgroups with odds ratios (see Table 5). Similar to the interpretation of odds ratios in a logistic regression, the odds ratios in Table 5 are adjusted for the effects of other covariates in the model. For example, the odds ratio for problem peers for Boys CP G4 vs. G1 is 1.27 (p < 0.01) indicating that one additional problem peer at 6th grade is related to an increase of 27% chance in Boys CP G4 relative to G1 while controlling other covariates. For odds ratios less than one, the chance is decreasing by 1 – odds ratio relative to the reference group. For example, the odds ratio for social competence related to Boys CP G4 vs. G1 is 0.88, indicating that with one unit increase in social competence, the chance in Boys CP G4 will decrease by 12% relative to G1.
Table 5. Odds Ratios Showing the Effects of Covariates on Subgroups for Boys and Girls.
| Conduct Problem | Boys | Girls | ||||
|---|---|---|---|---|---|---|
| Covariates Measured at Baseline | G4 vs. G1 | G3 vs. G1 | G2 vs. G1 | G4 vs. G1 | G3 vs. G1 | G2 vs. G1 |
| SES | 0.77 | 0.94 | 0.85 | 1.09 | 0.88 | 0.94 |
| Problem Peers | 1.27** | 1.13** | 1.13** | 1.22** | 1.17** | 1.13** |
| Child Social Competence | 0.88** | 0.88** | 0.99** | 0.83** | 0.87** | 0.92** |
| Parent Child Conflict | 1.14** | 1.09* | 1.08* | 1.21** | 1.04 | 1.13** |
| Parent Knowledge | 1.01 | 1.05 | 1.11 | 0.87* | 0.83** | 1.00 |
| Treatment Effect | 0.85 | 0.76 | 0.75 | 0.57* | 0.97 | 0.82 |
|
| ||||||
| Depressive Symptoms | Boys | Girls | ||||
|
|
|
|||||
| Covariates Measured at Baseline | G4 vs. G1 | G3 vs. G1 | G2 vs. G1 | G4 vs. G1 | G3 vs. G1 | G2 vs. G1 |
|
|
|
|
|
|
|
|
| SES | 1.00 | 0.29* | 0.59 | 1.78 | 1.13 | 1.08 |
| Problem Peers | 1.04 | 1.02 | 1.04 | 1.01 | 1.02 | 0.95 |
| Child Social Competence | 1.03 | 1.00 | 1.00 | 0.92* | 0.87** | 0.93* |
| Parent Child Conflict | 1.04 | 1.08 | 0.93 | 0.96 | 1.02 | 0.97 |
| Parent Knowledge | 0.83 | 0.76** | 0.82* | 0.88 | 1.08 | 1.07 |
| Treatment Effect | 1.75 | 1.33 | 1.40 | 1.92 | 0.32* | 0.83 |
Note. Probability was modeled with the normative group G4 as reference.
p < 0.05.
p < 0.01.
We first evaluate the effects of covariates that significantly differentiated CP subgroups (see top panel in Table 5). Problem peers and social competence differentiated G1 from all other three subgroups, with less problem friends and more social competence related to increased chances in Boys G1 and Girls G1, the subgroups with lowest CP over time. Parent-child conflict differentiated Boys and Girls G1 to almost all other subgroups except for Girls G3, with higher levels of parent-child conflict related to deduced chances in Boys G1 and Girls G1 subgroups. Parent knowledge has effects only for girls' CP but not for boys, with more parent knowledge associated to increased chance in Girls G1 relative to Girls G4 and G3. The SES showed no significant effects to differentiate CP subgroups.
Only a few significant covariates were found to differentiate DS subgroups (see the bottom panel in Table 5). The most noticeable is child social competence that differentiated Girls G1 from all other subgroups with more social competence related to higher chance to stay in Girls G1 relative to other subgroups. However social competence was not significant for differentiating Boys subgroups. Parent knowledge differentiated Boys G1 from Boys G2 and G3, with more parent knowledge related to increased chance in Boys G1. But parent knowledge was not significant for differentiating girls' subgroups.
Results from Multivariate Analysis of Variance (MANOVA)
The predicted memberships in CP and DS subgroups were used to categorize the sample into new groups to serve as an independent variable in MANOVA comparison. A two-way mosaic plot presented in Figure 5 is helpful to understand this categorization based on conditional distributions in CP and DS subgroups. A frequency is displayed for each mosaic showing the number of adolescents in this conditional subgroup. For example, the mosaic plot shows there are 197 boys in CP G1 and in DS G1, the lowest levels in both CP and DS over time. For another example, among the boys who were in Boys CP G4, there are 15 (6.3%) boys in DS G4, 48 (20.2%) in DS G3, 99 (41.6%) in DS G2, and 76 (31.9%) in DS G1. We can see from the conditional distributions that only 6.3% boys with the highest level of CP were in the highest DS subgroup and a majority of those boys (41.6% + 31.9% = 73.5%) experienced low levels of DS over time. However the distribution of CP conditional on DS turned out a different picture: among adolescents in highest levels of DS, about 43% boys (15 out of 35) and 10% girls (6 out of 59) reported highest levels of CP. Clearly, depressed boys are at increased risks of experiencing co-occurrence of CP and DS
Figure 5.

Mosaic plot presenting conditional frequencies of subgroups of conduct problems and depressive symptoms for boys and girls
The categorization based on memberships resulted in four new groups: High-High (high in CP and DS), CP only, DS only, and Low-Low (low in CP and DS). Specifically, for both boys and girls G1 and G2 were considered as low in CP or DS and G3 and G4 were categorized as high in CP or DS. Sample sizes and percentages for the four new groups are presented in Table 6. For example, we can see from Table 6 there are 471 (51.4%) boys and 828 (41%) girls in the Low-Low group. The mosaic plot in Figure 5 helps visualizing the four new groups. For instance, mosaic plot shows that Girls Low-Low group (a total of 4 mosaics) has relatively larger area than Boys Low-Low group.
Table 6. Results from 4 × 2 Factorial MANOVA Examining Gender and Group Differences.
| Boys
(N = 916) |
Girls
(N = 1,104) |
p-value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| CP: | Low- | Low- | High- | High- | Low- | Low- | High- | High- | |||
| DS: | Low | High | Low | High | Low | High | Low | High | |||
| N = | 471 | 51 | 313 | 81 | 828 | 85 | 150 | 41 | |||
| % = | 51.4 | 5.6 | 34.2 | 8.8 | 75.0 | 7.7 | 13.6 | 3.7 | group | sex | group × sex |
| (covariate variables) | |||||||||||
| SES | 0.17 | 0.20 | 0.21 | 0.12 | 0.21 | 0.28 | 0.28 | 0.41 | .14 | .01 | .17 |
| Problem Peers | 1.90a | 2.37a | 5.45b | 6.74c | 1.53a | 2.29a | 4.68b | 8.37c | .00 | .75 | .18 |
| Competence | 25.00a | 24.22a | 21.19b | 20.57b | 24.96a | 23.06b | 20.70c | 18.39d | .00 | .01 | .07 |
| Family Conflict | 7.20a | 7.96ab | 8.47c | 10.10d | 7.32a | 7.86a | 9.34b | 9.54b | .00 | .82 | .23 |
| Parent Know. | 16.74a | 15.96b | 15.98b | 14.73c | 17.04a | 16.53a | 15.50b | 14.61c | .00 | .77 | .06 |
| (distal variables) | |||||||||||
| GPA | 3.00a | 2.27b | 2.85a | 2.50b | 3.05a | 2.75ab | 2.90b | 2.69bc | .00 | .00 | .07 |
| Academic Fail | 0.05a | 0.30b | 0.11a | 0.30b | 0.05a | 0.13a | 0.07a | 0.15a | .00 | .00 | .01 |
Note: Means with different subscripts are significantly different with p < 0.05 from post hoc tests.
Group and Sex were used as two independent variables in a 4 × 2 factorial MANOVA to compare the mean differences in covariates and academic achievement variables. Results from this factorial MANOVA are presented in Table 6. The overall MAMOVA tests for the two main effects (Group and Sex) and the interaction (Group × Sex) were all significant with p < 0.01, which gave permissions to examine each dependent variable individually with some controlling in making Type I errors. The p values for the two main effects and the interaction for each dependent variable are presented in the last three columns in Table 6. It can be seen that none of the interaction terms is significant except for academic failure. An obvious interaction for academic failure was that for the Low-Low groups, the failure rate was the same for boys and girls but for the High-High groups, 30% of the boys failed but only 15% girls failed. This finding suggests gender difference in the adverse consequences of co-occurring CP and DS with boys having a relatively poorer academic adjustment than girls.
The main effect of Sex showed that girls had significantly higher proportion to have free lunch (0.27 vs. 0.15, p < 0.01), lower social competence (21.9 vs. 23.0, p < 0.01), higher GPA (2.85 vs. 2.66, p < 0.01) and lower academic failure rates (0.10 vs. 0.19, p < 0.01). The main effects of Group were of major interests in this study and we were particularly concerned with the comparison between the High-High group vs. other groups. Since the interaction (Group × Sex) was not significant for individual variables, we present simple effects (boys and girls separately) for comparing group differences in Table 6. The post hoc tests showed that except for SES, the High-High group was significantly different in all dependent variables relative to the Low-Low group, and this finding applies to both boys and girls. Specifically, the High-High group had significantly more problem friends at 6th grade, lower social competence, higher levels of parent-child conflict, less parent knowledge, lower GPA and higher rates for academic failure. These findings support the multiple factor model (Greenberg, et al. 2001) and the transaction model (Cicchetti & Toth, 1998) to explain the diverse pathways to the development of CP and DS respectively.
Discussion
The co-occurrence of CP and DS is an important topic in developmental psychopathology. Studies on issues related to the co-occurrence of CP and DS may reveal more insightful knowledge about the nature of problem behaviors than if we consider them as isolated outcomes. Most previous studies on the topic, however, were based on clinical, at-risk or male samples and mostly focused on identifying risk factors. The present study examined various aspects of the co-occurrence of CP and DS using a non-clinical, longitudinal sample with a relatively large sample size (N = 2,453) including both boys and girls. This is one of the few studies on the co-occurrence of CP and DS with a longitudinal sample with both boys and girls. A salient feature of the study is that the methodology we applied is consistent with the theoretical framework we adopted, specifically, where person-centered methods (GGMM) were used to explore and interpret the findings to be in harmony with the framework of the multiple factor model and the transactional model to examine the etiology of the co-occurrence problem. GGMM is the methodology that is becoming popular only in recent years and it is able to include the precursor variables as covariates, the distal outcome as consequence, and the latent categorical variables to uncover the population heterogeneity in the development of CP and DS. Muthen (2004) argues that the inclusion of the covariates and distal variables in one mixture model increases the accuracy and validity of predicted memberships in subgroups.
Overall levels of CP and DS
As hypothesized, boys reported higher CP than girls at waves in this study, and girls experienced more DS than boys except at the baseline where no meaningful difference appeared. The findings are in line with previous reports (e.g., Ge, Natsuaki & Conger, 2006, Harrington, Rutter & Fombonne, 1996, Cicchetti & Toth, 1998). Researchers consistently reported that adolescent girls experienced more DS than boys, but no consensus has reached regarding at what age this gender difference actually started. Our data show that gender differences existed at 6th grade and the gap increased to reach significant levels around 8th grade. Similar findings were reported by Cole et al. (1999) who found that gender difference in depression started at 12 years old and depression remained higher among girls than than boys during adolescence. Hankin et al. (1998) reported that small gender difference in depression, with girls greater than boys, first began to emerge at 13 years old and the difference started to increase at 15 years old. Our study in general replicated these findings, although Hankin's report showed one or two years older than our study when gender difference in DS started to appear. Designers of prevention and intervention programs may use the information to pinpoint the appropriate time to increase treatment efficiency and efficacy.
The consistency between our findings and the previous reports related to overall DS levels, the shapes of DS curves, and the gender differences in DS demonstrated some validity of the items we used to measure DS in this study. We used a brief questionnaire from the Weinberger Adjustment Inventory (Weinberger, 1991) with 6 items summed into a scale for measuring DS. The questionnaire was not designed for the diagnosis of clinical depression and we used it in a non-clinical sample for gauging adolescent levels of depressive mood in daily life. We argue that in studies on youth depression and CP, a clear distinction should be made between clinical and non-clinical samples in terms of specific measures and interpretation of findings. This distinction may clear up some inconsistent findings in literature.
Prevalence of Co-occurrence of CP and DS
A foremost issue in the study of the co-occurrence of CP and DS is the estimation of population prevalence and the conditional distributions of the two problem behaviors. A few studies reported the prevalence estimates from clinical samples but reports from non-clinical samples are rare. We defined the co-occurrence of CP and DS based on pathways over time instead of using cross-sectional measures at one time point. As hypothesized the majority of adolescents experienced little CP and DS over time. However, our major interest is the group of adolescents with high levels over time in both CP and DS. The method we used to define high and low levels in CP and DS was somewhat subjective in that subgroups G1 and G2 were classified as low levels, and subgroups G3 and G4 were defined as high levels of CP and DS. We provide the following reasons to defend the appropriateness of this classification. First, the prevalence estimated with this method is close to previous reports from non-clinical sample. For example, Capaldi (1991) classified about 13% boys into a group that had high in both CP and DS; we had about 8.8% boys in High-High group. Considering that Capaldi (1991) used an at-risk sample while our sample is school-based, the two estimates are quite close. Secondly, for girls DS subgroups there is no distinctive subgroup that experienced the highest DS level over time, and therefore it is appropriate to include the two subgroups (Girls DS G3 and G4) in one category to indicate high DS. Finally the trajectories in Figure 4 show that both G1 and G2 are in the low levels of CP and DS over time and it is reasonable to categorize the two subgroups into one category. With this categorization we found that 8.8% boys and 3.7% girls are in the High-High group and 51.4% boys and 75% girls in Low-Low group, respectively. The results indicate that boys had a higher prevalence of co-occurrence of CP and DS than girls in this non-clinical. Conditional distributions are also of interest to compare relative risks in ‘pure’ CP and ‘pure’ DS groups. We found that depressed boys were at highest risk to experience both high in CP and DS. This finding is informative for educators and parents to be aware of the risks related to depressed boys and take appropriate measures. Clinicians working with depressed boys may need to control the levels of CP as a likely co-occurring problem behavior in the treatment of depression.
Recently Ruchkin et. al. (2006) reported a cross-culture study on the prevalence of adolescent DS associated with other psychopathological symptoms. The study found in an epidemiological sample that, among depressed adolescents from age 14 to 17, about 6.9% boys and 4.2% girls had severe antisocial behavior. Unfortunately, Ruchkin et al. did not report the prevalence of SD conditional on CP, therefore we cannot make a direct comparison to our findings. The conditional prevalence in our study is higher than that reported in Ruchkin et. al. (2006) probably because we used longitudinal data that defined co-occurrence based on pathways of CP and DS over time, while Ruchkin et al. collected data at one time point.
Vulnerable Precursors of the Co-occurrence of CP and DS
Considerable efforts have been made to identify the etiology of adolescent problem behaviors but most studies treated the behaviors as isolated outcomes instead of co-occurring phenomenon. In this study we sought to examine the effects of demographical, psychosocial, and family factors on the changes in both CP and DS. We recognized that a single factor could not likely be sorted out as the precursor responsible of the emergence and maintenance of the co-occurrence problems. We hypothesized that it was the combination of biological (e.g. sex), individual characteristics (e.g., social competence), and family environment (e.g., family conflict or parent knowledge) variables that may be associated with the co-occurrence problem through some additive or interactive mechanisms.
We evaluated this hypothesis with three available modeling techniques, for the purposes of comparing the findings and the benefits of different methods. First, we estimated the predictive effects with the parallel processing LGC models. Although most covariates were associated with the intercepts of CP and DS, only a few covariates showed significant predictive power on the slopes. Parent-child conflict was the only factor that predicted the change in DS for both boys and girls, but it did not show significant predictive effects on the change in CP. It is possible that this variable-centered method assumes the same level of effect on each individual, but the existence of heterogeneity in population may obscure the power of predictability. The second method used odds ratios to differentiate the predicted subgroups, showing that social competence was the only factor that had predictive effects on both CP and DS, but only for girls. These two methods did not provide clear findings about the etiological precursors to the co-occurring CP and DS.
The third method was to create new groups based on predicted memberships with a major interest in the comparison between the High-High group and the other groups. This method was more sensitive, probably because only extreme groups were involved in comparisons. Results from this method showed significant differences in almost all covariates between High-High group and other three groups. SES was not significant, probably because it was indicated by a dichotomous measure, so that the variability in social-economic status was not properly represented in the variable. In sum, the results demonstrated that a combination of adverse factors was associated with the occurrence of CP and DS. This finding directly supports the multiple domain model and the transactional model that a mixture of multiple factors is responsible for the emergence and maintenance of co-occurrence in CP and DS. It also demonstrates the power of person-centered method when heterogeneity does exist in population.
Consequences of Co-Occurrence of CP and DS
Issues related to the consequences of co-occurrence are particularly appealing. The comparisons between the High-High group and the ‘pure’ groups may reveal the nature of the co-occurrence of CP and DS regarding whether it is the additive effects of the two problem behaviors or it is merely a same underlying entity with two different forms of expressions. Previous studies showed that the co-occurrence of CP and DS was associated with poor academic skills (Capaldi, 1991) and substance dependence (Marmorstein & Iacona, 2002), but longitudinal studies demonstrated that in a later time adolescents with both CP and DS did not show more adverse effects compared to ‘pure’ CP or ‘pure’ SD adolescents (Harrington, Rutter & Fombonne, 1996). We used MANOVA to compare group differences in average GPA and academic failure rates at 9th grade. The findings showed that the High-High group did significantly poorer than the Low-Low group for both genders. One surprising finding was that the average GPA is the lowest (2.27) for the ‘pure’ DS boys, although it was not significantly different from the High-High group (2.50). This finding replicates Harrington, Rutter and Forbonne's (1996) seemingly paradoxical finding that ‘…the subgroup of depressed youth people (had?) the worst overall social outcome’ (page 614). Is it possible that some aggressive activities had alleviated certain adverse consequences of SD? Clearly, further empirical and theoretical work is needed to examine this hypothesis.
Limitations
The data we used in this study have several limitations, so caution should be taken when interpreting and generalizing the findings. First, the data were obtained from a single source: self-reporting from the adolescents themselves except for the academic achievement scores that were drawn from school files. Correlations in the data from the same source are likely to be artificially inflated. The modeling techniques we applied in this study are based on covariance structures among the variables, and type I errors are likely to be higher than nominal levels if the covariance is biased towards higher side. A second limitation is that CP, a major outcome in the study, was measured with items heavily weighted on boy problems such as fighting and weapon carrying. It is possible that the girls' CP was not adequately measured so that the comparisons on CP between boys and girls may not be fair. Another limitation is that CP and DS, the major outcomes in this study, were measured with a limited number of items, which may reduce measurement reliability. However the measure of DS turned out to be to a reasonably valid ones because the overall levels and the shapes of the DS pathways for boys and girls are quite consistent to those reported in previous studies (e.g., Harrington, Rutter & Fombonne, 2001; Ge, Natsuaki & Conger, 2006). Finally the data were both right and left censored due to the limitation of data collection period between 6th and 9th grade. Some important models concerning the development of CP and DS, such as the early vs. later onset of CP and DS, are difficult to examine due to this data limitation.
Acknowledgments
This research was funded by NIH contract number N01-HD-4-3207 and approved by the NICHD Human Subjects Review Committee.
We are grateful to Linda Muthen at Muthen & Muthen Inc. for providing technical assistance in our data analysis.
Contributor Information
Rusan Chen, Georgetown University.
Bruce Simons-Morton, National Institutes of Health.
References
- Allen JP, Porter MR, McFarland FC. Leaders and followers in adolescent close friendships: Susceptibility to peer influence as a predictor of risky behavior, friendship instability, and depression. Developmental Psychopathology. 2006;18(1):155–172. doi: 10.1017/S0954579406060093. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Beyers JM, Loeber R. Untangling developmental relations between depressed mood and delinquency in male adolescents. Journal of Abnormal Child Psychology. 2003;31:247–266. doi: 10.1023/a:1023225428957. [DOI] [PubMed] [Google Scholar]
- Bollen KA, Curran PJ. Latent Curve Models: A Structural Equation Perspective. John Wiley & Sons; New Jersey: 2006. [Google Scholar]
- Capaldi DM. Co-occurrence of conduct problems and depressive symptoms in early adolescent boys: I. Familial factors and general adjustment at grade 6. Development and Psychopathology. 1991;3:277–300. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Capaldi DM. Co-occurrence of conduct problems and depressive symptoms in early adolescent boys: II. A 2-year follow-up at grade 8. Development and Psychopathology. 1992;4:125–144. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Capaldi DM, Stoolmiller M. Co-occurrence of conduct problems and depressive symptoms in early adolescent boys: III. Prediction to young-adult adjustment. Development and Psychopathology. 1999;11:59–84. doi: 10.1017/s0954579499001959. [DOI] [PubMed] [Google Scholar]
- Cicchetti D. Developmental psychopathology: Reactions, reflections, projections. Developmental Review. 1993;13:471–502. [Google Scholar]
- Cicchetti D, Toth SL. The development of depression in children and adolescents. American Psychologist. 1998;53:221–241. doi: 10.1037//0003-066x.53.2.221. [DOI] [PubMed] [Google Scholar]
- Cicchetti D, Rogosch FA, Toth SL. Maternal depressive disorder and contextual risk: Contributions to the development of attachment insecurity and behavior problems in toddlerhood. Development and Psychopathology. 1998;10:283–300. doi: 10.1017/s0954579498001618. [DOI] [PubMed] [Google Scholar]
- Cole DA, Martin JM, Peeke LA, Seroczynski AD, Fier J. Children's over- and underestimation of academic competence: A longitudinal study of gender differences, depression, and anxiety. Child Development. 1999;70:459–473. doi: 10.1111/1467-8624.00033. [DOI] [PubMed] [Google Scholar]
- Compton K, Snyder J, Schrepferman L, Bank L, Shortt JW. The contribution of parents and siblings to antisocial and depressive behavior in adolescents: A double jeopardy coercion model. Development and Psychopathology. 2003;15:163–182. doi: 10.1017/s0954579403000099. [DOI] [PubMed] [Google Scholar]
- Curran PJ. A latent curve framework for the study of developmental trajectories in adolescent substance use. In: Rose JS, et al., editors. Multivariate Applications in Substance Use Research: New Methods for New Questions. Lawrence Erlbaum Asso. Publishers; New Jersey: 2000. pp. 1–42. [Google Scholar]
- Formoso D, Gonzales NA, Aiken L. Family conflict and children's internalizing and externalizing behavior: Protective factors. American Journal of Community Psychology. 2000;28:175–199. doi: 10.1023/A:1005135217449. [DOI] [PubMed] [Google Scholar]
- Ge X, Natsuaki MN, Conger RD. Trajectories of depressive symptoms and stressful life events among male and female adolescents in divorced and nondivorced families. Development and Psychopathology. 2006;18:253–273. doi: 10.1017/S0954579406060147. [DOI] [PubMed] [Google Scholar]
- Greenberg MT, Speltz ML, DeKlyen M, Jones K. Correlates of clinic referral for early conduct problems: Variable- and person-oriented approaches. Development and Psychopathology. 2001;13:255–276. doi: 10.1017/s0954579401002048. [DOI] [PubMed] [Google Scholar]
- Gutman LM, Sameroff AJ. Continuities in depression from adolescence to young adulthood: Contrasting ecological influences. Development and Psychopathology. 2004;16:967–984. doi: 10.1017/s095457940404009x. [DOI] [PubMed] [Google Scholar]
- Hankin BL, Abramson LY, Moffitt TE, Silva PA, McGee R, Angell KE. Development of depression from preadolescence to young adulthood: Emerging gender difference in a 10-year longitudinal study. Journal of Abnormal Psychology. 1998;107:128–140. doi: 10.1037//0021-843x.107.1.128. [DOI] [PubMed] [Google Scholar]
- Harrington R, Rutter M, Fombonne E. Developmental pathways in depression: Multiple meanings, antecedents, and endpoints. Development and Psychopathology. 1996;8:601–616. [Google Scholar]
- Harter S. The perceived competence scales for children. Child Development. 1982;53:87–97. [PubMed] [Google Scholar]
- Hollenstein T, Granic I, Stoolmiller M, Snyder J. Rigidity in parent-child interactions and the development of externalizing and internalizing behavior in early childhood. Journal of Abnormal Child Psychology. 2004;32:595–607. doi: 10.1023/b:jacp.0000047209.37650.41. [DOI] [PubMed] [Google Scholar]
- Lansford JE, Malone PS, Stevens KI, Dodge KA, Bates JE, Pettit GS. Developmental trajectories of externalizing and internalizing behaviors: Factors underlying resilience in physically abused children. Development and Psychopathology. 2006;18:35–55. doi: 10.1017/S0954579406060032. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Little RJ, Rubin DB. Statistical analysis with missing data. Second. New York: Join Wiley & Sons; 2002. [Google Scholar]
- Marmorstein NR, Iacono WG. Major depression and conduct disorder in a twin sample: gender, functioning, and risk for future psychopathology. Journal of American Academy of Child and Adolescent Psychiatry. 2002;42:225–233. doi: 10.1097/00004583-200302000-00017. [DOI] [PubMed] [Google Scholar]
- McDonald RP, Ho M. Principles and practice in reporting structural equation analysis. Psychological Methods. 2002;7:64–82. doi: 10.1037/1082-989x.7.1.64. [DOI] [PubMed] [Google Scholar]
- Moffitt TE, Rutter M, Silva PA. Sex difference in antisocial behavior: conduct disorder, delinquency and violence in the Dunedin longitudinal study. Cambridge: Cambridge University Press; 2001. [Google Scholar]
- Muthen B. Latent variable analysis: Growth mixture modeling and related techniques for longitudinal data. In: Kaplan D, editor. Handbook of quantitative methodology for the social sciences. Newbury Park, CA: Sage Publications; 2004. pp. 345–368. [Google Scholar]
- Muthen B, Curran PJ. General longitudinal modeling of individual differences in experimental designs: a latent variable framework for analysis and power estimation. Psychological Methods. 1997;2:371–402. [Google Scholar]
- Muthen LK, Muthen BO. MPlus User's Guild. Third. Los Angeles, CA: Muthen & Muthen; 19982004. [Google Scholar]
- Robin AL, Foster SL. Negotiating parent-adolescent conflict: A behavioral – family systems approach. New York: Guilford Press; 1989. [Google Scholar]
- Ruchkin V, Sukhodolsky DG, Vermeiren R, Koposov RA, Schwab-Stone M. Depressive symptoms and associated psychopathology in urban adolescents: a cross-cultural study of three countries. The Journal of Nervous and Mental Disease. 2006;194:106–113. doi: 10.1097/01.nmd.0000198142.26754.18. [DOI] [PubMed] [Google Scholar]
- Rutter M. Isle of Wight revisited: twenty-five years of child psychiatric epidemiology. Journal of American Academy of Child and Adolescent Psychiatry. 1989;28:633–653. doi: 10.1097/00004583-198909000-00001. [DOI] [PubMed] [Google Scholar]
- Simons-Morton BG, Chen R, Abroms L, Haynie DL. Latent growth curve analysis of peer and parent influence on smoking progression among early adolescents. Health Psychology. 2004;23:612–621. doi: 10.1037/0278-6133.23.6.612. [DOI] [PubMed] [Google Scholar]
- Simons-Morton BG, Haynie D, Crump AD, Eitel P, Saylor K, Yu K. Expectancies and other psychosocial factors associated with alcohol use among early adolescent boys and girls. Addictive Behaviors. 1999;24:229–238. doi: 10.1016/s0306-4603(98)00095-1. [DOI] [PubMed] [Google Scholar]
- Simons-Morton BG, Haynie D, Saylor K, Crump AD, Chen R. The effects of the going places program on early adolescent substance use and antisocial behavior. Prevention Science. 2005;6(3):187–197. doi: 10.1007/s11121-005-0005-2. [DOI] [PubMed] [Google Scholar]
- Snyder J, Schrepferman L, Oeser J, Patterson G, Stoolmiller M, Johnson K, et al. Deviancy training and association with deviant peers in young children: Occurrence and contribution to early-onset conduct problems. Development and Psychopathology. 2005;17:397–413. doi: 10.1017/s0954579405050194. [DOI] [PubMed] [Google Scholar]
- Weinberger DA. Social-emotional adjustment in older children and adults: Psychometric properties of the Weinberger Adjustment Inventory. Case Western Reserve University; 1991. Unpublished manuscript. [Google Scholar]
- Wiesner M, Kim HK, Capaldi DM. Developmental trajectories of offending: Validation and prediction to young adult alcohol use, drug use, and depressive symptoms. Development and Psychopathology. 2005;17:251–270. doi: 10.1017/s0954579405050133. [DOI] [PMC free article] [PubMed] [Google Scholar]