

Abstract
High schools specifically designed for students recovering from a substance use disorder (substance abuse or dependence) have been emerging as a continuing care resource since 1987. This study of 17 schools provides the first systematic description of recovery school programs and their students. The most common school model is that of a program or affiliated school, embedded organizationally and physically with another school or set of alternative school programs. Although embedded, there are serious efforts to maintain physical separation of recovery school students from other students, using scheduling and physical barriers. Affiliation with public school systems is the case for most recovery schools, and seems to be a major factor in assuring fiscal and organizational feasibility.
The students in the recovery high schools studied were predominantly white (78%), with about one-half from two parent homes. Overall parent educational levels suggest a higher mean SES than in the general population. Most students (78%) had prior formal treatment for substance use disorders, often concomitantly with treatment for mental health concerns, and were often referred by treatment providers. Students came with a broad and complex range of mental health issues, traumatic experiences, drug use patterns, criminal justice involvement, and educational backgrounds. The complexity of these problems clearly limits the enrollment capacity of the schools.
Retrospective pretest to post-test analysis suggests significant reduction in substance use as well as in mental health symptoms among the students. Students were very positive in their assessment of the therapeutic value of the schools, but less enthusiastic regarding the educational programs. The school programs appear to successfully function as continuing care to reinforce and sustain the therapeutic benefits students gained from their treatment experiences.
Introduction
High schools specifically designed for students recovering from a substance use disorder1 (substance abuse or dependence) began opening in the United States in 1987, with the opening of Sobriety High in Minnesota. According to the Association of Recovery Schools (ARS), this continuing care model has slowly grown since that time to include 31 high schools in 10 states . With some exceptions (Godley, Godley, Dennis, Funk, & Passetti, 2002; McKay, 2001; Spear & Skala, 1995; Winters, Stinchfield, Opland, Weller, & Latimer, 2000), overall research about post-treatment continuing care is sparse. Even more sparse is research conducted on recovery schools, which has been limited to theses and dissertations (e.g., Finch, 2003; Rubin, 2002; Teas, 1998) and unpublished reports (Moberg, 1999; Moberg & Thaler, 1995). Despite a lack of cross-school research and no published model for replication, growth has been impressive. Most of the schools have opened in the last seven years. Recovery high schools received federal recognition in summer 2002 when the Center for Substance Abuse Treatment (CSAT) funded a three-day conference for existing recovery school administrators. Hazelden Press recently published a manual by Dr. Finch on “Starting a Recovery School: A How-To Manual” (Finch, 2005).
As recovery schools generate awareness, and more states and foundations consider funding such schools, exploratory research is needed to describe and explicate school models in order to inform replication and prepare for rigorous evaluation of the effectiveness of recovery schools. This paper provides initial results from an ongoing descriptive research project designed to begin evaluating this promising model for providing continuing care for adolescents with substance use disorders. Specifically, we describe the characteristics of the existing recovery high schools and their students, addressing the following questions:
What services are provided in recovery schools?
What educational and therapeutic models are being implemented?
How are these schools funded to assure institutional viability?
What goals exist for the schools and their students?
What are the characteristics of the students in terms of substance use disorder, treatment history, co-morbidity, and socio-economic status?
How do students gain access to the programs?
Further work with these data will attempt to develop a descriptive typology of recovery school programs, and assess the feasibility of conducting more rigorous research. The data will also be examined to enhance our understanding of issues affecting the long-term institutionalization and viability of recovery school programs, which has been problematic to date. Thus we are laying the groundwork for future studies to prospectively evaluate the cost effectiveness of these programs of continuing care for adolescents with substance use disorders.
The methodology for this study was built upon prior single-site research on recovery schools conducted independently by the authors. Site visits were scheduled for each participating school, and included document review, observation, staff interviews and surveys, student surveys and interviews with key external constituents.
Terminology
The concepts of “treatment” and “recovery” are evolving. Indeed, until recently, much less focus was placed in the U.S. on adolescent treatment than on prevention of adolescent substance abuse. As in any growing field, terminology, though often elusive, is important in attaining a common level of understanding. Some terms used frequently in this paper are “substance abuse”, “dependence”, “treatment” and “recovery”. They are defined here.
Substance Abuse and Dependence
This paper uses the term “substance use disorder” to encompass both substance dependence and substance abuse, each of which are considered substance use disorders in the Diagnostic and Statistical Manual of Mental Disorders, 4th edition (DSM-IV) (American Psychiatric Association, 1994). According to the DSM-IV, “The essential feature of Substance Abuse is a maladaptive pattern of substance use manifested by recurrent and significant adverse consequences related to repeated use of substances” (American Psychiatric Association, 1994, p. 182). The DSM-IV preempts a diagnosis of substance abuse with one of substance dependence if a person’s pattern of substance use has ever met the criteria for substance dependence. Dependence is defined as, “a cluster of cognitive, behavioral, and physiological symptoms indicating that the individual continues use of the substance despite significant substance-related problems” (American Psychiatric Association, 1994, p. 176). These problems can be categorized as tolerance, withdrawal, or compulsive use behaviors. Thus substance use without “recurrent and significant adverse consequences” is not sufficient to warrant a substance use disorder diagnosis, nor does it qualify students for participation in a recovery school.
The Substance Abuse and Mental Health Administration (SAMHSA) provides this clarification:
“Dependence is considered to be a more severe substance use problem than abuse because it involves the psychological and physiological effects of tolerance and withdrawal. Although individuals may meet the criteria specified for both dependence and abuse, persons meeting the criteria for both are classified as having dependence, but not abuse. Persons defined with abuse do not meet the criteria for dependence” (Substance Abuse and Mental Health Services Administration, 2006, p. 67).
Much of the national data referenced in this study was collected from the National Survey on Drug Use and Health (NSDUH), conducted annually by SAMHSA. Substances monitored by the NSDUH include alcohol and illicit drugs, such as marijuana, cocaine, heroin, hallucinogens, and inhalants, and the nonmedical use of prescription-type psychotherapeutic drugs (Substance Abuse and Mental Health Services Administration, 2006).
Treatment
“Treatment” is an evolving concept, especially for adolescents. The NSDUH creates a distinction between “specialty treatment” for a substance use disorder and more generalized treatment. The NSDUH defines specialty treatment as:
“treatment received at any of the following types of facilities: hospitals (inpatient only), drug or alcohol rehabilitation facilities (inpatient or outpatient), or mental health centers. It does not include treatment at an emergency room, private doctor’s office, self-help group, prison or jail, or hospital as an outpatient. An individual is defined as needing treatment for an alcohol or drug use problem if he or she met the DSM-IV (APA, 1994) diagnostic criteria for dependence on or abuse of alcohol or illicit drugs in the past 12 months, or if he or she received specialty treatment for alcohol use or illicit drug use in the past 12 months” (Substance Abuse and Mental Health Services Administration, 2006, p. 73).
These distinctions helped guide our understanding of the students in the schools, and they represent the meaning of our terminology in the paper. As the term “specialty treatment” can be cumbersome, we use the term “treatment” synonymously. Note, we do not consider Twelve Step meetings to be “treatment” in the context of this paper.
Recovery and the Continuum of Care
“Recovery” may be the most ambiguous of the terms discussed here. While recovery has often been considered to begin once treatment ends (i.e., “aftercare”), this understanding has proven insufficient. Since many people who meet the criteria for a substance use disorder do not ever receive treatment, recovery cannot be contingent upon the receipt of specialty treatment. Indeed, the field has embraced a “continuum of care” paradigm to replace the traditional, linear intervention-treatment-aftercare mindset. In his plenary presentation at the 2007 Joint Meeting on Adolescent Treatment Effectiveness (JMATE), Dr. Jack Stein, an administrator in SAMHSA’s Center for Substance Abuse Treatment (CSAT), suggested that the field has started to view recovery as beginning with the decision to get treatment rather than after treatment ends (Stein, 2007). This corresponds well with Bill White’s definition of “recovery” in his addiction recovery “glossary” as:
“the process of resolving, or the status of having resolved, alcohol and other drug problems…. While recovering conveys the dynamic, developmental process of addiction recovery, recovered provides a means of designating those who have achieved stable sobriety and better conveys the real hope for a permanent resolution of alcohol and other drug problems. The period used to designate people recovered from other chronic disorders is usually five years without active symptoms” (White, 2002, p. 29).
This view of recovery is consistent with that of the schools selected for this study. Recovery schools typically limit enrollment to students with a “substance use disorder”, as defined above. While few schools require treatment, most of the students in these schools have received some form of specialty treatment prior to and/or during their enrollment. Furthermore, using White’s distinction between “recovering” or “recovered”, none of the students in this study had attained five years of sobriety. Presumably, as high schools are typically four-years of school, no recovery school student would achieve the “recovered” status unless they stopped using in 7th Grade.
Background
Post-treatment continuing care or “aftercare” services for persons recovering from a substance use disorder has been described by researchers to be a “logical”, “essential”, and “important” component of the treatment continuum (Brown & Ashery, 1979; Hawkins & Catalano, 1985; McKay, 2001). According to the National Survey on Drug Use and Health (NSDUH) (Substance Abuse and Mental Health Services Administration, 2006), 2.1 million youths aged 12 to 17 needed treatment for an illicit drug or alcohol use problem in the U.S. in 2005, and of this group, 181,000 youths received treatment at a specialty facility (8.6 percent of youths who needed treatment). This left an additional 1.9 million youths in the U.S. who “needed” treatment for a substance use disorder but did not receive it at a specialty facility.
Rates of substance use disorders are associated with age. In 2005, 8.0 percent of youths aged 12 to 17 had a substance use disorder, and this increased to 21.8 percent for young adults aged 18 to 25 (Substance Abuse and Mental Health Services Administration, 2006).
The lives underlying these statistics show youths suffering from a variety of adverse consequences, including fatal and nonfatal injuries from motor-vehicle accidents, suicides, homicides, violence, delinquency, psychiatric disorders, and risky sexual practices (Winters, 1999). Additionally, the rate of physical, sexual, and emotional traumatization is high among adolescents in substance treatment Dennis (2004). Thus, the risk of post-traumatic stress is high for students in recovery.
Adolescents often initiate drug use due to experimentation and social conformity. Compared to adults with a substance use disorder, teens exhibit shorter use histories, more involvement with alcohol and cannabis, and greater binge drinking and poly-drug abuse (Titus et al., 2002; Winters, Stinchfield, Opland, Weller, & Latimer, 2000). It is widely agreed that, while adolescents have many of the same issues as adults, the unique challenges of adolescence require treatment and post-treatment continuing interventions designed specifically for youth. Research conducted on aftercare programs has linked continuing care with positive treatment outcomes (Donovan, 1998; Godley, Godley, Dennis, Funk, & Passetti, 2002; Kelly, Myers, & Brown, 2000; Marlatt, 1985). Research on post-treatment continuing care in general, let alone on adolescent aftercare, is lacking.
Recovery and Schooling
For teenagers, school often sits at the heart of the relapse threat. Because they are minors, the majority of adolescents must return to their pretreatment neighborhoods and schools (in the case of residential treatment). Students treated as outpatients may never have a respite from using peers in their school and neighborhood. One study found that virtually all adolescents returning to their old school reported being offered drugs on their first day back in school (Spear & Skala, 1995). Students who attend schools with high overall use levels are particularly susceptible to use (Cleveland & Wiebe, 2003; Piper, Moberg, & King, 2000). For many adolescents, schools not only represent the environment of previous use and contact with pretreatment using friends, but the emotional turmoil involved with life transitions (Isakson & Jarvis, 1999). When young people leave residential treatment or while receiving outpatient treatment, if a private school is not financially possible, their options usually are limited to their former school or dropping out.
Hawkins, Catalano, and Miller (1992) use the terms “risk factors” and “protective factors” in their study reviewing elements that contribute to adolescent substance use disorders (the former) as well as substance use avoidance (the latter). While their review is focused upon “the factors that have been shown to precede drug abuse”, the concepts are salient for continuing care programs that have a goal of preventing relapse. Among the risk factors noted by Hawkins and colleagues are association with drug-using peers, alcohol or drug availability, physiological and genetic factors, and academic challenges. Svensson (2000) also situates time spent with friends and peer deviance among the most important risk factors. In addition to peer pressure, difficulty coping with negative feelings and interpersonal conflict can endanger a teen’s newly-established sobriety (Winters, 1999). Spear and Skala (1995) paint a picture of adolescent recidivism that includes:
a lack of involvement in productive activities;
a return to the environment of previous use;
a failure to establish social contact with nonusers;
a lack of family involvement;
less likelihood of Twelve Step meeting attendance or leisure activities without drugs; and
increased likelihood of engaging in activities with pretreatment friends.
Additionally, adolescent relapsers are less likely to stay in school and more likely to skip school. Succeeding academically can help students stay sober, which in turn can help them graduate. Poor academic performance is the “single strongest predictor of dropping out” (Gibson, 1997, p. 5), and adolescents who drop out of school have a higher risk of relapsing than those who finish school (Casemore, 1990). Among adults aged 18 or older, those who graduated from high school but did not attend any college and those who graduated from college had lower rates of substance use disorders (9.0 and 8.0 percent, respectively) than those who were not high school graduates and those with some college (10.2 and 10.3 percent, respectively) (Substance Abuse and Mental Health Services Administration, 2006). This implies that educational attainment is a factor in a person’s ability to avoid abusing substances.
Vaillant (1988) finds that prosocial activities such as school assist the recovering person, and Resnick et al. (1997) believe “connectedness with school” is a general protective factor for adolescents. Under these premises, the first schools designed specifically to aid the newly sober teen opened in the late 1980s. According to White and Finch (2006), the first wave of recovery high schools opened between 1987 and 1998. These schools were truly experimental in nature, with the goal of “sober schooling” but no existing blueprints to guide them. Ecole Nouvelle (now Sobriety High) in Minnesota was established in 1986 and opened in a community center with four students and one teacher in 1987. Other early recovery high schools included several Minnesota schools: PEASE (Peers Enjoying a Sober Education) Academy (1989), the Gateway Program (1992), the Arona Campus (now Arona Academy) (1995), YES (Youth Education Sobriety) (1997, now closed), ExCEL Sober School (1998, now closed), and the Aateshing Program (1998). Early programs outside Minnesota included Unity High School in Phoenix, AZ (1992, now closed), Recovery High School in Albuquerque, NM (1992, now closed), Phoenix Academy in San Mateo, CA (1992), Thoreau High School in Woodland Hills, CA (1996), Oasis Academy (now Community High School) in Nashville, TN (1997), Santa Rosa (CA) Clean & Sober High School (1998), and the Summit School in Spokane, WA (1998, now closed).
Recovery High Schools and the Continuum of Treatment Care
The first recovery schools were designed to fit into the established treatment continuum of care. Winters et al. (1999, p. 24) suggest that for adolescents, “the period right after completion of a treatment program, when the youth returns to family, peers, and the neighborhood, is often the time of greatest risk of relapse.” Spear and Skala (1995, p. 346) concur that the first 60 days are “the greatest time of risk for each level of relapse”, suggesting “the need for intense post-treatment services during this time”. Students often transition into recovery high schools immediately upon leaving residential treatment or completing intensive outpatient programs. The schools thus are designed to reduce the relapse risk factors in a student’s experience by incorporating a “social bonding” perspective similar to the one advocated by Hawkins and colleagues (1992).
Moving to a life without drugs represents a major life change for the students of recovery schools. Since alcohol and other illicit drugs are considered mind or mood-altering, the removal of them affects how students experience the world. For drug dependent adolescents, alcohol and other drugs provide, among other things, support systems, coping mechanisms, recreational activities, and access to a peer group. A life without chemicals necessitates the replacement of each of these components or a decision to live without them. The support they receive in their first school experience after “getting clean and sober” can be a crucial factor in their ability to sustain their recovery. Most recovery high schools expect students to participate in mutual-aid programs to support their recovery from substance use disorders. Additionally, alternative learning environments can provide peer support vital to a young person’s attempts to avoid alcohol and drugs (Harrison & Hoffmann, 1987). With this goal in mind, recovery schools provide services to a specialized population with the intent of developing a strong internal community around a shared issue.
These schools fit the paradigm of continuing care within a “recovery management” system. Reviewing a number of recommended approaches to continuing care, Godley and colleagues (2002) summarize key components of post-treatment programs, suggesting they:
“offer sufficient intensity and duration of contact;
target multiple life-health domains (e.g., educational, emotional, physical health, vocational, legal, psychiatric);
be sensitive to the cultural and socioeconomic realities of the client;
encourage family involvement;
increase prosocial leisure habits;
encourage compliance with a wide range of social services to provide additional support;
focus on relapse prevention; and
provide cognitive behavior and problem solving skill training to help reduce cravings and to cope with anger, depression and anxiety.”
Recovery high schools focus on each of these domains during the school day, while providing an education and creating a non-using social network. Hawkins and Catalano (1985) cite the “correlates of relapse” (p. 918) as absence of a strong prosocial network (including family, peer, and isolative factors), lack of involvement in productive roles or active recreational activities, negative emotional states, and physical symptoms.
Past Research
Spear and Skala (1995, p. 356) state, “Post-treatment intervention research must focus on modalities or combinations of modalities that have a significant impact on recovery rates and behavior associated with establishing a drug-free lifestyle.” They further elaborate, “At this point, the discussion is not about fine tuning interventions but rather identifying which post-treatment modalities have a significant impact on relapse rates for which adolescents.” The call for literature on sound continuing care resources is still valid, and especially so for educational services. As an emergent form of recovery management for adolescents, much remains to be learned about the structure, institutionalization, and effectiveness of these programs. By systemically describing and examining recovery high schools, this project aims to establish their place in the continuum of care and to understand practices across schools.
No multi-site studies have been conducted on this model of schooling and continuing care prior to this study. Both the authors, however, have independently conducted previous single site case studies of recovery high schools.
Evaluation of Recovery High School, Albuquerque, New Mexico
Recovery High School (ARHS), located in Albuquerque, New Mexico, was an innovative alternative public high school for youth in recovery from substance use disorders. The development of the initial plan for the school, its implementation and evaluation were funded through grants from the Robert Wood Johnson Foundation. Moberg and Thaler (1995) conducted an evaluation of this program, focusing on the feasibility and replicability of the program model and its institutionalization into the Albuquerque Public Schools (APS) and the Albuquerque community. This study provided a model for the data collection and analysis methods used in this paper.
Moberg and Thaler (1995) concluded that the ARHS model - as modified over the life of the project - is feasible programmatically, with impressive evidence of therapeutic effectiveness but limited educational success. The programmatic feasibility was limited by the high per pupil costs encountered due to the severity of the presenting problems among the students who were attracted to the program. The nature of the students also led to an emphasis on therapy over traditional educational experiences. Thus the model which emerged is that of a day treatment program for students with substance use and co-occurring disorders, provided in an alternative educational setting. Structural and governance issues that plagued the program from its inception were never overcome. Criteria for assessing institutionalization - a commitment by the school district to continue the program, success in developing other funding sources, the development of routine ongoing relationships with other schools, and the maintenance of stable referral relationships in the community - were in general not accomplished.
Evaluation of Chicago Preparatory Charter High School
The Robert Wood Johnson foundation subsequently funded the evaluation of another attempt to develop a recovery high school benefiting from the lessons learned in the Albuquerque program. The evaluation was funded to provide an external evaluation of the implementation, feasibility, and preliminary effectiveness of the Chicago Preparatory Charter High School (CPCHS) program, partially funded by the Foundation. CPCHS was established as a charter school within the Chicago Public Schools to support students in their recovery from substance use disorders, while providing a rigorous educational program leading to a high school diploma. Due to premature closure of the school, resulting from a failure to implement the very well conceived plan, the evaluation was not implemented (Moberg, 1999).
Boundaries and a Sense of Place at “Recovery High School”
Finch’s (2003) study centered on the dynamics of recovery within one recovery high school. His study utilized ethnographic data to examine Recovery High School (RHS), a private school with 25 students who had entered voluntarily and agreed to work “programs of recovery” for a substance use disorder. A key finding concerned the effect of boundaries upon the sense of place within the school experienced by staff and students at RHS. The research focused on naturally occurring events, which were the usual events of the classrooms and the school being studied. RHS attempted to support the recovery of its students, and boundaries existed to define the sense of place in the community. Findings showed that supports and threats did not align neatly with permeable or firm boundaries. Some students found rigid structures helpful, while others preferred the freedom of permeability. Ultimately, the individual personalities and mental health of the collective staff and students involved with the school determined the appropriate levels of structure and flexibility necessary to provide a healthy learning environment.
Thus past research has examined single schools, emphasizing initial implementation, feasibility and institutionalization, as well as micro-level interaction patterns within a school. The current study builds on this work to provide a multi-site examination of recovery schools.
Association of Recovery Schools (ARS) — Definition of Recovery Schools
The Association of Recovery Schools (ARS) is a network of recovery high schools developed in 2002. ARS has developed membership criteria for schools that wish to join the association. These criteria guided (but did not completely limit) the selection of schools for this study. Officially recognized recovery high schools are expected to fit each of the following criteria:
“Recovery schools at the secondary level meet state requirements for awarding a secondary school diploma. Such schools are designed specifically for students recovering from substance abuse or dependency…
Recovery Schools provide academic services and assistance with recovery (including post-treatment support) and continuing care. However, they do not generally operate as treatment centers or mental health agencies.
Recovery Schools require that all students enrolled in the program be in recovery and working a program of recovery determined by the student and the School. Consequences of relapse are addressed by the individual School.
Recovery Schools offer academic courses for which students receive credit towards a high school or college degree. At the secondary level, schools assist students in making the transition into another high school, college or a career.
- Recovery Schools are prepared through policies and protocols to address the needs of students in crisis, therapeutic or other. These procedures can involve
- full or part-time licensed counselors on staff, or
- out-sourced counseling contracts through which a specific outside agency consults with staff in the event of a student crisis or relapse” (Association of Recovery Schools, 2007).
Because there is a remunerative obligation for membership and because these criteria have no evidence-base, membership in ARS was not a requirement for participation in this study. By providing a frame which was deliberatively conceived by professionals and recovering students, however, the ARS membership criteria did serve as a guide for defining schools which were invited to participate.
Methods
The study was conducted as an exploratory, descriptive analysis with the goal of yielding a typology of the schools and their operative program theories/models. Survey data provided information on the staff and on the students attending these schools. While an outcome study is needed, it was determined that a rigorous experimental or quasi-experimental trial would be premature before (a) understanding the nature of programs in operation and (b) assessing the feasibility of an outcome study.
The prior projects described above and the ARS guidelines for membership set the stage for the project. A general design and approach for studying the characteristics of recovery schools and their students was established and demonstrated to be useful in the Albuquerque and Chicago studies. Student data collection tools and mechanisms were piloted in these two schools. Additionally, a new small school was used as a pilot site for the current study before scheduling the official site visits.
The complete project included startup, protocol and survey development, and contracting with recovery schools to assure their participation; a one-day site visit to each of the participating schools during which survey and interview data were collected; and data analysis, interpretation and presentation of reports and publications. Data collection occurred over three school semesters. As the study of the Albuquerque Recovery High School discovered, the program evolved considerably over its first year of operation. With this in mind, our sample of schools was limited to 18 high schools (17 research sites and one pilot) that fit the ARS defining criteria (above) and that had been operating for at least two years. Data collected included observational field notes, interviews, documents (school charters, policy manuals, student handbooks, accountability reports), anonymous surveys of students, staff and administrators, and various secondary data such as school administrative data, attendance reports, graduation rates, and other reports available from the schools. This paper provides an initial analysis of student survey and site visit data.
Site Visits
A central component of the methodology was the use of in-person site visits of at least one full day on site. Site visits facilitated collection of survey data but also complemented and extended that data by allowing for exploration of the school and community, direct observation of settings and activities, and access to key individuals for interviewing. Site visits were conducted by teams of two-to-three researchers (though in two cases, only one researcher visited due to the extremely small size of the schools), in order to allow for multiple insights, differential expertise, cross-validation of findings, and enhanced scope. Increased validity of results was facilitated by this team approach. Due to IRB concerns regarding protection of human subjects, students were not interviewed.
As the purpose of the site visits was to gather descriptive information about the programs and students rather than to carry out a complete naturalistic inquiry or case study, we conducted scheduled, relatively standardized oral interviews (LeCompte, Preissle, & Tesch, 1993) with administrators, teachers, counselors, and other key personnel, such as volunteers or Board Members. We also attempted to interview at least one external constituent from each school’s inter-organizational network (such as school district administrators and referring treatment providers.) Interviewees were chosen based on discussions with school leaders and accessibility on the day of the site visit.
The interviews used detailed interview guides (tailored to the type of respondent) to assure that all of the conceptual areas of interest were covered at each site. While the interview guide provided structure, relevant probes and exploration of relevant divergent topics were also incorporated to maximize the learning from these interviews.
Observations were conducted during academic classes, staff meetings, and therapeutic programs (such as community meetings and “check-in” groups) and other routine activities. Interview data was collected on the nature, structure, and general goals of confidential therapy sessions, both individual and group, from staff perspectives (since these could not be directly observed). Also, facility tours were conducted during each visit, along with observation of the surrounding neighborhoods. Similar to the limitations placed on the interviews, observational data focused upon specific details of the events rather than an attempt to glean the representational nature, frequency, or participants’ sense of the events. With written permission of the participants, interviews were recorded and subsequently transcribed and erased.
Surveys
Administrators
In each school the responsible administrator was asked to complete a survey which summarized information about the school program itself. This included items about the organizational and physical structure of the school, number and characteristics of students, number and characteristics of staff, testing and employment policies, and other related items. A number of these items were adapted from the National Center for Education Statistics’ annual Schools and Staffing Survey (U.S. Department of Education, 2004).
School Staff
All staff were invited to complete anonymous surveys which include information specifically about their own demographic background, training, credentials and attitudes regarding education and recovery. Included in the survey were a series of attitude questions regarding operational aspects of the recovery school. (Staff survey data are not included in the present article.)
Students
An anonymous survey was developed for students to complete during the site visit. Since the limitations of our funding and the purpose of the project limited us to one survey opportunity with no follow-up data, a “retrospective pretest post-test” design was incorporated into the survey (Pratt, McGuigan & Katzev, 2000; Hill & Betz, 2005). The content of the survey adapted the Global Appraisal of Individual Needs-Quick (GAIN-Q) (Dennis, Titus, White, & Unsicker, 2005) as the basic instrument. The GAIN-Q contains a brief subset of items from the comprehensive GAIN-I, which is being used extensively in adolescent treatment programs and provides us with ready comparisons of the students in recovery schools to youth receiving treatment in other settings. GAIN-Q items which form scales on substance use disorders, emotional health, and behavioral health were included. In addition, we included standard items and/or our own constructed measures on educational, juvenile justice and treatment history; opinions and satisfaction with the recovery school; self perception/self esteem (Rosenberg & Rosenberg, 1978); and basic demographics.
Protection of Participants
To assure anonymity for the survey respondents and to obtain an IRB waiver of written parental consent, the student survey was designed so that all demographic items were on a separate page which was removed from and stored separately from the remaining items at the end of each survey administration. The schools sent IRB-approved informational letters (prepared by our research staff) to all parents and students prior to site visit days, with instructions on who on the school staff to contact if they wished to withhold consent from student involvement—which none did. Thus by not requiring written consent, and separating demographics from other data, no record of student identity nor means of inferentially linking substantive responses to individual students is possible. All student surveys were conducted by our research team with no involvement of local school staff, held by our staff and removed from the schools immediately at the conclusion of the site visit. Students were not interviewed. Staff interviewed and recorded at site visits signed informed consent forms.
Findings
In this section, we summarize what we have learned to date about the programmatic, organizational, and physical characteristics of recovery schools themselves. We then provide descriptive information on the students, their history and background, their self-reported behaviors, and their perceptions of the schools. Future articles will provide diagnostic estimates, compare these students to other adolescent treatment samples, and conduct further analysis of co-occurrence of the various complex concerns the students are struggling with. Survey and depth interview data from staff will be analyzed in future reports.
Recovery High School Programs
As described earlier, our study included 18 schools — the first school in Wisconsin was included as a pilot to test our data-collection tools and methods, and the subsequent 17 were included in the final data. Those 17 were in the following states (number of schools in parentheses):
California (3)
Colorado (1)
Minnesota (8)
Pennsylvania (1)
Tennessee (1)
Texas (3)
The sample approximated the national distribution of schools, with Minnesota, California, and Texas being the only states with more than one school in operation more than two years, and Minnesota being the only state with more than 10 recovery high schools.
Self-Referential Language
While for heuristic purposes this study uses the term “recovery high schools”— in line with the language of the Association of Recovery Schools — programs use a number of titles. In keeping with frequent embedding of recovery schools in larger organizations, some participants referred to the schools as “programs” rather than “schools”, even though the school had its own staff and student base. In many cases, staff, students, literature, and stakeholders of the same school might each refer to it differently. Some of the referential terms other than recovery school — which was most common in discussions with the researchers — included: “sober school”, “alternative school”, “community school”, “charter school”, and “area learning center”. The original schools in Minnesota were commonly known as “sober schools”, and this term was used most often by people associated with schools in that state. School representatives universally embraced their designation as “schools” or “school programs” rather than “treatment”.
Area Learning Centers (ALC) are an organizational form that is unique to Minnesota. These programs were authorized by the Minnesota State Legislature in 1987 as part of the so-called “second chance law” for secondary and post-secondary students (Boyd, Hare, & Nathan, 2002). ALCs are an educational program modality serving students with certain emotional and behavioral needs, including substance use disorders. Interestingly, participants often referred to this incorrectly as “Alternative Learning Center”.
Characteristics of Schools and Models
Most of the schools were embedded organizationally and physically, with students separated from other programs. While facilities and staff might be shared with another program or school, students were not. In every case, students spent the entire day in a homogeneous recovery school setting. Students were referred primarily from treatment programs and parents, and in some cases juvenile justice. It was rare that a student’s prior school was the referral source.
The schools had small enrollments, usually ranging from 12-25 students. Staff and administrators stated a preference to remain small, even though official and budgeted enrollments were usually larger than attendance observed during site visits (which on average was about 65% of the official number.) This could be accounted for by the variance of school population over the course of a school year. Many schools see enrollment changes daily, and most at least weekly to semi-weekly. Based on the administrators’ surveys, turnover is such that the total number of students enrolled at the fall official enrollment count is estimated to be 45% of the total students who enroll over the course of a school year. The median stated capacity was 35 students, but median enrollments on the days of researcher visits were 75% of that stated capacity.
School Facilities
As can be seen in Figure 1, facilities varied widely, with most schools sharing space with another school or program.
Figure 1.
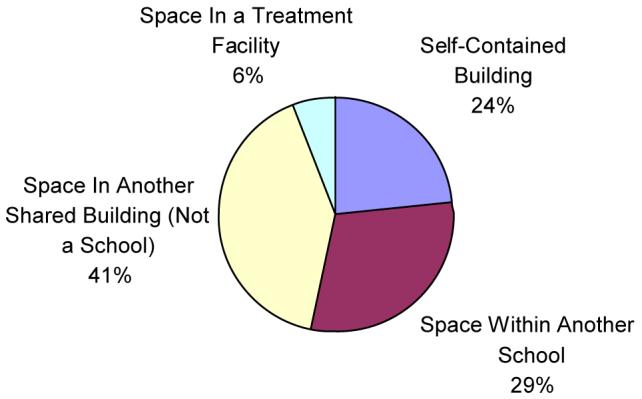
Recovery High School Facilities (n=17)
The seven schools that shared space with another building usually did so with a business or non-profit organization. In one case, the school was one of multiple non-profit programs located in a church facility. Only one school was located in an alcohol and drug treatment facility, and this was an outpatient treatment center.
In the five schools that shared space with another school, there was usually some division, such as a wall, doorway, or floor between the recovery school and the other school. Classrooms were distinct and were not shared at the same time. While students might take classes in the “other” part of the building, this was due to the teachers’ location, and the non-recovery school students would not be present. In several cases, schools altered start times so that the recovery school students would start, eat lunch, and leave at times different from the non-recovery school students, to minimize the opportunity for interaction. The total stated enrollment capacity of the 17 school facilities was 648.
School Funding
Funding was usually tied to enrollment, as schools were allotted funds on a per pupil basis by the local districts. In order to have some income certainty, most schools combined public funding with other fees, donations, and in two cases an actual “tuition” was charged.
Two of the schools received no public funding. Of the 15 that did receive public funding, the ratios provided were as follows:
75-100 percent: 8
50-75 percent: 4
25-50 percent: 1
Data not provided: 2
The median amount of public or tax-based funding was 80 percent. The two most common public school funding categories were alternative schools/area learning centers (9) and charter schools (5).
Admission Requirements
Schools were selected for this study based on their assertion that their school was designed for students in recovery from a substance use disorder. We found that admission criteria around this description varied. No school required an official diagnosis for admission, and the usual criteria corresponded more with Alcoholic/Narcotic Anonymous’ requirement of “a desire to quit drinking/using”. Sobriety duration prior to enrollment ranged from no official number of days stated up to 30 days of sobriety prior to admission.
Corresponding to the “stages of change” model (DiClemente, Schlundt, & Gemmell, 2004; Prochaska, DiClemente, & Norcross, 1992), students were admitted anywhere from contemplation through active recovery maintenance, though schools stated a desire to enroll students only in active recovery maintenance. Three schools had arrangements with the juvenile justice system to admit students on probation for alcohol and drug or other violations. Most schools stated an openness to accept students who exhibited symptoms of a substance use disorder who had a “willingness” to stop drinking/using, even if the student had no official diagnosis and did not exhibit all the symptoms of dependence or abuse. This appeared often to be driven by budgetary needs and responsiveness to community needs.
Most schools required some type of prior treatment for substance use, though this was undefined. Usually, this meant outpatient treatment. The three schools with juvenile justice agreements did not require prior treatment, and many students in these schools were coerced to attend by judges and parole officers. In the other schools, however, enrollment was almost completely voluntary on the part of students and their families. Recovery schools were seen as a school choice in order to support an alcohol and drug-abstinent lifestyle.
Frameworks of Recovery and Therapeutic Support
All schools included support groups during the academic day, many holding these groups once (or more) per day. All schools utilized some variant of the Twelve Step or Minnesota Model (Winters et al., 2000; Room, 1998), with an expectation of ongoing abstinence while attending the school.
One-on-one counseling was readily available across the schools as well. All schools involved a counselor or therapist, though some contracted with treatment centers to provide this service rather than having someone on-staff. Counseling credentials for staff members varied. Most common were licensed alcohol and drug counselors, licensed professional counselors, and licensed professional social workers. Therapeutic approaches ranged from the confrontational style of traditional alcoholism counseling to various forms of client-centered motivational approaches.
Academic Programs
Most schools shared academic staff with other schools or programs. The schools sharing facilities with other schools usually shared the parent organization’s administration and teachers. Most schools, however, had at least one or two dedicated staff members.
Teaching and learning was individualized and self-paced, often tutorial in nature. Class sizes were small, ranging from two or three students up to 10-15, depending on the enrollment of the school. Schools usually blended grade levels into one class or subject, and sometimes blended multiple subjects into one class period. A few schools only had one or two teachers available for the entire school. These schools used an externally-created modular curriculum aligned with state standards. Schools employed licensed or license-eligible teachers.
The academic programs were designed to either transition students from drug treatment to their regular schools (n=3) or to graduate them from the recovery high school (n=9). The remaining schools indicated flexibility on this goal depending on the student’s needs and choices. Typically, there was no set limit on length of stay, and some schools regularly had students enrolled for three or all four years of high school.
Summary Observations
While more precise exploration remains to be done, some general conclusions can be made about the schools. Schools tend to:
Be more publicly than privately funded;
Have more voluntary than involuntary enrollment;
Emphasize recovery maintenance and support more than primary treatment;
Balance their emphasis between academics and therapeutics;
Offer an eclectic recovery-support model that incorporates Twelve Step philosophy more than a Twelve Step exclusive model;
Be integrated with another school/program rather than be freestanding;
Share facilities with another school/program rather than stand alone;
Share staff with another program rather than employ dedicated staff;
Have slightly more intent to graduate their own students rather than transition them to another school; and
Have funding based on enrollment rather than sum certain funding.
As these data are examined in more detail, we will be able to quantify these distinctions more accurately. Part of the complexity of that process is that school descriptions often varied across a school’s staff both in interviews and surveys. In some cases, it is difficult, if not impossible, to place a school completely in one category or another on these continua due to conflicting staff reports. This is due in part to the evolving nature of these schools as well as the lack of an explicit model for most recovery schools to follow.
Students in Recovery High Schools
The demographic characteristics of the 321 students who completed surveys in the 17 schools we studied are summarized in Table 1. Here we see that the most of the students are classified as being in 10th, 11th or 12th grades, with 11th being the grade level with the largest enrollment. There is a slight over-representation of male students (54%). Most students (78%) are white, followed by 7% Hispanic/Latino and 4% American Indian. African American students are under-represented at three percent of enrolled students. For comparison, white non-Hispanics made up 69.1% of the total US population in 2000; African Americans made up 12.9%, Hispanic or Latinos 12.5%; and American Indians 0.9% (2000 U.S. Census, Table DP-1).
Table 1.
Demographic Characteristics of 321 Students in 17 Recovery High Schools
| Percent | |
|---|---|
| Grade Level | |
| Eighth | < 1% |
| Ninth | 12 |
| Tenth | 25 |
| Eleventh | 35 |
| Twelfth | 27 |
| Sex | |
| Female | 46 |
| Male | 54 |
| Ethnicity | |
| American Indian | 4 |
| Asian or Pacific islander | 3 |
| African American/Black | 3 |
| Hispanic/Latino | 7 |
| White/Caucasian | 78 |
| Other/Mixed | 4 |
| Family Structure | |
| Two Parent Home | 54 |
| Mother only | 22 |
| Father only | 10 |
| Other relatives | 5 |
| Other | 4 |
| Father Education: (64 missing) | |
| LT High School | 10 |
| High School Graduate | 28 |
| Some College or Technical School | 19 |
| College Degree | 22 |
| Advanced Degree | 21 |
| Mother Education: (53 missing) | |
| LT High School | 8 |
| High School Graduate | 30 |
| Some College or Technical School | 16 |
| College Degree | 30 |
| Advanced Degree | 16 |
Family structure reported by the students included 54% in two-parent homes (compared to 65.3% of all households with children in the US in 2000), and 22% living with mother only (close to the 19% nationally). Parental educational attainment, our only indicator of socio-economic status, shows that 43% of fathers and 46% of mothers had a college degree or more; 55% reported at least one parent had a college degree or higher. This compares to 24.4% of the US population aged 25 years and over in 2000 (US Census Table DP-2), suggesting that recovery schools are serving a population at higher than average SES.
Students had fairly extensive treatment histories for substance use disorders as well as various mental health issues (Table 2). Seventy-eight percent reported past substance treatment, including 54% with at least one episode of inpatient or residential service and 55% with outpatient treatment. Sixty percent reported an arrest history, and 20% were currently on probation or parole. Mental health specific treatment had been received by 49%, and nearly half were currently receiving outside treatment services. Currently, 80% report participating at least weekly in AA, NA, or some other form of 12-step group (often a requirement for continued enrollment in a recovery school).
Table 2.
Treatment history for 321 Students in 17 Recovery High Schools
| Percent | |
|---|---|
|
Past treatment for Substance Abuse or Dependency |
78 |
| Inpatient or residential | 54 |
| Outpatient | 55 |
| Past treatment for mental health problem | 49 |
| Inpatient or residential | 23 |
| Outpatient | 25 |
|
Currently receiving treatment outside the school |
48 |
| For substance use | 18 |
| For mental health | 16 |
| For both | 22 |
In keeping with the extensive treatment histories, the primary reported referral source (Table 3) to the recovery school was a substance treatment facility (50%). This was followed by self referral (25%), and friends or family (20%). Immediately prior to entering the recovery school, 42% reported they had been in a treatment setting, 33% in another school, and 22% out of school and/or not attending.
Table 3.
Referral Source for 321 Students in 17 Recovery High Schools
| Referred by: | Percent |
|---|---|
| Substance treatment facility | 50 |
| Self | 25 |
| Friends/family | 20 |
| Therapist | 15 |
| Previous school | 12 |
| Probation/parole | 11 |
| Immediately Prior Setting: | |
| Treatment setting | 42 |
| Another school | 33 |
| Regular school | 21 |
| Alternative, charter, etc. | 12 |
| Out of school/ not attending | 22 |
| Incarcerated | 5 |
Self reported student substance use patterns are summarized in Tables 4-6. A sampling of symptoms used for diagnosis of substance use disorders are shown in Table 4. Here we see that, using the retrospective pretest approach, all symptoms were reported to be very significantly (p < .001) reduced when students were asked to report what their use was like during the twelve months before entering the school (while in the community) compared to currently while attending a recovery school. For example, reports of at least weekly use of alcohol, cannabis or other illicit drugs were reduced from 90% to 7% now. Nearly one in five students (18%) reported continued withdrawal symptoms, however.
Table 4.
Student Substance Use Behaviors and Symptoms—Before and Now (n= 291)
| Pct Before* |
Pct Now | p | |
|---|---|---|---|
| Weekly use of alcohol, marijuana or other drugs | 90 | 7 | <.001 |
| Use caused to feel depressed, nervous, suspicious, uninterested, other psychological problems |
77 | 12 | <.001 |
| Used in dangerous or unsafe situation | 82 | 10 | <.001 |
| Use caused repeated problems with the law | 57 | 8 | <.001 |
| Reports tolerance | 81 | 7 | <.001 |
| Reports withdrawal problems | 71 | 18 | <.001 |
| Used larger amounts, more often or longer time than meant to |
84 | 11 | <.001 |
| Continued in spite of medical, psychological or emotional problems |
78 | 10 | <.001 |
“Before” is based on retrospective report at the time of survey regarding “the 12 months before your started this school.”
Table 6.
Student Drug Use Abstinence 90 Days Before Entered School and Since Entered School (n= 174 students who have been in school at least 90 days)
| Pct Before | Pct Now* | p | |
|---|---|---|---|
| Percent abstinent from all alcohol and other drugs | 20 | 56 | <.001 |
| Percent abstinent alcohol | 24 | 62 | <.001 |
| Percent abstinent cannabis | 30 | 71 | <.001 |
| Percent abstinent other drugs | 40 | 74 | <.001 |
| Percent of days abstinent | 32 | 82 | <.001 |
Since started school, not limited to 90 days
Table 5 provides student reports of their current drug use patterns, for those students who have been enrolled 90 or more days in the school. Students report a mean of 28.5 days abstinent in the prior 90 days before they entered the school. They reported an average of 266 days abstinent since entering the schools. These numbers translate to 32% of all days abstinent before entering the school, compared to 82% of all days since they entered the school. Similarly, we see large significant reductions in days used alcohol, “binge” drinking, days used cannabis, and days used other drugs. Current cigarette use was nearly universal (91%) among the students in recovery schools, however.
Table 5.
Student Drug Use Patterns 90 Days Before Entered School and Past 90 Days (n= 174 students who have been in school at least 90 days)
| Mean (s.d) Before |
Mean (s.d.) Now* |
p | |
|---|---|---|---|
| Days abstinent | 28.5 (36.8) |
266.1 (258.8) |
<.001 |
| Days used alcohol | 33.6 (35.4) |
3.5 (11.2) |
<.001 |
| Days drank 5 or more drinks at one time | 31.3 (34.2) |
3.0 (11.1) |
<.001 |
| Days used cannabis | 47.2 (40.0) |
3.1 (12.3) |
<.001 |
| Days used other drugs | 30.9 (37.3) |
2.8 (10.5) |
<.001 |
| Smoked cigarettes in last 30 days | NA | 91% (67% daily) |
NA |
Total days since entered school; not limited to 90 days.
Reported rates of complete abstinence from drug use were also calculated (Table 6). Continuous abstinence from all alcohol or other drugs increased from 20% during the 90 days before entering the school to 56% now. Complete abstinence since entering the school was reported by 62% for alcohol, 71% for cannabis, and 74% for other drugs.
In order to report meaningful contrasts to the 90 days before entering the school, these data are reported for the 174 students with at least 90 days in the school (54% of our sample). When we look at abstinence for all students completing our survey, we find a slightly higher rate of reported complete abstinence since entering the school (59% versus 56%), perhaps due to shorter time at risk.
Concomitant with the reported reductions in substance use are significant reductions in mental health symptoms (Table 7). Symptoms of depression, suicidal ideation, anxiety, ADHD all decreased significantly now, relative to the year prior to entering the school. The percent reporting they are bothered by any nervous, mental or psychological problem dropped from 69% to 33%. While also dropping significantly, symptoms of post-traumatic stress disorder remain high at 55%.
Table 7.
Selected Student Mental Health Symptoms—Before* and Now (n= 291)
| Pct Before | Pct Now | p | |
|---|---|---|---|
| Feel very trapped, lonely, sad, blue, depressed or hopeless about the future |
73 | 31 | <.001 |
| Have no energy, losing interest in work, school, friends, sex or other things you cared about? |
60 | 20 | <.001 |
| Thought about ending your life or committing suicide |
53 | 16 | <.001 |
| Felt very anxious, nervous, tense, fearful, scared, panicked…. |
68 | 44 | <.001 |
| Trembling, heart racing, restless… | 60 | 40 | <.001 |
| Very distressed, upset when reminded of the past | 65 | 55 | .003 |
| Had a hard time expressing feelings, even to people you cared about. |
83 | 49 | <.001 |
| Had a hard time paying attention at school, work or home. |
86 | 63 | <.001 |
| Been unable to stay in a seat or where you were supposed to be |
71 | 41 | <.001 |
| Bothered by any nervous, mental or psychological problems? |
69 | 33 | <.001 |
| Disturbed by memories of things from the past that you did, saw or happened to you? |
76 | 55 | <.001 |
“Before” is based on retrospective report at the time of survey regarding “the 12 months before your started this school.”
Students were asked to provide their opinions about their progress, comparing how they feel now compared to before coming to this school (Table 8). Here we see the most improvement is reported regarding improvement in alcohol/drug issues (80% better than before, 14% the same—good), followed by academic progress (71% better, 18% same-good). Emotional, family and peer issues are also reported to be improved.
Table 8.
Student Opinions about their Progress (n=290-315)
| How do you feel you are doing NOW compared to before coming to this school… |
Better | Same- Good |
Same—Not Good |
Worse |
|---|---|---|---|---|
| Academically (school work and grades) |
71% | 18% | 6% | 5% |
| Emotionally | 59 | 28 | 8 | 5 |
| With your alcohol/drug issues | 80 | 14 | 6 | 1 |
| With family issues | 57 | 28 | 11 | 4 |
| With peer/friendship/social issues |
56 | 33 | 7 | 4 |
Finally, students were asked a number of opinion items regarding their recovery school (Table 9). Highlights of these data are that about 75% report they came to the school completely voluntarily; 86% report they get more attention than they did at other high schools, 85% agree the school offers a good clinical /therapeutic program, and 87% report overall satisfaction (47% strongly). Indicators of perceived academic rigor are less strong. Most (71%) agree that classes are easier than at other schools; only 15% agree they “spend a lot of time doing homework after school”; and while 69% agree that the school has a “high quality academic program” only 14% “strongly agree” with this statement.
Table 9.
Student Opinions about their Recovery Schools (n=290-315)
| Strongly Agree |
Agree | Disagree | Strongly Disagree |
|
|---|---|---|---|---|
| I came to this school completely voluntarily |
42% | 33% | 17% | 8% |
| I get more attention here than I did at my other high schools |
55 | 31 | 10 | 4 |
| I think classes are easier here than at other schools |
26 | 45 | 24 | 5 |
| I spend a lot of time doing homework after school |
2 | 13 | 45 | 40 |
| This school has a high quality academic program |
14 | 55 | 23 | 8 |
| I think this school offers a good clinical/therapeutic program |
42 | 43 | 9 | 5 |
| I think the clinical program here is better than at other treatment programs I have been to |
18 | 35 | 35 | 12 |
| Overall, I am satisfied with this school |
47 | 40 | 9 | 4 |
DISCUSSION
The data collected for this study provide the first systematic description of recovery school programs and their students. Based on selection process and knowledge of the range of recovery schools, we believe the 17 schools studied are representative of the 34 some schools in existence at this time. As a new phenomena, recovery schools are dynamic in nature and vary in student population size and stability, financial and governance arrangements, staffing and organizational and physical arrangements. The most common school model is that of a program or affiliated school, embedded organizationally and physically with another school or set of alternative school programs. Although embedded, there are serious efforts to maintain physical separation of recovery school students from other students, using scheduling and physical barriers in most cases studied. Affiliation with public school systems is the case for most recovery schools, and seems to be a major factor in assuring fiscal and organizational feasibility.
The students in the recovery high schools studied slightly overrepresented male students (54%), were predominantly white (78%), with about one-half from two parent homes. Overall parent educational levels suggest a higher mean SES than in the general population. Most students (78%) had prior formal treatment for substance use disorders, often concomitantly with treatment for mental health concerns, and were often referred by treatment providers. Students came with a broad and complex range of mental health issues, traumatic experiences, drug use patterns, criminal justice involvement, and educational backgrounds. The complexity of these problems clearly limits the enrollment capacity of the schools.
Retrospective pretest to post-test analysis suggests significant reduction in substance use as well as in mental health symptoms among the students in recovery schools. Students were very positive in their assessment of the therapeutic value of the schools, but with less enthusiastic but positive ratings of the educational programs. The school programs do appear to successfully function as continuing care to reinforce and sustain the benefits students gained from their treatment experiences.
Limitations
The limitations of this descriptive study are consistent with our intent to conduct pilot or feasibility research. We expect that our results will further elucidate models for recovery schools and begin to describe the students and programs. We do not intend to draw any more than general impressions about effectiveness at this time. The limitations that prohibit drawing firm conclusions include the sample selected for the study, which we believe is representative but which was not randomly selected from all known recovery schools. The site visits were short (one day) and capture only a brief snapshot of what we have learned are very dynamic environments in terms of resources, staffing, student enrollment, and organizational characteristics. By selecting schools with at least a two year history, we stratified to assure some level of stability, but none-the-less our results must be seen to represent only a snapshot in time for these schools.
The student survey data also have a number of serious limitations. As a preliminary report, we have not completed the programming needed to score all the diagnostic scales tapped by our survey, so have instead reported on a sampling of representative items in this paper. Future articles will include analysis of a number of scales, and will compare to data on other adolescent populations in treatment. The retrospective pretest —post-test design, while having some evidence of validity (e.g., Pratt et al., 2000), is not an adequate substitute for a longitudinal design with multiple data collection points. Respondents to these surveys can be expected to slightly heighten or reduce the contrasts between the before and after items, depending on demand characteristics of the situation and their personal circumstances. However, this design remains superior to a purely single point in time measurement, which was our only alternative in this study.
Since we used a self-completed paper and pencil survey, there are a number of data quality problems that would be reduced in an interview situation or a computer-aided self interview (CASI) system. These data quality and missing data problems have been resolved by careful data cleaning, and where data are missing, using the general assumption of “missing at random” in our analysis. Thus we have reported results assuming that the distribution would be the same if every student had completed every item, in this paper.
As the data collected was descriptive in nature, this study did not address effectiveness of recovery schools, although such an assessment is needed and is a planned next step in our research. Furthermore, both time and cost limitations did not allow for a deep naturalistic inquiry. Such case studies will be needed to complement future evaluative research.
Finally, while there is extensive literature on self-report of adolescent behaviors, it is commonly acknowledged that biological validation of self-reported drug use is desirable in rigorous treatment research situations. In our case, the situations of survey reporting were structured to elicit honest responses with no repercussions, so our estimates of use rates are likely relatively close to reality. However, any future rigorous studies we conduct of this population would incorporate urinalysis into the design.
Future Research
We anticipate that this descriptive study will set the stage for a multi-site service effectiveness study. A lack of understanding currently exists about what tools recovery schools utilize to serve their students, who the students are, whether they show effects for students significantly different from those attained by recovering students attending non-recovery schools, and how student and programmatic differences affect outcomes. There are two critical endpoints in future research—on the program level, institutionalization with a stable flow of appropriate students and funding is critical. On the student level, relapse avoidance (or, at minimum, significantly reduced substance use and reduction of problems in other life areas) is the most critical outcome, with successful educational attainment a highly related and important secondary outcome. Our future research will address these issues, informed by the results of this preliminary work.
Acknowledgements
Funding for this research was provided by the National Institute on Drug Abuse, Grant # R21-DA-019045. We are indebted to Barbara Hill for managing many of the details of this research and participating in most of the site visits. We particularly wish to thank the staff and students of the following schools for their enthusiastic participation in this research: Aateshing — Cass Lake, MN; Archway Academy — Houston, TX; Clean & Sober — Santa Rosa, CA; Clean & Sober — Petaluma, CA; Community High — Nashville, TN, Gateway Program — St. Paul, MN, Horizon High — Madison, WI, INSIGHT — White Bear Lake, MN; Phoenix Academy — San Rafael, CA; Safe Harbor — Spring Lake Park, MN; Serenity High — McKinney, TX; Sobriety High — Burnsville, MN; Sobriety High — Maplewood, MN; Sobriety High — Edina, MN; SOAR — Broomfield, CO; Solace Academy — Chaska, MN; Transitions High—Harrisburg, PA; and Winfree Academy — Dallas, TX .
Footnotes
The term “substance use disorder” is used in this paper to refer to either substance abuse or dependence, as defined by the DSM-IV (American Psychiatric Association, 1994).
References
- American Psychiatric Association . Diagnostic and statistical manual of mental disorders : DSM-IV. 4th American Psychiatric Association; Washington, DC: 1994. [Google Scholar]
- Association of Recovery Schools Membership criteria Retrieved June 19, 2007, from 2007http://www.recoveryschools.org/applicants_info.html#criteria
- Boyd WL, Hare D, Nathan J. What really happened? In: Hubert H, editor. Minnesota’s experience with statewide public school choice programs: Center for School Change. Humphrey Institute of Public Affairs, University of Minnesota; Minneapolis, MN: 2002. [Google Scholar]
- Brown BS, Ashery RS. Aftercare in drug abuse programming. In: DuPont RL, Goldstein A, O’Donnell JA, editors. Handbook on drug abuse. Department of Health Education and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration, National Institute on Drug Abuse; Rockville, MD: 1979. pp. 165–173. [Google Scholar]
- Casemore BP. Teen drug use: Impacts and outcomes. U.S. Department of Education Office of Educational Research and Improvement; Washington, D.C.: 1990. [Google Scholar]
- Cleveland HH, Wiebe RP. The moderation of adolescent-to-peer similarity in tobacco and alcohol use by school levels of substance use. Child Development. 2003;74(1):279–291. doi: 10.1111/1467-8624.00535. [DOI] [PubMed] [Google Scholar]
- Dennis ML. Traumatic victimization among adolescents in substance abuse treatment: Time to stop ignoring the elephant in our counseling rooms. Counselor. 2004;(April):36–40. [Google Scholar]
- Dennis ML, Titus JC, White M, Unsicker J. Global Appraisal of Individual Needs - Quick. Chestnut Health Systems; Bloomington, IL: 2005. [Google Scholar]
- DiClemente CC, Schlundt D, Gemmell L. Readiness and stages of change in addiction treatment. American Journal on Addictions. 2004;13(2):103–119. doi: 10.1080/10550490490435777. [DOI] [PubMed] [Google Scholar]
- Donovan DM. Continuing care: Promoting the maintenance of change. In: Miller WR, Heather N, editors. Treating addictive behaviors. 2nd Plenum; New York: 1998. pp. 317–336. [Google Scholar]
- Finch AJ. Unpublished Ph.D. Dissertation. Vanderbilt University; Nashville, TN: 2003. A sense of place at Recovery High School: Boundary permeability and student recovery support. [Google Scholar]
- Finch AJ. Starting a recovery school: A how-to manual. Hazelden Publishing and Educational Services; Center City, MN: 2005. [Google Scholar]
- Gibson JT. Rekindling the spirits of throw-away children. New Directions for School Leadership. 1997;6:1–9. [Google Scholar]
- Godley MD, Godley SH, Dennis ML, Funk R, Passetti LL. Preliminary outcomes from the assertive continuing care experiment for adolescents discharged from residential treatment. Journal of Substance Abuse Treatment. 2002;23(1):21–32. doi: 10.1016/s0740-5472(02)00230-1. [DOI] [PubMed] [Google Scholar]
- Harrison PA, Hoffmann NG. CATOR Report: Adolescent residential treatment, intake and follow-up findings. Ramsey Clinic; St. Paul: 1987. [Google Scholar]
- Hawkins JD, Catalano RF. Aftercare in drug abuse treatment. The International Journal of the Addictions. 1985;20(6 7):917–945. doi: 10.3109/10826088509047759. [DOI] [PubMed] [Google Scholar]
- Hawkins JD, Catalano RF, Miller JY. Risk and protective factors for alcohol and other drug problems in adolescence and early adulthood: Implications for substance abuse prevention. Psychological Bulletin. 1992;112(1):64–105. doi: 10.1037/0033-2909.112.1.64. [DOI] [PubMed] [Google Scholar]
- Hill LG, Betz DL. Revisiting the retrospective pretest. American Journal of Evaluation. 2005;26(4):501–517. [Google Scholar]
- Isakson K, Jarvis P. The adjustment of adolescents during the transition into high school: A short-term longitudinal study. Journal of Youth and Adolescence. 1999;28(1):1–26. [Google Scholar]
- Kelly JF, Myers MG, Brown SA. A multivariate process model of adolescent 12-Step attendance and substance use outcome following inpatient treatment. Psychology of Addictive Behaviors. 2000;14(4):376–389. [PMC free article] [PubMed] [Google Scholar]
- LeCompte MD, Preissle J, Tesch R. Ethnography and qualitative design in educational research. 2nd Academic Press; San Diego, CA: 1993. [Google Scholar]
- Marlatt GA. Relapse prevention: Theoretical rationale and overview of the the model. In: Marlatt GA, Gordon JR, editors. Relapse prevention: Maintenance strategies in the treatment of addictive behaviors. Guilford; New York: 1985. [Google Scholar]
- McKay JR. Effectiveness of continuing care interventions for substance abusers. Evaluation Review. 2001;25(2):211–232. doi: 10.1177/0193841X0102500205. [DOI] [PubMed] [Google Scholar]
- Moberg DP. Evaluation of Chicago Preparatory Charter High School. Final Grant Report to the Robert Wood Johnson Foundation. University of Wisconsin Center for Health Policy and Program Evaluation; Madison, WI: 1999. [Google Scholar]
- Moberg DP, Thaler SL. An evaluation of Recovery High School: An alternative high school or adolescents in recovery from chemical dependence. An Unpublished Report to the Robert Wood Johnson Foundation; Princeton, N.J.: 1995. [Google Scholar]
- Piper DL, Moberg DP, King MJ. The Healthy for Life Project: Behavioral outcomes. Journal of Primary Prevention. 2000;21(1):47–73. [Google Scholar]
- Pratt CC, McGuigan WM, Katzev AR. Measuring program oiutcomes: Using retrospective pretest methodology. American Journal of Evaluation. 2000;21(3):341–349. [Google Scholar]
- Prochaska JO, DiClemente CC, Norcross JC. In search of how people change: Applications to addictive behaviors. American Psychologist. 1992;47:1102–1113. doi: 10.1037//0003-066x.47.9.1102. [DOI] [PubMed] [Google Scholar]
- Resnick M, Bearman P, Blum R, Bauman K, Harris K, Jones J, et al. Protecting adolescents from harm: Findings from the National Longitudinal Study on Adolescent Health. Journal of the American Medical Association. 1997;278(10):823–832. doi: 10.1001/jama.278.10.823. [DOI] [PubMed] [Google Scholar]
- Room, Robin Mutual help movements for alcohol problems in an international perspective. Addiction Research. 1998;6:131–145. [Google Scholar]
- Rosenberg FR, Rosenberg M. Self esteem and delinquency. Journal of Youth and Adolescence. 1978;7:279–294. doi: 10.1007/BF01537978. [DOI] [PubMed] [Google Scholar]
- Rubin BT. Unpublished Ph.D. Dissertation. Vanderbilt University; Nashville, TN: 2002. Changing lives through changing stories: A phenomenological study of adolescents in recovery from addiction. [Google Scholar]
- Spear SF, Skala SY. Posttreatment services of chemically dependent adolescents. In: Rahdert E, Czechowicz D, editors. Adolescent drug abuse: Clinical assessment and therapeutic interventions (NIDA Research Monograph 156) U.S. Department of Health and Human Services, National Institute on Drug Abuse; Rockville, MD: 1995. pp. 341–364. [Google Scholar]
- Stein J. Adolescent treatment—The road forward: A CSAT perspective. Paper presented at the Joint Meeting on Adolescent Treatment Effectiveness; Washington, D.C.. 2007. [Google Scholar]
- Substance Abuse and Mental Health Services Administration . Results from the 2005 National Survey on Drug Use and Health: National Findings. Office of Applied Studies; Rockville, MD: 2006. [Google Scholar]
- Svensson R. Risk factors for different dimensions of adolescent drug use. Journal of Child and Adolescent Substance Abuse. 2000;9(3):67–90. [Google Scholar]
- Teas TG. Chemically dependent teens with special needs: Educational considerations for after treatment. Bethel College; St. Paul, MN: 1998. [Google Scholar]
- Titus JC, Dennis ML, White MK, Godley SH, Tims F, Diamond G. An examination of adolescents’ reasons for starting, quitting, and continuing use to use drugs and alcohol following treatment (abstract) Drug and Alcohol Dependence. 2002;66(supplement 1):s183. [Google Scholar]
- U.S. Department of Education . Schools and staffing survey: 2003-2004 school year, OMB No. 1850-0598. National Center for Education Statistics; Washington, D.C.: 2004. [Google Scholar]
- Vaillant GE. What can long-term follow-up teach us about relapse and prevention of relapse in addiction? British Journal of Addiction. 1988;83:1147–1157. doi: 10.1111/j.1360-0443.1988.tb03021.x. [DOI] [PubMed] [Google Scholar]
- White WL.An addiction recovery glossary: The languages of American communities of recovery [Electronic Version] Retrieved June 11, 2007 from 2002www.bhrm.org
- White WL, Finch AJ. The recovery school movement: Its history and future. Counselor. 2006;7(2):54–57. [Google Scholar]
- Winters KC, editor. Treatment of adolescents with substance use disorders (TIP 32) U.S. Department of Health and Human Services, Public Health Service, Substance Abuse and Mental Health Services Administration, Center for Substance Abuse Treatment; Rockville, MD: 1999. [PubMed] [Google Scholar]
- Winters KC, Stinchfield RD, Opland E, Weller C, Latimer WW. The effectiveness of the Minnesota Model approach in the treatment of adolescent drug abusers. Addiction. 2000;95(4):601–612. doi: 10.1046/j.1360-0443.2000.95460111.x. [DOI] [PubMed] [Google Scholar]