

Abstract
Trajectories of emotion regulation processes were examined in a community sample of 269 children across the ages of 4 to 7 using hierarchical linear modeling. Maternal depressive symptomatology (Symptom Checklist-90) and children’s physiological reactivity (respiratory sinus arrhythmia [RSA]) and vagal regulation (ΔRSA) were explored as predictors of individual differences in trajectories of emotion regulation and negativity (mother-reported Emotion Regulation Checklist; A. M. Shields & D. Cicchetti, 1997). In addition, the authors explored whether children’s physiological regulation would moderate the effect of maternal depressive symptomatology on children’s emotion regulation trajectories. Results indicated that over time, emotion regulation increased whereas negativity decreased, though considerable individual variability in the pattern of change was observed. Greater maternal depressive symptomatology was associated with less steep emotion regulation trajectories. There was a significant Maternal Depressive Symptomatology × Baseline RSA × Age interaction predicting emotion regulation trajectories. Overall, it appears that the development of emotion regulation over time is compromised when mothers report greater depressive symptomatology. There is also evidence that children’s capacity for physiological regulation can buffer some of the adverse consequences associated with maternal depressive symptomatology.
Keywords: emotion regulation and reactivity, maternal depressive symptomatology, respiratory sinus arrhythmia (RSA)
The ability to regulate one’s emotions is a critical achievement attained during childhood that has important implications for many dimensions of children’s development (Calkins & Howse, 2004; Eisenberg et al., 2001; Sroufe, 1996). Research suggests that deficits in emotion regulation and higher levels of negativity in emotional expression are linked to greater levels of behavior problems, difficulties with peers, and later psychopathology (Calkins, Gill, Johnson, & Smith, 1999; Eisenberg et al., 2001; Keenan, 2000; Shipman, Schneider, & Brown, 2004). Conversely, a greater capacity for emotion regulation has been linked to better academic achievement (Gumora & Arsenio, 2002; Howse, Calkins, Anastopoulos, Keane, & Shelton, 2003) and social skills (Keane & Calkins, 2004). Overall, research indicates that the greatest risk for poor psychosocial outcomes occurs when children are highly reactive in emotionally arousing situations, tend to be negative rather than positive in their expressiveness, and have not developed adaptive strategies for managing their emotions (Calkins, Smith, Gill, & Johnson, 1998; Eisenberg, Fabes, Guthrie, & Reiser, 2000). Given the importance of children’s capacity for emotion regulation across multiple domains of adjustment, it is important to identify the factors that contribute to individual differences in the development of these skills across early childhood and to understand how trajectories of positive development may be facilitated. The developmental psychopathology perspective posits that there are multiple pathways to both adaptive and maladaptive functioning (Cicchetti, 1993; Rutter & Sroufe, 2000). Of particular interest from this perspective is developing an understanding of how particular factors interact to either enhance or impede children’s normative development.
Recent frameworks conceptualize emotion regulation as a process that encompasses both the reactive and regulatory dimensions of emotional expressions, in which emotional reactivity is viewed as a dimension of, but still distinct from, efforts to manage it (Calkins & Johnson, 1998; Fox & Calkins, 2003). Specifically, reactivity reflects the characteristic threshold, intensity, and duration of affective arousal (Rothbart & Bates, 2006). Emotion regulation refers to the behaviors, skills, and strategies, whether intrinsic or extrinsic, that modulate, inhibit, and enhance emotional experiences and expressions to meet situational demands and achieve personal goals (Calkins & Hill, 2007; Cole, Martin, & Dennis, 2004; Gross & Thompson, 2007). Although related, reactivity and regulation uniquely contribute to the prediction of children’s psychosocial functioning (Eisenberg et al., 1997; Rydell, Berlin, & Bohlin, 2003). For the current study, we were particularly interested in how physiological and environmental factors interact to influence children’s expression of negative affect and their ability to control their emotions.
Normative Development of Emotion Regulation Processes Across Childhood
Rapid changes have been documented in children’s emotion regulation and reactivity across early childhood as their capacity for self-regulation increases (Calkins et al., 1999; Calkins & Johnson, 1998; Kochanska, 1994; Kopp, 1989). Preschool children are capable of more active and planful regulation strategies, including an increasing ability to distract themselves and an emerging ability to reevaluate frustrating and disappointing situations in a more positive manner (Kalpidou, Power, Cherry, & Gottfried, 2004; Stansbury & Sigman, 2000). However, young children’s strategies for controlling their reactivity to challenging events are not always successful. Underlying these changes in children’s strategies for regulating their emotions are increasing language and cognitive skills in addition to maturational changes in neural and physiological systems (Fox, 1994). Recent evidence from developmental neuroscience suggests that the regions of the brain associated with the emotion regulation process include the prefrontal cortex, the anterior cingulate cortex, and the amygdala, some of which continue to mature through childhood and into adolescence (Beauregard, Lévesque, & Paquette, 2004). During this time there is also a shift in children’s developmental context. From preschool to early grade school there is an important transition characterized by greater demands on the child to engage in more autonomous self-control with larger class sizes and decreased supervision (Bronson, Tivnan, & Seppanen, 1995; Rimm-Kaufman & Pianta, 2000).
Therefore, the first aim of the current study was to explore the normative developmental trajectories of children’s emotion regulation and negativity across early childhood. Specifically, we expected that children’s emotion regulation would, on average, increase from 4 to 7 years of age in conjunction with a decrease in their tendency to display negative affect. We chose to use maternal reports of emotion regulation so that a comparable measure of emotion regulation could be used across each time point, which is a necessity for growth curve modeling. It has also been recognized that mothers observe their children across multiple contexts and situations, which places them in the unique position to observe general patterns of behavior (Rothbart & Bates, 2006).
Emotion Regulation Processes and Maternal Depressive Symptomatology
The development of children’s emotion regulation is embedded within the family socialization context and children’s early social interactions (Cummings, Keller, & Davies, 2005; Rogosch, Cicchetti, & Toth, 2004; Thompson & Meyer, 2007). For young children, caregivers are a critical external factor in emotion regulation, as they help children regulate their arousal and emotional states (Calkins, 1994; Kopp, 1989). For instance, sensitive parents generally monitor their young children’s environment so that the situational demands are developmentally appropriate, and they provide support, often suggesting strategies children can use to regulate their emotional response when they are distressed (Thompson & Meyer, 2007). Research suggests that parents’ direct intervention tends to decrease as children’s regulatory capacities increase. Therefore, as children grow parents may continue to monitor their child’s responses, but rather than intervening to alleviate distress, parents may suggest strategies for managing emotional responses, such as distraction. In this way, children are able to learn skills and strategies for dealing constructively with their emotional states to meet different situational demands (Calkins & Hill, 2007).
A number of factors may interfere with parents’ ability to support children’s growing reactivity and regulation skills during challenging situations. One key factor is maternal depression, which has been linked to children’s adjustment problems and a heightened risk for later psychopathology (Cummings & Davies, 1994; Goodman & Gotlib, 1999; Weissman et al., 2006). There is evidence to suggest that toddlers of depressed mothers are more likely to react negatively in response to stressful situations and exhibit deficits in their acquisition and use of emotion regulation strategies (Goodman & Gotlib, 1999). This also appears to be the case during early childhood. For example, during a delay-of-gratification task 4- to 7-year-old children of depressed mothers were more likely to focus on the desired object and less likely to use distraction than children of nondepressed mothers (Silk, Shaw, Skuban, Oland, & Kovacs, 2006).
Several mechanisms by which maternal depression may disrupt the normative development of children’s emotional regulation have been proposed (Downey & Coyne, 1990; Goodman & Gotlib, 1999). One is through the disruption of the parent-child relationship. Mothers with higher levels of depressive symptomatology exhibit increased psychological control and less warmth during interactions with their children (Cummings, Keller, & Davies, 2005) and are more likely to criticize their children (Rogosch, Cicchetti, & Toth, 2004). Maternal depression has also been found to alter the general emotional climate of the family, such that depressed mothers exhibit greater levels of trait negative affect, have more negative cognitions and attributions, are more self-focused, and engage in more negative behaviors than nondepressed mothers (Goodman & Gotlib, 1999; Rogosch et al., 2004). Therefore, even outside of specific parent-child interactions, when mothers have higher levels of depressive symptomatology they provide maladaptive models of emotional expression and regulation within the family. Our second aim, therefore, was to explore whether maternal depressive symptomatology predicted children’s trajectories of emotion regulation and negativity.
Children’s Physiological Regulation
Recent evidence indicates that children’s biological functioning is a critical factor in the development of adaptive behavior, particularly well-regulated emotional functioning (Calkins & Dedmon, 2000; Calkins, Graziano, & Keane, 2007; Calkins & Keane, 2004). It has been proposed that individual differences in nervous system functioning might mediate the expression and regulation of emotion (Porges, 2001, 2003; Porges, Doussard-Roosevelt, & Maita, 1994). Porges’s polyvagal theory implicates the maturation of the parasympathetic nervous system in the regulation of state, motor activity, and emotion (Porges, 1996, 2001, 2003; Porges et al., 1994). Parasympathetic nervous system functioning, as reflected in heart rate variability influenced by the vagal system, has been linked to the control of attention, emotion, and behavior (Calkins, 1997; Calkins & Dedmon, 2000; DeGangi, DiPietro, Greenspan, & Porges, 1991; Huffman et al., 1998; Porges, Doussard-Roosevelt, Portales, & Greenspan, 1996). Although there are multiple ways to measure this variability, Porges (1985, 1991, 1996) and colleagues developed a method that measures the amplitude and period of the oscillations associated with inhalation and exhalation. This measure refers to the variability in heart rate that occurs at the frequency of breathing (respiratory sinus arrhythmia [RSA]) and is thought to reflect the parasympathetic influence on heart rate variability via the vagus nerve. It has been proposed that baseline RSA may be a measure of an individual’s characteristic level of arousal and as such may reflect temperamental reactivity, which is commonly considered a traitlike individual characteristic (Calkins, 1997; Gunnar, Porter, Wolf, Rigatuso, & Larson, 1995). Some studies have shown high resting RSA to be associated with appropriate observed emotional reactivity (Stifter & Fox, 1990). However, other studies have found that higher baseline vagal tone is associated with greater negative emotional expressivity and more problem behavior (Cole, Zahn-Waxler, Fox, Usher, & Welsh, 1996; Eisenberg et al., 1995).
Porges’s theory further suggests that one particular measure of cardiac activity that may be more directly related to the kinds of regulatory behaviors children begin to display in toddlerhood and early childhood is vagal regulation of the heart as indexed by a decrease in RSA (vagal withdrawal) during situations where coping or emotional and behavioral regulation is required (Porges, 2001, 2003). Evidence of vagal withdrawal during demanding tasks may reflect physiological processes that allow the child to shift focus from internal homeostatic demands to the generation of coping strategies to control affective or behavioral arousal. Thus, vagal regulation is thought to be a physiological strategy that permits sustained attention and behaviors indicative of active coping that are mediated by the parasympathetic nervous system (Porges, 1991, 1996; Wilson & Gottman, 1996) and that result in greater cardiac output in the form of heart rate acceleration. Considerable research indicates that greater vagal withdrawal during challenging situations is related to better state regulation, greater self-soothing, and more attentional control in infancy (DeGangi et al., 1991; Huffman et al., 1998); more appropriate emotion regulation in preschool children (Calkins, 1997; Calkins & Dedmon, 2000; Calkins & Keane, 2004; Porges et al., 1996); and sustained attention in school-age children (Suess, Porges, & Plude, 1994). Therefore, the third aim of this study was to examine the link between children’s early physiological reactivity and regulation and their trajectories of emotion regulation and negativity over time. Given that children’s self-regulatory capacity is hierarchical in nature (Calkins & Fox, 2002), we expected that early physiological indices of appropriate reactivity and control would be linked with observable emotion negativity and regulation. Specifically, we hypothesized that children with higher baseline RSA and higher ΔRSA (vagal regulation) scores would be more likely to exhibit better emotion regulation and less negativity over time.
From a developmental psychopathology perspective, exploring how particular factors interact to either enhance or impede children’s normal development is particularly important. Although research indicates that maternal depression is a risk factor for poor emotion regulation, there are individual differences in children’s response to parental psychopathology such that not all children suffer maladaptive consequences (Goodman & Gotlib, 1999; Weissman et al., 2006). Several factors may account for children’s differing outcomes despite the risk that is associated with maternal depression. We were interested in child physiological factors that may buffer the effect of maternal depression on children’s emotional functioning. For example, there is some recent evidence to suggest that children’s capacity for physiological regulation can moderate the influence of family stressors on children’s emotional and physical outcomes. Specifically, children’s vagal regulation has been found to buffer children from the effects of marital conflict such that children with greater vagal regulation were less likely to exhibit internalizing behavior problems in the face of marital conflict as compared with children with lower vagal regulation (El-Sheikh, Harger, & Whitson, 2001; El-Sheikh & Whitson, 2006). Our final aim was to explore whether physiological regulation as indexed by children’s baseline RSA and ΔRSA during an attention task when they were 4 years of age was associated with greater regulatory abilities and decreased negativity from 4 to 7 years of age.
The Current Study
The current study addressed questions regarding the growth in emotion regulation expected to occur during the transition from preschool to school age in a large community sample of children. To summarize, the four aims were (a) to describe the developmental trajectory of emotion regulation and the display of negative affect from 4 to 7 years of age; (b) to examine whether maternal depressive symptomatology accounts for individual differences in children’s trajectories of emotion regulation and negativity; (c) to determine whether children’s physiological regulation, indexed by measures of RSA and ΔRSA, predicts children’s trajectories of emotion regulation and negativity; and (d) to determine whether children’s physiological regulation moderates the effect of maternal depression on children’s emotion regulation and negativity trajectories.
Method
Recruitment and Attrition
The current sample utilized data from two cohorts of children who are part of a larger ongoing longitudinal study. The goal for recruitment was to obtain a sample of children that was representative of the surrounding community in terms of race and socioeconomic status (SES) and who were at risk for developing future externalizing behavior problems. Both cohorts were recruited through child day-care centers, the County Health Department, and the local Women, Infants, and Children program. Potential participants were recruited at 2 years of age (Cohort 1: 1994-1996; Cohort 2: 2000-2001) and screened using the Child Behavior Checklist 2-3 (Achenbach, 1992) completed by the mother in order to oversample for externalizing behavior problems. Children were identified as being at risk for future externalizing behaviors if they received an externalizing T score of 60 or above. Efforts were made to obtain approximately equal numbers of boys and girls. A total of 307 children were selected. Of these, 47% were identified as being at risk for future externalizing problems. At 4 years of age, 275 families participated. Families lost to attrition (10%) included those who could not be located, who had moved out of the area, who declined participation, and who did not respond to phone and letter requests to participate. There were no significant differences between families who did and did not participate in terms of race, χ2(1, N = 307) = 0.70, p = .49; 2-year SES, t(305) = 0.41, p = .68; or 2-year externalizing T score, t(305) = -0.23, p = .08. Families with boys were more likely not to participate at the 4-year assessment than families with girls: gender, χ2(1, N = 307) = 4.18, p = .04. At 5 years of age, 253 families participated including 2 that did not participate in the 4-year assessment (attrition = 8%). There were no significant differences between families who did and did not participate in terms of gender, χ2(1, N = 307) = 3.02, p = .08; race, χ2(1, N = 307) = 1.38, p = .71; or 2-year SES, t(305) = 1.45, p = .15, although families of children with higher externalizing T scores at age 2 were more likely not to participate, t(305) = -1.97, p = .05. At 7 years of age, 240 families participated including 11 that did not participate at the 5-year assessment (attrition = 5%). There were no significant differences between families who did and did not participate in terms of gender, χ2(1, N = 307) = 1.54, p = .21; race, χ2(1, N = 307) = 0.79, p = .85; or 2-year externalizing T score, t(305) = -0.77, p = .44. Families with higher SES at age 2 were more likely to participate at year 7, t(424) = 0.81, p = .42 (M = 40.20 vs. M = 37.78).
Participants
The current sample included 269 children (125 male, 144 female) who had outcome data from at least one assessment (4-year n = 260, 5-year n = 236, 7-year n = 221). Children were on average 54.5 months (SD = 3.3 months), 68.6 months (SD = 3.2 months), and 91.4 months (SD = 3.5 months) at the 4-, 5-, and 7-year assessments, respectively. At the 4-year assessment, 66% were European American, 30% were African American, 3% were biracial, and 3% were Hispanic. The children were primarily from intact families at age 4 (77%; single parents = 16%, divorced/separated parents = 7%), and families were economically diverse according to Hollingshead (1975) SES scores (M = 43.13, SD = 10.77). The 5- and 7-year SES scores were on average 43.54 (SD = 10.82) and 45.16 (SD = 11.43), respectively.
Procedures
Children and their mothers participated in an ongoing longitudinal study when the children were 4, 5, and 7 years of age. During the laboratory assessments, the children and their mothers engaged in a series of tasks designed to elicit emotional and behavioral responding and mother-child interaction. The mother-child interaction tasks during the 4-year assessment included a teaching task, in which mothers were asked to teach their children how to replicate a model made of blocks (4 min); a free-play session, in which the mother-child dyads were asked to play with toys as they normally would at home (5 min); a compliance task, in which mothers were asked to have their children clean up toys from the free-play session (2 min); a puzzle task, in which mothers were asked to work on a series of two puzzles of increasing difficulty and assist their child when needed (5 min); and a pretend play task, in which mother-child dyads were instructed to play with a toy train set as they would at home. Heart rate data were collected during some of these tasks at the 4-year assessment. Mothers also completed questionnaires assessing family demographics, their own functioning, and their child’s behavior at each assessment. The current study utilized data from the 4-year laboratory assessment and maternal questionnaires from all three laboratory assessments.
Measures
Emotion regulation and negativity
Mothers completed the Emotion Regulation Checklist (Shields & Cicchetti, 1997, 2001), which assesses the parent’s perception of the child’s emotionality and regulation. This measure includes 23 items that are rated on a 4-point Likert scale indicating how frequently the behaviors occur (1 = almost always to 4 = never). The Emotion Regulation subscale includes 8 items that assess aspects of emotion understanding and empathy and includes items such as “displays appropriate negative affect in response to hostile, aggressive or intrusive play” and “is a cheerful child.” The Negativity subscale includes 15 items that assess aspects such as angry reactivity, emotional intensity, and dysregulated positive emotions and includes items such as “exhibits wide mood swings” and “is easily frustrated.” Validity has been established using correlations with observers’ ratings of children’s regulatory abilities and the proportion of expressed positive and negative affect (Shields & Cicchetti, 1997). In the current sample, Cronbach’s alpha for emotion regulation across the three waves ranged from .59 to .66 and for negativity ranged from .84 to .87. The correlations across the three assessments between regulation and negativity ranged from -.37 to -.48. Additionally, mother reports of regulation and negativity were significantly (p < .05) correlated with teacher reports assessed the same year (for regulation, r = .17 to .25; for negativity, r = .30 to .43).
Maternal depressive symptomatology
The Symptom Checklist-90-Revised (Derogatis, 1986) was used to assess self-reported symptoms of maternal psychopathology at the 4-year assessment. The 90 items were rated on how much distress they caused over the previous 7 days using a 5-point scale ranging from 0 to 4 (not at all, a little bit, moderately, quite a bit, and extremely). Twelve factor scores can be derived from the questionnaire, and reliability for the overall measure and the individual scales is good (Derogatis, 1986; Derogatis & Cleary, 1977). The current study used the 13-item Maternal Depression subscale (α = .91), which includes items such as “feeling low in energy or slowed down,” “crying easily,” and “feelings of worthlessness.” For the present study we used the maternal depression T score (M = 50, SD = 10), which was normed to adult nonpatients. For the current sample, 68 mothers had T scores of 60 and above, which is considered at risk in terms of clinical significance.
Negative parenting
Global codes of maternal behavior were adapted from the Early Parenting Coding System (Winslow, Shaw, Bruns, & Kiebler, 1995). Behaviors coded included warmth/positive affect (displaying positive affect and warmth toward the child); sensitivity/responsiveness (promptly and appropriately responding to the child’s bids to her); strictness/punitiveness (being too strict, demanding, or harsh relative to the child’s behavior; exerting influence toward completion of the child’s activity; displaying a no-nonsense attitude; constantly guiding the child and creating a very structured environment); and hostility (expression of anger toward the child). Each behavior was coded once for each mother-child interaction task (i.e., teaching, free-play, cleanup, puzzle, and pretend play) on a 4-point scale (1 = low to 4 = high). Four coders trained on 10% of the videotaped sessions and independently coded another 10% for reliability. The average adjusted kappas between each pair of coders were all above .70. The correlations across each mother-child interaction task ranged from .14 to .40 for strictness/punitiveness and .23 to .62 for hostility. For the current study a negative parenting composite was created by averaging strictness/punitiveness and hostility scores across each of the mother-child interaction tasks. The strictness/punitiveness average score and hostility average score (r = .34, p < .001) were then summed to create a negative parenting composite.
Children’s Physiological Regulation
At the beginning of the laboratory assessment, an experimenter placed three disposable pediatric electrodes in an inverted triangle pattern on the child’s chest. The electrodes were connected to a preamplifier, and the output from the preamplifier was transmitted to a vagal tone monitor (VTM-I, Delta Biometrics, Bethesda, MD) for R-wave detection. A data file containing the interbeat intervals (IBIs) for the entire period of heart rate collection was saved on a laptop computer for later artifact editing (e.g., resulting from child movement) and analysis. Measures of children’s baseline RSA and change in RSA from baseline during an attention task at age 4 were obtained by editing IBI files using MXEDIT software (Delta Biometrics). To edit the files, the data were scanned for outlier points, relative to adjacent data, and the outliers were replaced by dividing or summing them so they would be consistent with the surrounding data. Only data files in which less than 10% of the data required editing were included in the current study. The Porges (1985) method of analyzing IBI data was used to calculate RSA. This method applies an algorithm to the sequential heart period (HP) data. The algorithm uses a moving 21-point polynomial to detrend periodicities in HP that are slower than RSA. Next, a bandpass filter extracts variance in HP within the frequency band of spontaneous respiration in young children, 0.24-1.04 Hz. The natural log of this variance is taken and reported in units of ln(ms)2. RSA was calculated every 30 s for the baseline and attention tasks, and the average across the 30-s epochs for each episode was used in subsequent analyses. Data were excluded if the standard deviation for an episode was over 1.0.
Baseline RSA
Baseline RSA was obtained at the beginning of the laboratory assessment while the child watched one of two 5-min segments of the videotape Spot, about a puppy who explores his neighborhood. In one video clip, Spot is hiding from his mother and she tries to find him in various locations. In the second video clip, Spot is exploring a garden and runs into various characters and is scared by a cat. The use of the video stimulus was necessary to limit movement artifact in the data, given that the children were 4 years of age. Although this episode is not a true baseline, as the child’s attention was engaged, it was sufficient to gain a measure of RSA while the child was sitting quietly and showing little affect.
Change in RSA (ΔRSA)
Children also participated in an effortful attention task adapted from LAB-TAB procedures (Goldsmith & Rothbart, 1993). They watched a PowerPoint slide show with different types of pictures, such as mothers and children, animals, and other nature scenes. Children were instructed to sit quietly and continue to look at each picture as long as it was presented. Three blocks of five slides were presented. The first slide was presented for 2 s, and each successive slide was presented for approximately 2 s longer than the previous slide in that block. The task lasted approximately 2 min. Children’s ΔRSA was calculated by subtracting the average RSA during the attention task from the average RSA during the baseline episode. Negative change scores occurred when there was an increase in RSA from the baseline to the effortful attention episode and reflected a state that does not require regulation. Positive change scores occurred when there was a decrease in RSA from baseline to the effortful attention episode, which reflected attempts at vagal regulation. Therefore, higher positive ΔRSA scores indicate the child had greater vagal regulation. In the current study, we found that 70% of children showed some evidence of suppression from the baseline to the attention task (i.e., had positive change scores).
Data Analytic Strategy
Growth curve analyses were conducted to examine the developmental trajectories of emotion regulation and negativity in early childhood using hierarchical linear modeling (HLM; Raudenbush & Bryk, 2002). HLM was used because it allows for unbalanced designs, and so children with incomplete outcome data across the three waves could be included in the analyses. For the current study, emotion regulation and negativity were assessed when children were 4, 5, and 7 years of age. Age was centered at 90 months (7.5 years) so that the intercept indicated the status at the end of the growth period examined and the coefficients indicated the change that occurred in 1-month increments starting at age 4. Linear within-child growth trajectories were fit using full maximum likelihood estimation, and the results reported are based on the robust standard errors. Linear models have been recognized as providing a good approximation of the nature of change that occurs even when the actual change is more complex (Rogosa, Brant, & Zimowski, 1982). Gender was coded (male = 0, female = 1) and all continuous variables were mean centered. Significant interactions with continuous variables were plotted at ±1 SD from the mean, and simple slopes were calculated (Aiken & West, 1991; Preacher, Curran, & Bauer, 2006). Simple slopes were also calculated for predictors that were significantly related to the slope (i.e., cross-level interactions; Preacher et al., 2006).
Results
The results are presented as follows. First, we report on preliminary analyses conducted to assess the pattern of missing data and examine descriptive statistics and intercorrelations for all study variables. Second, we report the results from the unconditional growth models that explore developmental trajectories of emotion regulation and negativity across early childhood.1 Next, we report results from the explanatory models that characterize how well changes in children’s emotion regulation were predicted by maternal depression and children’s RSA.2 The Maternal Depressive Symptomatology × Child RSA interaction terms were included as predictors of the slope to explore whether trajectories of emotion regulation and negativity vary over time as a function of maternal depressive symptomatology and whether the magnitude of this relation depends on the level of children’s RSA.
Preliminary Analyses
Missing data
The use of HLM accounts for missing data longitudinally under the assumption that the data are missing at random (MAR). This indicates specifically that the missing data are predicted by the available data included in the model (Singer & Willett, 2003). Thus, despite attrition between 4 and 7 years of age, the analysis included all participants who had some outcome data. Examination of patterns of missing data revealed that missing data were predicted by the continuous 4-year variables included in the model, as determined using Little’s MCAR test, χ2(669) = 808.39, p < .001, indicating that the data were MAR as opposed to missing completely at random (MCAR; Little & Rubin, 1987). HLM does not allow for missing data within the time-invariant (Level 2) predictor variables, therefore data were imputed for Level 2 predictor variables. Listwise deletion of cases without complete data would have resulted in a reduction in sample size, which would have produced a significant loss in power and possible bias. The amount of missing data for any one variable was relatively small: maternal depressive symptomatology, 15.5%; baseline RSA, 17.8%; and ΔRSA, 19.8%. Missing values were imputed through maximum likelihood estimation using the expectation maximization method algorithm in SPSS 14. The expectation maximization method is an iterative process to impute missing values that has been found to be superior to listwise deletion, mean substitution, and multiple regression (Garson, 2006). All analyses presented are based on the imputed Level 2 data.
Descriptive statistics
Maternal negative parenting behavior was moderately positively skewed and therefore was square root transformed prior to any analyses. Descriptive statistics for all study variables are presented in Table 1. Intercorrelations among study variables indicate that maternal depressive symptomatology was associated with children’s emotion regulation and negativity, whereas children’s baseline RSA and ΔRSA were generally not (Table 2).
Table 1.
Descriptive Statistics for Predictor and Outcome Measures
| Measure | n | M | SD | Range |
|---|---|---|---|---|
| 4-year measures | ||||
| Negative parentinga | 269 | 1.80 | 0.15 | 1.47-2.45 |
| Maternal depressive symptomatology | 269 | 51.59 | 9.98 | 34.00-81.00 |
| Baseline respiratory sinus arrhythmia (RSA) | 269 | 5.83 | 1.16 | 1.05-10.20 |
| ΔRSA (Baseline-Attention) | 269 | 0.26 | 0.49 | -1.41-2.36 |
| Emotion regulation | 269 | 3.33 | 0.31 | 2.13-4.00 |
| Negativity | 269 | 1.90 | 0.37 | 1.13-3.07 |
| 5-year measures | ||||
| Emotion regulation | 236 | 3.33 | 0.33 | 2.38-4.00 |
| Negativity | 236 | 1.91 | 0.39 | 1.13-3.13 |
| 7-year measures | ||||
| Emotion regulation | 221 | 3.40 | 0.38 | 1.00-3.07 |
| Negativity | 221 | 1.72 | 0.34 | 2.25-4.00 |
Descriptives are for square-root-transformed variable.
Table 2.
Intercorrelations for Study Variables
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Predictor variables | ||||||||||
| 1. Negative parentinga | — | |||||||||
| 2. Maternal depressive symptomatology | .13* | — | ||||||||
| 3. Baseline respiratory sinus arrhythmia (RSA) | .02 | -.02 | — | |||||||
| 4. ΔRSA (Baseline - Attention) | .06 | .08 | .16*** | — | ||||||
| Outcome variables | ||||||||||
| 5. Emotion regulation, 4-year | -.04 | -.11 | -.13* | -.08 | — | |||||
| 6. Negativity, 4-year | .14* | .38*** | .08 | .05 | -.37*** | — | ||||
| 7. Emotion regulation, 5-year | .03 | -.17*** | -.08 | .02 | .59*** | -.40*** | — | |||
| 8. Negativity, 5-year | .07 | .33*** | .08 | -.01 | -.30*** | .79*** | -.44*** | — | ||
| 9. Emotion regulation, 7-year | -.04 | -.31*** | -.10 | .04 | .53*** | -.38*** | .67*** | -.40*** | — | |
| 10. Negativity, 7-year | -.02 | .41*** | -.03 | -.06 | -.30*** | .73*** | -.40*** | .78*** | -.48*** | — |
Square-root-transformed negative parenting.
p < .05.
p < .001.
Developmental Trajectories of Emotion Regulation and Negativity in Early Childhood
Unconditional growth models were fit to explore the developmental trajectories of children’s emotion regulation and negativity from 4 to 7 years of age (Table 3). The fixed effects indicated that from 4 to 7 years of age, children’s emotion regulation increased on average by 0.002 points each month (range of individual estimates = -0.004 to 0.006), with an average increase from 4 to 7 years of 0.07 points. At 7 years of age, the average emotion regulation score was 3.39. The correlation between the slope and children’s level of emotion regulation at age 7 was .40, indicating that greater increases in emotion regulation over time were associated with higher emotion regulation scores at age 7. Negativity decreased from 4 to 7 years of age at a rate of 0.005 points each month (range of individual estimates = -0.009 to -0.001), with an average decrease from 4 to 7 years of 0.18 points. At 7 years of age, the average estimated negativity score was 1.76. The correlation between the slope and children’s negativity when they were 7 years of age was .35. The parameter estimates had adequate reliability for both emotion regulation (intercept reliability = .64, slope reliability = .17) and negativity (intercept reliability = .76, slope reliability = .16).
Table 3.
Unconditional Growth Models for Emotion Regulation and Negativity
| Regulation |
Negativity |
|||||
|---|---|---|---|---|---|---|
| Fixed effects | Coefficienta | SE | t | Coefficienta | SE | t |
| Intercept (90 months) | 3.39 | .02 | 158.52*** | 1.76 | .02 | 73.77*** |
| Slope | .002 | .001 | 3.55** | -.005 | .00 | -10.05*** |
| Random effects | Variance component | df | χ2 | Variance component | df | χ2 |
| Intercept (90 months) | .08 | 242 | 763.90*** | .12 | 242 | 1,243.10*** |
| Slope | .00001 | 242 | 296.30* | .00 | 242 | 294.39* |
The coefficient represents the change that occurs in one-month increments.
p < .05.
p < .01.
p < .001.
The variances around the intercept and slope (random effects) indicate whether the parameter estimates varied across children and represent individual differences in the linear change that occurred from 4 to 7 years of age and overall levels of regulation and negativity at age 7. For both emotion regulation and negativity, the random effects were significant (Table 3). This indicates that there was substantial interindividual heterogeneity that can be explained by including predictors in the model.
Emotion Regulation and Negativity Trajectories
Next we examined whether maternal depressive symptomatology and child RSA, when children were 4 years of age, predicted both the rate of change in emotion regulation and negativity over time and children’s level of emotion regulation and negativity when they were 7 years of age. To control for parenting behavior we included observed maternal negative parenting as a predictor of both the intercept and the slope. The interaction terms between Maternal Depressive Symptomatology × Baseline RSA and Maternal Depressive Symptomatology × ΔRSA during an attention task were also included in the model as predictors of the intercept and slope. These results indicated whether trajectories of emotion regulation and negativity varied over time as a function of maternal depressive symptomatology and whether the magnitude of this relation depended on the level of children’s RSA.
Results for emotion regulation are displayed in Table 4. The fixed effects indicated that higher mean levels of emotion regulation at year 7 (intercept) were predicted by lower levels of maternal depressive symptomatology and lower baseline RSA. Girls were, on average, marginally more likely to have better emotion regulation than boys. There was also a significant Maternal Depressive Symptomatology × Baseline RSA interaction (Figure 1). Simple slopes analyses indicated that for children with high baseline RSA, greater maternal depressive symptomatology was associated with lower levels of emotion regulation at age 7 (simple slope = -.02, SE = .003, t = -5.71, p < .001), whereas the line representing low baseline RSA was not significant (simple slope = -.005, SE = .003, t = -1.61, ns).
Table 4.
Emotion Regulation Trajectories
| Fixed effects | Coefficienta | SE | t |
|---|---|---|---|
| Intercept (90 months) | 3.35 | .030 | 109.74*** |
| Female | .072 | .040 | 1.81† |
| Negative parenting | -.012 | .14 | -0.08 |
| Maternal depressive symptomatology (MDS) | -.010 | .002 | -5.17*** |
| Baseline respiratory sinus arrhythmia (RSA) | -.036 | .018 | -1.99* |
| ΔRSA (Baseline - Attention Task) | .055 | .040 | 1.38 |
| MDS × Baseline RSA | -.005 | .002 | -2.80** |
| MDS × ΔRSA | -.001 | .004 | -0.19 |
| Slope | .002 | .001 | 2.61* |
| Female | -.001 | .001 | -0.68 |
| Negative parenting | -.0003 | .004 | -0.10 |
| MDS | -.0002 | .000 | -2.85** |
| Baseline RSA | -.0003 | .001 | 0.57 |
| ΔRSA (Baseline - Attention Task) | .003 | .001 | 1.97* |
| MDS × Baseline RSA | -.0001 | .000 | 2.66** |
| MDS × ΔRSA | -.000 | .000 | -0.02 |
| Random effects | Variance component | df | χ2 |
| Intercept | .06 | 235 | 675.32*** |
| Slope | .000 | 235 | 279.30* |
The coefficient represents the change that occurs in one-month increments.
p < .10.
p < .05.
p < .01.
p < .001.
Figure 1.
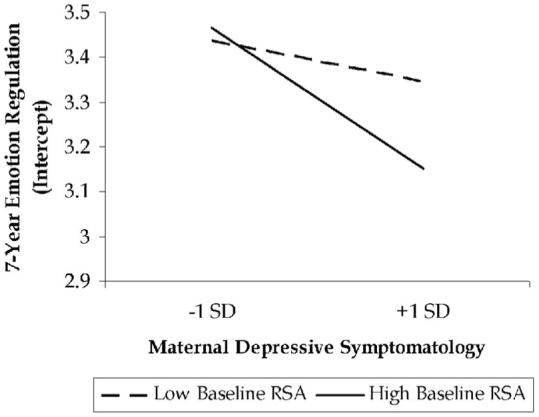
Interaction between maternal depressive symptomatology and child’s baseline respiratory sinus arrhythmia (RSA) predicting 7-year emotion regulation.
For the change in emotion regulation from 4 to 7 years of age, we found that having lower levels of maternal depressive symptomatology was associated with greater linear increases in emotion regulation over time (simple slope = .002, SE = .001, t = 2.16, p < .05), whereas higher levels of maternal depressive symptomatology were associated with stable levels of emotion regulation over time (simple slope = -.001, SE = .001, t = -1.33, ns). In addition, greater ΔRSA was associated with steeper linear increases in emotion regulation (simple slope = .004, SE = .001, t = 3.50, p < .001), whereas lower ΔRSA scores were associated with stable levels of emotion regulation across early childhood (simple slope = .001, SE = .001, t = 0.97, ns). There was also a significant Maternal Depressive Symptomatology × Baseline RSA × Age interaction predicting the change in emotion regulation over time (Figure 2). The simple slopes were significant for low depressive symptomatology/low baseline RSA (simple slope = .006, SE = .001, t = 4.85, p < .001), low depressive symptomatology/high baseline RSA (simple slope = .04, SE = .001, t = 26.55, p < .001), and high depressive symptomatology/high baseline RSA (simple slope = -.03, SE = .001, t = -22.02, p < .001). The simple slope representing high maternal depressive symptomatology/low baseline RSA was not significantly different from zero (simple slope = -.001, SE = .001, t = -0.84, ns), indicating that for this group emotion regulation was stable over time.
Figure 2.
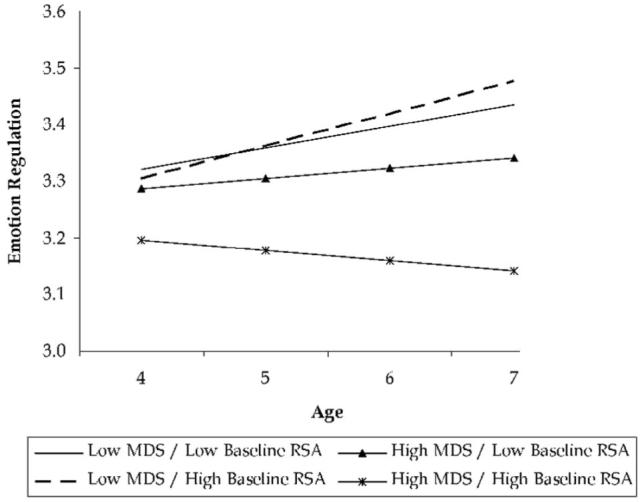
Interaction between maternal depressive symptomatology (MDS), child’s baseline respiratory sinus arrhythmia (RSA), and age predicting the change in emotion regulation from 4 to 7 years of age.
To test the fit of the conditional model versus the unconditional growth model, we used the deviance statistic, χ2(14) = 44.97, p < .001, which indicated that the conditional model provides a better fit than the unconditional growth model.
Results for negativity are displayed in Table 5. The fixed effects indicated that being male and experiencing greater maternal depressive symptomatology were associated with greater mother-reported negativity, on average, at 7 years of age (intercept). In addition, there was a Depressive Symptomatology ×ΔRSA interaction predicting the intercept (Figure 3) that approached significance. Simple slopes analyses indicated that for children who had higher vagal suppression (ΔRSA), greater maternal depressive symptomatology tended to be associated with greater negativity (simple slope = .02, SE = .003, t = 6.01, p < .001). Greater maternal depressive symptomatology was also associated with greater negativity under conditions of low vagal suppression (ΔRSA); however, the slope was less steep (simple slope = .01, SE = .003, t = 3.12, p < .01).
Table 5.
Emotional Negativity Trajectories
| Fixed effects | Coefficienta | SE | t |
|---|---|---|---|
| Intercept (90 months) | 1.81 | .030 | 59.87*** |
| Female | -.113 | .04 | -2.62* |
| Negative parenting | .005 | .15 | 0.04 |
| Maternal depressive symptomatology (MDS) | .013 | .002 | 6.38*** |
| Baseline respiratory sinus arrhythmia (RSA) | -.012 | .021 | -0.58 |
| ΔRSA (Baseline - Attention Task) | -.067 | .047 | -1.44 |
| MDS × Baseline RSA | -.001 | .002 | -0.44 |
| MDS × ΔRSA | .008 | .004 | 1.77† |
| Slope | -.006 | .001 | -8.51*** |
| Female | .002 | .001 | 1.62 |
| Negative parenting | -.006 | .003 | -1.74† |
| MDS | .000 | .000 | 0.50 |
| Baseline RSA | -.001 | .001 | -2.62* |
| ΔRSA (Baseline - Attention Task) | -.002 | .001 | -1.75† |
| MDS × Baseline RSA | -.000 | .000 | -0.95 |
| MDS × ΔRSA | .000 | .000 | 1.36 |
| Random effects | Variance component | df | χ2 |
| Intercept | .09 | 235 | 1,026.28*** |
| Slope | .000 | 235 | 270.88† |
The coefficient represents the change that occurs in one-month increments.
p < .10.
p < .01.
p < .001.
Figure 3.
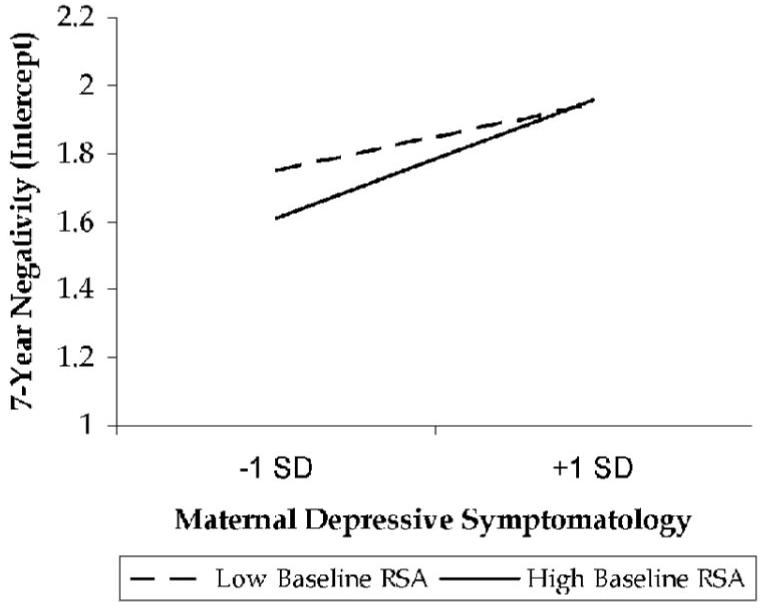
Interaction between maternal depressive symptomatology and child’s vagal regulation (ΔRSA) predicting 7-year negativity.
The change in negativity from 4 to 7 years (slope) was predicted by children’s baseline RSA, negative maternal parenting behavior, and children’s ΔRSA; the simple slopes are reported for these cross-level interactions. Specifically, greater linear decline in negativity from 4 to 7 years of age was associated with higher baseline RSA (simple slope + 1 SD = -.007, SE = .001, t = -8.27, p < .001; simple slope - 1 SD = -.004, SE = .001, t = -4.96, p < .001). Higher levels of negative maternal parenting behavior were marginally associated with slower declines in negativity (simple slope + 1 SD = -.002, SE = .001, t = -1.71, p = .08; simple slope - 1 SD = .0003, SE = .001, t = 0.36, ns). In addition, higher levels of ΔRSA were marginally associated with a steeper linear decline in negativity from 4 to 7 years of age (simple slope + 1 SD = -.007, SE = .001, t = -7.99, p < .001; simple slope - 1 SD = -.005, SE = .001, t = -5.83, p < .001). To test the fit of the conditional model versus the unconditional growth model, we used the deviance statistic, χ2(14) = 82.90, p < .001, which indicated that the conditional model provides a better fit than the unconditional growth model.
Finally, the random effects from the conditional models indicated that for both emotion regulation and negativity, there was still significant variation in the intercept and slope that was not accounted for by the predictors included in the model.
Discussion
The current study investigated the growth and change that occurred in children’s emotion regulation and the expression of negative affect during the transition from preschool to school age in a large community sample. Given that deficits in the emotion regulation process have been linked to adjustment problems, including difficulties with peers and an increased risk for later psychopathology, it is important to develop a more nuanced understanding of the factors that are associated with individual differences in patterns of emotional reactivity, regulation, and expressiveness throughout the early childhood years. Specifically, we modeled trajectories of children’s emotion regulation and negativity from 4 to 7 years of age, as reported by the mother, where the intercept was coded to predict the children’s average level of emotion regulation and negativity at the end of the developmental period examined. Maternal depressive symptomatology and children’s RSA and the ΔRSA at age 4 were explored as factors that may predict individual differences in children’s emotion regulation and negativity trajectories. Given that several studies have found maternal depression to be a risk factor for children’s problem behavior, we were particularly interested in whether child physiological factors would buffer the effect of maternal depressive symptomatology on children’s trajectories of emotion regulation and their expression of negative affect.
The first aim of the study was to examine the trajectories of emotion regulation and negativity across early childhood. Results from the unconditional growth models supported our prediction that emotion regulation would increase and emotional negativity would decrease over time. Given children’s increasing cognitive abilities and the maturation of the prefrontal cortex and the anterior cingulate cortex, which have been associated with emotion regulation processes (Ochsner, Bunge, Gross, & Gabrieli, 2002; Ochsner & Gross, 2005), we expect that children’s increasing ability for regulating their emotions may be due, in part, to their ability to be more planful in and exert greater effortful control over their behavior. These underlying developmental achievements allow them to utilize more complex strategies, such as reappraising negative events to find meaning in them or planning to avoid certain situations that may cause distress, to manage their emotions in emotionally arousing situations (Larsen & Prizmic, 2004). Important changes also occur in the developmental context during this period of time, particularly in school, where larger class sizes and decreased supervision make children’s ability to regulate their emotional states important for their academic success (Bronson, Tivnan, & Seppanen, 1995; Rimm-Kaufman & Pianta, 2000). These classroom changes occur in conjunction with greater interaction with peers, providing different situations in which children can practice their emotion regulation strategies (Fox & Calkins, 2003). Overall, this highlights the need to explore the developmental course of emotion regulation processes through childhood.
While, on average and as expected, children’s ability to control their emotions increased and their negativity decreased from 4 to 7 years of age, there was also significant variability in the intercept and slope for both emotion regulation and negativity. This indicated that there were important individual differences in the development of emotion regulation processes over time. In exploring the predictors of individual differences in children’s trajectories, we found that the pattern of results differed for emotion regulation and negativity, further supporting the need to examine the reactivity and control dimensions of the emotion regulation process independently (Calkins & Hill, 2007; Gross & Thompson, 2007). For emotion regulation, interesting interactions emerged predicting children’s emotion regulation at age 7 and the change in emotion regulation across early childhood even after controlling for maternal negative parenting behavior. There was a significant Maternal Depressive Symptomatology × Children’s Baseline RSA interaction predicting emotional regulation at age 7. Specifically, children who exhibit higher levels of baseline RSA in conjunction with higher levels of maternal depressive symptoms have lower overall levels of emotion regulation at age 7. Contrary to our hypothesis, higher baseline RSA appeared to exacerbate the effect of maternal depressive symptomatology on children’s emotion regulation rather than buffer it. Specifically, when maternal depressive symptomatology was high, children had lower overall emotion regulation. In some instances, baseline RSA has been associated with appropriate observed emotional reactivity (Stifter & Fox, 1990). Specifically, baseline RSA has been found to be positively correlated with positive emotional reactivity and negatively correlated with negative emotional reactivity (Calkins, 1997). However, Cole et al. (1996) found that children who expressed greater negative emotionality during negative mood eliciting events had significantly higher baseline RSA relative to children who were able to modulate their response. This research suggests that children of depressed mothers, who have been found to be more likely to react negatively in response to stressful situations, may have poorer socioemotional outcomes associated with higher baseline RSA (Goodman & Gotlib, 1999).
Maternal depressive symptomatology predicted the change that occurred in emotion regulation across early childhood. Mothers who reported fewer depressive symptoms reported that their children’s ability to regulate their emotions increased over time, but when mothers reported more depressive symptoms, children’s emotion regulation remained relatively stable across early childhood. It may be the case that children whose mothers exhibit more depressive symptoms may not be learning more complex strategies for dealing with emotion, particularly negative emotion, which they otherwise would acquire given the cognitive development that occurs during this period. This is consistent with other research demonstrating that young children of depressed mothers are more likely to focus on a desired object rather than use distractions during a delay task, which is a relatively immature way to manage one’s emotions during this task (Silk et al., 2006). In these instances, there is a greater likelihood that mothers are modeling more maladaptive strategies for dealing with emotionally challenging events (Goodman & Gotlib, 1999). Research has also found that individuals’ expectations for good versus bad events are linked to depressive symptoms (Peterson & Vaidya, 2001). If this is the case, mothers may also be modeling a general explanatory style of expecting bad things to happen, which may affect how children behave, particularly in emotionally arousing ambiguous situations.
We had hypothesized that higher levels of vagal regulation, indexed by the ΔRSA from the baseline to the attention task, would be associated with better emotion regulation over time. Indeed, we found that for children who exhibited greater vagal regulation, their ability to regulate their emotions increased more rapidly from 4 to 7 years of age as compared with children with low vagal regulation. This contributes to the growing body of research that has shown a strong link between greater vagal regulation during emotionally or cognitively demanding tasks and children’s ability to manage their emotions (Calkins, 1997; Calkins & Dedmon, 2000; Calkins & Keane, 2004). Considered within the larger framework of self-regulation, these results support the view that more basic physiological regulatory capacities earlier in childhood do have an effect on the development of observable aspects of emotion regulation later in childhood (Calkins & Fox, 2002; Calkins & Hill, 2007); however, this effect may differ depending on the context in which it occurs. Specifically, in the current study it appears to be the case that children who exhibited higher levels of baseline RSA in families where mothers are experiencing more depressive symptoms may be, in general, more emotionally reactive.
In addition, there was a significant three-way Maternal Depressive Symptomatology × Baseline RSA × Age interaction that predicted how children’s emotion regulation changed from 4 to 7 years of age. It appears that the development of emotion regulation was primarily inhibited by the presence of maternal depressive symptoms when children had higher baseline RSA. Specifically, the simple slopes analyses indicated that when mothers have higher levels of depressive symptoms and children have high baseline RSA scores, these children have poorer regulation skills and they tend to decrease (0.05 points) over time rather than increase. When mothers have high depressive symptoms and children have low baseline RSA, children’s emotion regulation remains stable and does not change significantly over time. This is in contrast to the other groups—low depressive symptoms/low baseline RSA (increased 0.12 points) and low depressive symptoms/high baseline RSA (increased 0.17 points)—who exhibited significant increases in emotion regulation across early childhood.
Overall, three important points emerge from our findings regarding emotion regulation. First, the early development of the ability to regulate oneself at the level of physiology is important for the later development of more complex emotion regulation processes. Second, as we expected, it appears that children have better emotion regulation over time when their mothers report fewer depressive symptoms versus when mothers report more depressive symptoms. This indicates that maternal depressive symptomatology does present a specific risk for deficits in children’s ability to manage their emotions. Third, low levels of physiological reactivity appear to buffer children from some of the negative consequences of maternal depressive symptomatology such that children with low baseline RSA evidence increases over time in their ability to control their emotions, albeit to a lesser extent than those children whose mothers report fewer depressive symptoms. This is consistent with the biological sensitivity to context theory, which proposes that high biological reactivity may operate differentially depending on the context in which it occurs (Boyce & Ellis, 2005; Ellis, Essex, & Boyce, 2005). Specifically, under stressful conditions high reactivity may actually result in maladaptive outcomes, whereas high reactivity may be protective in low-stress conditions. Indeed, it may be the case that children who are more physiologically reactive are ill equipped to deal with the stresses that may arise given their sensitivity to the negative aspects of the family environment, such as a less supportive mother-child relationship and more overall family negativity, when mothers report higher levels of depressive symptoms. When trying to intervene with those children who are at the greatest risk for later serious maladjustment problems, understanding the person-environment fit may be particularly important.
As noted previously, the pattern of results differed for children’s trajectories of emotional negativity. On average, boys evidenced marginally higher levels of negativity at age 7 despite the fact that no gender differences emerged with respect to children’s ability to regulate their emotions. This is consistent with research that has found that boys are more likely to exhibit externalizing behavior problems than girls (Maccoby, 1998). The link between sex and regulation processes may become more apparent during adolescence given that there are different social norms for men and women in terms of emotional expression (Brody, 2000). In the current study, what may have emerged is the beginning of a possible divergence in emotion regulation processes for girls and boys. In addition, consistent with our hypothesis, children were more negative when they were 7 years old if their mothers reported higher levels of depressive symptoms when they were 4. There was also a Maternal Depressive Symptomatology × Vagal Regulation interaction that approached significance, which, contrary to what we had hypothesized, indicated that maternal depressive symptoms were more positively associated with children’s higher levels of negativity when children had higher levels of vagal regulation (ΔRSA).
We found, as expected, that higher levels of maternal depressive symptomatology were associated with slower declines in negativity across early childhood. This is not unexpected, given that when mothers report greater depressive symptoms they are in general more likely to exhibit greater negative trait affect and to engage in more negative behaviors (Rogosch et al., 2004). This modeling of negative affect in the family may influence children’s expression of negative affect such that greater negative affect appears more normative in these families. Indeed, maternal negative parenting behavior was also marginally associated with slower declines in children’s negative emotional behavior over time. Of interest, the effect of baseline RSA differed from that found with emotion regulation. Indeed, we found that children who exhibited higher levels of baseline RSA had greater declines in negativity across early childhood. This is different from the results for emotion regulation, which suggested that children with high baseline RSA did not exhibit increases in their ability to manage their emotions. It is, however, consistent with earlier research, which has found that high baseline RSA is associated with children’s appropriate emotional reactivity (Porges, 1991; Stifter & Fox, 1990). The results also indicated, as hypothesized, that greater vagal regulation was marginally associated with greater declines in negativity over time. There is some research to suggest that baseline RSA, which is regarded as the underlying physiological basis for observed behavioral reactivity, is more strongly and consistently correlated with observed measures of behavioral reactivity than regulation, whereas vagal regulation appears to be correlated with observed measures of regulation and not reactivity (Calkins, 1997; Porges, 1991).
The study has a number of limitations that must be noted. First, the sample was overselected for externalizing behavior problems and thus may not be representative of community samples, given that emotion dysregulation has been implicated in the stability of externalizing problems across childhood. However, it should be noted that the levels of baseline RSA and ΔRSA are consistent with other studies with similarly aged children (Blair & Peters, 2003; Kennedy, Rubin, Hastings, & Maisel, 2004). Second, measures of emotion regulation and negativity were obtained exclusively through maternal report. Given that maternal depressive symptomatology was also measured through maternal report, there was a greater likelihood of single-rater bias. However, important elements of the study included children’s physiological regulation, which would not have suffered from this problem. It should be noted, however, that maternal reports of emotion regulation and negativity were correlated with teacher reports from the same year. In addition, there is some evidence that maternal reports of emotion regulation and reactivity are valid measures of children’s observed behavior. Earlier research has found that maternally reported anger and soothability were correlated with observed distress and specific emotion regulation strategies (Calkins et al., 1999). It is also important to consider that in longitudinal studies across childhood, regulation is assessed in different types of tasks and children engage in different types of strategies (LAB-TAB; Goldsmith & Rothbart, 1993). Maternal reports of children’s emotional behavior, therefore, are one of the best methods for examining trajectories of emotion regulation from 4 to 7 years of age given the need to use the same measures across the different assessments (Singer & Willett, 2003). In addition, although the mothers in the current study were not diagnosed as clinically depressed, it should be noted that there is conflicting research regarding reports of children’s behavior from depressed mothers. Some studies show that depressed mothers may overreport symptoms (Chilcoat & Breslau, 1997), while others do not (Tarullo, Richardson, Radke-Yarrow, & Martinez, 1995). It is also important to note that genetic sources of shared variance between mothers and children were not included in this study. Finally, we were not able to explore nonlinear patterns of change in emotion regulation and negativity given that we had only three waves of data available.
Overall, this study extends the literature on the development of children’s emotion regulation through early childhood beyond the infant-toddler period. Our data appear to demonstrate that children’s emotion regulation processes change across early childhood such that reactivity decreases and emotion control increases over time. There are individual differences in the change that occurs in children’s emotion regulation and negativity across early childhood. Several interesting results emerged highlighting the interactions between children’s physiological indices of reactivity and regulation and their socialization environment in predicting observed emotion regulation and the expression of negative affect. Although it appears that development of emotion regulation over time is compromised when children grow up in the context of maternal depression, there is some evidence that children’s capacity for physiological regulation may buffer some of the adverse consequences associated with maternal depressive symptomatology. In the current study we focused specifically on negative reactivity, although there is emerging evidence that positive emotional reactivity is also linked to children’s behavioral outcomes, including externalizing behavior problems and prosocial behavior (Rydell et al., 2003), suggesting that it is an area that needs to be explored further and in conjunction with negative reactivity. The results of this study emphasize the importance of developing an understanding of the factors that may inhibit or support the development of emotion regulation across early childhood.
Acknowledgments
This research was supported by a National Institute of Mental Health (NIMH) Behavioral Science Track Award for Rapid Transition (MH 55625), an NIMH FIRST Award (MH 55584), and an NIMH K-award (MH 74077) to Susan D. Calkins and by an NIMH grant (MH 58144A) awarded to Susan D. Calkins, Susan P. Keane, and Marion O’Brien. We thank the parents and children who have repeatedly given their time and effort to participate in this research. Additionally, we are grateful to the entire RIGHT Track staff for their help in data collection, entry, and coding.
Footnotes
The unconditional linear growth models for emotion regulation and negativity were specified as follows: Level 1: Yij = π0i + π1i (age in months - 90) + eij, where π0i represents the score on the outcome at age 7 (intercept); π1i represents the rate of change in the outcome in 1-month increments; and eij represents the residual for person j at time i. Level 2: π0i = β00 + r0i, π1i = β10 + r1i. In the Level 2 equations, π0i and π1i represent the population average intercept and slope, respectively, and r0i and r1i represent the variance or random effects associated with these estimates.
The Level 2 equations for the explanatory models, which depict the interindividual variation in growth trajectories, were specified as follows: π0i = β00 + β01 (female) + β02 (negative parenting) + β03 (MDS) + β04 (baseline RSA) + β05 (ΔRSA) + β06 (MDS) (baseline RSA) + β07 (MDS) (ΔRSA) + r0i; and π1i = β10 + β01 (female) + β12 (negative parenting) + β13 (MDS) + β14 (baseline RSA) + β15 (ΔRSA) + β16 (MDS) (baseline RSA) + β17 (MDS) (ΔRSA) + r1i, where π0i and π1i represent the population average intercept and slope, respectively, for individuals, with a value of zero for all predictor variables (i.e., female, negative parenting, MDS, baseline RSA, ΔRSA). The βs represent the average difference in the intercept and linear slope for a one-unit difference in the specific predictor. Finally, 0i and r1i represent the variance or random effects associated with these estimates.
Contributor Information
Alysia Y. Blandon, Department of Human Development and Family Studies, University of North Carolina at Greensboro
Susan D. Calkins, Department of Human Development and Family Studies, University of North Carolina at Greensboro
Susan P. Keane, Department of Psychology, University of North Carolina at Greensboro
Marion O’Brien, Department of Human Development and Family Studies, University of North Carolina at Greensboro.
References
- Achenbach TM. Manual for the Child Behavior Checklist/2-3 and 1992 profile. Department of Psychiatry, University of Vermont; Burlington: 1992. [Google Scholar]
- Aiken LS, West SG. Multiple regression: Testing and interpreting interactions. Sage; London: 1991. [Google Scholar]
- Beauregard M, Lévesque J, Paquette V. Neural basis of conscious and voluntary self-regulation of emotion. In: Beauregard M, editor. Consciousness, emotional self-regulation and the brain. John Benjamins; Philadelphia: 2004. pp. 35–59. [Google Scholar]
- Blair C, Peters R. Physiological and neurocognitive correlates of adaptive behavior in preschool among children in Head Start. Developmental Neuropsychology. 2003;24:479–497. doi: 10.1207/S15326942DN2401_04. [DOI] [PubMed] [Google Scholar]
- Boyce WT, Ellis BJ. Biological sensitivity to context: I. An evolutionary-developmental theory of the origins and functions of stress reactivity. Development and Psychopathology. 2005;17:273–301. doi: 10.1017/s0954579405050145. [DOI] [PubMed] [Google Scholar]
- Brody LR. The socialization of gender differences in emotional expression: Display rules, infant temperament, and differentiation. In: Fischer A, editor. Gender and emotion: Social psychological perspectives. Cambridge University Press; New York: 2000. pp. 24–47. [Google Scholar]
- Bronson M, Tivnan T, Seppanen P. Relations between teacher and classroom activity variables and the classroom behaviors of prekindergarten children in Chapter 1 funded programs. Journal of Applied Developmental Psychology. 1995;16:253–282. [Google Scholar]
- Calkins SD. Origins and outcomes of individual differences in emotion regulation. In: Fox NA, editor. Emotion regulation: Behavioral and biological considerations. 23. Vol. 59. 1994. pp. 53–72. Monographs of the Society for Research in Child Development. Serial No. 240. [PubMed] [Google Scholar]
- Calkins SD. Cardiac vagal tone indices of temperamental reactivity and behavioral regulation in young children. Developmental Psychobiology. 1997;31:125–135. doi: 10.1002/(sici)1098-2302(199709)31:2<125::aid-dev5>3.0.co;2-m. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Dedmon SE. Physiological and behavioral regulation in two-year-old children with aggressive/destructive behavior problems. Journal of Abnormal Child Psychology. 2000;2:103–118. doi: 10.1023/a:1005112912906. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Fox NA. Self-regulatory processes in early personality development: A multilevel approach to the study of childhood social withdrawal and aggression. Development and Psychopathology. 2002;14:477–498. doi: 10.1017/s095457940200305x. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Gill KA, Johnson MC, Smith C. Emotional reactivity and emotion regulation strategies as predictors of social behavior with peers during toddlerhood. Social Development. 1999;8:310–341. [Google Scholar]
- Calkins SD, Graziano P, Keane SP. Cardiac vagal regulation to emotional challenge differentiates among child behavior problem subtypes. Biological Psychology. 2007;74:144–153. doi: 10.1016/j.biopsycho.2006.09.005. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Calkins SD, Hill A. Caregiver influences on emerging emotion regulation: Biological and environmental transactions in early development. In: Gross JJ, editor. Handbook of emotion regulation. Guilford Press; New York: 2007. pp. 3–26. [Google Scholar]
- Calkins SD, Howse RB. Individual differences in self-regulation: Implications for childhood adjustment. In: Philipport P, Feldman RS, editors. The regulation of emotion. Erlbaum; Mahwah, NJ: 2004. pp. 307–332. [Google Scholar]
- Calkins SD, Johnson MC. Toddler regulation of distress to frustrating events: Temperamental and maternal correlates. Infant Behavior and Development. 1998;21:379–395. [Google Scholar]
- Calkins SD, Keane SP. Cardiac vagal regulation across the preschool period: Stability, continuity, and implications for childhood adjustment. Developmental Psychobiology. 2004;45:101–112. doi: 10.1002/dev.20020. [DOI] [PubMed] [Google Scholar]
- Calkins SD, Smith CL, Gill KL, Johnson MC. Maternal interactive style across contexts: Relations to emotional, behavioral and physiological regulation during toddlerhood. Social Development. 1998;7:350–369. [Google Scholar]
- Chilcoat HD, Breslau N. Does psychiatric history bias mothers’ reports? An application of a new analytic approach. Journal of the American Academy of Child and Adolescent Psychiatry. 1997;36:971–979. doi: 10.1097/00004583-199707000-00020. [DOI] [PubMed] [Google Scholar]
- Cicchetti D. Developmental psychopathology: Reactions, reflections, projections. Developmental Review. 1993;13:471–502. [Google Scholar]
- Cole PM, Martin SE, Dennis TA. Emotion regulation as a scientific construct: Methodological challenges and directions for child development research. Child Development. 2004;75:317–333. doi: 10.1111/j.1467-8624.2004.00673.x. [DOI] [PubMed] [Google Scholar]
- Cole PM, Zahn-Waxler C, Fox NA, Usher BA, Welsh JD. Individual differences in emotion regulation and behavior problems in preschool children. Journal of Abnormal Psychology. 1996;105:518–529. [PubMed] [Google Scholar]
- Cummings EM, Davies PT. Maternal depression and child development. Journal of Child Psychology and Psychiatry. 1994;35:73–112. doi: 10.1111/j.1469-7610.1994.tb01133.x. [DOI] [PubMed] [Google Scholar]
- Cummings EM, Keller PS, Davies PT. Towards a family process model of maternal and paternal depressive symptoms: Exploring multiple relations with child and family functioning. Journal of Child Psychology and Psychiatry. 2005;46:479–489. doi: 10.1111/j.1469-7610.2004.00368.x. [DOI] [PubMed] [Google Scholar]
- DeGangi G, DiPietro J, Greenspan S, Porges SW. Psychophysiological characteristics of the regulatory disordered infant. Infant Behavior and Development. 1991;14:37–50. [Google Scholar]
- Derogatis LR. Manual for the Symptom Checklist 90 Revised (SCL-90R) Author; Baltimore: 1986. [Google Scholar]
- Derogatis LR, Cleary PA. Conformation of the dimensional structure of the SCL-90: A study in construct validation. Journal of Clinical Psychology. 1977;33:981–989. [Google Scholar]
- Downey G, Coyne JC. Children of depressed parents: An integrative review. Psychological Bulletin. 1990;108:50–76. doi: 10.1037/0033-2909.108.1.50. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Cumberland AL, Spinrad TL, Fabes R, Shepard SA, Reiser M, et al. The relations of regulation and emotionality to children’s externalizing and internalizing problem behavior. Child Development. 2001;72:1112–1134. doi: 10.1111/1467-8624.00337. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Fabes RA, Guthrie IK, Reiser M. Dispositional emotionality and regulation: Their role in predicting quality of social functioning. Journal of Personality and Social Psychology. 2000;78:136–157. doi: 10.1037//0022-3514.78.1.136. [DOI] [PubMed] [Google Scholar]
- Eisenberg N, Fabes RA, Murphy B, Maszk P, Smith M, Karbon M. The role of emotionality and regulation in children’s social functioning: A longitudinal study. Child Development. 1995;66:1360–1384. [PubMed] [Google Scholar]
- Eisenberg N, Guthrie IK, Fabes RA, Reiser M, Murphy BC, Holgren R, et al. The relations of regulation and emotionality to resiliency and competent social functioning in elementary school children. Child Development. 1997;68:295–311. [PubMed] [Google Scholar]
- Ellis BJ, Essex MJ, Boyce WT. Biological sensitivity to context: II. Empirical explorations of an evolutionary-developmental theory. Development and Psychopathology. 2005;17:303–328. doi: 10.1017/s0954579405050157. [DOI] [PubMed] [Google Scholar]
- El-Sheikh M, Harger J, Whitson SA. Exposure to interparental conflict and children’s adjustment and physical health: The moderating role of vagal tone. Child Development. 2001;72:1617–1636. doi: 10.1111/1467-8624.00369. [DOI] [PubMed] [Google Scholar]
- El-Sheikh M, Whitson SA. Longitudinal relations between marital conflict and child adjustment: Vagal regulation as a protective factor. Journal of Family Psychology. 2006;20:30–39. doi: 10.1037/0893-3200.20.1.30. [DOI] [PubMed] [Google Scholar]
- Fox NA. Dynamic cerebral processes underlying emotion regulation. In: Fox NA, editor. The development of emotion regulation: Biological and behavioral considerations. 23. Vol. 59. 1994. pp. 152–166. Monographs of the Society for Research in Child Development. Serial No. 240. [PubMed] [Google Scholar]
- Fox NA, Calkins SD. The development of self-control of emotion: Intrinsic and extrinsic influences. Motivation and Emotion. 2003;27:7–26. [Google Scholar]
- Garson GD. Data implications for missing values. Quantitative Research in Public Administration; from North Carolina State University PA 765: 2006. Retrieved February 1, 2006. Web site: http://www2.chass.Ncsu.edu/garson/pa765/missing.htm. [Google Scholar]
- Goldsmith HH, Rothbart MK. The Laboratory Temperament Assessment Battery: Locomotor Version 2.02 (LAB-TAB) University of Wisconsin Press; Madison: 1993. [Google Scholar]
- Goodman SH, Gotlib IH. Risk for psychopathology in the children of depressed mothers: A developmental model for understanding mechanisms of transmission. Psychological Review. 1999;106:458–490. doi: 10.1037/0033-295x.106.3.458. [DOI] [PubMed] [Google Scholar]
- Gross JJ, Thompson RA. Emotion regulation: Conceptual foundations. In: Gross JJ, editor. Handbook of emotion regulation. Guilford Press; New York: 2007. pp. 3–26. [Google Scholar]
- Gumora G, Arsenio WF. Emotionality, regulation, and school performance in middle school children. Journal of School Psychology. 2002;40:395–413. [Google Scholar]
- Gunnar MR, Porter FL, Wolf CM, Rigatuso J, Larson MC. Neonatal stress reactivity: Predictions of later emotional temperament. Child Development. 1995;66:1–13. doi: 10.1111/j.1467-8624.1995.tb00851.x. [DOI] [PubMed] [Google Scholar]
- Hollingshead AB. Four-Factor Index of Social Status. Yale University; New Haven, CT: 1975. [Google Scholar]
- Howse RB, Calkins SD, Anastopoulos AD, Keane SP, Shelton TL. Regulatory contributors to children’s kindergarten achievement. Early Education & Development. 2003;14:101–119. [Google Scholar]
- Huffman LC, Bryan YE, del Carmen R, Pederson FA, Doussard-Roosevelt JA, Porges SW. Infant temperament and cardiac vagal tone: Assessments at twelve weeks of age. Child Development. 1998;69:624–635. [PubMed] [Google Scholar]
- Kalpidou MD, Power TG, Cherry KE, Gottfried NW. Regulation of emotion and behavior among 3- and 5-year-olds. Journal of General Psychology. 2004;131:159–178. doi: 10.3200/GENP.131.2.159-180. [DOI] [PubMed] [Google Scholar]
- Keane SP, Calkins SD. Predicting kindergarten peer social status from toddler and preschool problem behavior. Journal of Abnormal Child Psychology. 2004;32:409–423. doi: 10.1023/b:jacp.0000030294.11443.41. [DOI] [PubMed] [Google Scholar]
- Keenan K. Emotion dysregulation as a risk factor for child psychopathology. Clinical Psychology: Science and Practice. 2000;7:418–434. [Google Scholar]
- Kennedy AE, Rubin KH, Hastings PD, Maisel B. Longitudinal relations between child vagal tone and parenting behavior: 2 to 4 years. Developmental Psychobiology. 2004;45:10–21. doi: 10.1002/dev.20013. [DOI] [PubMed] [Google Scholar]
- Kochanska G. Beyond cognitions: Expanding the search for early roots of internalization and conscience. Developmental Psychology. 1994;30:20–22. [Google Scholar]
- Kopp CB. Regulation of distress and negative emotions: A developmental view. Developmental Psychology. 1989;25:343–354. [Google Scholar]
- Larsen RJ, Prizmic Z. Affect regulation. In: Baumeister RF, Vohs KD, editors. Handbook of self-regulation: Research, theory, and applications. Guilford Press; New York: 2004. pp. 40–61. [Google Scholar]
- Little RJA, Rubin DB. Statistical analysis with missing data. Wiley; New York: 1987. [Google Scholar]
- Maccoby EE. The two-sexes: Growing apart, coming together. Harvard University Press; Cambridge, MA: 1998. [Google Scholar]
- Ochsner KN, Bunge SA, Gross JJ, Gabrieli JDE. Rethinking feelings: An fMRI study of the cognitive regulation of emotion. Journal of Cognitive Neuroscience. 2002;14:1215–1229. doi: 10.1162/089892902760807212. [DOI] [PubMed] [Google Scholar]
- Ochsner KN, Gross JJ. The cognitive control of emotion. Trends in Cognitive Science. 2005;9:242–249. doi: 10.1016/j.tics.2005.03.010. [DOI] [PubMed] [Google Scholar]
- Peterson C, Vaidya RS. Explanatory style, expectations, and depressive symptoms. Personality and Individual Differences. 2001;31:1217–1223. [Google Scholar]
- Porges SW. U.S. Patent No. 4520944. U.S. Patent Office; Washington, DC: Method and apparatus for evaluating rhythmic oscillations in aperiodic physiological response systems. 1985
- Porges SW. Vagal tone: Autonomic mediator of affect. In: Garber JA, Dodge KA, editors. The development of affect regulation and dysregulation. Cambridge University Press; New York: 1991. pp. 111–128. [Google Scholar]
- Porges SW. Physiological regulation in high-risk infants: A model for assessment and potential intervention. Development and Psychopathology. 1996;8:43–58. [Google Scholar]
- Porges SW. The polyvagal theory: Phylogenetic substrates of a social nervous system. International Journal of Psychophysiology. 2001;42:123–146. doi: 10.1016/s0167-8760(01)00162-3. [DOI] [PubMed] [Google Scholar]
- Porges SW. The polyvagal theory: Phylogenetic contributions to social behavior. Physiology and Behavior. 2003;79:503–513. doi: 10.1016/s0031-9384(03)00156-2. [DOI] [PubMed] [Google Scholar]
- Porges SW, Doussard-Roosevelt JA, Maita AK. Vagal tone and the physiological regulation of emotion. In: Fox NA, editor. Emotion regulation: Behavioral and biological considerations. 23. Vol. 59. 1994. pp. 167–186. Monographs of the Society for Research in Child Development. Serial No. 240. [PubMed] [Google Scholar]
- Porges SW, Doussard-Roosevelt JA, Portales AL, Greenspan SI. Infant regulation of the vagal “brake” predicts child behavior problems: A psychobiological model of social behavior. Developmental Psychobiology. 1996;29:697–712. doi: 10.1002/(SICI)1098-2302(199612)29:8<697::AID-DEV5>3.0.CO;2-O. [DOI] [PubMed] [Google Scholar]
- Preacher KJ, Curran PJ, Bauer DJ. Computational tools for probing interaction effects in multiple linear regression, multilevel modeling, and latent curve analysis. Journal of Educational and Behavioral Statistics. 2006;31:437–448. [Google Scholar]
- Raudenbush SW, Bryk AS. Hierarchical linear models: Applications and data analysis methods. 2nd ed. Sage; Newbury Park, CA: 2002. [Google Scholar]
- Rimm-Kaufman S, Pianta R. An ecological perspective on the transition to kindergarten: A theoretical framework to guide empirical research. Journal of Applied Developmental Psychology. 2000;21:491–511. [Google Scholar]
- Rogosa D, Brant D, Zimowski M. A slow growth curve approach to the measurement of change. Psychological Bulletin. 1982;92:726–748. [Google Scholar]
- Rogosch FA, Cicchetti D, Toth SL. Expressed emotion in multiple subsystems of the families of toddlers with depressed mothers. Development and Psychopathology. 2004;16:689–709. doi: 10.1017/s0954579404004730. [DOI] [PubMed] [Google Scholar]
- Rothbart MK, Bates JE. Temperament. In: Damon W, Lerner R, Eisenberg N, editors. Handbook of child psychology: Vol. 3. Social, emotional, and personality development. 6th ed. Wiley; New York: 2006. pp. 99–166. [Google Scholar]
- Rutter M, Sroufe LA. Developmental psychopathology: Concepts and challenges. Development and Psychopathology. 2000;12:265–296. doi: 10.1017/s0954579400003023. [DOI] [PubMed] [Google Scholar]
- Rydell A, Berlin L, Bohlin G. Emotionality, emotion regulation, and adaptation among 5- to 8-year-old children. Emotion. 2003;3:30–47. doi: 10.1037/1528-3542.3.1.30. [DOI] [PubMed] [Google Scholar]
- Shields AM, Cicchetti D. Emotion regulation among school-age children: The development and validation of a new criterion Q-sort scale. Developmental Psychology. 1997;33:906–916. doi: 10.1037//0012-1649.33.6.906. [DOI] [PubMed] [Google Scholar]
- Shields AM, Cicchetti D. Narrative representations of children’s emotion dysregulation as predictors of maltreated children’s rejection by peers. Developmental Psychology. 2001;37:321–337. doi: 10.1037//0012-1649.37.3.321. [DOI] [PubMed] [Google Scholar]
- Shipman K, Schneider R, Brown A. Emotion dysregulation and psychopathology. In: Beauregard M, editor. Consciousness, emotional self-regulation and the brain. John Benjamins; Philadelphia: 2004. pp. 61–85. [Google Scholar]
- Silk JS, Shaw DS, Skuban EM, Oland AA, Kovacs M. Emotion regulation strategies in offspring of childhood-onset depressed mothers. Journal of Child Psychology & Psychiatry. 2006;47:69–78. doi: 10.1111/j.1469-7610.2005.01440.x. [DOI] [PubMed] [Google Scholar]
- Singer JD, Willett JB. Applied longitudinal data analysis: Modeling change and event occurrence. Oxford University Press; New York: 2003. [Google Scholar]
- Sroufe LA. Emotional development: The organization of emotional life in the early years. Cambridge University Press; New York: 1996. [Google Scholar]
- Stansbury K, Sigman M. Responses of preschoolers in two frustrating episodes: Emergence of complex strategies for emotion regulation. Journal of Genetic Psychology. 2000;161:182–202. doi: 10.1080/00221320009596705. [DOI] [PubMed] [Google Scholar]
- Stifter CA, Fox NA. Infant reactivity: Physiological correlates of newborn and 5-month temperament. Developmental Psychology. 1990;26:582–588. [Google Scholar]
- Suess PE, Porges SW, Plude DJ. Cardiac vagal tone and sustained attention in school-age children. Psychophysiology. 1994;31:17–22. doi: 10.1111/j.1469-8986.1994.tb01020.x. [DOI] [PubMed] [Google Scholar]
- Tarullo LB, Richardson DT, Radke-Yarrow M, Martinez PE. Multiple sources in child diagnosis: Parent-child concordance in affectively ill and well families. Journal of Clinical Child Psychology. 1995;24:173–183. [Google Scholar]
- Thompson RA, Meyer S. Socialization of emotion regulation in the family. In: Gross JJ, editor. Handbook of emotion regulation. Guilford Press; New York: 2007. pp. 249–268. [Google Scholar]
- Weissman MM, Wickramaratne P, Nomura Y, Warner V, Pilowsky D, Verdeli H. Offspring of depressed parents: 20 years later. American Journal of Psychiatry. 2006;163:1001–1008. doi: 10.1176/ajp.2006.163.6.1001. [DOI] [PubMed] [Google Scholar]
- Wilson B, Gottman J. Attention—The shuttle between emotion and cognition: Risk, resiliency, and physiological bases. In: Hetherington E, Blechman E, editors. Stress, coping and resiliency in children and families. Erlbaum; Mahwah, NJ: 1996. [Google Scholar]
- Winslow EB, Shaw DS, Bruns H, Kiebler K. Parenting as a mediator of child behavior problems and maternal stress, support, and adjustment; Paper presented at the biennial meeting of the Society for Research in Child Development; Indianapolis, IN. 1995.Mar, [Google Scholar]