

Abstract
Community integration research explores community contexts and factors that encourage or hinder individuals with serious mental illness (SMI) from actively participating in community life. This research agenda can be advanced by using mixed-methods that better document the relationships between contextual factors and individual experience. Two such methods were applied to a mixed-methods study of 40 adults with SMI living in independent housing in the Southeastern United States. Their contextualized experiences of community integration were measured by applying innovative participatory mapping and Geographic Information Systems (GIS) mapping techniques. Use of these methods in conjunction with one another facilitated the creation of activity spaces, which can measure geographic accessibility and help to represent an individual's experience of place and degree of mobility. The utility of these newly applied methods for better understanding community integration for persons with SMI is explored and implications for using these measures in research and practice are discussed.
Keywords: Psychiatric disabilities, Community integration, Geographic Information Systems, Participatory Mapping, Activity Space
All too often, individuals with serious mental illness experience isolation and lack opportunities to fulfill meaningful roles and activities in their communities. This is unfortunate because there is abundant evidence that participation in community life positively affects health (Antze, 1979; Barrera, 2000; Strauss & Carpenter, 1977). While most research on the experience of serious mental illness (SMI) has focused on individual's functioning, we argue that it is important to understand the role of place in participation in community life, particularly as it relates to health. The emerging body of community integration research has been devoted to studying the community contexts and factors that encourage or hinder individuals with serious mental illness from actively participating in community life (e.g., Aubry & Myner, 1996; Gulcer, Tsemberis, Stefancic, & Greenwood, 2007; Prince & Gerber, 2005; Wong & Solomon, 2002). This research agenda can be advanced by using methods that better document the relationships of contextual factors to individual experience. The overwhelming majority of community integration studies have used survey and self-report data to understand the experience of community life for persons with SMI. Further, few studies have directly assessed the impact of place on community integration, despite suggestions that it may be a critical component in the integration process (Carling, 1995; Yanos, 2007). The authors of this paper aim to contribute to the literature by presenting the methods and findings from a pair of innovative approaches to conceptualizing and measuring community integration. We argue that an expansion of the methods used for community integration research can better ground investigation in the physical and mental experience of place.
The paper begins with a brief overview of community integration research for persons with SMI, including an outline of key theoretical and empirical work in this area. We then discuss the need for expanding the methodological approaches used to investigate the physical and mental experience of place for individuals with serious mental illness. From our research aimed at better understanding these contextual factors, we outline the methods and advantages of participant created community maps and Geographic Information Systems (GIS). We then present findings from these specific methods and suggest how these can be used to progress community integration research.
Community integration of individuals with serious mental illness
Serious mental illness is a term used to classify persistent psychiatric conditions that can greatly affect a person's behavior, thinking, emotions, and relationships (Kloos, 2005). Diagnoses considered to be serious mental illnesses include schizophrenia, bipolar disorder, and severe and persistent depression. Traditionally, individuals with serious mental illness have received high levels of intervention, often in specialized settings dedicated to the treatment of these psychiatric problems. The prevailing model of such mental health care has been to take people out of community settings for care in institutional, residential treatment or hospital settings aimed at rehabilitating the patient and eventually readmitting her or him into the community (Nelson, Lord, & Ochocka, 2001).
The past thirty years have seen profound changes in care for people with SMI, and many of these shifts have focused on housing opportunities and support. Specifically, the current trend toward supported housing, marked by principles of consumer choice, holding a lease to community-based housing, and availability of flexible services, is becoming a preferred alternative to residential treatment facilities or long-term institutional treatment (Carling, 1993; Nelson, Lord, & Ochocka, 2001). A major distinguishing feature of the supported housing model is an emphasis on community integration, in which clients have opportunities to become citizens who are engaged in all facets of community life (Carling, 1995).
Community integration has traditionally been conceptualized as physical presence in the community (Cummins & Lau, 2003) and operationalized as the cumulative frequency of self-initiated participation in community activities and use of community resources (e.g., shopping, working, going to church, and visiting health centers) (Aubry & Myner, 1996). This conceptualization is useful because individuals with SMI are often isolated in their homes with few meaningful activities to fill their days (McCormick, Funderbunk, Lee, & Hale-Fought, 2005). Difficulties with isolation are compounded by the fact that over 85% of persons with SMI are unemployed, and studies have reported a lack of participation among many members of this population in educational and leisure activities (Bond, Salyers, Rollins, Rapp, and Zipple., 2004; Dewees, Pulice, & McCormick, 1996). This lack of engagement in meaningful activities can be a barrier to community integration, and it can also lead to isolation and negative mood states (McCormick et al., 2005).
More recently, researchers have noted that the concept of community integration should encompass more than simply being in the physical presence of the general public and participating in activities (Aubry & Myner, 1996; Cummins & Lau, 2003; Wong & Solomon, 2002). For instance, Aubry & Myner (1996) suggest that the conceptualization and measurement of the construct should be multi-dimensional and include physical, social, and psychological integration. They argue that physical integration is comprised of participation in activities of daily living in the broader community; social integration focuses on social contact with non-mentally ill neighbors and other community members; and psychological integration can be conceptualized as an individual's sense of community and belonging (Aubry & Myner, 1996; Wong & Solomon, 2002). Community integration appears to have an important relationship with positive mental health outcomes. Prince and Gerber (2005) found that both physical and psychological integration were positively related to subjective quality of life for persons with SMI, suggesting that both physical presence in the community and perceptions of sense of community and belonging can enhance life satisfaction. Aubry & Myner (1996) found social integration was positively related to quality of life for persons with SMI. Within this conceptual framework, community integration can include both tangible and intangible components, ranging from the number of activities performed to perceptions of belonging to the community (Gulcer et al., 2007).
Community integration experiences for persons with SMI are also likely affected by community tolerance for mental illness, not solely one's participation in activities located in community settings. Prince& Prince (2002) examined the relationship between perceived stigma and community integration in 95 clients of assertive community treatment (ACT) teams and found that clients’ perceptions of stigmatization were inversely related to their psychological integration. Thus, individuals who perceived greater amounts of community stigma experienced lower levels of sense of community and belonging. Similarly, Townley and Kloos (under review) found participants’ perceptions of neighborhood tolerance for mental illness to significantly predict their reports of feeling a sense of community in their neighborhoods. From a qualitative study of 80 individuals with a mental illness diagnosis and a history of homelessness, one-third of participants reported difficulties fitting in to their neighborhoods (Yanos, Barrow, & Tsemberis, 2004). Factors that reportedly impeded individuals’ ability to fit in included a lack of neighborhood safety and low neighborhood tolerance for “different” types of behaviors. However, community factors that can promote integration are not well understood. There is a need to expand empirical methods used to examine the intersections of personal experience and place that can affect health.
Community integration and the need to advance methods that investigate context
Community integration research has emerged as a high priority among a growing group of researchers studying serious mental illness. For example, Bond et al., 2004 refer to community integration as “a unifying concept providing direction and vision in community mental health for people with severe mental illness” (p.570). Similarly, Yanos (2007) instructs that “first and foremost, it is important that community integration be placed on the agenda of researchers who study the effects of place on people with mental illness” (p.673). The authors of this report agree with the importance placed upon this area of research but believe that a wider range of methods are needed to better conceptualize and measure the physical and mental experience of place as it relates to community integration.
Thus far, community integration research has largely been dominated by the use of survey data and other self-report indicators to determine individuals’ perceptions of their environments. Such methods can be quite useful; and, indeed, as the brief review above illustrates, they have helped to investigate both predictors and outcomes of community integration. However, there are limits to what survey data can demonstrate. Survey questions may not be sensitive to the experiences of all persons, and they may fail to capture specific aspects of integration that are better assessed by qualitative or observable measures. Indeed, it might be that a reliance on survey methods misses crucial components (both theoretical and measurable) of what community integration, and indeed community, mean for individuals with serious mental illness.
In the current study, we draw upon community psychology, geography, and community-based participatory research (CBPR) to apply two methods used to understand context in other disciplines to address perceived gaps in community integration research. Writing about the study of context within community psychology, Luke (2005) has advocated for using Geographic Information Systems for understanding persons’ experience in physical space. Building upon Luke, we have incorporated a participatory research component (e.g., Jason, Keys, Suarez-Balcazar, Taylor, & Davis, 2004; Israel et al., 2003;) to the use of mapping that allows us to consider the “meaning of place” for each person in analyses. That is, participants worked with interviewers to create maps of their communities, highlighting locations where they 1) spend time, 2) feel a sense of belonging, and 3) deem important. Second, activity spaces were created using Geographic Information Systems (GIS) technology. Each of these methods is briefly presented before we describe the current study.
Geographic Information Systems
A Geographic Information System (GIS) is a computer system used for cataloguing, storing, querying, analyzing, and displaying geospatial data (Chang, 2005). This system can be used to examine social environments and social processes at a community level, including mapping of community assets and resources, community health assessments, and community development (Linney, 2000; Luke, 2005; Pearce, Witten, & Bartie, 2006). Recently, GIS has been used to conceptualize and measure place identity and place attachment (Mason, 2007). Despite its potential, GIS remains largely underutilized in behavioral science research (e.g., psychology, psychiatry, social work). Its uses have been limited primarily to: 1) producing maps which display data and visually illustrate relationships, and 2) developing objective social indicator variables from census data which are then compared to self-report survey data (e.g., combining median household income, percent owner-occupancy, and percent of residents employed to create an index of neighborhood socioeconomic status). Although each of these practices is potentially useful, they tend to force arbitrary aggregation that may obscure the experience of geography and place for individual participants, thus overlooking the importance of person-environment transactions.
The underutilization of GIS in behavioral science research likely stems in part from its reputation as a purely quantitative tool (Kwan & Knigge, 2006). Researchers tend to utilize GIS software to conduct spatial analyses that rely on quantitative geographical information. However, this approach is a limited conceptualization of what the technology has to offer in terms of theory development and generation of new knowledge. Geographic Information Systems can also handle diverse types of information, such as photographs, narratives, and other types of ethnographic materials (Kwan & Knigge, 2006). In this way, we propose that GIS methods can be used in a manner more akin to mixed-methods approach to data analysis that incorporates quantitative and qualitative methodologies to investigate important contextual factors that would be missed by using single methods alone (e.g., Creswell & Plano-Clark, 2007). For this reason, researchers have suggested similarities between the visual capabilities of GIS and qualitative grounded theory. According to Knigge and Cope (2006), both tools can be used in an exploratory manner, involve iterative processes, are attentive to the particular and the general, and can accommodate multiple views of the world.
GIS has also been underutilized due to perceptions that it is too difficult and expensive to be used by people without expertise in the method. While this may have been a reality in the mid-1990s, the work of Helen Couclelis, John Pickles, and, more recently, Sarah Elwood has helped to alter the “technological, political, and intellectual practice of GIS” (Elwood, 2006, p 693). Participatory GIS has emerged from this movement, and it encourages individuals and social groups to participate equally in spatial analyses, knowledge production, and communication of data. GIS technology has also become more user-friendly and capable of capturing and displaying the unique meaning of place for individuals and groups.
Participatory Mapping
In the last decade, a renewed interest in research methods that involve the “research subject” in the creation of the knowledge has become prominent in several fields (Grant, Nelson, & Mitchell, 2008; Rappaport, 1990) and even some NIH program announcements, though not in community integration research. In its current form, community-based participatory research (CBPR) involves research participants in defining questions of interest, data collection, and interpretation of findings (Israel et al., 2003; Jason et al., 2004). CBPR methods have had broad appeal in community psychology, public health, and other health-focused research. The ethos of this approach to research is to find ways for research participants to be meaningfully involved in the research process and have a voice in the knowledge that is created. Proponents of these methods assume that the knowledge derived from CBPR informed studies will be more representative, have access to data not available with standard methods, and be useful in addressing health concerns of research participants (Israel et al., 2003; Jason et al., 2004)
In geography, this trend toward more inclusive methods of defining mental and physical boundaries of space has led to an increased emphasis among social geographers and other researchers on involving local communities and individuals in a process called participatory mapping (Aberley, 1993; Parker, 2006). This method asks participants to identify the physical boundaries of their own neighborhoods and communities, as well as important resources in their communities (Green & Kloos, 2008). Some of the earliest work in this area was conducted by Kevin Lynch, an urban planner who was interested in how people organize spatial information about their environments. He asked respondents in three different cities to draw sketch maps showing significant features of their cities and discuss the importance of the inclusion of these elements on the maps (Lynch, 1960).
Having people draw their own maps, as opposed to relying on pre-drawn maps or census boundaries, allows the researcher to understand what types of resources and activities are most important to individuals’ daily functioning and well-being. Accordingly, this method can be useful in challenging assumptions and testing theories of what people appreciate in their community and what they contribute to them. Additionally, when individuals are able to define their communities based on their own unique experiences and expertise, their perceptions of belonging to the community, as well as their intrinsic motivation to actively engage in community life, are increased (Parker, 2006).
Activity Spaces
The construct of “activity spaces” is one approach to research which is particularly well-suited for our interest in integrating GIS technology and participatory mapping methods. Activity spaces have been defined in various ways, including “the local areas within which people move or travel in the course of their daily activities” (Gesler & Albert, 2000) and “the spatial movement component of an individual's day-to-day lived experience” (Golledge & Stimson, 1987, pg. 345). Activity spaces can measure geographic accessibility and help to represent an individual's experience of place (Nemet & Bailey, 2000) and degree of mobility (Gesler & Meade, 1988). They have been used as an analytic technique by researchers working in various areas, including travel and transportation, city planning, crime mapping, and medical geography (e.g., Harries, 1999; Sherman, Spencer, Preisser, Gesler, &Arcury, 2005).
A research focus on participant-defined activity spaces may help to measure and represent the unique experience of place for individuals with serious mental illness. This methodology may also serve a role in advancing the community integration research literature,, as the remainder of this paper will help to illustrate. Broadly, this study evaluates the participatory mapping and activity space methods to determine their utility in understanding the experience of community integration for individuals with serious mental illness. Three research questions guide the inquiry. First, we aim to document the activity settings in which respondents participate. Second, we aim to examine participants’ assessments of meaning by activity settings. Third, we aim to investigate the relationships between community integration (as measured by activity space size) and adaptive outcomes (see Figure 1)
Figure 1.
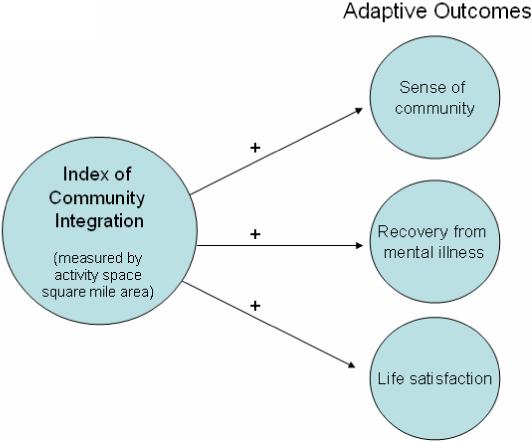
Model of suggested relationships between the index of community integration and adaptive outcomes
Overview of Study
This study draws upon participatory inquiry and GIS methods to understand better the experience of place and community living for persons with SMI living in their own apartments. There has been a growing literature on experiences of persons with SMI who have supported housing (e.g., Newman, 2001; Rog, 2004, Wong & Solomon, 2002). By recruiting participants from a range of housing programs, we want to test the utility and capacity of these new methods to understand participants’ experiences in community living. In the terminology of mixed-methods research (Cresswell & Plano-Clark, 2007), we use a Qual-Quant research design that first collects qualitative data about research participants’ experiences that are then combined with quantitative data and analyzed primarily in quantitative terms. The combination of new methods within a mixed-methods framework is critical to this approach to study the intersection of contextual and experiential factors of community living.
Method
Participants
The participants in this study were 40 residents of two counties in South Carolina who utilized mental health services from the South Carolina Department of Mental Health (SCDMH). Of the 40 participants, 21 lived in supported housing and 19 lived in non-supported housing at the time of the interview. The 21 participants in supported housing were randomly selected from a larger study of 533 individuals who receive a housing subsidy (e.g., HUD-support or Section 8) and living in South Carolina (Kloos, Townley, & Green, 2008; Wright & Kloos, 2007). The first 21 persons from the randomly generated list were then recruited via telephone call or personal invitation; their acceptance rate was 100%. The participants in non-supported housing were recruited at day program facilities and a local mental health clubhouse. Requirements for participation for this non-supported part of the sample were that individuals were currently utilizing mental health services, were living independently (i.e., not with a guardian or in housing with on-site staff support), and were not receiving a housing subsidy. For this second half of the sample, 19 of the 28 persons living independently without supported housing who were invited agreed to participate.
The 40 participants were nearly evenly divided by sex, with 55% of the sample being female. The racial composition of the sample was as follows: 18 (45%) participants were African American, 21 (52.5%) participants were White, and 1 (2.5%) reported being bi-racial. Participants ranged in age from 32 to 77, with the average age being 46. Only two participants in the sample were married, nine owned cars (a distinction relevant for activity spaces), and nine participants were working or attending school full-time. The predominant diagnosis (> 50%) for this sample was a thought disorder (e.g., schizophrenia), with the remaining participants having such diagnoses as major depression and bipolar disorder. There were no significant differences in type of mental illness diagnosis between those participants living in supported housing sites and those living in non-supported housing sites.
Study Design
Study participants were interviewed at three separate time intervals. At the first interview, participants were asked questions about their experiences in housing and neighborhood environments and the activities in which they participated. Participants also drew maps of their communities, including their homes and locations where they spend time (please see next section for more details on this method). At the second interview, follow-up questions were asked based on information that needed clarification from the first interview. Participants also took interviewers on a “walk-about” whereby they conducted a guided tour of their neighborhoods and provided descriptions of important locations in the neighborhoods. This allowed us to understand participants’ neighborhood experiences from their own perspectives rather than assuming what their experiences may be. Finally, at the third interview, participants responded to a brief quantitative survey about their perceptions of neighborhood factors, life satisfaction, and recovery from mental illness.
Procedure
Creating community maps with participants
After talking about their housing and experiences in their neighborhood and broader community, participants were presented with a sheet of paper and asked, “Please use this sheet of paper to draw the places that are important to you.” Participants were allowed to draw the physical map in any manner that they wanted to. After participants completed their maps, they were asked to narrate the personal meanings of the places, as well as the social and physical aspects of the map. Probes included the following:
“Which of these places are most important to you?”
“Where do you spend the most time?”
“Where do you feel you belong the most?”
“Who do you spend time with at particular places on the map?”
“How do you get to particular places on the map?”
“What do you do at particular places on the map?”
After the interview session, each interviewer used the drawn map and information from the interview transcript to locate each place and plot it on a printed map from a South Carolina atlas.
Geocoding map locations
In order for the participant maps to be used in the Geographic Information Systems (GIS) interface, the addresses had to be geocoded. Geocoding is the process of converting addresses to longitude and latitude coordinates. Addresses were obtained for each location on participants’ maps using Google Maps and information from the interview transcripts. After all addresses were located, they were geocoded using the geocoding service at www.batchgeocode.com. This is a free service that is unique because it provides a coordinate lookup in bulk and maps many addresses at once, rather than one at a time. Finally, the longitude and latitude points for each participants’ map locations were entered onto a digital map of Richland and Lexington counties using ESRI ArcMap 9.2
Creating activity spaces
Activity spaces were created in GIS using the standard deviational ellipse (SDE) method. The SDE is a bivariate statistical measure that provides a comparable estimate of an individual's activity space (Sherman et al., 2005). Using the designated points that were plotted for each participant, the SDE method calculates the standard deviation of the distances of the x coordinates and y coordinates of each individual point from the mean center of all points to define the major and minor axis of the ellipse. The user can specify the number of standard deviations to represent. The SDE at one standard deviation will contain 68% of the points within the boundary of the ellipse, the SDE at two standard deviations will contain 95% of the points, and the SDE at three standard deviations will contain 99% of the points. After examining the types of activities and the conditions under which they were undertaken (e.g., monthly trip of social club; weekly visit to church, daily trip to store), one standard deviation was used, as this would most closely represent the daily experiences of the majority of participants. That is, it is unlikely that the participants traveled to each of the locations identified on their maps every day. If we had asked them to include only locations that they travel to each day, we would have greater confidence using a three-standard deviation ellipse to represent their common experience. However, we used one standard deviation to capture 68% of their points to account for the likelihood that participants only travel regularly to some—not all—of their activity locations. Additionally, most of our participants traveled by foot or by public transportation, so this also reduces the likelihood that they traveled to all of their map locations on a daily basis. A final justification for creating ellipses using one standard deviation is that doing so has been shown to have higher statistical power to predict well-being outcomes than using two or three standard deviations (Sherman et al., 2005).
Once created, the ellipses created a general distribution of points in each participant's activity space. Although a potential limitation of this method is that it is an abstract representation of where people actually go (i.e., it does not provide a direct route from point A to point B), we propose that the activity space ellipses can be used as an indicator of individual access or opportunity of movement throughout a community. Using tools in GIS, it is also possible to calculate the area of each activity spaces. We propose that this area, measured in square miles, can be interpreted as a quantifiable index of community integration. That is, the square mile area represents the geographical spread of community activities in which the individual reports engaging. The importance of quantifying this figure is that it can then be compared to self-report survey data to uncover potentially interesting relationships between psychosocial variables and the square mile area of the activity space ellipse.
Measures
Sense of Community
Participants’ sense of community was measured with the Brief Sense of Community Inventory (BSCI), developed by Long and Perkins (2003). The BSCI is an eight-item scale adapted in part from the original 12-item Sense of Community Index (Perkins et al., 1990). The BSCI was found to have enhanced psychometric properties from the original scale, and it consists of three subscales: (a) social connections, (b) mutual concern, and (c) community values. Participants were asked to think about their neighborhood when responding, and items were on a Likert scale where 1= “Strongly Disagree” and 5 = “Strongly Agree.” The internal consistency for the scale was 0.78.
Life Satisfaction
Participants’ general satisfaction with their lives was assessed using a single question from the Quality of Life survey (Lehman, 1995): “How do you feel about your life overall right now?” Scores ranged from 1 = ‘Terrible” to 7 = “Delighted.”
Recovery
Participants’ attitudes regarding their recovery from mental illness were assessed using the Recovery Assessment Scale – Short Version (RAS-sf) (Corrigan, Salzer, Ralph, & Keck, 2004). The RAS-sf is comprised of 20 items that represent the following five factors: a) personal confidence and hope, b) willingness to ask for help, c) goal and success orientation, d) reliance on others, and e) not dominated by symptoms. Responses were given on a 5-point Likert Scale where 1= “Strongly Disagree” and 5= “Strongly Agree.” The internal consistency for the scale in this sample was 0.90.
Neighborhood Social Climate (HES-NSC)
This scale consists of 10 questions assessing perceptions of belonging and acceptance in the neighborhood (Kloos, et. al., in preparation; Wright & Kloos, 2007). Items were on a 5-point Likert Scale, where 1 = “Strongly Disagree” and 5 = “Strongly Agree.” The Cronbach alpha for the scale in the dataset was 0.82 and the test-retest correlation was 0.67.
Results
Participant maps
Each participant was able to create a graphic representation of their neighborhood and community locations that were personally important. Although most participants expressed some confusion and apprehension at the beginning of the mapping exercise, the majority reported that they enjoyed the task and its discussion. Several described the experience as empowering to be able to explain their communities from their own unique perspectives. For example, one European American male participant said at the beginning of the map task, “There's no telling how this is going to turn out. I really can't draw.” At the end of the task, he said, “That was fun. It was cool telling you all the places that I go during the day. I've never thought about it like that.” Most participants (n = 26) drew more traditional maps with labeled roads, accurately placed and scaled locations, and accurate geographic orientation (see Figure 2). The remainder (n = 14) placed more emphasis on drawing detailed structures that they travel to in their communities but did not rely on geographic accuracy (see Figure 3). For the current study, the authors did not analyze differences in the cognitive representation of place. Here, analyses focus on understanding the number, types, and importance of activity locations that participants reported in their maps. These data, along with the participants’ explanations of the locations, were used to create the activity spaces in GIS.
Figure 2.
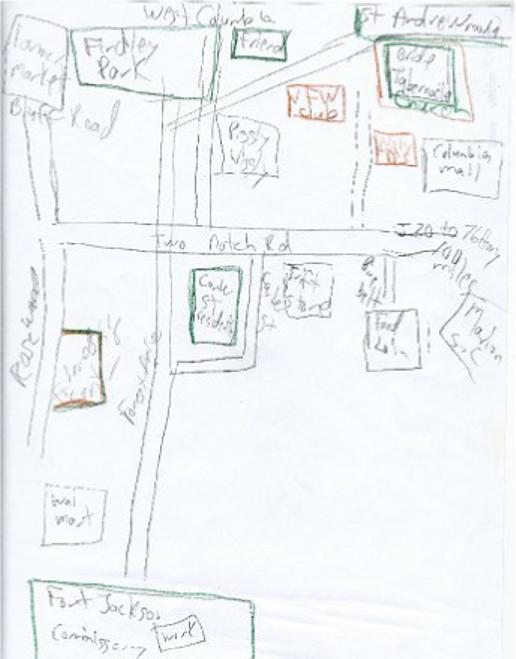
Illustration of a map in which participants adhered to more traditional conventions of map-making, including labeled roads, accurately placed and scaled locations, and accurate geographic orientation
Figure 3.
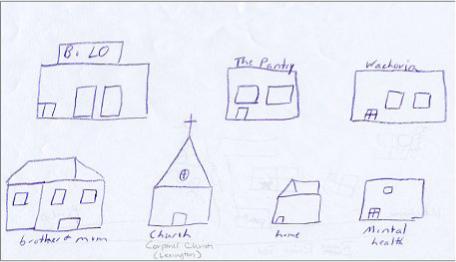
Illustration of a map in which participants placed more emphasis on drawing detailed structures that they travel to in their communities but did not rely on geographic accuracy
Documenting the activity settings in which respondents participate
The average number of activity locations that participants reported on their maps was 7.44 (range = 4 to 14, SD = 2.83). There were no significant differences between numbers of activities reported by participants living in supported housing and participants living in non-supported housing; thus, the results are reported with the groups combined rather than separated. The following five clusters represent the types of activity locations most frequently reported by participants: 1) Home (i.e., participants’ own homes); 2) Social/ leisure (e.g., churches, homes of friends/ family, movie theaters, parks, YMCA), 3) Activities of daily living (e.g., shopping centers, restaurants, grocery stores), 4) Work/ volunteer/ educational (e.g., locations where participants work, volunteer, or are enrolled in educational classes), and 5) Physical/ Mental health-related (e.g., mental health centers, mental health clubhouses, hospitals). Please see Table 1 for the number of participants who reported activities in each of the activity location clusters. Further analyses of thematic content are presented below.
Table 1.
Number of participants who reported activities in each of the activity location clusters
| Map activity location cluster | Number and percent of participants reporting cluster |
|---|---|
| Residential | 40 (100%) |
| Leisure/ social | 26 (65%) |
| Activities of daily living | 37 (93%) |
| Work/ volunteer/ education | 9 (23%) |
| Health-related | 30 (75%) |
GIS Activity Spaces
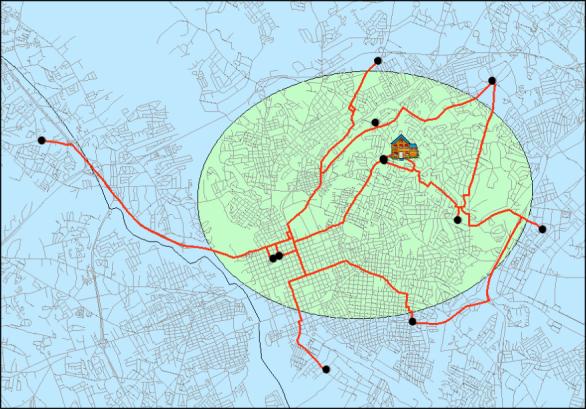
The activity space areas ranged from 0.06 to 37.40 square miles. The mean area for participants’ activity spaces was 9.27 square miles (SD= 9.49). There were no significant differences between activity space areas for participants living in supported housing and participants living in non-supported housing. Interestingly, there were also no significant differences between activity spaces areas for participants who owned cars and those who did not own cars. For purposes of illustrating variation in activity space ellipses, please see Figure 4 for an example of several participants’ activity spaces created using GIS.
Figure 4.
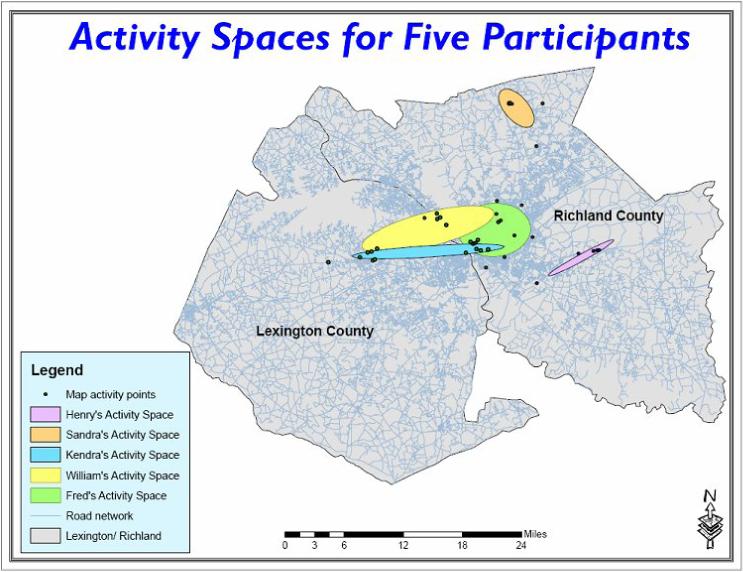
Map of Richland and Lexington counties displaying five activity space ellipses. The points on the map represent the participants’ various activity locations. The activity spaces were created using the standard deviational ellipse method to capture 68% of the activity locations.
Relationships between activity space area and adaptive outcomes
Pearson correlations were conducted between activity space area and self-report indices of adaptive outcomes (results are displayed in Table 2). First, there was a significant positive correlation between the activity space area and general life satisfaction (r = 0.51, p < 0.01). Individuals with larger activity spaces (i.e., those who engaged in more activities farther from home) reported feeling more satisfied with their lives than those participants with smaller activity spaces (i.e., those who engaged in more activities closer to home). Secondly, there was a significant negative correlation between the activity space area and neighborhood sense of community (r = −0.40, p < 0.05). That is, participants who had smaller activity spaces experienced a stronger sense of community than those participants who had larger activity spaces. This finding was contrary to expectation. Finally, there was a positive trend observed between the activity space area and participants’ attitudes toward recovery from mental illness (r = 0.22, p < 0.10). Participants with larger activity spaces had a trend for more positive attitudes toward their own recovery from mental illness. However, this relationship needs further examination and should only be interpreted as a trend relationship.
Table 2.
Correlation matrix of relationships between activity space area and self-report indices of well-being and community integration (N = 40)
| Variable | 1 | 2 | 3 | 4 | 5 |
|---|---|---|---|---|---|
| 1. Activity space area | -- | ||||
| 2. Life satisfaction | 0.51*** | -- | |||
| 3. Recovery | 0.22* | 0.46*** | -- | ||
| 4. Sense of community | −0.40** | 0.14 | 0.28* | -- | |
| 5. Neighborhood social climate | −0.10 | 0.20 | 0.46*** | 0.64*** | -- |
p < 0.10
p < 0.05
p < 0.01
Participant assessments of meaning by activity settings
In order to contextualize the experience of place further as it related to community integration for the current sample, we supplemented quantitative analyses of activity spaces with thematic analyses of qualitative interview data. In particular, we were interested in whether research participants would make distinctions between the meaning of activities by location. Participants were asked to report which activity locations they (a) spent the most time at, (b) considered being the most important, and (c) felt they belonged the most. Not surprisingly, home emerged as the area that participants spent the most time (n=29, 72%), considered to be most important (n=18, 45%), and felt the strongest sense of belonging (n=22, 55%). For example, a 43-year-old European American female said, “Here at the apartment. That's where I feel my best. I can decorate it, put my groceries in it, and I know it's mine.” Physical/ mental health-related facilities also emerged as areas where a subset of participants spend a lot of time (n=8, 20%), consider most important (n=6, 15%), and belong the most (n=5, 13%). As a 34-year-old African American male related, “The clubhouse is most important to me because the people and the staff, they have the background and everything to help me to cope and deal with my mental illness. Everybody there understands me and knows what I come there for.”
Some participants listed activities of daily living (e.g., grocery stores and shopping centers) (n = 10, 25%), social/ leisure, (n = 4, 10%), and work/ volunteer/ educational facilities (n = 2, 5%) as their most important activity locations. As one 38-year-old African American female said, “I love going to church. It's somewhere to go instead of just being around the house. I love going ‘cause I want to hear what the preacher has to say, what his sermon is going to be.” Activities of daily living (n = 7, 17%) and social/ leisure locations (n = 6, 15%) also emerged as areas where individuals feel a strong sense of belonging. For example, a 51-year-old European American male said, “I've met a lot of people at the YMCA and you know you can always stop and talk to them, and everybody knows you, and it's good to be able for me to just see regular people. I mean, I don't know if that makes any sense to you, but it's good for me to feel a part of something.” Finally, a minority of participants reported that work/ volunteer/ educational facilities are where they spend the most time (n = 3, 8%). A 42-year-old African American male related, “I spend most of the time on the job or working in the garden. I don't like sitting around my apartment much. I like staying active, feeling like I'm getting things done.”
Comparing locations of most important, most time spent, and sense of belonging assessments
As part of the integration of qualitative and activity space data, the patterns of convergence or divergence of the three location assessments were investigated. A total of 23 (58%) participants reported convergence in their activity location assessments. That is, the place where they spent the most time, they considered to be most important, and where they felt a sense of belonging was the same. For the majority of these participants (n = 18, 78%), the home was the location which satisfied each of these three conditions. Two participants assigned this distinction to mental health clubhouses, while work, church, and a local bar were each listed by one participant as filling all three conditions.
A total of 17 participants (42%) reported divergence in their activity locations assessments. That is, the place where they spend the most time, consider to be most important, and feel a sense of belonging was not the same. For example, Sandra, an African American female, said that her home is her most important activity location and the location where she spends the most time; however, she reported that she achieves the greatest sense of belonging when she is at church. Participants who did not have convergence of the three location assessments had larger activity spaces (area = 11.92 square miles) than participants for whom there was a match across all three assessments (area = 7.62), although the difference was not statistically significant in this small sample, F (1, 39) = 1.95, p > 0.05. Additionally, there were not significant differences in sense of community [F (1, 39) = 0.164, p > 0.05], life satisfaction [F (1, 39) = 0.652, p > 0.05], or recovery orientation [F (1, 39) = 0.332, p > 0.05] between participants who reported a match across all three assessments and those who reported a mismatch.
Discussion
The introduction of methodological advances from community-based research and social sciences has the potential to advance the science of community integration research. We have presented examples of two methods that appear to be particularly promising. Participatory methods and geo-spatial analyses offer new ways of investigating the meaning of place and experience in community settings for individuals with serious mental illness. This work can link to past research focused on neighborhood characteristics, mental illness, and geo-spatial influences of place. For instance, Dear and Wolch (1987) documented the tendency for ex-patients to gravitate toward specific zones within urban North American settings, thus forming “service-dependent ghettos.” Similarly, research concerning the “breeder-drift” hypothesis (see for example Verheij, 1996) suggests that urban environments attract selective migration of individuals with mental illness (drift) or exacerbate symptoms due to stress-exposure or prompting of unhealthy behaviors (breeder).
By embedding this research within a GIS framework, it provides a structure for what might otherwise be quite diffuse qualitative responses. We argue that incorporation of these methods into community integration research can facilitate different conceptualizations of community integration and participation, as illustrated by the results of these analyses. That is, the findings can make contributions to theory and propose a research agenda that better understand the richness of community experiences for persons with serious mental illness than a reliance on survey methods. While these analyses are the first efforts to draw conclusions using these methods in community integration research, there appears to be potential to warrant continued methodological development and empirical research.
The results of this study revealed that most participants considered home to be the most important activity location, as well as the place where they spend the most time and belong the most. Although this information is somewhat discouraging, as it reinforces perceptions that many people with serious mental illness remain isolated in their homes, it clarifies the shortcomings of methods that simply count the number and type of activities in which people engage. In this case, the experience of home was the most central and salient to research participants’ experiences of community. We suggest this finding emphasizes the value of methods that investigate the meaning of place in understanding community integration. However, the primacy of residential patterns was not uniform across the sample. A considerable percentage of participants also reported that social/ leisure activities (e.g., churches, movies, YMCAs, etc.) and activities of daily living (e.g., grocery stores, shopping centers, and restaurants) were locations where they spend the most time, deem most important, and obtain a sense of belonging. Future investigation may do well to concentrate on the meaning of these places in the lives of these research participants and understanding the facilitating factors that contribute to patterns of activity more extensively rooted in non-residential community settings. Facilitating factors may include access to transportation or locations being within walking distance, perceptions of community acceptance, and opportunities for activity provided by mental health centers.
The second set of findings focus on the utility of geo-spatial methods in community integration research. The construct of an activity space, as measured in square-mile area, was found to be significantly related to higher life satisfaction and lower neighborhood sense of community for research participants. The first relationship (i.e., persons whose plotted activities constitute a larger area reported more positive subjective assessment of their current life situation) makes intuitive sense and supports similar findings in other community integration research (e.g., Aubry & Myner, 1996; Prince & Gerber, 2005). Participating in activities in the community may provide individuals with a sense of meaning and purpose, and it likely offers them opportunities to interact with others and obtain positive social support.
The second finding (i.e., persons whose plotted activities constitute a larger area reported lower sense of community in their neighborhoods) requires more thoughtful interpretation. Sense of community is traditionally thought of as a positive, supportive component of community life. It has been linked to increased psychological well-being (Pretty, Conroy, Dugay, Fowler, & Williams, 1996; Prezza, Amici, Roberti, & Tedeschi, 2001), perceptions of belonging and community connectedness (Sonn & Fisher, 1996), and participation in the community (Chavis & Wandersman, 1990). This construct may be particularly important for individuals with mental illnesses given challenges with isolation and societal stigma (Segal, Aviram, & Silverman, 1989; Townley & Kloos, under review). The results of this study suggest that individuals who have smaller activity spaces experience a stronger sense of community in their neighborhoods. This makes intuitive sense, as individuals who remain closer to home likely have more opportunities to interact with their neighbors and become familiar with their neighborhoods. However, it also suggests that as individuals with mental illness move beyond the proximal “zones” of their residences and daily living sites, they may feel disconnected. They may also fear that stigma will become more intense as they interact with people who are not familiar with them. This finding points to the need to uncover mechanisms through which individuals can feel supported by community members. Vanessa Pinfold's work on mental health networks in community settings (e.g., 2000) suggests the importance of creating ‘safe havens’ in which individuals feel supported by other community members. She also argues for the value of participation in activities that occur in both mainstream community settings as well as more traditional mental health settings (e.g., attending a day program). It may be that individuals will initially feel a stronger, more secure connection to individuals in mental health settings; but as they progress in their recovery process, they can begin to participate and feel supported in more mainstream settings within the broader community.
Importance of new methods for community integration research
This study was designed to expand the empirical inquiry in community integration research for individuals with serious mental illnesses. The methods contribute to this research literature in two important ways. First, participatory mapping allows participants to illustrate and discuss areas in their communities where they spend time, obtain a sense of belonging, and to discuss which activities they consider to be important. When compared to traditional survey methods, an interactive, participatory approach can better capture the richness of persons’ experiences (Tebes, 2005). This is particularly important in community-based research that needs to understand individual's experiences better to expand its empirical and theoretical foundations (Kloos, 2005b). It is interesting to note that all the persons in the study sample were able to reflect on their activities and report opportunities for activities in community settings. This method appears to offer a way to gather information about community experience that may be more “accessible” to persons who are not accustomed to translating their experience into scale scores. Second, the GIS activity spaces allow for the geospatial representation of these activities, as well as the square-mile quantification of the spread of activities. While the activity space area is an abstraction of experience not easily recognizable to research participants, it creates an index of person-environment interactions. Furthermore, combining the qualitative data with GIS technologies allows researchers to harness the richness of qualitative responses while simultaneously plotting their participation in community settings. It allows for comparisons across individuals and across time. When these methods are thoughtfully combined, we suggest that they provide a richer understanding of persons’ experience of place and participation in community settings. These new understandings can advance the science of community integration research.
Although many features of community life certainly operate similarly among mentally ill and non-mentally ill persons, certain components are likely quite unique (Carling, 1995; Kloos 2005a). By asking individuals to draw maps featuring locations in the community that are important to them and which provide a sense of belonging, we can better understand their perceptions of what is around them and what is available to them. This may help highlight gaps in service availability and service utilization. It may also document unanticipated alternatives that some individuals use to meet their various community integration needs.
The participant maps and activity spaces can further help to illustrate perceptions of community membership and identity. If individuals only include locations on their maps that are mental health-related facilities (e.g., psychosocial clubhouses, mental health centers, etc.), or if they say that they go to activities primarily with staff or fellow mental health consumers, then we may hypothesize that their identification with the consumer community is more salient (Wong & Solomon, 2002). In contrast, if an individual includes primarily routine activities in the broader community rather than mental health-related activities, we may hypothesize that they identify more with the general population than the consumer community. This distinction is important because it may point to differences in the types of support that individual need in order to effectively engage with the broader community. Some individuals may feel competent to join a church, apply for a job, or attend a college course independently. However, others may need to do so via support from mental health staff and fellow consumers. This information can help understand how involvement with mental health services helps or hinders community integration processes.
Central to the effectiveness of these methods is a greater reliance on participatory approaches to research. Participatory research aims to empower people and facilitate social, organizational, and political change by engaging participants in the research process and allowing them to have a certain level of control (Balcazar et al., 2004). Gulcer et al. (2007) suggest that we move toward participatory qualitative research designs in which consumer input dictates the ways in which we define and measure community integration. In order to successfully produce the maps and activity spaces, the researcher must work in collaboration with the research participant to identify and define locations in the community that are important to them. Rather than being given pre-designed surveys, participants are asked to draw maps of their communities and allowed the freedom to define the various components of these communities as they see fit. This ensures that rather than testing what we think community integration should be, the participant is allowed to tell us what community integration and community is for them. Creating maps can also provide individuals with an empowering sense of competency and authority. They are the experts of their own experiences in the community, and we want to understand and measure these experiences accurately and appropriately.
Implications of this work for policy and practice
The activity space methodology discussed here has numerous potential clinical and policy applications. First, it can be used as a heuristic by case managers and other service providers when preparing treatment plans with clients. If one of the treatment goals decided upon by the client and therapist is to engage in more community activities, the activity space framework can be used to track client progress. Each time a client begins a new activity (or ends an old one), it can be added to (or removed from) the activity space, and the change in area can be calculated and interpreted as a sort of reliable change index.
Activity space research may also be able to impact mental health policy around important factors related to community integration, such as transportation and housing location. For example, if individuals who live in urban settings are shown to consistently have larger activity spaces than individuals who live in rural settings, this could speak to the importance of improving transportation access to individuals in rural settings or building more supported housing sites in urban settings. Community integration is hindered when individuals are not able to walk to services or access public transportation (Yanos, 2007). It is vital for research to provide a bridge to mental health policy, and we suggest that our work provides a systematic way to do this.
Shortcomings and limitations
The small sample is a limitation of this study that must be recognized Although, the sample size was large enough to uncover relationships between activity space area and two of the adaptive outcomes, we had insufficient power to detect a significant association between activity space area and the recovery measure. A future study should collect data from a larger number of individuals to increase both variability of results and also likelihood of detecting relationships that likely exist in the real world.
There are also several limitations to the methodology used in this study. When creating the activity spaces from participant maps, it may not always be possible to get exact locations for each activity. In this study, a total of nine addresses could not be located. In these cases, the participants either did not know the exact address or it could not be determined from the information they provided. This problem may be unavoidable when conducting this type of research. One alternative is to geocode a centroid point in the city or county to represent the addresses that could not be located, as was used in this study.
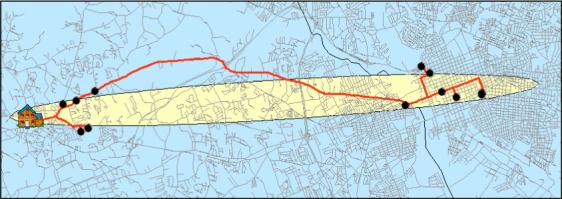
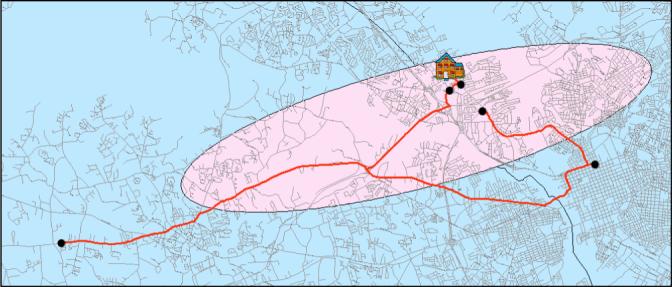
Second, there needs to be refinement of how activity spaces are measured and conceptualized. As already discussed, the activity spaces are created in GIS based on the distance of points from the mean center of points. In cases in which activity locations are evenly distributed throughout an area, this method represents an unbiased approach (see Figure 5). However, this method may underestimate the amount of “community integration” represented by an activity space area if locations of activities are clustered near each other (see Figure 6). Alternatively, this method could overestimate community integration associated with activity spaces that are inflated by a relatively infrequent activity completed a great distance from their home (see Figure 7). The following scenarios illustrate potential problems: Kendra travels to 11 locations regularly to perform activities in the community. The activity locations are clustered in two sections of the city (refer to Figure 6). In contrast, William travels to five locations regularly to perform activities in the community. Four of the locations are within walking distance, but one is located 20 miles from his home (refer to Figure 7). Clearly, Kendra performs more activities in the community than William; yet, her activity space would actually be smaller in area than William's because her activities are clustered in two sections of the city and are closer to her home, whereas he performs one activity that is far from his home. Potential method modifications could focus on weighting the activity spaces by (a) the number of activities that each participant performs, (b) their frequency, or (c) subjective meaning. These modifications would likley reduce potential bias by having the activity space size be impacted both by the distance of points from the participants’ homes, and how they engage in activities. Adding a third dimension to activity spaces can allow for integration of patterns of activity or subjective meaning along with spatial relations. We do not suggest “deleting” outliers (i.e., activities far from home) even if they do bias the activity space size because they help to reflect the lived community experience of participants.
Figure 5.
Example of an activity space in which activity locations are evenly distributed around the city.
Figure 6.
Example of an activity space in which activity locations are clustered in two sections of the city.
Figure 7.
Example of an activity space that includes one activity location located a far distance from the individual's home.
Finally, activity space methods should not be viewed as easily interpretable indices of community integration across study location. It is important to point out that although the methods of participatory mapping and activity space methods presented in the study are relevant across many research settings, the representation of particular activity spaces in terms of community integration is likely context bound and probably to unique samples. Our sample came from a mid-size city in the Southeastern United States. It is likely that results would look considerably different—and would have different implications—for a sample in a large metropolitan setting or a rural setting with their setting-specific transportation, services, and recreation resources. We observe, however, that this challenge common to community integration research as a field (Yanos, 2007).
Conclusions and suggestions for future research
Capturing transactional aspects of experience in settings has been problematic for community integration research methodology. While transactional-ecological theories have been useful in conceptualizing human problems and approaches to research (Altman & Rogoff, 1987; Felner, Felner, & Silverman, 2000), measurement of these phenomena has been relatively underdeveloped. The activity space methodology creates an index for an individual that provides a snapshot of their interactions for a given period of time in geographic space. While this method is reductionistic in terms of representing an individual's experience (as is all data analysis), it facilitates comparisons of transactional experiences which has been difficult methodologically. By plotting experiences in space, activity space research allows for more description of the “context” of a persons’ experience than survey methods we have relied upon previously. That is, there is more information that could be helpful to plan interventions for the particular individual. It may also facilitate looking for patterns in people's types of experiences, types of resources, or barriers that are associated with particular measures.
Above all else, the participatory mapping and activity space methods are important because they allow for new and innovative ways to measure indices of community integration of individuals with mental illness. As already discussed, community integration is typically measured by a variety of surveys. The activity spaces, created from the participant maps, allow for a quantifiable, observable indicator of community integration. The participant maps and activity spaces in and of themselves primarily represent physical aspects of community integration (i.e., physical presence in the community and participation in activities). However, they can be combined with survey data and qualitative interviewing to better understand social and psychological aspects of integration at the various activity locations. For example, individuals may be asked questions regarding what types of individuals they interact with at various locations in the community and whether or not they feel a sense of belonging at these locations. These two methods represent only two possible avenues for advancing community integration research. Continued development of the field will refine and add other methods that better incorporate the study of contextual factors in community integration.
Table 3.
Rank order of participants’ qualitative assessments of meaning by activity location clusters
| Map activity location cluster | Spent Most Time | Most important | Belonged most |
|---|---|---|---|
| Residential | 1 (72%) | 1 (45%) | 1 (55%) |
| Social/ leisure | 4/5 0% | 4 (10%) | 3 (15%) |
| Activities of daily living | 4/5 0% | 2 (25%) | 2 (17%) |
| Work/ volunteer/ education | 3 (8%) | 5 (5%) | 5 0% |
| Health-related | 2 (20%) | 3 (15%) | 4 (13%) |
Acknowledgments
Preparation of this manuscript was supported by funding from the National Institute of Mental Health—K23-MH65439. Thanks to staff and consumers of the South Carolina Department of Mental Health, who made this research possible, and to David Cowen, Lynn Shirley, and Kevin Remington, Geography Department, University of South Carolina
References
- Aberley D. Boundaries of home: Mapping for local empowerment. New Society; Gabriola Island, B.C.: 1993. [Google Scholar]
- Antze P. The role of ideologies in peer psychotherapy organizations: Some theoretical considerations and three case studies. Journal of Applied Behavioral Science. 1976;12:323–346. [Google Scholar]
- Altman I, Rogoff B. World Views in Psychology: Trait, Interactional, Organismic, And Transactional Perspectives. In: Stokols D, Altman I, editors. Handbook of Environmental Psychology. John Wiley & Sons; New York: 1987. [Google Scholar]
- Aubry T, Myner J. Community integration and quality of life: A comparison of persons with psychiatric disabilities in housing programs and community residents who are neighbors. Candian Journal of Mental Health. 1999;15:5–20. doi: 10.7870/cjcmh-1996-0001. [DOI] [PubMed] [Google Scholar]
- Barrera M. Social support research in community psychology. In: Rappaport J, Seidman E, editors. Handbook of Community Psychology. Kluwer/ Plenum; New York: 2000. pp. 215–246. [Google Scholar]
- Bond GR, Salyers MP, Rollins AL, Rapp CA, Zipple AM. How evidence-based practices contribute to community integration. Community Mental Health Journal. 2004;40:569–588. doi: 10.1007/s10597-004-6130-8. [DOI] [PubMed] [Google Scholar]
- Carling PJ. Housing and supports for persons with mental illness: Emerging approaches to research and practice. Hospital and Community Psychiatry. 1993;44:439–449. doi: 10.1176/ps.44.5.439. [DOI] [PubMed] [Google Scholar]
- Carling PJ. Return to Community: Building Support Systems for People with Psychiatric Disabilities. The Guilford Press; New York: 1995. [Google Scholar]
- Chang K. Introduction to Geographic Information Systems. 3rd ed. McGraw Hill; New York: 2005. [Google Scholar]
- Corrigan PW, Salzer M, Ralph RO, Sangster Y, Keck L. Examining the factor structure of the recovery assessment scale. Schizophrenia Bulletin. 2004;30:1035–1041. doi: 10.1093/oxfordjournals.schbul.a007118. [DOI] [PubMed] [Google Scholar]
- Cresswell JW, Plano Clark VL. Designing and conducting mixed methods research. Sage Publications; Thousands Oaks, CA: 2007. [Google Scholar]
- Cummins RA, Lau ALD. Community integration or community exposure? A Review and discussion in relation to people with an intellectual disability. Journal of Applied Research in Intellectual Disabilities. 2003;16:145–157. [Google Scholar]
- Dear MJ, Wolch JR. Landscapes of Despair: From deinstitutionalization to homelessness. Princeton University Press; Princeton, NJ: 1987. [Google Scholar]
- Dewees M, Pulice RT, McCormick LI. Community integration of former state hospital patients: Outcomes of a policy shift in Vermont. Psychiatric Services. 1996;47:1088–1092. doi: 10.1176/ps.47.10.1088. [DOI] [PubMed] [Google Scholar]
- Elwood S. Critical issues in participatory GIS: Deconstruction, reconstruction, and new research directions. Transactions in GIS. 2006;10:693–708. [Google Scholar]
- Felner RD, Felner TY, Silverman MM. Prevention in mental health and social intervention: Conceptual and methodological issues in the evolution of the science and practice of prevention. In: Rappaport J, Seidman E, editors. Handbook of Community Psychology. Kluwer Academic / Plenum Publishers; New York: 2000. pp. 9–42. [Google Scholar]
- Gerber GJ, Prince PN, Duffy S, McDougall L, Cooper J, Dowler S. Adjustment, integration, and quality of life among forensic patients receiving community outreach services. International Journal of Forensic Mental Health. 2003;2:129–136. [Google Scholar]
- Gesler WM, Albert DP. How spatial analysis can be used in medical geography. In: Albert DP, Gesler WM, Levergood B, editors. Spatial Analysis, GIS, and Remote Sensing Applications in the Health Sciences. Ann Arbor Press; Chelsea, MI: 2000. pp. 11–38. [Google Scholar]
- Gesler WM, Meade MS. Locational and population factors in health care-seeking behavior in Savannah, Georgia. Health Services Research. 1988;23:443–462. [PMC free article] [PubMed] [Google Scholar]
- Gollege RG, Stimson RJ. Analytical Behavioral Geography. Croon Helm; London: 1987. [Google Scholar]
- Grant J, Nelson G, Mitchell T. Negotiating the challenges of participatory action research: Relationships, power, participation, change, and credibility. In: Reason P, Bradbury H, editors. The Sage handbook of action research: Participatory inquiry in practice. 2nd Ed. Sage Publications; Los Angeles: 2008. [Google Scholar]
- Green EP, Kloos B. Using geospatial technologies to learn about communities, build relationships, and pursue social action. 2008 Manuscript under review. [Google Scholar]
- Gulcer L, Tsemberis S, Stefancic A, Greenwood RM. Community integration of adults with psychiatric disabilities and histories of homelessness. Community Mental Health Journal. 2007;43:211–228. doi: 10.1007/s10597-006-9073-4. [DOI] [PubMed] [Google Scholar]
- Harries K. Mapping Crime: Principles and Practice. U.S. Department of Justice; Washington, D.C.: 1999. [Google Scholar]
- Israel BA, Schulz AJ, Parker EA, Becker AB, Allen A, Guzman JR. Critical issues in developing and following community-based participatory research principles. In: Minkler M, Wallerstein N, editors. Community-Based Participatory Research for Health. Jossey-Bass; San Francisco: 2003. pp. 56–73. [Google Scholar]
- Jason LA, Keys CB, Suarez-Balcazar YS, Tayor RR, Davis I. Participatory community research: Theories and methods in action. American Psychological Association; Washington, D.C.: 2004. [Google Scholar]
- Kloos B. Creating new possibilities for promoting liberation, well-being, and recovery: Learning from experiences of psychiatric consumers/ survivors. In: Nelson G, Prillitensky I, editors. Community Psychology: In Pursuit of Well-being and Liberation. MacMillan, London; London: 2005a. pp. 426–447. [Google Scholar]
- Kloos B. Community science: An alternative place to stand? American Journal of Community Psychology. 2005b;35:259–267. doi: 10.1007/s10464-005-3405-3. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Kloos B, Townley G, Green EP. Housing environment predictors of residential stability in supported housing for persons with SMI. Manuscript under review. [Google Scholar]
- Kloos B, Shah S, Green EP, Townley G, Wright PA, Stillman L, Lau J, McGregor B, Smolowitz R, McDaneil J, Chien V. Investigating the impact of housing environments on the adaptive functioning for persons with serious mental illness living in residences. 2008 Manuscript in preparation. [Google Scholar]
- Knigge L, Cope. M. Grounded visualization: Integrating the analysis of qualitative and quantitative data though grounded theory and visualization. Environment and Planning A. 2006;38:2021–2037. [Google Scholar]
- Kwan M-P, Knigge L. Doing qualitative research using GIS: An oxymoronic endeavor? Environment and Planning A. 2006:1999–2002. [Google Scholar]
- Lehman AF. Measuring quality of life in a reformed health system. Health Affairs. 1995;14:90–101. doi: 10.1377/hlthaff.14.3.90. [DOI] [PubMed] [Google Scholar]
- Linney JA. Assessing ecological constructs and community context. In: Rappaport J, Seidman E, editors. Handbook of Community Psychology. Klumer Academic/Plenum; New York: 2000. pp. 647–668. [Google Scholar]
- Long DA, Perkins DD. Confirmatory Factor Analysis of the Sense of Community Index: Development of a Brief SCI. Journal of Community Psychology. 2002;31:279–296. [Google Scholar]
- Luke DA. Getting the big picture in community science: Methods that capture context. American Journal of Community Psychology. 2005;35:185–200. doi: 10.1007/s10464-005-3397-z. [DOI] [PubMed] [Google Scholar]
- Lynch, Kevin . The Image of the City. MIT Press; Cambridge M.A.: 1960. [Google Scholar]
- Mason M. Applications of Geographic Information Systems to Community Psychology Research & Practice; Discussant Paper presented at the annual meeting of the Society for Community Research and Action; Pasadena, CA. Jun, 2007. [Google Scholar]
- McCormick BP, Funderburk JA, Lee Y, Hale-Fought M. Activity characteristics and emotional experience: Predicting boredom and anxiety in the daily life of community mental health clients. Journal of Leisure Research. 2005;37:236–253. [Google Scholar]
- Nemet GF, Bailey AJ. Distance and health care utilization among the rural elderly. Social Science Medicine. 2000;50:197–208. doi: 10.1016/s0277-9536(99)00365-2. [DOI] [PubMed] [Google Scholar]
- Nelson G, Lord J, Ochocka J. Empowerment and mental health in community: Narratives of psychiatric consumer/survivors. Journal of Community and Applied Social Psychology. 2001;11:125–142. [Google Scholar]
- Newman S. Housing attributes and serious mental illness: Implications for research and practice. Psychiatric Services. 2001;52:1309–1317. doi: 10.1176/appi.ps.52.10.1309. [DOI] [PubMed] [Google Scholar]
- Parker B. Constructing community through maps? Power and praxis in community mapping. The Professional Geographer. 2006;58:470–484. [Google Scholar]
- Pearce J, Witten K, Bartie P. Neighbourhoods and health: A GIS approach to measuring community resource accessibility. Journal of Epidemiology & Community Health. 2006;60:389–395. doi: 10.1136/jech.2005.043281. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Pinfold V. ‘Building up safe havens.. all around the world’: Users’ experiences of living in the community with mental health problem. Health & Place. 2000;6:201–212. doi: 10.1016/s1353-8292(00)00023-x. [DOI] [PubMed] [Google Scholar]
- Prince PN, Gerber GJ. Subjective well-being and community integration among clients of assertive community treatment. Quality of Life Research. 2005;14:161–169. doi: 10.1007/s11136-004-2407-1. [DOI] [PubMed] [Google Scholar]
- Prince PN, Prince CR. Perceived stigma and community integration among clients of Assertive Community Treatment. Psychiatric Rehabilitation Journal. 2002;25:323–331. doi: 10.1037/h0095005. [DOI] [PubMed] [Google Scholar]
- Rappaport J. Research methods and the empowerment social agenda. In: Tolan P, Keys C, Chertok F, Jason L, editors. Researching community psychology: Issues and methods. American Psychological Association; Washington, D.C.: 1990. [Google Scholar]
- Rog DJ. The evidence on supported housing. Psychiatric Rehabilitation Journal. 2004;27:334–344. doi: 10.2975/27.2004.334.344. [DOI] [PubMed] [Google Scholar]
- Segal SP, Baumohl J, Moyles EW. Neighborhood types and community reaction to the mentally ill: A paradox of intensity. Journal of Health and Social Behavior. 1980;21:345–359. [PMC free article] [PubMed] [Google Scholar]
- Sherman JE, Spencer J, Preisser JS, Gesler WM, Arcury TA. A suite of methods for representing activity spaces in a healthcare accessibility study. International Journal of Health Geographics. 2005;4 doi: 10.1186/1476-072X-4-24. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Strauss JS, Carpenter WT. Prediction of outcome in schizophrenia: III. Five-year outcome and its predictors. Archives of General Psychiatry. 1977;34:159–163. doi: 10.1001/archpsyc.1977.01770140049005. [DOI] [PubMed] [Google Scholar]
- Tebes JK. Community science, philosophy of science, and the practice of research. American Journal of Community Psychology. 2005;35:213–230. doi: 10.1007/s10464-005-3399-x. [DOI] [PubMed] [Google Scholar]
- Townley G, Kloos B. Examining the psychological sense of community among individuals with serious mental illness residing in supported housing environments. 2008 doi: 10.1007/s10597-010-9338-9. Manuscript under review. [DOI] [PubMed] [Google Scholar]
- Verheij RA. Explaining urban-rural variations in health: A review of interactions between individual and environment. Social Science Medicine. 1996;42:923–935. doi: 10.1016/0277-9536(95)00190-5. [DOI] [PubMed] [Google Scholar]
- Wong Y-L, I, Solomon P. Community integration of persons with psychiatric disabilities in supportive independent housing: Conceptual model and methodological issues. Mental Health Services Research. 2002;4:13–28. doi: 10.1023/a:1014093008857. [DOI] [PubMed] [Google Scholar]
- Wright PA, Kloos B. Housing Environment and Mental Health Outcomes: A Levels of Analysis Perspective. Journal of Environmental Psychology. 2007;27:79–89. doi: 10.1016/j.jenvp.2006.12.001. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yanos PT. Beyond “landscapes of despair”: The need for new research on the urban environment, sprawl, and the community integration of persons with serious mental illness. Health and Place. 2007;13:672–676. doi: 10.1016/j.healthplace.2006.10.002. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yanos PT, Barrow SM, Tsemberis S. Community integration in the early phase of housing among homeless persons diagnosed with severe mental illness: Success and challenges. Community Mental Health Journal. 2004;40:133–150. doi: 10.1023/b:comh.0000022733.12858.cb. [DOI] [PubMed] [Google Scholar]