

Abstract
We report a case of a 55-year-old male patient with breast carcinoma, who developed choroidal metastasis. The patient had undergone mastectomy for carcinoma of right breast, five years ago. The patient was advised close follow-up for the left eye, as he was already on tamoxifen therapy (started a month ago) for spinal metastasis. On last follow-up, a year later, the choroidal lesion had completely scarred, with no recurrences. Systemic hormonal therapy like tamoxifen given for the breast primary and other systemic metastases may cause regression of the choroidal metastasis, thereby avoiding ocular radiotherapy. Medline search revealed only one published case of regression of choroidal metastasis from a male breast primary, on tamoxifen therapy.
Keywords: Choroidal metastasis, male breast carcinoma, tamoxifen
Choroidal metastases occur most frequently from the breast in females and from the lungs in males.1 Breast carcinoma in males is very rare, accounting for 1% of all breast carcinomas, with choroidal metastasis in males being still rarer.2 We report a male patient with breast carcinoma with choroidal metastasis, which regressed on systemic tamoxifen therapy.
Case Report
A 55-year-old male patient presented with complaints of sudden, painless decrease of vision in the left eye, since 10 days. Past history was significant for right breast carcinoma and subsequent mastectomy, five years ago [Fig. 1]. Yearly routine evaluation had revealed spinal metastasis, a month prior to presentation with ocular symptoms. As the metastasis and the primary were both very high in hormonal receptors, the medical oncologist had started the patient on oral tamoxifen 20 mg a day, for the spinal metastasis.
Figure 1.

External photograph of chest of patient, showing right-sided mastectomy
The best corrected visual acuity (BCVA) was 20/60 and 3/120, in the right and left eye respectively. Right eye and left eye anterior segment examination was unremarkable.
Left fundus examination revealed a grayish yellow macular mass; approximately 20x15 mm in size, with surrounding exudative retinal detachment [Fig. 2a]. Ultrasonography (USG) B-Scan of the left eye showed a raised subretinal mass with high surface reflectivity and moderate internal reflectivity, associated with a surrounding retinal detachment [Fig. 2b]. Fundus fluorescein angiography could not be performed as the patient refused any invasive diagnostic intervention. A choroidal metastasis from the breast carcinoma was diagnosed. The patient refused ocular external beam radiotherapy (EBRT) for the choroidal lesion and was advised close follow-up, every three months, as he was already on systemic hormonal therapy started a month ago.
Figure 2A.
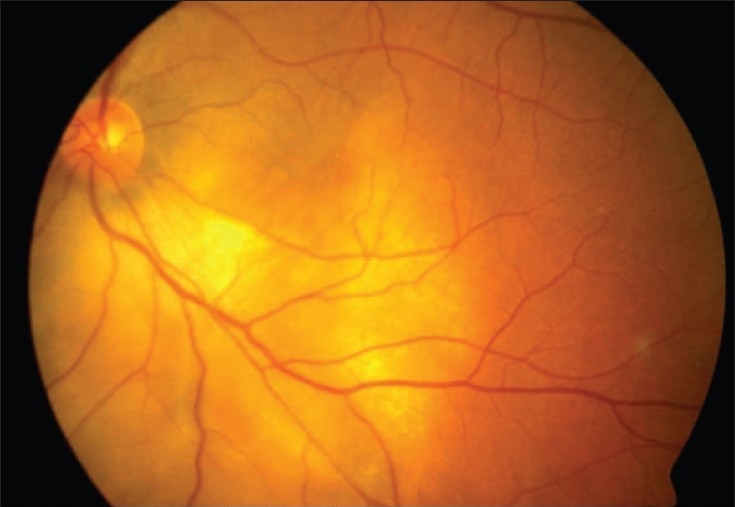
a: Color fundus photograph of the left eye showing the presence of a dome-shaped yellow-colored irregular choroidal mass with surrounding subretinal fluid, measuring approximately 20 × 15 mm in size, in the macular region and extending below the inferotemporal vascular arcade
Figure 2B.
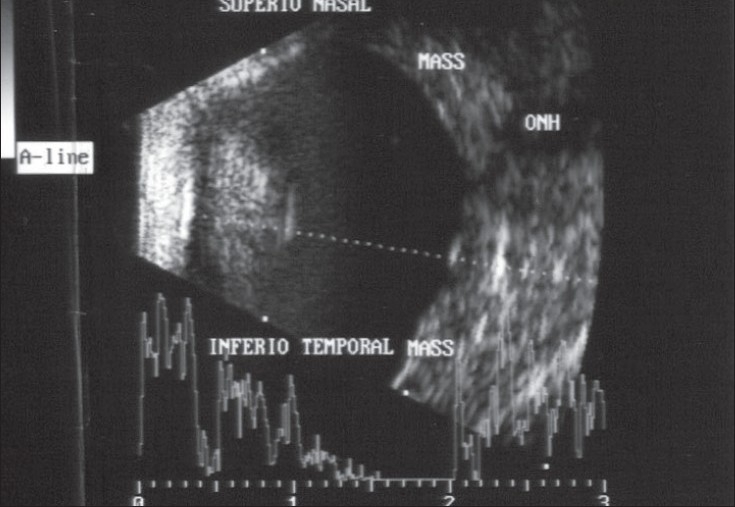
b: USG B-Scan with A-Scan vector showing the presence of a raised inferotemporal choroidal mass with high surface reflectivity and low to moderate internal reflectivity
The choroidal lesion gradually scarred, with complete absorption of subretinal fluid.
On final follow-up one year later, the choroidal lesion had completely healed with scarring [Fig. 3a] with no recurrences in either eye. The USG B-scan of the left eye showed flattening of the subretinal mass [Fig. 3b]. Optical coherence tomography of the left eye revealed no sign of activity [Fig. 3c]. The BCVA was counting fingers at two feet, at final visit.
Figure 3a.
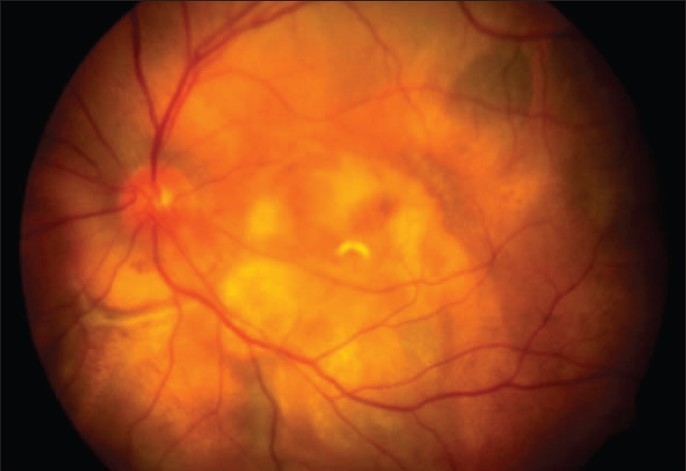
a: Color fundus photograph of the left eye showing the presence of scarring with surrounding hyperpigmentation in the area of the earlier mass, in the macular region and extending below the inferotemporal vascular arcade
Figure 3b.
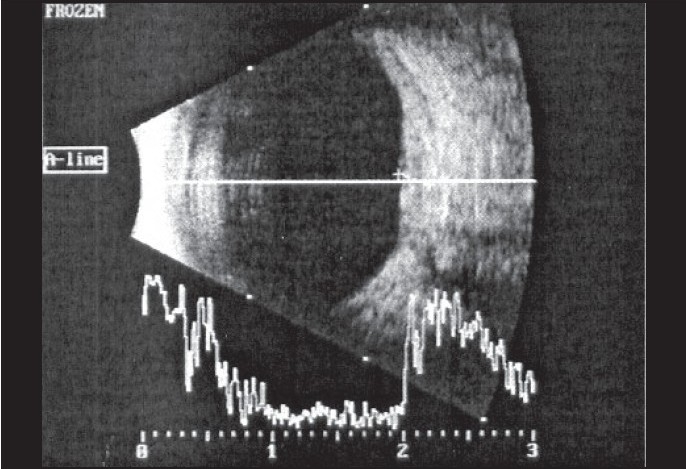
b: USG B-Scan with A-Scan vector showing the flattening of the inferotemporal mass
Figure 3c.

c: Optical coherence tomography of the left eye showing normal foveal architecture
Discussion
Breast carcinoma in males presenting with a median age of 67 years is virtually silent, hence needing a high index of suspicion for diagnosis.3 Systemic chemotherapy4 and hormonal therapy5 given for the systemic condition have been reported to cause regression of choroidal metastasis. This obviates the need for ocular intervention like radiotherapy, preventing its side-effects. Breast carcinoma in males has a higher concentration of estrogen and progesterone receptors than in the female, thus rendering both the primary and the metastasis more susceptible to hormonal manipulation.5
The probable reason why there is only one reported case of regression on tamoxifen therapy may be partly because choroidal metastasis in breast carcinoma in males is so rare and also partly because most clinicians and patients opt for localized radiotherapy as a mode of control of the choroidal lesion. It is difficult to comment on whether the patient would have had better final visual acuity if the fundus lesion had been subjected to EBRT. EBRT usually leads to a flat scar while in this case there was elevated scarring. It would not be possible to comment on the above without evaluating two sets of patients, one of whom was subjected to ocular EBRT versus another treated with systemic therapy alone. But, in debilitated patients who refuse EBRT with its associated ocular side-effects as a mode of therapy, it may be worthwhile to remember that hormonal therapy may itself cause regression of the choroidal mass. This might also have some clinical relevance for females with choroidal metastases from breast carcinoma.
In summary, we report a case of breast carcinoma in males with suspected choroidal metastasis which completely healed with systemic hormonal therapy. We report this case to highlight this rare source of choroidal metastasis, in males and to document the role of systemic therapy in its regression.
References
- 1.Chong JT, Mick A. Choroidal metastasis: case reports and review of the literature. Optometry. 2005;76:293–301. doi: 10.1016/s1529-1839(05)70312-2. [DOI] [PubMed] [Google Scholar]
- 2.Carmalt HL, Mann LJ, Kennedy CW, Fletcher JM, Gillett DJ. Carcinoma of the male breast: A review and recommendations for management. Aust N Z J Surg. 1998;68:712–5. doi: 10.1111/j.1445-2197.1998.tb04657.x. [DOI] [PubMed] [Google Scholar]
- 3.Donegan WL, Redlich PN. Breast cancer in men. Surg Clin North Am. 1996;76:343–63. doi: 10.1016/s0039-6109(05)70443-6. [DOI] [PubMed] [Google Scholar]
- 4.Paoli D. Regression of choroidal metastasis from a carcinoma of the male breast: Case report. Ophthalmologica. 1998;212:74–6. doi: 10.1159/000055432. [DOI] [PubMed] [Google Scholar]
- 5.Cohen VM, Moosavi R, Hungerford JL. Tamoxifen-induced regression of a choroidal metastasis in a man. Arch Ophthalmol. 2005;123:1153–4. doi: 10.1001/archopht.123.8.1153. [DOI] [PubMed] [Google Scholar]