

Abstract
We report a case of sudden loss of vision due to the development of acute myopia after the intake of chlorthalidone used for treating systemic hypertension. Clinically this was associated with ciliary spasm, shallow peripheral choroidal effusion and retinal striae at the macula with increase in macular thickness seen on optical coherence tomography. All these findings were reversed completely once the drug was discontinued. Development of acute myopia should be kept in mind as an adverse effect of a commonly used antihypertensive drug, namely chlorthalidone.
Keywords: Acute myopia, chlorthalidone, diuretic
Acute myopia is a rare idiosyncratic response to systemic use of medications. Different drugs have been reported to be the cause of this rare phenomenon.1,2,3,4,5,6 The frequent culprits reported belong to the Sulphonamide group of drugs3,4 and diuretics.5,6 Here we present a case of sudden onset of blurring of vision in a young male following ingestion of chlorthalidone for systemic hypertension. The transient myopia disappeared on discontinuation of the drug.
Case Report
A 30-year-old male presented in the emergency department with a history of bilateral blurring of vision of one-day duration. He had never worn glasses and past medical history was notable for hypertension. He was taking atenelol 50 mg (Hipres, CIPLA Pharmaceuticals). Since his systemic hypertension was not well controlled with this drug his physician had switched over to a combination of atenelol 50 mg with chlorthalidone 12.5 mg (Tenoric 50, IPCA Pharmaceuticals). He started this medication four days prior to the episode of blurring of vision. Visual acuity at presentation was 20/120 in both eyes. Slit-lamp examination of the anterior segment was unremarkable. Direct and consensual pupillary reactions were normal. Color vision testing using Ishihara′s pseudo isochromatic chart was within normal limits. Refraction was done and his visual acuity was improving to 20/20 in both eyes with a spherical correction of -5 diopter sphere (DS). Gonioscopy revealed normal open angle in both the eyes. A cycloplegic refraction revealed a value of -3 DS/-0.5 diopter cylinder (DC) x 80° in the right eye and -3.75 DS/-1.0 DC x 130° in the left eye. Indirect ophthalmoscopic examination revealed shallow peripheral choroidal elevation. Slit-lamp biomicroscopy revealed retinal striae radiating from the fovea [Figs. 1A and B]. There were no vitreous cells. B-scan ultrasonography showed shallow peripheral serous choroidal detachment [Fig. 2]. A-scan biometry was done to measure the axial length. An optical coherence tomogram (OCT - Stratus version 4.0, Zeiss ophthalmics) was also done since retinal striae were present, which showed a mild thickening of the macula. The patient′s blood pressure was 140/100 mmHg in the forearm in supine position. Hematological evaluation including renal parameters and computerized tomogram of the head were within normal limits.
Figure 1A.
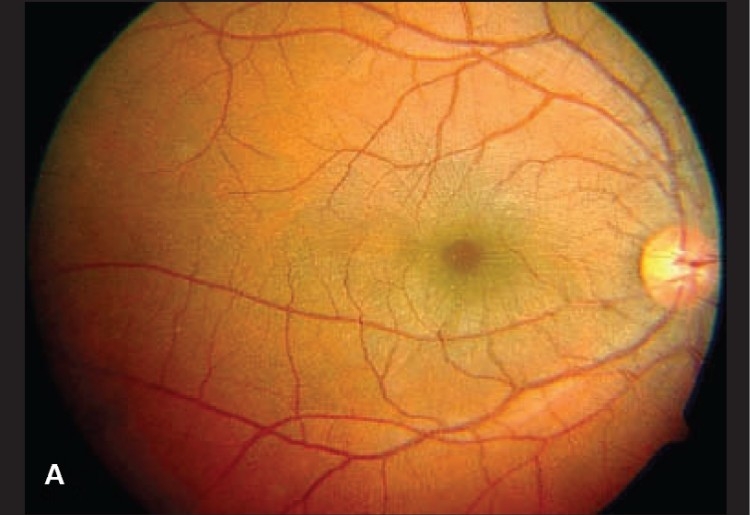
A: Color fundus photograph showing retinal striae radiating from the fovea in the right eye at presentation
Figure 1B.
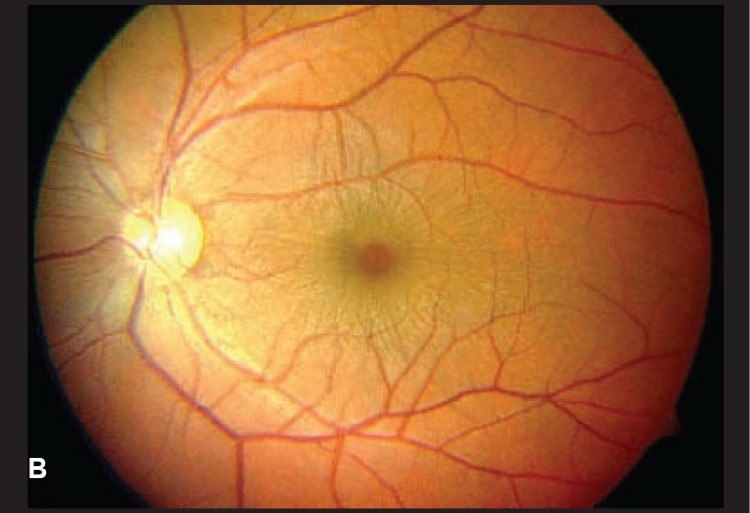
B: Left eye showing retinal striae at presentation
Figure 2.

B scan Ultrasonography of retinal periphery using transverse section showing shallow choroidal effusion
The patient was advised to stop atenelol chlorthalidone combination drug. He was reviewed after five days and his visual acuity had improved to 20/20 without any refractive error. Fundus examination revealed disappearance of retinal striae at the macula and peripheral choroidal effusion had also resolved [Figs. 3A and B]. The OCT was repeated which showed reduction in the thickening at the macula. A change analysis was done using the software in Stratus OCT version 4.0 which revealed definite reduction in the thickness of the macula. A presumptive diagnosis of drug-induced acute myopia due to chlorthalidone was made.
Figure 3A.
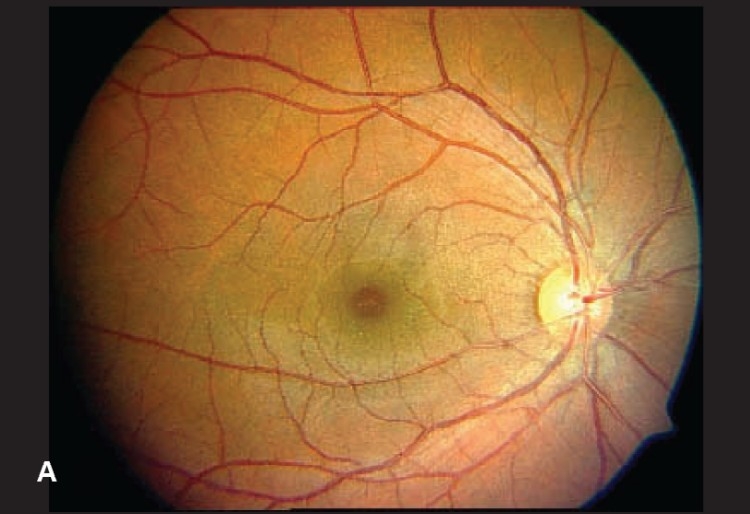
A: Disappearance of retinal striae in the right eye after stopping the drug
Figure 3B.
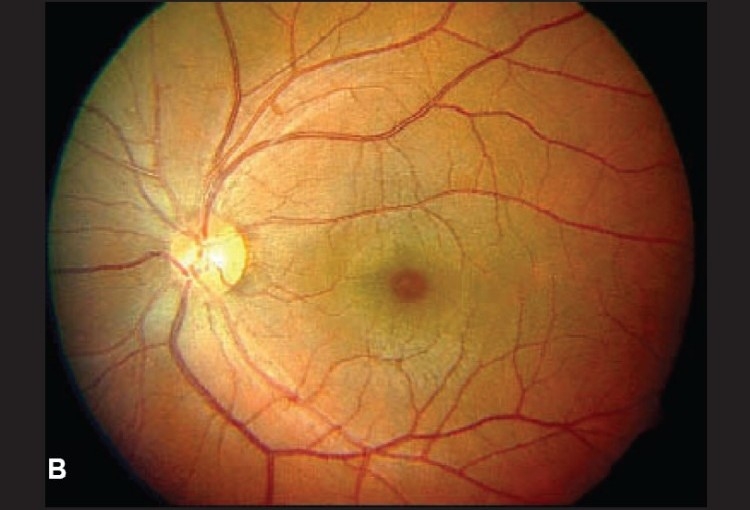
B: Left eye with normal macula at the end of one week
Discussion
We report a case of acute myopia induced by oral consumption of chlorthalidone for systemic hypertension. Chlorthalidone is a monosulfonyl diuretic used widely for the treatment of systemic hypertension. Acute transient myopia may be induced by several drugs and different mechanisms have been described. The exact mechanism producing acute myopia is not very clear even though it has been postulated to be due to ciliary body effusion,1 peripheral uveal effusion2 and ciliary spasm3 and lens swelling. Oral sulphonamides cause transient myopia as a result of forward displacement of the lens due to allergic ciliary body edema and rotation.3,4 Intravenous administration of equine anti lymphocytic globulins causes transient myopia due to ciliary spasm.7 Some of the other drugs that have been described to cause transient myopia include indapamide,5 hydrochlorothiazide,2 triamterene2 and topiramate.8,9 In this case a combination of ciliary spasm and peripheral choroidal effusion explain the induced myopia. Since the cycloplegic refraction showed a decrease in myopic shift by about 2 diopter it is evident that there was an element of ciliary spasm. Peripheral choroidal effusion was documented by B scan ultrasonography. Retinal striae have been reported to occur with acute myopia after drug intake.10 Ciliary body rotation and edema resulting in forward movement of iris lens diaphragm has been reported as a possible cause for induced myopia by some authors.1,2,3,11 In this case there was no definite shallowing of the anterior chamber. We feel that this mechanism may not explain the pathogenesis of myopia in this case. To our knowledge this is the first report of this adverse reaction of chlorthalidone from India. Since this is a common diuretic used in the treatment of systemic hypertension, we feel that it is important to be aware of this possible idiosyncratic adverse effect.
References
- 1.Krieg PH, Schipper I. Drug-induced ciliary body edema: A new theory. Eye. 1996;10:121–6. doi: 10.1038/eye.1996.21. [DOI] [PubMed] [Google Scholar]
- 2.Soylev MF, Green RL, Feldon SE. Choroidal effusion as a mechanism for transient myopia induced by hydrochlorothiazide and triamterene. Am J Ophthalmol. 1995;120:395–7. doi: 10.1016/s0002-9394(14)72174-9. [DOI] [PubMed] [Google Scholar]
- 3.Grinbaum A, Ashkenazi I, Gutman I, Blumenthal M. Suggested mechanism for acute transient myopia after sulfonamide treatment. Ann Ophthalmol. 1993;25:224–6. [PubMed] [Google Scholar]
- 4.Bovino JA, Marcus DF. The mechanism of transient myopia induced by sulfonamide therapy. Am J Ophthalmol. 1982;94:99–102. doi: 10.1016/0002-9394(82)90199-4. [DOI] [PubMed] [Google Scholar]
- 5.Blain P, Paques M, Massin P, Erginay A, Santiago P, Gaudric A. Acute transient myopia induced by indapamide. Am J Ophthalmol. 2000;129:538–540. doi: 10.1016/s0002-9394(99)00402-x. [DOI] [PubMed] [Google Scholar]
- 6.Stennis SD. Drug-induced myopia: A case report. Am J Optom Physiol Opt. 1976;53:422–3. [PubMed] [Google Scholar]
- 7.Milea D, Zech C, Dumontet C, Coiffier B, Trepsat C. Transient acute myopia induced by antilymphocyte globulins. Ophthalmologica. 1999;213:133–4. doi: 10.1159/000027406. [DOI] [PubMed] [Google Scholar]
- 8.Craig JE, Ong TJ, Louis DL, Wells JM. Mechanism of topiramate-induced acute-onset myopia and angle closure glaucoma. Am J Ophthalmol. 2004;137:193–5. doi: 10.1016/s0002-9394(03)00774-8. [DOI] [PubMed] [Google Scholar]
- 9.Desai CM, Ramchandani SJ, Bhopale SG, Ramchandani SS. Acute myopia and angle closure caused by topiramate, a drug used for prophylaxis of migrane. Indian J Ophthalmol. 2006;54:195–7. doi: 10.4103/0301-4738.27072. [DOI] [PubMed] [Google Scholar]
- 10.Ryan EH, Jr, Jampol LM. Drug-induced acute transient myopia with retinal folds. Retina. 1986;6:220–3. doi: 10.1097/00006982-198606040-00005. [DOI] [PubMed] [Google Scholar]
- 11.Postel EA, Assalian A, Epstein DL. Drug-induced transient myopia and angle-closure glaucoma associated with supraciliary choroidal effusion. Am J Ophthalmol. 1996;122:110–2. doi: 10.1016/s0002-9394(14)71972-5. [DOI] [PubMed] [Google Scholar]