

Abstract
Context:
There is growing body of evidence that use of computers can adversely affect the visual health. Considering the rising number of computer users in India, computer-related asthenopia might take an epidemic form. In view of that, this study was undertaken to find out the magnitude of asthenopia in computer operators and its relationship with various personal and workplace factors.
Aims:
To study the prevalence of asthenopia among computer operators and its association with various epidemiological factors.
Settings and Design:
Community-based cross-sectional study of 419 subjects who work on computer for varying period of time.
Materials and Methods:
Four hundred forty computer operators working in different institutes were selected randomly. Twenty-one did not participate in the study, making the nonresponse rate 4.8%. Rest of the subjects (n = 419) were asked to fill a pre-tested questionnaire, after obtaining their verbal consent. Other relevant information was obtained by personal interview and inspection of workstation.
Statistical Analysis Used:
Simple proportions and Chi-square test.
Results:
Among the 419 subjects studied, 194 (46.3%) suffered from asthenopia during or after work on computer. Marginally higher proportion of asthenopia was noted in females compared to males. Occurrence of asthenopia was significantly associated with age of starting use of computer, presence of refractive error, viewing distance, level of top of the computer screen with respect to eyes, use of antiglare screen and adjustment of contrast and brightness of monitor screen.
Conclusions:
Prevalence of asthenopia was noted to be quite high among computer operators, particularly in those who started its use at an early age. Individual as well as work-related factors were found to be predictive of asthenopia.
Keywords: Asthenopia, computer operators, epidemiological factors
The number of computer users is rising exponentially worldwide and is expected to exceed 1 billion by 2010, up from around 670 million today, fueled primarily by new adopters in developing nations such as China, Russia and India, according to analysts.1 However, working at a computer terminal is not free from health hazards to eyes as it puts significant stress on visual functions. There is growing body of evidence that use of computers can adversely affect visual health.2-6 The adverse health effects on eyes include asthenopic symptoms such as eyestrain, tired eyes, irritation, redness, blurred vision and double vision.
The problem is significant in countries like USA, with visual display terminal (VDT) workers complaining of asthenopia one and a half times as often as patients who perform conventional office work.5 Computer-related headache and eyestrain are reported during as many as 10 to 15% of routine eye examinations, and some state that nearly 50% of VDT workers experience some eye discomfort. The yearly cost of diagnosing and treating these issues may approach $2 billion.5 In India, the major symptoms related to computer use reported by the ophthalmologists were eyestrain, headache, tiredness and burning sensation, watering and redness.7
The estimated numbers of computers and net connections in India for 2005 were 15 million and 5 million respectively.8 Looking to the huge population at risk of developing asthenopia associated with computer use, it may take an epidemic form in the near future. The aim of the study was to estimate the prevalence of asthenopia among computer operators and its association with various epidemiological factors.
Materials and Methods
The study was carried out in two talukas of Anand district in Gujarat, namely, Anand and Petlad, from May 2004 to January 2006. A pilot study was done in one of the colleges of Vallabh Vidyanagar (where students use computers as a part of their curriculum), under PSBH (Problem Solving for Better Health) project by final MBBS students of P. S. Medical College, Karamsad. This study revealed 20% prevalence of computer- related health problems. Considering 20% allowable error and using formula Z2α/2 pq/E2, sample size turned out to be 400. Forty were added to this figure, taking into account 10% nonresponders. Thus, 440 was the final sample size.
After seeking approval of the human research ethical committee of P. S. Medical College, Karamsad, establishments and institutes where computers are extensively used, in Anand and Petlad taluka, were enlisted. These included banks, computer training centers and colleges running degree courses in computer applications. Heads of these institutes were approached for permitting institute′s faculty members and final year students to participate in the study. They were explained the aims, objectives and methodology of the project. After seeking their permission, all the staff and faculty members, as well as final year students, were enlisted. Four hundred and forty subjects were selected randomly. Twenty-one subjects did not participate in the study, making the nonresponse rate 4.8%. Rest of the subjects (n = 419) were asked to fill a pre- tested questionnaire, after obtaining their verbal consent. Other relevant information was obtained by personal interview and inspection of workstation. None of the subjects were found to be suffering from conjunctivitis or inflammation of eyelids. To know about the habit of taking breaks, respondents were asked whether they take a 3 to 5 min break after each hour of continuous computer work and a 10 to 15-min break after 2 hours of continuous computer work (as per OR-OSHA guidelines),9 i.e., moving around or doing some work other than computer operation. Asthenopia was considered when two of the following symptoms were reported during or after work on computer: smarting sensation, gritty feeling, itching in eyes, aches, sensitivity, redness, tears in excess, dryness, discomfort in seeing, blurring of vision and discoloration of objects. Observations were analyzed and χ2 test was applied to find out the association.
Results
Mean age of the subjects who participated in this study was 25.04 years, with a range of 18 to 55 years. Three-fourths of the subjects were young, with age of 15 to 25 years; and 279 (66.6%) were male [Table 1]. Out of all respondents, only 1 (0.2%) was diabetic and 4 (1.0%) were hypertensive. A majority of subjects, i.e., 391 (93.3%) subjects, started use of computers at a young age, of less than 25 years; and 294 (70.2%) subjects reported habit of taking breaks during computer work [Table 2]. Two hundred thirty-six (56.3%) subjects were using computers since less than 5 years, and 172 (41.1%) subjects used to work on computers for about 21 to 40 h in a week [Table 3]. Out of total 151 (36.0%) subjects with refractive error [Table 4], 148 (35.3%) were using glasses; and only 3 (0.7%) were wearing contact lenses during computer work. Table 5 depicts that 277 (66.1%) subjects used to keep an eye distance of 13 to 24 inches from the monitor screen while working on the computer, whereas 262 (62.5%) subjects had the top of their computer screen at the same level of eyes. Antiglare screen was used by 142 (33.9%) computer operators, while 327 (78.0%) were adjusting contrast and brightness of the computer screen as per their need [Table 6]. In our study, asthenopia was reported in 194 (46.3%) subjects during or after work on computer, out of which 51 (26.0%) were strongly asthenopic, reporting at least one of the symptoms of asthenopia every day, while 145 (74.0%) experienced it occasionally. Eighteen out of 33 subjects in the age group of 36 to 55 years reported asthenopia. Marginally higher proportion of asthenopia was noted in females compared to males. Asthenopia was not found to be associated with age or gender of subject [Table 1], habit of taking breaks [Table 2] and duration of computer use, both in terms of number of years as well as hours per week [Table 3]; while statistically significant association (P < 0.05) was found between occurrence of asthenopia and age of starting use of computers [Table 2], presence of refractive error [Table 4], eye distance from the screen of monitor and level of top of the computer screen [Table 5], as well as use of antiglare screen and adjustment of contrast and brightness as per need [Table 6].
Table 1.
Occurrence of asthenopia in relation to age and gender of the subject
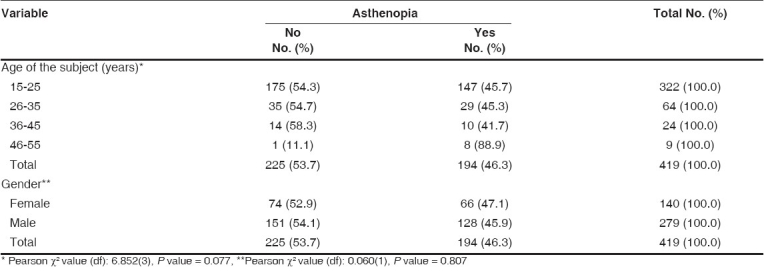
Table 2.
Occurrence of asthenopia in relation to background variables
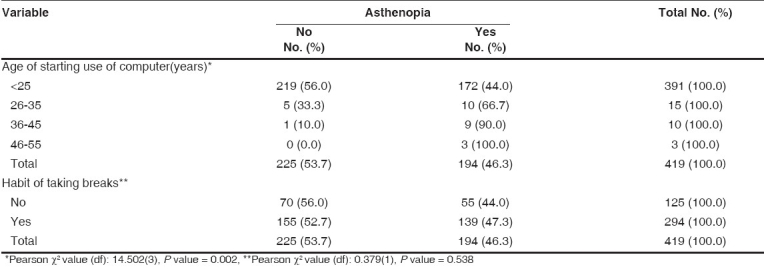
Table 3.
Occurrence of asthenopia in relation to duration of computer use
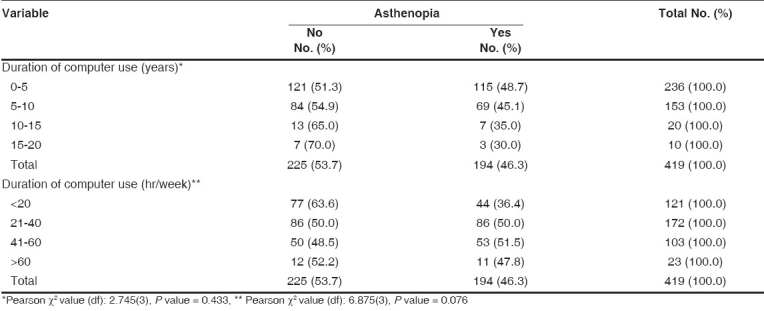
Table 4.
Occurrence of asthenopia in relation to presence of refractive error (corrected)

Table 5.
Occurrence of asthenopia in relation to background variables
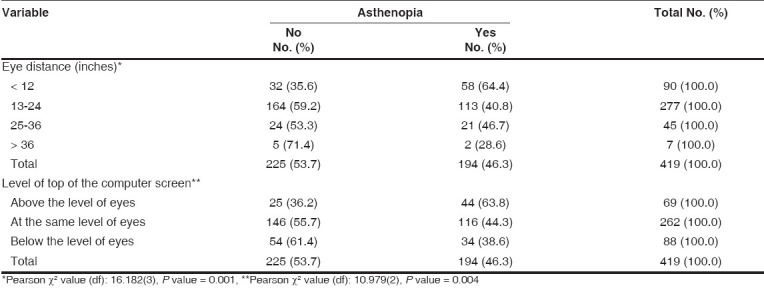
Table 6.
Occurrence of asthenopia in relation to background variables

Discussion
Computer has now become basic and essential desktop equipment in almost every establishment. But the human- computer interface is not free from health hazards. The research over the past two decades shows that visual-comfort problems associated with VDTs such as computer are real.10 Our study found a high prevalence of asthenopia (46.3%) in computer operators. Mocci et al. reported the prevalence of this asthenopia as 31.9% in their study performed on 385 bank workers of Italy, out of which 13.6% were strongly asthenopic6; while Sanchez- Roman et al. found this prevalence to be as high as 68.5% in their study in Spain.11
Though asthenopia was reported to be higher in the older age group and in females in our study, it was not statistically significant. Asthenopia was correlated with age and gender in the study by Mocci et al.6 Visual symptom scores in VDT operators were found to be higher among females than males in a Japanese study by Shima et al.12 However, they did not find any difference with respect to age. Rocha and Debert- Ribeiro studied systems analysts in Brazil and found that visual fatigue was associated with gender, being higher in female analysts.13
Correlation of age of starting use of computers with occurrence of visual discomfort has not been studied much. In our study, age of starting use of computer was found to be a predictor of asthenopia. While considering duration of computer use, review of literature reveals a mixed picture as far as occurrence of asthenopia is concerned. Hanne et al. found a significant difference in asthenopia and daily hours of VDT work between workers working less than 6 h daily and those working more than 6 hours daily.14 Similarly, a review by Kanitkar et al. showed that duration of computer work is directly related to eye symptoms, and longer duration tends to result in long-lasting complaints, well after VDT work is finished.5 Bergqvist and Knave,3 Sanchez-Roman et al.11 and Shima et al.12 reported similar results. However, no correlation was found between asthenopia and number of hours of work a day at the VDT or number of years spent performing the same work duties in a study by Mocci et al.6 Similarly, our study did not find any association between duration of computer use, both in terms of hours/ week and number of years, and asthenopia. Habit of taking breaks during computer work also showed similar result in the present study.
Our study observed that the subjects having refractive error (even when corrected) are more likely to develop asthenopia. Investigations on visual health complaints by VDT operators by Bergqvist et al.3 and Nakaishi et al.15 have shown similar relationship between asthenopia and presence of refractive error in the subjects.
The viewing distance, i.e., the distance between the operator′s eyes and monitor screen, should be individually adjusted. However, placing the VDT 50 to 70 cm away allows for physiologic resting levels of convergence and accommodation. Recent studies demonstrate that farther placement of the monitor (90 to 100 cm) may produce even fewer symptoms.5 Taptagaporn et al. based on their study, recommended viewing distance of 50 to 70 cm.16 Jaschinski et al. found that the change from greater to lesser viewing distance produced a larger increase in eyestrain when the VDTs were at eye level.17 Their study also revealed that when operators were free to adjust the viewing distance to achieve the most comfortable screen position, the participants preferred viewing distances between 60 and 100 cm. In our study, asthenopia was less in subjects whose viewing distance was more than 30 cm (12 inches) and highest when it was less than 30 cm (12 inches), which was statistically significant.
Various studies have shown that apart from viewing distance, viewing angle can be a contributing factor in the occurrence of asthenopia. Taptagaporn et al.16 as well as Quaranta et al.18 recommended a downward gaze so as to work comfortably on VDT. Bergqvist and Knave reported increased odds ratios for certain eye discomfort symptoms when the computer operator keeps the terminal at about eye level rather than below eye level.3 Jaschinski et al. in their study, found that high screens result in greater eyestrain than low screens.17 We classified the respondents in our study into three categories: those who have the top of their computer screen (1) above the level of eyes, (2) at the same level of eyes and (3) below the level of eyes. Significantly higher proportion of subjects who had their computer screen at or above the eye level reported asthenopia.
A WHO press release (1998) mentions that glare and reflections from VDT displays can be a source of eyestrain and headache. Use of antiglare filters over VDT screens has been associated with shorter, less frequent and less intense eye complaints in some studies.5 Our study observed significantly lower prevalence of asthenopia in the subjects who used antiglare screen. Similar was the observation in those who adjusted the contrast and brightness of the monitor screen as per their need.
Conclusion
Our study suggests that asthenopia is a common problem among computer operators, particularly in those who start its use at an early age. Presence of refractive error, eye distance from the monitor screen and level of eyes in relation to top of the screen were other associated factors identified for occurrence of asthenopia. Our study also found that use of antiglare screen and adjustment of contrast and brightness as per need might reduce the risk of asthenopia.
Footnotes
Source of Support: Funded by Charutar Arogya Mandal Medical Research Society, H. M. Patel Center for Medical Care and Education, Karamsad, Gujarat
Conflict of Interest: None declared.
References
- 1.A billion PC users on the way. [Last accessed on 2007 Jun 30]. Available from http://news.com. com/A+billion+PC+users+on+the+way/2100-1003_3-5290988.html.
- 2.Tamez Gonzalez S, Ortiz-Hernandez L, Martinez-Alcantara S, Mendez-Ramirez I. Risks and health problems caused by the use of video terminals. Salud Publica Mex. 2003;45:171–80. [PubMed] [Google Scholar]
- 3.Bergqvist UO, Knave BG. Eye discomfort and work with visual display terminals. Scand J Work Environ Health. 1994;20:27–33. doi: 10.5271/sjweh.1432. [DOI] [PubMed] [Google Scholar]
- 4.Dainoff MJ, Happ A, Crane P. Visual fatigue and occupational stress in VDT operators. Hum Factors. 1981;23:421–37. doi: 10.1177/001872088102300405. [DOI] [PubMed] [Google Scholar]
- 5.Kanitkar K, Carlson AN, Richard Y. Ocular problems associated with computer use: The ever-increasing hours spent in front of video display terminals have led to a corresponding increase in visual and physical ills. [Last accessed on 2007 Jun 30];Review of Ophthalmology E-Newsletter. 2005 12:04. Available from: http://www.revophth.com/publish/content/1_699.htm. [Google Scholar]
- 6.Mocci F, Serra A, Corrias GA. Psychological factors and visual fatigue in working with video display terminals. Occup Environ Med. 2001;58:267–71. doi: 10.1136/oem.58.4.267. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 7.Bali J, Navin N, Thakur BR. Computer vision syndrome: A study of the knowledge, attitudes and practices in Indian Ophthalmologists. Indian J Ophthalmol. 2007;55:289–93. doi: 10.4103/0301-4738.33042. [DOI] [PubMed] [Google Scholar]
- 9.India launches its first cheap PC. [Last accessed on 2007 Jun 30]. Available from http://news.bbc.co.uk/1/hi/world/south_asia/4735927.stm.
- 8.Evaluating your computer workstation, How to make it work for you. OR-OSHA Standards and Technical Resources publication. [Last accessed on 2007 Jun 30]. Available from http://www.cbs.state.or.us/osha/pdf/pubs/1863.pdf.
- 10.Boulton M, Sliney DH. Non-ionizing radiation and the eye. In: Baxter PJ, Adams PH, Tar-Ching A, Cockcroft A, Harrington JM, editors. Hunter′s diseases of occupations. 9th ed. London: Arnold; 2000. p. 430. [Google Scholar]
- 11.Sanchez-Roman FR, Perez-Lucio C, Juarez-Ruiz C, Velez-Zamora NM, Jimenez-Villarruel M. Risk factors for asthenopia among computer terminal operators. Salud Publica Mex. 1996;38:189–96. [PubMed] [Google Scholar]
- 12.Shima M, Nitta Y, Iwasaki A, Adachi M. Investigation of subjective symptoms among visual display terminal users and their affecting factors-analysis using log-linear models. Nippon Eiseigaku Zasshi. 1993;47:1032–40. doi: 10.1265/jjh.47.1032. [DOI] [PubMed] [Google Scholar]
- 13.Rocha LE, Debert-Ribeiro M. Working conditions, visual fatigue and mental health among systems analysts in São Paulo, Brazil. Occup Environ Med. 2004;61:24–32. [PMC free article] [PubMed] [Google Scholar]
- 14.Hanne W, Brewitt H, Augenklinik rechts DI, Munchen TU. Changes in visual function caused by work at a data display terminal. Ophthalmologe. 1994;91:107–12. [PubMed] [Google Scholar]
- 15.Nakaishi H, Yamada Y. Abnormal tear dynamics and symptoms of eyestrain in operators of visual display terminals. Occup Environ Med. 1999;56:6–9. doi: 10.1136/oem.56.1.6. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 16.Taptagaporn S, Sotoyama M, Saito S, Suzuki T, Saito S. Visual comfort in VDT workstation design. J Hum Ergol (Tokyo) 1995;24:84–8. [PubMed] [Google Scholar]
- 17.Jaschinski W, Heuer H, Kylian H. Preferred position of visual displays relative to the eyes: A field study of visual strain and individual differences. Ergonomics. 1998;41:1034–49. doi: 10.1080/001401398186586. [DOI] [PubMed] [Google Scholar]
- 18.Quaranta Leoni FM, Molle F, Scavino G, Dickmann A. Identification of the preferential gaze position through elevation of visual fatigue in a selected group of VDU operators: A preliminary study. Doc Ophthalmol. 1994;87:189–97. doi: 10.1007/BF01204797. [DOI] [PubMed] [Google Scholar]