

Abstract
Cutaneous melanoma of the eyelid is a rare entity. We present a 53-year-old male who had a nevus on the left upper eyelid skin since childhood, which transformed into a huge ulcerated hanging mass in the same region. Excision of the mass was done and histopathology confirmed the diagnosis of nodular malignant melanoma. A small preauricular lymph node showed metastatic melanoma on fine needle aspiration cytology.
Keywords: Eyelid neoplasms, malignant melanoma
Melanoma of the eyelid has an incidence of approximately 1% of all eyelid tumors, the conjunctival surface being excluded.1,2 Nodular melanoma of a large size arising and hanging from the skin of the upper eyelid as seen in this case, is an unusual finding.
Case Report
A 53-year-old male presented with an enlarging mass of the left upper eyelid since one year. He gave history of a nevus in the same location since childhood. On examination, a protuberant, nodular, ulcerated brown to black mass measuring 5 × 4.5 × 4 cm was seen arising from the skin of the upper eyelid and hanging downwards over the cheek [Fig. 1]. The lid margin was not involved. The conjunctiva was normal. The best corrected visual acuity was 20/30 N6 and 20/40 N8 in the right and left eyes respectively. Vision did not improve beyond that due to nuclear sclerosis and posterior subcapsular cataract. A small preauricular lymph node was palpable on the left side. Excision of the mass was done maintaining a margin of 8 mm around the tumor base to ensure adequate excision. There was loss of about three-fourths of the upper eyelid. Hence, for reconstruction a free tarsal graft was sourced from the right upper eyelid and sutured in position to the remnant of the tarsus on the excised eyelid of the left eye. The skin and orbicularis oculi muscle were undermined from the area above the eyelid and then advanced inferiorly to cover the tarsal graft. Postoperative appearance was cosmetically acceptable and there was neither lagophthalmos nor corneal exposure on closure of the eye. Histopathologically, features were of malignant melanoma (Clark′s level V, Breslow thickness 45 mm). Epithelioid and spindle tumor cells containing melanin pigment were seen with brisk mitoses (3 to 5 mitoses/high-power field) and junctional activity [Fig. 2]. There was no evidence of the nevus. Nontumorogenic radial growth phase was absent. Fine needle aspiration cytology of the preauricular lymph node showed metastatic melanoma. The patient was briefed about additional investigations for staging, further surgery and radiotherapy/chemotherapy as advised by the oncologist. He was not willing to undergo further treatment. Keeping in mind the poor prognosis for survival in melanoma with metastasis the patient was discharged after palliative surgery.
Figure 1.

Photograph showing the ulcerated tumor of the eyelid hanging on the cheek
Figure 2.
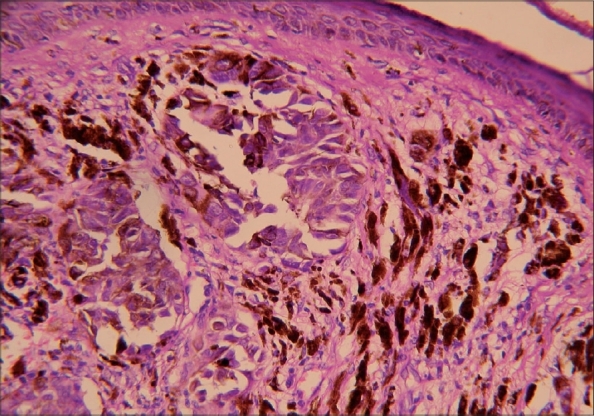
Histopathology showing skin with infiltrating melanin pigment containing epithelioid tumor cells (Hematoxylin and Eosin ×100)
Discussion
Melanoma of the eyelid accounts for less than 7% of head and neck region cutaneous melanomas.1 The majority are seen in the sixth to seventh decade of life. Either the upper or lower eyelid may be involved and predominantly it is of nodular type.1,3 To the best of our knowledge in the available literature, among the nodular melanomas the present case is the largest.1-3-6 The maximum size recorded is 40 × 42 mm but the type of melanoma is not mentioned.6 Among the different types of melanomas, lentigo maligna melanoma was among the largest tumors at presentation (750 mm2), which despite being thinner, was considered to be a greater surgical challenge.7 Melanoma of the eyelid skin has slightly better prognosis than its counterpart elsewhere. Though melanomas developing at the mucocutaneous lid margins were described to be at a greater risk of metastasis in one series,1 the same was not confirmed by the other.3 Simple thickness measurement is preferred to stage melanoma of the eyelid skin since the total dermis is exceptionally thin in this region and a Stage V melanoma on Clark′s scale would often be a much smaller lesion than such a lesion at other sites.7 The recommended treatment is complete surgical excision with a margin of normal skin to surround the tumor. A narrow excision margin of 5 mm or less is associated with a greater frequency of recurrence.7 Regional lymph node dissection in cases of completely excised cutaneous melanoma of head and neck did not result in increased survival, regardless of depth of tumor invasion.8
About 15 months later the patient presented with marked enlargement of the left preauricular metastatic lymph node. There was no local recurrence. Clinically, there was no evidence of metastatic disease at any other site. The patient refused further radiological investigations and treatment.
References
- 1.Garner A, Koorneef L, Levene A, Collin JR. Malignant melanoma of the eye lid skin: Histopathology and clinical behaviour. Br J Ophthalmol. 1985;69:180–6. doi: 10.1136/bjo.69.3.180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 2.Sunderraj P. Malignant tumours of the eye and adnexa. Indian J Ophthalmol. 1991;39:6–8. [PubMed] [Google Scholar]
- 3.Grossniclaus HE, McClean IW. Cutaneous melanoma of the eye lid-Clinicopathologic features. Ophthalmology. 1991;98:1867–73. doi: 10.1016/s0161-6420(91)32037-2. [DOI] [PubMed] [Google Scholar]
- 4.Tahery DP, Goldberg R, Moy RL. Malignant melanoma of the eyelid. J Am Acad Dermatol. 1992;27:17–21. doi: 10.1016/0190-9622(92)70148-9. [DOI] [PubMed] [Google Scholar]
- 5.Malhotra R, Chen C, Huilgol SC, Hill DC, Selva D. Mapped serial excision for perioricular lentigo maligna and lentigo maligna melanoma. Ophthalmology. 2003;110:2011–8. doi: 10.1016/S0161-6420(03)00670-5. [DOI] [PubMed] [Google Scholar]
- 6.Chan FM, O′Donnell , Whitehead K, Ryman W, Sullivan TJ. Treatments and outcomes of malignant melanoma of the eyelid a review of 29 cases in Australia. Ophthalmology. 2007;114:187–92. doi: 10.1016/j.ophtha.2006.08.043. [DOI] [PubMed] [Google Scholar]
- 7.Vaziri M, Buffam FV, Martinka M, Oryschak A, Dhaliwal H, White VA. Clinicopathologic features and behaviour of cutaneous eye lid melanoma. Ophthalmology. 2002;109:901–8. doi: 10.1016/s0161-6420(02)00962-4. [DOI] [PubMed] [Google Scholar]
- 8.Wanebo HJ, Cooper PH, Young DV, Harpole DH, Kaiser DL. Prognostic factors in head and neck melanoma: Effect of lesion location. Cancer. 1988;62:831–7. doi: 10.1002/1097-0142(19880815)62:4<831::aid-cncr2820620432>3.0.co;2-x. [DOI] [PubMed] [Google Scholar]