

Abstract
This section provides guidelines on medical therapy of patients with infectious keratitis. In addition to initial empirical therapy, preferred medications, once the organisms responsible are isolated, are discussed. Atypical mycobacterial keratitis following lasik is described. General guidelines for supportive therapy and follow-up, of these patients are presented. Clinical response to treatment and indications for intervention are discussed. Possible causes and approach to cases refractory to medical therapy are discussed.
Keywords: Infectious keratitis, medical therapy
Infectious keratitis is one of the major causes of avoidable blindness. Appropriate management could reduce the incidence of severe visual loss and restrict corneal damage. Delay in diagnosing the nature of infection is one of the paramount factors, which is responsible for inappropriate initial therapy. Standard guidelines, though available, are often not adhered to resulting in progressive ulceration. Emergence of drug resistance and availability of newer antimicrobials has made it essential for us to update our knowledge and change our treatment guidelines. This article attempts to provide current medical management options for infectious keratitis.
Management of Bacterial Ulcers
Bacterial keratitis should be treated as an ocular emergency due to its rapid progression and disastrous complications. Empirical antibiotic therapy should be promptly started and there are broadly two treatment options available [Table 1]. Commercially available fluoroquinolone monotherapy or a combination therapy of fortified antibiotics (cefazolin 5% and tobramycin or gentamicin 1.4%). The frequency of drops depends upon the severity, but it is usual to start half-hourly drops all through 24 h for most patients. A loading dose of a drop every 5 min for the first 30 min is used in severe ulcers. The frequency is reduced based on the clinical response.
Table 1.
Comparison of fluoroquinolones and fortified eye drops
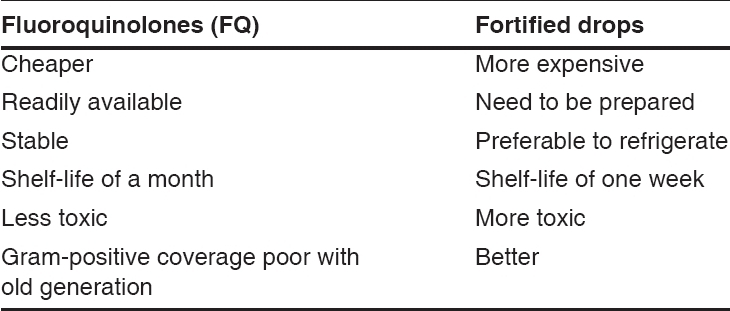
The aminoglycoside antibiotics used in fortified drops are gentamicin and tobramycin. They give an excellent Gram- negative coverage and are also active against staphylococci and some streptococci but not against pneumococci. They are however epitheliotoxic. Fortification is done by adding 80 mg/2 ml of antibiotic injection to 5 ml of commercially available antibiotic eye drops (0.3%) to get a concentration of 1.35%. The most commonly used cephalosporin in fortified drops is cefazolin. It gives good coverage for non-penicillinase producing Gram- positive bacteria. It is prepared by adding 5 ml of water for injection, to Injection Cefazolin 250 mg. The drops are refrigerated and should be discarded if they discolor to yellow or after a week, whichever is earlier.
Initial treatment of suspected cases of microbial keratitis with topical fortified antibiotics has long been the gold standard and the role for fluoroquinolone monotherapy continues to be debated, although studies have shown both treatment options to be comparable.1-4 Emerging resistance of Staphylococcus aureus,5-7 Streptococcal species5-7 and Pseudomonas8-9 to the earlier generation fluoroquinolones has raised concern over the use of monotherapy with these agents for suspected cases of bacterial keratitis. This is especially true given the high rates of microbial keratitis caused by Gram-positive organisms. Gatifloxacin and moxifloxacin [Table 2] demonstrate improved activity against Gram-positive pathogens, including Staphylococcus aureus and epidermidis and Streptococcus pneumoniae, as well as excellent activity against atypical pathogens such as atypical Mycobacteria, Mycoplasma, Legionella, Chlamydia and the anaerobic Propionibacterium acnes. The aqueous penetration of the newer quinolones is also significantly better. Aqueous penetration was highest for moxifloxacin followed by gatifloxacin and was lowest for ciprofloxacin.10
Table 2.
Empiric therapy - comparison of fluoroquinolones
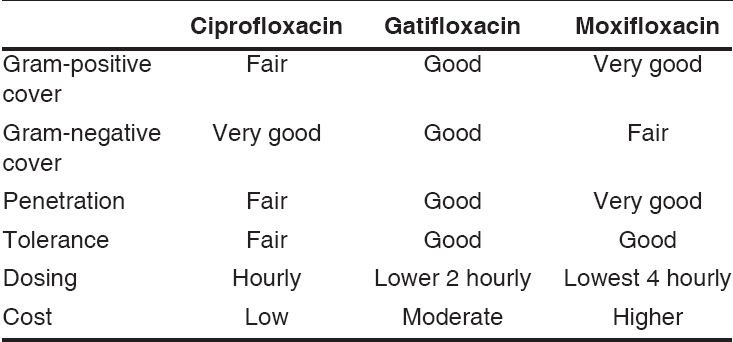
It remains to be seen whether the relative reduction in Gram-negative activity of these newer quinolones will allow monotherapeutic application for routine management of corneal ulcers. Moxifloxacin was shown to be comparable to ofloxacin and fortified antibiotics for treatment of bacterial keratitis in a recent study.11 Gatifloxacin has been shown to be superior to ciprofloxacin for management of bacterial keratitis.12 Gatifloxacin demonstrated a significantly better action than ciprofloxacin against Gram-positive cocci in vitro (P < 0.001) and the percentage of ulcers caused by these pathogens that healed in the gatifloxacin group was significantly better than in the ciprofloxacin group (P = 0.009). Mean time taken for healing of ulcer and the efficacy against Gram-negative bacteria did not significantly differ between the two groups. The authors suggest that gatifloxacin may be a preferred alternative to ciprofloxacin as the first-line monotherapy in bacterial keratitis.
Although controversial, it is the opinion of many authorities that results of Gram′s staining should not be used to alter the initial therapy started.13 It is recommended to initiate therapy with a broad-spectrum regimen14 and change it based on the clinical response and culture results.
Avascularity of cornea, as well as poor penetration of the drug in the stroma requires frequent application of topical antibiotics and is the basis for the loading dose concept. It is essential that minimum inhibitory concentration (MIC) of the drug be achieved at the site of infection. Drug concentrations achieved in the eye may be above the serum MIC levels and this may explain a good clinical response to an antibiotic to which the organism is not very sensitive in vitro. In these situations, a change in therapy is not warranted.15 In a nutshell, clinical response should be the first guideline of therapy, although in non-healing ulcer, in vitro sensitivity should be given due attention. It is also important that in vitro sensitivity should be correlated with in vivo response before considering change in therapy, as inadequate frequency, poor penetration, stromal lysis, and necrotic debris covering the site of infection can be the causes of non-responsiveness of ulcer to therapy.
Subconjunctival antibiotics16 are associated with pain, redness, patient apprehension, risk of globe perforation and failure to provide enhanced corneal levels of antibiotic compared to drops. They are no longer advisable for routine management of corneal infections. Oral or parenteral antibiotics have been shown to be of no benefit17 and are indicated only in ulcers with perforation, scleral involvement or endophthalmitis. Gonococcal infections require systemic ceftriaxone.
Other Antibiotics
Amikacin (40-100 mg/ml): It is useful for infections due to Gram-negative organisms resistant to tobramycin and gentamicin. It is also used in infections due to atypical mycobacteria and Nocardia.
Vancomycin (50 mg/ml): It is useful for Gram-positive infections including methicillin-resistant staphylococci. Empirical use is not recommended since it will escalate drug resistance.
Methicillin (50 mg/ml): It is useful for penicillinase producing Staphylococci.
Cotrimoxazole (Trimethoprim 16 mg/ml + sulfamethoxazole 80 mg/ml): It is recommended for Nocardia infections. The intravenous preparation is used directly as eye drops.
Anti-pseudomonas antibiotics: Piperacillin (7 mg/ml), ceftazidime (50 mg/ml), cefoperazone and imipenem may be used in multidrug-resistant infections.
Clarithromycin (10-40 mg/ml): Useful in atypical mycobacterial infections.
Atypical Mycobacterial Infections and Post-lasik Infectious Keratitis
Atypical mycobacterial infections are being seen and diagnosed more often because of more awareness and better microbiology techniques. Though they have been seen in patients of infectious keratitis and in post-cataract wound infections, the clusters of mycobacterial outbreaks following lasik have been more serious. All cases of suspected infectious keratitis following lasik require a flap lift and microbiologic evaluation.
The traditional drug of choice for the treatment of mycobacterial keratitis has been the aminoglycoside amikacin. However, the non-response rate to amikacin may be as high as 60%, likely due to poor penetration through intact epithelium. Ciprofloxacin could be used for isolates resistant to amikacin. In vitro data suggests that M. fortuitum is more sensitive to amikacin and ciprofloxacin than M. chelonae.18 Another report suggested good in vitro antimicrobial activity of amikacin, clarithromycin, imipenem and ciprofloxacin against M. chelonae. However, no synergistic effects were demonstrated for combinations of an aminoglycoside with other effective drugs.19 Though the fourth generation quinolones are known to be effective, a change in sensitivity patterns has also to be kept in mind. Seventeen out of 18 mycobacterial isolates (3 M. abscessus and 14 M. chelonae) recovered from post-lasik infectious keratitis cases in Brazil were resistant to ciprofloxacin, ofloxacin, gatifloxacin and moxifloxacin.20 Topical and oral macrolides, such as clarithromycin (10-40 mg/ml) and azithromycin (2 mg/ml) are also effective in these cases.21,22
Steroids may yield an initial clinical improvement, but the overall course is worsened due to suppression of cell-mediated immunity, an integral part of combating mycobacterial disease.21
Despite intensive topical treatment, post-lasik mycobacterial keratitis frequently does not respond to medical therapy. Poor drug penetration and sequestration of the organism frequently necessitate flap amputation. Penetrating keratoplasty may also be required for extirpation of the organism or for visual rehabilitation.
Supportive Therapy and Follow-up for Corneal Infections
All patients require frequent and close observation until they start responding to treatment. Admission to hospital is advisable for patients where compliance with medical therapy or follow-up is an issue. Cycloplegics, antiglaucoma medications, and analgesics are used as required. Corticosteroids as anti-inflammatory are best avoided, until the infection is completely eradicated or under control. Non-steroidal anti-inflammatory drugs are also better to avoid in patients with corneal ulceration due to the risk of corneal melting and perforation.
Signs of improvement are:
Stabilization and no progression
Reduced activity at infiltrate margins/blunting of ulcer edges
Reduction in adjacent stromal inflammatory reaction and anterior chamber inflammation
Resolution of infiltration and progressive healing of epithelial defect.
If a patient with negative scrape report continues to worsen, non-infectious ulcers or infections due to other organisms must be considered. A corneal biopsy may help in deep-seated infections where a surface scrape is likely to be negative.
Progressive corneal thinning or perforations less than 2 mm can be managed with cyanoacrylate tissue adhesive and bandage contact lens application. Larger perforations require a therapeutic penetrating keratoplasty. Conjunctival flaps may help selected cases of refractory ulceration.
Management of Fungal Ulcers
Natamycin 5% suspension is the first choice for treatment of filamentous fungal keratitis23[Table 3]. Surface debridement helps to remove slough and reduce load of infection. It also enhances the drug penetration. Drops are used every half to one hourly initially and tapered as per the clinical response. Response to treatment in fungal infections is very slow and complete resolution often may require 4-8 weeks of treatment.
Table 3.
Antifungals for fungal corneal ulcers
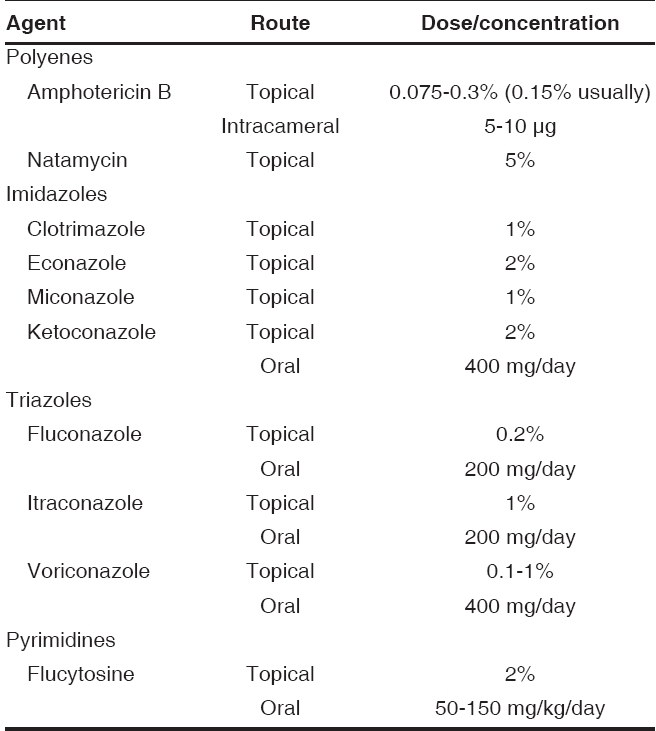
Amphotericin B is particularly effective against yeasts but less effective against filamentous fungi; it is therefore the first agent of choice against yeasts. Amphotericin B (0.15%) drops can be considered alone or in combination with natamycin in refractory cases; however, their penetration through an intact epithelium is less than natamycin.24 Intracameral 5-10 µg amphotericin B has also been used25 successfully in patients refractory to topical and oral antifungals. Amphotericin B is available as a 50-mg injection. Drops are prepared by adding 10 ml water for injection to the vial to get a stock solution (5 mg/ml). 3.5 ml of water for injection is added to 1.5 ml of this stock solution to get 5 ml of 0.15% drops, which can be dispensed. The drops should be refrigerated and should not be exposed to light. The drops should be inspected at each visit for any turbidity, which may indicate contamination or drug precipitation.
The azoles and fluocytosine are generally employed as alternative agents for advanced ulcers or for ulcers not responding to polyenes. Experimental models suggest an antagonism26 between amphotericin B and imidazoles and some do not recommend this combination, although clinical evidence has been contradictory. Topically applied, the imidazoles have poor corneal penetration, and so they are more effective in treating superficial infections especially due to Aspergillus. Topical itraconazole 1%, clotrimazole 1%, ketoconazole 2%, econazole 2%, and miconazole 1% have also been used for fungal keratitis. A study showed that 2% econazole was as effective as natamycin 5%;27 however, the concurrent use of 5% natamycin and 2% econazole28 did not offer additional benefits over monotherapy with 5% natamycin alone for the management of fungal keratitis. Natamycin 5% has been shown to be superior to itraconazole 2%29 for filamentous fungal keratitis. Fluconazole has high corneal penetration and reaches therapeutic corneal levels when given orally. It is effective against Candida and also useful against Aspergillus. Its clinical role in filamentous fungal keratitis is yet to be precisely defined; however, it could be considered in patients with deep fungal keratitis.
Patients, with deep infiltrates, with exudates in the anterior chamber, are often refractory to medical therapy. Oral itraconazole 100 mg twice daily or ketoconazole 200 mg twice daily can be added in these cases. Liver function tests need to be done before and during the treatment.
Voriconazole has the broadest spectrum of the azole antifungals and has good intraocular penetration after oral administration.30 Voriconazole is a new, promising therapy for fungal keratitis that is refractory to standard antifungal agents. It is used orally 200 mg twice daily and as drops (0.1-1%).31,32
Newer agents33 such as triazoles (posaconazole and ravuconazole), echinocandins, sodarin derivatives and the nikkomycins might improve the treatment of fungal keratitis in future.
In vitro E-test34 for assessing antifungal drug susceptibility may provide information for choosing antifungal agents to treat fungal keratitis.
Supportive Therapy and Follow-up
This would be similar to bacterial ulcers as mentioned earlier. Corticosteroids are contraindicated in fungal keratitis. About 20% of fungal ulcers are refractory to medical therapy35 and continue to worsen despite maximal medical therapy. This may be due to the deeper penetration of fungal filaments, poor drug penetration or drug resistance. This subset of patients needs to be identified early and should undergo an early therapeutic penetrating keratoplasty. Delay in surgery often leads to scleral involvement, endophthalmitis and eventual loss of the eye.
Management of Acanthamoeba Keratitis
It is difficult to diagnose and treat Acanthamoeba keratitis. Chlorhexidine and polyhexamethylene biguanide (PHMB) are the most effective36,37 against trophozoites and cysts and are recommended as the first line of therapy [Table 4]. These drops are commercially not available; however, they can be obtained in India from tertiary care ophthalmic institutes on request. Medications have to be used for a long time after clinical resolution of infection to prevent relapses. This is because of the drugs being less effective against the cystic forms. Routine use of topical steroids38 is controversial though its use has been recommended specifically for limbitis, scleritis, and uveitis.
Table 4.
Antiamoebics for keratitis

Management of Microsporidiosis
Fumagillin39-41 10 mg/ml suspension is very effective in microsporidial keratoconjunctivitis. In refractory cases oral albendazole,42 oral itraconazole43 has been used successfully. Propamidine drops have also been used in some cases.
Management of Viral Infections
We shall restrict our discussion to management of Herpes simplex and Herpes zoster infections.
Herpes Simplex virus keratitis
Dendritic epithelial disease without stromal involvement
Infected epithelial cells are debrided with a sterile cotton tipped applicator and acyclovir 3% eye ointment is started five times a day. Antivirals are used for 2-3 weeks. Topical steroids are contraindicated in infectious epithelial disease.
Epithelial trophic ulceration (metaherpetic)
Intensive lubrication with preservative-free tear substitutes is usually successful in these patients. Antivirals have no role. Steroids and non-steroidal anti-inflammatory medications are best avoided in the presence of an epithelial defect. However, in the presence of stromal inflammation, diluted steroids could be used with extreme caution. Bandage contact lenses and amniotic membrane grafting could also be tried in refractory cases. Severe cases may require a tarsorrhaphy or a conjunctival flap. In the presence of progressive stromal melting or a small perforation, cyanoacrylate tissue adhesive is useful and allows one to postpone a therapeutic keratoplasty in an inflamed eye.
Stromal keratitis
The herpetic eye disease study (HEDS) concluded that a combination of topical steroids and antivirals reduces the persistence or progression of stromal inflammation and shortens the duration of stromal keratitis.33 Additional use of oral acyclovir was found to be of no benefit.45 Steroids once started need to be tapered very slowly and under observation for recurrent inflammation.
Trabeculitis and iridocyclitis
Topical steroid and antiviral combination is recommended. HEDS also recommends additional oral acyclovir for iridocyclitis.46
Recurrent ocular disease and oral prophylaxis
The HEDS study conclusively proved that oral acyclovir 400 mg twice daily reduces the recurrence of herpetic eye disease.47 This should be considered in patients at risk of visual loss due to repeated HSV stromal keratitis.
Herpes zoster
Herpes zoster ophthalmicus (HZO) should be treated with oral acyclovir 800 mg five times a day for 7-10 days, ideally initiated within 72 h of the onset of symptoms.
Newer antivirals can also be used for HZO. Famciclovir is more bioavailable when given orally than acyclovir and its active metabolite penciclovir triphosphate has an intracellular half-life nearly 10 times that of acyclovir. Recommended dosage is 500 mg/day for 7 days. Valacyclovir is a prodrug of acyclovir that is more bioavailable orally. It achieves three times higher plasma levels comparable to those achieved with intravenous acyclovir.48 Recommended dose is 1000 mg three times a day for 7-10 days. Both famciclovir and valacyclovir appear to be superior to acyclovir in reducing the duration of zoster-associated pain.49
Systemic corticosteroids reduce pain and improve patient functioning. However, they carry the risk of causing disseminated viral infection especially in the immunocompromised and should be used with caution.
Topical steroids are useful for reducing corneal and scleral inflammation and iridocyclitis. Topical antivirals are usually not employed for zoster keratitis.
Neurotrophic ulceration is a major complication of HZO. Preservative-free lubricants, bandage contact lens, tarsorrhaphy, amniotic membrane grafts, and conjunctival flaps may be required to treat these patients. Severe thinning or perforation may require cyanoacrylate tissue adhesive or a therapeutic keratoplasty.
Approach to Non-healing Infectious Corneal Ulcers
Any corneal ulcer not responding to appropriate treatment over a period of 2-3 weeks could be labeled as a non-healing ulcer. It could be infectious, sterile, immune mediated or due to a combination of these processes. There could be associated ocular or systemic problems contributing to the ulcerative process.
Wrong Line of Therapy
It is not unusual to see fungal ulcers being treated as bacterial and vice versa. This is because it is often difficult for ophthalmologists to distinguish the nature of infection clinically and due to our inertia (rather than a lack of facilities) that stops us from doing microbial work-up. Wrong or negative microbiology reports, due to various reasons, also complicate the situation. Improving clinical skills and using proper microbiologic techniques can improve management of corneal ulcers. Referral to centers equipped with a cornea specialist and good laboratory support in refractory cases is advisable.
Inadequate therapy
Despite correctly diagnosing the nature of infection, a wrong choice of antimicrobial drops or an inadequate frequency of use could also cause a lack of expected improvement. Poor drug penetration could also be an important cause of poor response. Routine use of combination therapies to encompass multiple organisms should be avoided, as it not only reduces clinical efficacy but also increases toxicity.
Drug resistance
Increasing resistance of micro-organisms to antimicrobials is being reported worldwide. In hospital-acquired infections, infections in hospital personnel and infections in eyes with chronic ocular surface disease, resistant Gram-negative and methicillin-resistant staphylococci are known to cause keratitis. Empiric use of higher generation antimicrobials in these situations may be warranted. Microbiologic evaluation and in vitro sensitivity data are a must and help to guide therapy. Similarly, fungal ulcers are often refractory to all available antifungals. In these situations, an early therapeutic keratoplasty is the only eye-saving option.
Toxicity
Continued aggressive antimicrobial therapy even after the infection has responded could be a cause of non-healing after the initial favorable response. Drug toxicity could by itself delay epithelization and cause more stromal thinning.
All patients with non-healing ulcers need to be re-evaluated to check for corneal sensations, tear film problems, lid and lash problems and missed foreign body. A systemic work-up is indicated in patients with sterile corneal melting to rule out collagen disease.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.O′Brien TP, Maguire MG, Fink NE, Alfonso E, McDonnell P. Efficacy of ofloxacin versus cefazolin and tobramycin in the therapy for bacterial keratitis: Report from the Bacterial Keratitis Study Research Group. Arch Ophthalmol. 1995;113:1257–65. doi: 10.1001/archopht.1995.01100100045026. [DOI] [PubMed] [Google Scholar]
- 2.Hyndiuk RA, Eiferman RA, Caldwell DR, Rosenwaser GO, Santos CI, Katz HR, et al. Comparison of ciprofloxacin ophthalmic solution 0.3% to fortified tobramycin-cefazolin in treating bacterial corneal ulcers. Comparison of ciprofloxacin ophthalmic solution 0.3% to fortified tobramycin-cefazolin in treating bacterial corneal ulcers. Ophthalmology. 1996;103:1854–62. doi: 10.1016/s0161-6420(96)30416-8. [DOI] [PubMed] [Google Scholar]
- 3.The Ofloxacin Study Group. Ofloxacin montherapy for the primary treatment of microbial keratitis: A double-masked, randomized, controlled trial with conventional dual therapy. Ophthalmology. 1997;104:1902–9. [PubMed] [Google Scholar]
- 4.Panda A, Ahuja R, Sastry SS. Comparison of topical 0.3% ofloxacin with fortified tobramycin plus cefazolin in the treatment of bacterial keratitis. Eye. 1999;13:744–77. doi: 10.1038/eye.1999.220. [DOI] [PubMed] [Google Scholar]
- 5.Goldstein MH, Kowalski RP, Gordon YJ. Emerging fluoroquinolone resistance in bacterial keratitis: A 5-year review. Ophthalmology. 1999;106:1313–8. [PubMed] [Google Scholar]
- 6.Alexandrakis G, Alfonso EC, Miller D. Shifting trends in bacterial keratitis in South Florida and emerging resistance to fluoroquinolones. Ophthalmology. 2000;107:1497–502. doi: 10.1016/s0161-6420(00)00179-2. [DOI] [PubMed] [Google Scholar]
- 7.Knauf HP, Silvany R, Southern PM, Jr, Knauf HP, Silvany R, Southern PM, Jr, et al. Susceptibility of corneal and conjunctival pathogens to ciprofloxacin. Cornea. 1996;15:66–71. [PubMed] [Google Scholar]
- 8.Garg P, Sharma S, Rao GN. Ciprofloxacin resistant Pseudomonas keratitits. Ophthalmology. 1999;106:1319–23. doi: 10.1016/S0161-6420(99)00717-4. [DOI] [PubMed] [Google Scholar]
- 9.Kunimoto DY, Sharma S, Garg P, Rao GN. In vitro susceptibility of bacterial keratitis pathogens to ciprofloxacin: Emerging resistance. Ophthalmology. 1999;106:80–5. doi: 10.1016/S0161-6420(99)90008-8. [DOI] [PubMed] [Google Scholar]
- 10.Solomon R, Donnenfeld ED, Perry HD, Snyder RW, Nedrud C, Stein J, et al. Penetration of topically applied Gatifloxacin 0.3%, Moxifloxacin 0.5% and Ciprofloxacin 0.3% into the aqueous humor. Ophthalmology. 2005;112:466–9. doi: 10.1016/j.ophtha.2004.09.029. [DOI] [PubMed] [Google Scholar]
- 11.Constantinou M, Daniell M, Snibson GR, Vu HT, Taylor HR. Clinical efficacy of Moxifloxacin in the treatment of bacterial keratitis. Ophthalomolgy. 2007;114:1622–9. doi: 10.1016/j.ophtha.2006.12.011. [DOI] [PubMed] [Google Scholar]
- 12.Parmar P, Salman A, Kalavathy CM, Kaliamurthy J, Prasanth DA, Thomas PA, et al. Comparison of topical Gatifloxacin 0.3% and Ciprofloxacin 0.3% for the treatment of bacterial keratitis. Am J Ophthalmol. 2006;141:282. doi: 10.1016/j.ajo.2005.08.081. [DOI] [PubMed] [Google Scholar]
- 13.Arffa RC. Grayson′s diseases of the cornea. St. Louis: Mosby Year Book; 1991. Infectious ulcerative keratitis: Bacterial; pp. 163–98. [Google Scholar]
- 14.McLeod SD, LaBree LD, Tayyanipour R, Flowers CW, Lee PP, McDonnell PJ. The importance of initial management in the treatment of severe infectious corneal ulcers. Ophthalmology. 1995;102:1943–8. doi: 10.1016/s0161-6420(95)30771-3. [DOI] [PubMed] [Google Scholar]
- 15.Ormerod LD, Heseltine PN, Alfonso E, Becker MI, Kenyon KR, Baerveldt G, et al. Gentamicin resistant pseudomonal infection: Rationale for a redefinition of ophthalmic antimicrobial sensitivities. Cornea. 1989;8:195–9. [PubMed] [Google Scholar]
- 16.Baum J, Barza M. Topical vs subconjunctival treatment of bacterial corneal ulcers. Ophthalmology. 1979;87:710–6. doi: 10.1016/s0161-6420(83)34583-8. [DOI] [PubMed] [Google Scholar]
- 17.Davis SD, Sarff LD, Hyndiuk RA. Comparison of therapeutic routes in experimental Pseudomonas keratiits. Am J Ophthalmol. 1979;87:710–6. doi: 10.1016/0002-9394(79)90309-x. [DOI] [PubMed] [Google Scholar]
- 18.Hu FR, Luh KT. Topical ciprofloxacin for treating nontuberculous mycobacterial keratitis. Ophthalmology. 1998;105:269–72. doi: 10.1016/s0161-6420(98)80018-3. [DOI] [PubMed] [Google Scholar]
- 19.Hu FR, Chang SC, Luh KT, Hung PT. The antimicrobial susceptibility of Mycobacterium chelonae isolated from corneal ulcer. Curr Eye Res. 1997;16:1056–60. doi: 10.1076/ceyr.16.10.1056.9023. [DOI] [PubMed] [Google Scholar]
- 20.Hofling-Lima AL, de Freitas D, Sampaio JL, Leao SC, Contarini P. In vitro activity of fluoroquinolones against Mycobacterium abscessus and Mycobacterium chelonae causing infectious keratitis after LASIK in Brazil. Cornea. 2005;24:730–4. doi: 10.1097/01.ico.0000154411.07315.0a. [DOI] [PubMed] [Google Scholar]
- 21.Ford JG, Huang AJ, Pflugfelder SC, Alfonso EC, Forster RK, Miller D. Nontuberculous mycobacterial keratitis in South Florida. Ophthalmology. 1998;105:1652–8. doi: 10.1016/S0161-6420(98)99034-0. [DOI] [PubMed] [Google Scholar]
- 22.Chandra NS, Torres MF, Winthrop KL, Bruckner DA, Heidemann DG, Calvet HM, et al. Cluster of Mycobacterium chelonae keratitis cases following laser in-situ keratomileusis. Am J Ophthal. 2001;132:819–30. doi: 10.1016/s0002-9394(01)01267-3. [DOI] [PubMed] [Google Scholar]
- 23.O′Day DM, Robinson RD, Head WS. Efficacy of anti-fungal agents in the cornea, I: A comparative study. Invest Ophthalmol Vis Sci. 1983;24:1098–102. [PubMed] [Google Scholar]
- 24.O′Day DM, Head WS, Robinson RD, Clanton JA. Corneal penetration of topical amphotericin B and natamycin. Curr Eye Res. 1986;5:877–82. doi: 10.3109/02713688609029240. [DOI] [PubMed] [Google Scholar]
- 25.Kaushik S, Ram J, Brar GS, Jain AK, Chakraborti A, Gupta A. Intracameral amphotericn B: Initial experience in severe keratomycosis. Cornea. 2001;20:715–9. doi: 10.1097/00003226-200110000-00009. [DOI] [PubMed] [Google Scholar]
- 26.Brajtburg J, Kobayashi D, Medoff G, Kobayashi GS. Antifungal action of amphoteracin B in combination with other polyene or imidazole antibiotics. J Infect Dis. 1982;146:138–46. doi: 10.1093/infdis/146.2.138. [DOI] [PubMed] [Google Scholar]
- 27.Prajna NV, John RK, Nirmalan PK, Lalitha P, Srinivasan M. A randomised clinical trial comparing 2% econazole and 5% natamycin for the treatment of fungal keratitis. Br J Ophthalmol. 2003;87:1235–7. doi: 10.1136/bjo.87.10.1235. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Prajna NV, Nirmalan PK, Mahalakshmi R, Lalitha P, Srinivasan M. Concurrent use of 5% natamycin and 2% econazole for the management of fungal keratitis. Cornea. 2004;23:793–6. doi: 10.1097/01.ico.0000134193.64357.82. [DOI] [PubMed] [Google Scholar]
- 29.Kalavathy CM, Parmar P, Kaliamurthy J, Philip VR, Ramalingam MD, Jesudasan CA, et al. Comparison of topical itraconazole 1% with topical natamycin 5% for the treatment of filamentous fungal keratitis. Cornea. 2005;24:449–52. doi: 10.1097/01.ico.0000151539.92865.3e. [DOI] [PubMed] [Google Scholar]
- 30.Haripasad SM, Mieler WF, Holz ER, Gao H, Kim JE, Chi J, et al. Determination of vitreous, aqueous and plasma concentration of orally administered voriconazole in humans. Arch Ophthalmol. 2004;122:42–7. doi: 10.1001/archopht.122.1.42. [DOI] [PubMed] [Google Scholar]
- 31.Bunya VY, Hammersmith KM, Rapuano CJ, Ayres BD, Cohen EJ. Topical and oral voriconazole in the treatment of fungal keratitis. Am J Ophthalmol. 2007;143:151–3. doi: 10.1016/j.ajo.2006.07.033. [DOI] [PubMed] [Google Scholar]
- 32.Jhanji V, Sharma N, Mannan R, Titiyal JS, Vajpayee RB. Management of tunnel fungal infection with voriconazole. J Cataract Refract Surg. 2007;33:915–7. doi: 10.1016/j.jcrs.2006.12.026. [DOI] [PubMed] [Google Scholar]
- 33.Ernst EJ. Investigational antifungal agents. Pharmacotherapy. 2001;21:165S–74S. doi: 10.1592/phco.21.12.165s.34509. [DOI] [PubMed] [Google Scholar]
- 34.Qiu WY, Yao YF, Zhu YF, Zhang YM, Zhou P, Jin YQ, et al. Fungal spectrum identified by a new slide culture and in vitro drug susceptibility using Etest in fungal keratitis. Curr Eye Res. 2005;30:1113–20. doi: 10.1080/02713680500423671. [DOI] [PubMed] [Google Scholar]
- 35.Forster RK, Rebell G. Therapeutic surgery in failures of medical treatment for fungal keratitis. Br J Ophthalmol. 1975;59:366–71. doi: 10.1136/bjo.59.7.366. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Elder MJ, Kilvington S, Dart JK. A clinicopathologic study of in vitro sensitivity testing and Acanthamoeba keratitis. Invest Ophthalmol Vis Sci. 1994;35:1059–64. [PubMed] [Google Scholar]
- 37.Hay J, Kirkness CM, Seal DV, Wright P. Drug resistance and acanthamoeba keratitis: the quest for alternative antiprotozoal chemotherapy. Eye. 1994;8:555–63. doi: 10.1038/eye.1994.137. [DOI] [PubMed] [Google Scholar]
- 38.Bacon AS, Frazer DG, Dart JK, Matheson M, Ficker LA, Wright P. A review of 72 consecutive cases of Acanthamoeba keratitis. Eye. 1993;7:719–25. doi: 10.1038/eye.1993.168. [DOI] [PubMed] [Google Scholar]
- 39.Theng J, Chan C, Ling ML. Microsporidial keratoconjunctivitis in a healthy contact lens wearer without human immunodeficiency virus infection. Ophthalmology. 2001;108:976–8. doi: 10.1016/s0161-6420(01)00542-5. [DOI] [PubMed] [Google Scholar]
- 40.Wilkins JH, Joshi N, Margolis TP, Cevallos V, Dawson CR. Microsporidial keratoconjunctivitis treated successfully with a short course of topical fumagillin. Eye. 1994;8:703–4. doi: 10.1038/eye.1994.177. [DOI] [PubMed] [Google Scholar]
- 41.Roseberger DF, Serderavic ON, Erlandson RA, Bryan RT, Schwartz DA, Visvesvara GS, et al. Successful treatment of microsporidial keratoconjunctivitis with topical fumagillin in a patient with AIDS. Cornea. 1993;12:261–5. doi: 10.1097/00003226-199305000-00013. [DOI] [PubMed] [Google Scholar]
- 42.Gritz DC, Holsclaw DS, Neger RE. Ocular and sinus microsporidial infection cured with systemic albendazole. Am J Ophthalmol. 1997;124:241–3. doi: 10.1016/s0002-9394(14)70792-5. [DOI] [PubMed] [Google Scholar]
- 43.Rossi P, Urbani C, Donelli G. Resolution of microsporidial sinusitis and keratoconjunctivitis by itraconazole treatment. Am J Ophthalmol. 1999;127:210–2. doi: 10.1016/s0002-9394(98)00352-3. [DOI] [PubMed] [Google Scholar]
- 44.Wilhelmus KR, Gee L, Hauck WW, Kurinij N, Dawson CR, Jones DB, et al. Herpetic eye disease study: A controlled trial of topical corticosteroids for herpes simplex stromal keratitis. Ophthalmology. 1994;101:1883–96. doi: 10.1016/s0161-6420(94)31087-6. [DOI] [PubMed] [Google Scholar]
- 45.Barron BA, Gee I, Hauck WW, Kurinij N, Dawson CR, Jones DB, et al. Herpetic eye disease study: A controlled trial of oral acyclovir for herpes simplex stromal keratitis. Ophthalmology. 1994;101:1871–82. doi: 10.1016/s0161-6420(13)31155-5. [DOI] [PubMed] [Google Scholar]
- 46.The herpetic eye disease study group. A controlled trial of oral acyclovir for iridocyclitis caused by herpes simplex virus. Arch Ophthalmol. 1996;114:1065–72. doi: 10.1001/archopht.1996.01100140267002. [DOI] [PubMed] [Google Scholar]
- 47.The herpetic eye disease study group. Acyclovir for the prevention of recurrent herpes simplex virus eye disease. N Engl J Med. 1998;339:300–6. doi: 10.1056/NEJM199807303390503. [DOI] [PubMed] [Google Scholar]
- 48.Beutner KR. Valacyclovir: A review of its antiviral activity, pharmacokinetic properties and clinical efficacy. Antiviral Res. 1995;28:281–90. doi: 10.1016/0166-3542(95)00066-6. [DOI] [PubMed] [Google Scholar]
- 49.Kost RG, Straus SE. Postherpetic neuralgia-pathogenesis, treatment and prevention. N Engl J Med. 1996;335:32–42. doi: 10.1056/NEJM199607043350107. [DOI] [PubMed] [Google Scholar]