

Abstract
India has a large number of patients with acquired immune deficiency syndrome (AIDS), the third largest population of this group in the world. This disease was first described in patients with Pneumocystis pneumonia in 1981. Ocular lesions can occur at any stage of the disease but are more commonly seen at the late stages. Human immunodeficiency virus (HIV), the causative agent of AIDS is a retrovirus with RNA genome and a unique ′Reverse transcriptase enzyme′ and is of two types, HIV-1 and 2. Most human diseases are caused by HIV-1. The HIV-1 subtypes prevalent in India are A, B and C. They act predominantly by reducing the CD4+ cells and thus the patient becomes susceptible to opportunistic infections. High viral titers in the peripheral blood during primary infection lead to decrease in the number of CD4+ T lymphocytes. Onset of HIV-1-specific cellular immune response with synthesis of HIV-1 specific antibodies leads to the decline of plasma viral load and chronification of HIV-1 infection. However, the asymptomatic stage of infection may lead to persistent viral replication and a rapid turnover of plasma virions which is the clinical latency. During this period, there is further decrease in the CD4+ counts which makes the patient′s immune system incapable of controlling opportunistic pathogens and thus life-threatening AIDS-defining diseases emerge. Advent of highly active antiretroviral treatment (HAART) has revolutionized the management of AIDS though there is associated increased development of immune recovery uveitis in a few of these patients.
Keywords: Acquired immuno deficiency syndrome, CD4 cells, CD8 cells, CXCR4, highly active antiretroviral therapy, CCR5, human immune deficiency virus, immune recovery uveitis
Since the report of an unusual occurrence of Pneumocystic carinii pneumonia in five cases on June 5, 1981 by Dr. Gotlieb and his colleagues - ′Pneumocystis pneumonia - Los Angeles′ Fascicle in the Bulletin of Morbidity and Mortality Weekly Report (MMWR),1 which was the first publication on this dreaded infection, there have been numerous studies and case reports pertaining to this disease. Nobody imagined that this was the first glimpse of a global pandemic that would threaten the very existence of much of the globe. Twenty-five years later, the human immunodeficiency virus (HIV), the causative agent of acquired immune deficiency syndrome (AIDS) has reached virtually every corner of the globe infecting more than 65 million till date. There are about 14,000 new HIV infections occurring globally each day, of which more than 95% are in developing countries. Eighty per cent are due to heterosexual transmission and about 12,000 are in persons aged 15 to 49 years (50% are women and about 50% are 15 to 24-year-old). Of these, 25 millions have already died.1
India has a large number of patients with AIDS, the third largest population of this group in the world. Human immunodeficiency virus was first identified in India in 1986 in prostitutes in Chennai and later in intravenous (IV) drug abusers in Manipur. Currently, there are about 2.5 million HIV-infected people in India.2 Ocular lesions associated with AIDS were first reported3 in India in 1995 and a series of 100 consecutive patients4 in India was reported in 2000, both from Sankara Nethralaya, Chennai. Since then, there have been several other reports from different parts of India of ocular lesions due to AIDS and we have recently reported the manifestations of ocular tuberculosis in AIDS.5
Progress has been probably far greater in this field than any other area of medicine in recent years and the lessons learnt from HIV research have broad applications to other fields of medicine. The lifetime cumulative risk of developing at least one abnormal ocular lesion for a HIV-positive person ranges from 52-100% in various studies.6 Ocular lesions usually occur in the late phase of HIV infection but can also be an early manifestation of the disease.
The predominant site of action of the virus is on the viral reverse transcriptase enzyme and the cell of action is the CD4 cell. We describe the immunology and pathogenesis of the virus leading to disease.
History
There have been many historical events in the evolution of AIDS and its treatment.
1981: Epidemic first identified
1982: The term ″AIDS″ first coined
1983: Identification of the HIV virus
1985: First commercial test to detect HIV
1987: First antiretroviral drug released (Zidovudine-AZT)
1991: 2nd and 3rd anti-retrovirals (ARVs) released (Didanosine- DDI, Zalcitabine-DDC)
1995: First protease inhibitor released (Saquinavir)
1998: Three-drug therapy (Highly active antiretroviral therapy-HAART) shown to delay sickness and death
1998: First non-nucleoside inhibitor released
The treatment of any patient with AIDS involves
Inhibiting the replication of the virus using antiretroviral drugs
Treatment of opportunistic infections
Psychosocial support
Immunology
Causative agent7
Human immunodeficiency virus is a human retrovirus with RNA genome and a unique ′Reverse transcriptase enzyme′ and is of two types, HIV-1 and HIV-2. Most human diseases are caused by HIV-1. The HIV-1 subtypes prevalent in India are A, B and C.
The virus (Virion) is 120 nm in diameter consisting of an outer envelope, a core shell of protein and a cone-shaped inner core containing RNA genome, ′Reverse transcriptase′ enzyme and core polypeptides [Figure 1]; HIV-2, on the other hand, is known to have a milder and slower effect on the immune system. People who have AIDS-like symptoms but test negative for HIV-1 should be tested for HIV-2.
Figure 1.
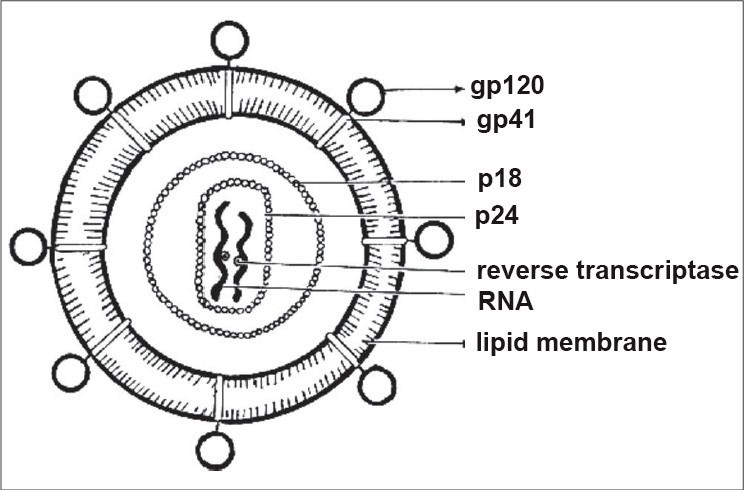
Schematic diagram of a human immunodeficiency virus
CD4 cells8
T lymphocytes, or Thymus derived cells, compose 65-80% of the peripheral blood lymphocyte population, 30-50% of the splenocyte population, and 70-85% of the lymph node cell population. B lymphocytes compose 5-15% of peripheral blood lymphocytes, 20-30% of splenocytes and 10-20% of lymph node cells.
Both B cells and T cells can be further subdivided into specialized subsets; B cells into those that synthesize five separate classes of immunoglobulins and T cells into helper (CD4) and cytotoxic (CD8) cells. Helper (CD4) T cells ″help″ in the induction of an immune response, in the generation of an antibody response and in the generation of other, more specialized components of the immune response. Cytotoxic (CD8) T cells, as the name implies, are involved in cell killing or cytotoxic reactions. Delayed type hypersensitivity (CD4) T cells are the classic participants in the chronic inflammatory responses characteristic of certain antigens such as mycobacteria. Regulatory (CD8) T cells are responsible for modulating immune responses, thereby preventing uncontrolled, host-damaging inflammatory responses.
Mosmann and Coffman9 described two types of helper (CD4) T cells with differential cytokine production profiles. These CD4 and CD8 cells are the cells predominantly affected in HIV infections. Normal CD4 counts are between 300 to 1000 cells/cu mm.
Correlation of CD4 cell count and HIV-associated ocular disease.
| CD4 count (cells/cu.mm) | Disease |
| 1000 | Normal |
| < 500 | Kaposi sarcoma |
| < 500 | Kaposi sarcoma |
| Lymphoma | |
| Tuberculosis | |
| < 250 | Pneumocystosis |
| Toxoplasmosis | |
| Retinal/conj microvasculopathy | |
| < 100 | Keratoconjunctivitis sicca |
| Varicella zoster virus retinitis | |
| Cytomegalovirus retinitis |
Course of HIV infection10
In approximately 50% of cases, primary HIV-1 infection remains asymptomatic,8 whereas 50% of the patients develop flu-like symptoms within the first four weeks after infection. During primary infection, virus titers are extremely high in peripheral blood (up to 108 HIV-1 RNA copies/ml plasma) and the number of CD4+ T lymphocytes decreases significantly. The onset of HIV-1-specific cellular immune response and the subsequent synthesis of HIV-1-specific antibodies lead to the decline of plasma viral load to a patient-specific level and chronification of HIV-1 infection. However, the asymptomatic stage of the infection is accompanied by persistent viral replication in lymph nodes and a rapid turnover of plasma virions and CD4+ T lymphocytes, called the ″clinical latency″. During the course of clinical latency, the number of CD4+ T lymphocytes decreases continuously. As a consequence the patient′s immune system is no more capable of controlling opportunistic pathogens and life-threatening AIDS-defining diseases emerge. The different stages of HIV-1 infection are commonly classified using the center for disease control (CDC) system. This system combines clinical data and the number of CD4+ T lymphocytes for HIV-1 infection classification.
Pathogenesis
The main steps in the replicative10 cycle of HIV are:
The virus is attached to CD4 and the appropriate co- receptor. However, other molecules on these cells may also play a role in the attachment of HIV, particularly chemokine receptors such as CCR5 and CXCR4. This results in fusion of the viral envelope and the cellular membrane and the release of viral nucleocapsid into the cytoplasm.
Following the uncoating, viral RNA is reverse transcribed by the reverse transcriptase (RT).
The resulting double-stranded proviral DNA migrates into the cell nucleus and is integrated into the cellular RNA polymerase II. This host cell can be either latently or actively infected. If latently infected, no viral RNA is produced and a productive infection may not develop. If actively infected, however, the cell may produce mature virions by transcription of proviral DNA.
The proviral DNA is transcribed by the cellular RNA polymerase II. This transcription also generates messenger RNA (mRNA).
The mRNAs are translated by the cellular polysomes. In the cytoplasm, mRNA is translated into HIV-specific structural proteins that are integrated with the viral core particles.
Viral proteins and genomic RNA are transported to the cellular membrane and are assembled there. Immature virions are released. Polypeptide precursors are processed by the viral protease to produce mature viral particles. These assembled virus particles then migrate to the plasma membrane of the infected cell. The virus undergoes final maturation by a process of reverse endocytosis (budding) at the plasma membrane. Subsequent dissemination of the virus occurs either through free infectious particles that are released by the budding process or more likely by cell to cell transfer.
Latency8,10
HIV-1 infection of resting memory or naive CD4+ T cells, macrophages or mononuclear cells leads to a nonproductive latent infection.11,12 The molecular mechanisms that determine whether a virus is to interrupt or continue its lifecycle are still unclear. Two forms of HIV-1 latency can be found in resting CD4+ T cells, a labile pre-integration form and a stable post- integration form. HIV-1 latency occurs even during highly active antiretroviral trerapy (HAART) that successfully reduces plasma viremia to undetectable levels. It has been shown that not only wild type but also resistant HIV-1 sequences persist in reservoirs. Although the number of latently infected cells harboring replication-competent virus is very low, it shows minimal decay and appears to be sufficient to guarantee lifelong persistence of HIV in the majority of patients on current antiretroviral regimes. To date, HIV-1 latency represents a major barrier to virus eradication, immune response and gene polymorphisms in HIV-1 infection.10
The major cause for AIDS progression in HIV-1 infected patients is the decline of CD4+ T lymphocytes which are the primary target for HIV and act as the crucial site for the induction of specific humoral and cell-mediated immune response. Thus, as a consequence of the slow but continuous depletion of CD4+ T lymphocytes during the course of infection, immune defence is damaged and the infected organism becomes susceptible to opportunistic infections that ultimately lead to death.
Cellular immune response9
During primary infection and normally prior to seroconversion, activation of HIV-1-specific cytotoxic CD8+ T lymphocytes (CTL) occurs. Presumably, CTL response is more effective in controlling viral replication rather than HIV-1-specific antibodies. Using quantitative techniques it could be demonstrated that the number of HIV-1-specific CTL is inversely correlated with viral load.13 There are various mechanisms for CTL-mediated virus inhibition. CTL recognition of HIV-1-infected antigen-presenting cells occurs via the T cell receptor (TCR). CTL TCR binds to viral peptides associated with MHC Class I molecules at the surface of infected cells and induces the release of proteases and perforin leading to lysis of infected cells.14 The second mechanism is the interaction of Fas ligand (FasL) on the CTL surface with Fas molecules on target cells resulting in apoptotic lysis of infected cells.15 Besides cell lysis, binding of CTL to HIV-1 infected cells induces the release of noncytotoxic antiviral acting compounds such as interferon-alpha and the CC chemokines MIP-1alpha, MIP-1beta and RANTES.16 These chemokines are the natural ligands of the HIV-1 coreceptor CCR5 and were shown to be capable of inhibiting infection of CD4+ T lymphocytes by R5 HIV-1 strains. CD8+ T lymphocytes reportedly secrete the yet unidentified soluble CD8 antiviral factor (CAF). The pivotal role of specific CTL for the control of viral replication is supported by the observation that long-term nonprogressors (LTNP)17 frequently show extraordinary strong qualitative and quantitative HIV-1-specific CTL response. It has been reported that highly exposed but seronegative individuals had detectable amounts of HIV-1-specific CTL. Irrespective of the observed CTL response the primary cause for the prevention of seroconversion and chronification in these individuals is still not proven.
Humoral immune response10
The contribution of specific humoral immune response appears to play a minor role in controlling HIVndash;1 infection. Crucial for antibody-mediated reduction of HIV-1 viral particles is the amount of neutralizing antibodies rather than the amount of total specific antibodies. Binding of neutralizing antibodies to viral particles mediates incorporation and destruction of virions by phagocytes. However, sera obtained from HIV-1 infected patients are not capable of reducing significantly viral infectivity in vitro.18 Additionally, no correlation between the amount of maternal neutralizing HIV-1-specific antibodies in infected pregnant women and the rate of vertical HIV-1 transmission could be observed.19 Moreover, antiviral activity of present neutralizing antibodies against HIV-1 glycoprotein gp120 is frequently overcome by complete replacement of neutralization-sensitive virus by immune escaping HIV-1 variants, either by mutation-induced conformational gp120 changes and/or by modified glycosylation patterns of gp120. Despite a multitude of antiretroviral mechanisms, the immune system of the majority of individuals does not have the ability to prevent chronification of HIV-1 infection or to eradicate HIV-1 infected cells. The extraordinary high mutation rate of HIV-1 leads to the implementation of viral strains, which escape from CTL recognition due to amino acid exchanges within viral epitopes. As a consequence, viral replication and de novo infection of CD4+ T cells still occurs, leading to the breakdown of the immune system and to death.
In summary, the initial target cells of HIV - namely, CD4 helper T cells and macrophages - show different cytopathic effects. The T cells gradually become fewer as the virus replicates. Helper T cells are known to play a pivotal role in immunologic response, and a decrease in their number leads to immune deficiency and subsequent secondary opportunistic infections. In contrast, the infected macrophages rarely undergo lysis or decrease in number. These circulating infected cells harbor the HIV and may disseminate it throughout the body. Human immunodeficiency virus alters the immune-related functions of these infected monocytes/macrophages in the following ways:
Decreased migration response to chemoattractants
Defective intracellular killing of various microorganisms (such as toxoplasma gondii and candida species)
Reduced expression of Class II MHC molecules, which impairs the processing and presentation of antigen to helper T cells
Excessive production by the macrophages of tumor necrosis factor-alpha which leads to dementia, wasting syndrome and unexplained fever.
Highly active antiretroviral therapy20
Antiretroviral drugs
The advent of potent antiretroviral therapy has had a profound impact on the ophthalmological manifestations of AIDS patients. As these drugs lead to improved immune function, patients have fewer opportunistic infections.
With the discovery of the relationship between a high level of plasma viral RNA and an increased rate of disease progression, therapeutic emphasis has been on reducing plasma viremia completely. Theoretically, all steps in the viral lifecycle represent targets for antiretroviral therapy. However, till date the three major groups of drugs being used in the clinical practice are inhibitors of the reverse transcriptase (nucleoside/nucleotide, NRTI, and non-nucleoside, NNRTI) and the protease inhibitors (PI).
Introduction of HAART is a landmark event in the history of AIDS therapy and involves the use of agents from at least two distinct classes of antiretrovirals. The advent of HAART, including protease inhibitors in the treatment of AIDS, has resulted in improvement of immune status with reduction in viral load in many patients with HIV/AIDS, as evidenced by laboratory and clinical reports.21 HAART has remarkably reduced systemic and ocular morbidity among patients with AIDS. Many AIDS patients are living longer and enjoying a higher quality of life. Immune reconstitution can take eight weeks or longer.
In the majority of HIV-1 infected individuals, HAART resulted in increased CD4+ T cell counts and reduction of plasma viremia to undetectable levels which can be maintained for years. However, long-term virological success of HAART is limited by development of resistance, severe side-effects, pharmacokinetic interactions, or patients′ personal choice. Therefore, new antiretrovirals acting on alternative targets (to avoid cross-resistance with old compounds) and with improved systemic tolerability profiles are required.
Currently, a wide variety of potential new antiretrovirals are under investigation, including integrase inhibitors, fusion inhibitors10 and maturase inhibitors.
Protease inhibitors (L-731, 988 and S-1360 compounds interacting with Tat/Tar (EM2487, tamacrazine, CGP 64222 or CGA 137053)
Maturation inhibitors (PA-457, DSB)
NC inhibitors (inhibitors of the gp120-CD4 interaction (zintevir, FP-21399, BMS-378806, PRO542,BMS806, PRO140)
CXCR4 coreceptor blockers (AMD3100; AMD3465; ALX40- 4C; T22, T134,T140),
CCR5 coreceptor antagonist (TAK-779, TAK-220, SCH-C, SCH-D, E913, AK-602 and NSC 651016) or
Fusion inhibitors (enfuvirtide)
The HAART-mediated improvement of immune function in patients with AIDS may also alter the way the eye responds to both opportunistic infections, especially cytomegalovirus (CMV) and to treatment, resulting in changes in the clinical manifestations of ocular lesions in AIDS. There have been newer ocular diseases in those patients on HAART.22
HAART responders
A patient who shows an improvement in CD4 cell counts of greater than 60 cells/mm3 and has maintained it for more than two months is by definition a person who has shown response to HAART therapy. HAART therapy leads to decreased plasma levels of HIV RNA and increased CD4 T-lymphocyte counts, with improved immune function in patients with HIV infection. This immune recovery has resulted in substantial decline in opportunistic infections and has allowed some patients with CMV retinitis to discontinue specific anti-CMV therapy without reactivation of eye disease.23
Clinical reports show a decrease in the incidence of CMV retinitis since the introduction of HAART. Tural et al.24 and MacDonald et al.,25 demonstrated that some patients who respond to combined antiretroviral treatment with an increase in CD4 T-lymphocyte levels regain the ability to suppress CMV without specific anti-CMV therapy, thereby providing clinical evidence of partial immune recovery in these patients.
Before the introduction of protease inhibitors, patients with CMV retinitis typically had CD4 T-lymphocyte counts less than 50 cells/ml with minimal intraocular inflammation.23 Substantial intraocular inflammation has now been reported in some patients with CMV retinitis who have had improved immune function with HAART. The ocular inflammation associated with clinical immune recovery in patients taking potent antiretroviral regimens is known as immune recovery uveitis (IRU).
Immune recovery uveitis
Immune recovery uveitis is a chronic intraocular inflammatory syndrome, the clinical spectrum of which includes anterior segment inflammation, cataract, vitritis, papillitis, cystoid macular edema, epiretinal membrane, vitreous hemorrhage, retinal neovascularization, and proliferative vitreoretinopathy.26,27 Since IRU in non-CMV retinitis eyes is not common, the ocular inflammation is postulated to be due to the CMV infection itself, which causes breakdown in the blood ocular barrier.28 This may allow CMV antigens to leak out of the eye and give the antigen access to lymphoid organs and stimulate an antigen-specific immune response.
A recent report29 suggested that all patients presenting with the clinical and ophthalmological characteristics of IRU showed the presence of HLA B 8-18.
Vaccine
In the laboratory and the clinic, HIV continues to resist our efforts to find a cure (eradication of the virus from an infected individual), or a vaccine.1 In 25 years, there has not been a single well-documented report of a person whose immune system has completely cleared the virus, with or without the help of the ART. But HIV remains an entirely preventable disease in adults; behavior modification, condom use and other approaches have slowed HIV incidence in many rich countries and a growing number of poor ones.
Immunological tests30
The important tests to detect HIV infection are
Antibody-based tests
HIV-2 P 24 antigen testing
Qualititative and quantitative HIV - 1 Plasma and peripheral blood monocyte culture (PBMC) test
RNA test
Noninvasive tests
The relative merits of different laboratory tests for HIV30
-
Antibody-based tests
-
ELISA, HIV 1 viral lysates-based EIA, synthetic peptide, DNA-recombinant derived antigen
Sensitivity: 99.5%
Specificity: 98.5%
Duration of time required: About 90 min
Remarks: Minimum number of sera needed for testing - batch testing, equipment and expertise required, false positive results occur and is cost-effective if done in batches of sera
-
Rapid HIV tests configured into flow-through cartridges - solid phase capture assays and Dot-immunoblot assays
Sensitivity: 96-99%
Specificity: 97-100%
Duration of time required: About 30-90 min
Remarks: Single serum samples can be tested, rapid; No specialized equipment needed and is cost-effective
-
Western blot antibodies to the following antigens HIV 1 core proteins - p17, p24 and p55, polymerase - p31, p5 and p66, Envelop - gp41, gp120 and gp160
Sensitivity: Variable
Specificity: 99-100%
Duration of time required: About 90 min
Remarks: Confirmatory test, Expertise required, done in batches, antibodies to envelope gp 41 and gp 120 along with p23 core antigen - WB positive and this test is relatively expensive
-
Indirect immunofluorescence
Sensitivity: 96-99%
Specificity: 97-100%
Duration of time required: About 30-90 min
Remarks: Confirmatory test, equipment and expertise required and is expensive
-
-
HIV-1, p24 core protein - ELISA capture
Sensitivity: Variable
Specificity: 100%
Duration of time required: Several hours
Remarks: Viral load assay, increase indicates progression, limited role in diagnosis and is expensive
-
HIV-1 Plasma and PBMC Culture
Sensitivity: Low
Specificity: 100%
Duration of time required: Several hours
Remarks: Useful in obtaining viral isolates but is an expensive test
-
Qualitative DNA PCR testing and Quantitative HIV - 1 RNA testing. Proviral DNA and RNA in clinical samples
Sensitivity: 100%
Specificity: 100%
Duration of time required: Several hours
Remarks: Early ″window″ diagnosis, Quantitative, monitors viral load for therapeutic management, technically difficult and expensive test
-
Noninvasive methods. Oral Fluids, Urine and Vaginal Secretions
Sensitivity: Low
Specificity: Low
Duration of time required: Up to 90 min
Remarks: Tests on easily available clinical samples - instead of blood, not yet standardized and is cost- effective
With further ongoing research, newer laboratory investigations are being developed which would help in identifying the infection earlier and more specifically.
Enhancement of our knowledge on the immunopathogenesis of HIV and its systemic manifestations has been very helpful in the management of AIDS. The newer second and third line HAART regimens are specifically based on our understanding of the basic mechanisms of immunology of HIV which has been of great value in the management of drug-resistant strains of HIV.
Footnotes
Source of Support: Nil
Conflict of Interest: None declared
References
- 1.Fanci AS. Twenty-five years of HIV-AIDS. Science. 2006;315:409. doi: 10.1126/science.1131993. [DOI] [PubMed] [Google Scholar]
- 2.HIV-AIDS epidemiological Surveillance and Estimation report for the year 2005. Indian National AIDS Control Organization (NACO) 2006 Apr
- 3.Biswas J, Madhavan HN, Badrinath SS. Ocular lesions in AIDS: A report of first two cases in India. Indian J Ophthalmol. 1995;43:69–72. [PubMed] [Google Scholar]
- 4.Biswas J, Madhavan HN, George AE, Kumarasamy N, Solomon S. Ocular lesions associated with HIV infection in India: A series of 100 consecutive patients evaluated at a referral center. Am J Ophthalmol. 2000;129:9–15. doi: 10.1016/s0002-9394(99)00415-8. [DOI] [PubMed] [Google Scholar]
- 5.Babu RB, Sudharshan S, Kumarasamy N, Therese KL, Biswas J. Ocular tuberculosis in acquired immunodeficiency syndrome. Am J Ophthalmol. 2006;142:413–8. doi: 10.1016/j.ajo.2006.03.062. [DOI] [PubMed] [Google Scholar]
- 6.Hodge WG, Seiff SR, Margolis TP. Ocular opportunistic infection incidences among patients who are HIV positive compared to patients who are HIV negative. Ophthalmology. 1998;105:895–900. doi: 10.1016/S0161-6420(98)95033-3. [DOI] [PubMed] [Google Scholar]
- 7.Biswas J, editor. Practical guidelines for diagnosis and management. Chennai, India: Gnanodaya Press; 2001. Ocular lesions in AIDS in India. [Google Scholar]
- 8.Basic and clinical science course. Intraocular inflammation and uveitis. Am Acad Ophthalmol. 2005-2006:241–62. [Google Scholar]
- 9.Mossman TR, Coffman R. Two types of mouse helper T cells clone: Implications from immune regulation. Immunol Today. 1987;8:233. doi: 10.1016/0167-5699(87)90171-X. [DOI] [PubMed] [Google Scholar]
- 10.Sierra S, Kupfer B, Kaiser R. Basics of the virology of HIV-1 and its replication - review. J Clin Virol. 2005;34:233–44. doi: 10.1016/j.jcv.2005.09.004. [DOI] [PubMed] [Google Scholar]
- 11.Chun TW, Carruth L, Finzi D, Shen X, DiGiuseppe JA, Taylor H, et al. Quantification of latent tissue reservoirs and total body viral load in HIV-1 infection. Nature. 1997;387:183–8. doi: 10.1038/387183a0. [DOI] [PubMed] [Google Scholar]
- 12.Chun TW, Davey RT, Jr, Ostrowski M, Shawn JJ, Engel D, Mullins JI, et al. Relationship between pre-existing viral reservoirs and the re-emergence of plasma viremia after discontinuation of highly active anti-retroviral therapy. Nat Med. 2000;6:757–61. doi: 10.1038/77481. [DOI] [PubMed] [Google Scholar]
- 13.Ogg GS, Jin X, Bonhoeffer S, Dunbar PR, Nowak MA, Monard S, et al. Quantitation of HIV-1-specific cytotoxic T lymphocytes and plasma load of viral RNA. Science. 1998;279:2103–6. doi: 10.1126/science.279.5359.2103. [DOI] [PubMed] [Google Scholar]
- 14.McMichael AJ, Rowland-Jones SL. Cellular immune responses to HIV. Nature. 2001;410:980–7. doi: 10.1038/35073658. [DOI] [PubMed] [Google Scholar]
- 15.Hadida F, Vieillard V, Mollet L, Clark-Lewis I, Baggiolini M, Debre P. Cutting edge: RANTES regulates Fas ligand expression and killing by HIV-specific CD8 cytotoxic T cells. J Immunol. 1999;163:1105–9. [PubMed] [Google Scholar]
- 16.Wagner L, Yang OO, Garcia-Zepeda EA, Ge Y, Kalams SA, Walker BD, et al. Beta-chemokines are released from HIV-1-specific cytolytic T-cell granules complexed to proteoglycans. Nature. 1998;391:908–11. doi: 10.1038/36129. [DOI] [PubMed] [Google Scholar]
- 17.Migueles SA, Laborico AC, Shupert WL, Sabbaghian MS, Rabin R, Hallahan CW, et al. HIV-specific CD8+ T cell proliferation is coupled to perforin expression and is maintained in nonprogressors. Nat Immunol. 2002;3:1061–8. doi: 10.1038/ni845. [DOI] [PubMed] [Google Scholar]
- 18.Kostrikis LG, Cao Y, Ngai H, Moore JP, Ho DD. Quantitative analysis of serum neutralization of human immunodeficiency virus type 1 from subtypes A, B, C, D, E, F, and I:lack of direct correlation between neutralization serotypes and genetic subtypes and evidence for prevalent serum-dependent infectivity enhancement. J Virol. 1996;70:445–58. doi: 10.1128/jvi.70.1.445-458.1996. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 19.Hengel RL, Kennedy MS, Steketee RW, Thea DM, Abrams EJ, Lambert G, et al. Neutralizing antibody and perinatal transmission of human immunodeficiency virus type 1. AIDS Res Hum Retroviruses. 1998;14:475–81. doi: 10.1089/aid.1998.14.475. [DOI] [PubMed] [Google Scholar]
- 20.Ho DD. Time to hit HIV, early and hard. N Engl J Med. 1995;333:450–1. doi: 10.1056/NEJM199508173330710. [DOI] [PubMed] [Google Scholar]
- 21.Belfort R. The ophthalmologist and the Global impact of the AIDS epidemic: LV Edward Jackson Memorial Lecture. Am J Ophthalmol. 2000;1:1–8. doi: 10.1016/s0002-9394(99)00428-6. [DOI] [PubMed] [Google Scholar]
- 22.Jabs DA, Bartlett JG. AIDS and Ophthalmology: A period of transition. Am J Ophthalmol. 1997;124:227–33. doi: 10.1016/s0002-9394(14)70789-5. [DOI] [PubMed] [Google Scholar]
- 23.Robinson MR, Reed G, Csaky KG, Polis MA, Whitcup SM. Immune- recovery uveitis in patients with cytomegalovirus retinitis taking highly active antiretroviral therapy. Am J Ophthalmol. 2000;130:49–56. doi: 10.1016/s0002-9394(00)00530-4. [DOI] [PubMed] [Google Scholar]
- 24.Tural C, Romeu J, Sirera G, Andreu D, Conejero M, Ruiz S, et al. Long lasting remission of cytomegalovirus retinitis without maintenance therapy in human immunodeficiency virus-infected patients. J Infect Dis. 1998;177:1080–3. doi: 10.1086/517399. [DOI] [PubMed] [Google Scholar]
- 25.Macdonald JC, Torriani FJ, Morse LS, Karavellas MP, Reed JB, Freeman WR. Lack of reactivation of cytomegalovirus retinitis after stopping CMV maintenance therapy in AIDS patients with sustained elevations in CD4 T cells in response to highly active antiretroviral therapy. J Infect Dis. 1998;177:1182–7. doi: 10.1086/515281. [DOI] [PubMed] [Google Scholar]
- 26.Karavellas MP, Azen SP, MacDonald JC, Shufelt CL, Lowder CY, Plummer DJ, et al. Immune recovery vitritis and uveitis in AIDS: Clinical predictors, sequelae and treatment outcomes. Retina. 2001;21:1–9. doi: 10.1097/00006982-200102000-00001. [DOI] [PubMed] [Google Scholar]
- 27.Zegans ME, Walton RC, Holland GN, O′Donnell JJ, Jacobson MA, Margolis TP. Transient vitreous inflammatory reactions associated with combination antiretroviral therapy in patients with AIDS and cytomegalovirus retinitis. Am J Ophthalmol. 1998;125:292–300. doi: 10.1016/s0002-9394(99)80134-2. [DOI] [PubMed] [Google Scholar]
- 28.Schrier RD, Song MK, Smith IL, Karavellas MP, Bartsch DU, Torriani FJ, et al. Intraocular viral and immune pathogenesis of immune recovery uveitis in patients with healed cytomegalovirus retinitis. Retina. 2006;26:165–9. doi: 10.1097/00006982-200602000-00007. [DOI] [PubMed] [Google Scholar]
- 29.Modorati G, Miserocchi E, Brancato R. Immune recovery uveitis and human leukocyte antigen typing: A report on four patients. Eur J Ophthalmol. 2005;15:607–9. doi: 10.1177/112067210501500511. [DOI] [PubMed] [Google Scholar]
- 30.Biswas J, Fogla R, Gopal L, Narayana KM, Banker AS, Kumarasamy N, et al. Current approaches to diagnosis and management of ocular lesions in human immunodeficiency virus positive patients. Indian J Ophthalmol. 2002;50:83–96. [PubMed] [Google Scholar]