

Abdominal compartment syndrome (ACS) is a life-threatening disorder caused by rapidly increasing intra-abdominal pressure. ACS can result in multiorgan failure and carries a mortality of 60%–70%.1 The treatment of choice in ACS is surgical decompression. We present a case of ACS that was successfully treated by ultrasound-guided percutaneous drainage.
CASE REPORT
A 20-year-old man presented after falling over the edge of a tractor. On examination, he was conscious and oriented. The pulse was feeble and blood pressure was not recordable. The abdomen was distended, and there was tenderness in the right upper quadrant. Bowel sounds were sluggish. Bedside ultrasonography detected a hemoperitoneum and a liver laceration. Chest radiography showed elevated diaphragmatic domes.
Contrast-enhanced computed tomography (CT) showed a shattered right lobe and segment 4 of the liver; segments 2 and 3 were spared. The portal venous and hepatic arterial branches were seen opening into the peritoneal cavity not covered by liver parenchyma, suggesting a grade V liver injury (Fig. 1). There were associated multiple rib fractures, pelvic fracture, moderate hemoperitoneum (Fig. 2), minimal right hemothorax and an attenuated inferior vena cava. He was resuscitated and managed conservatively.
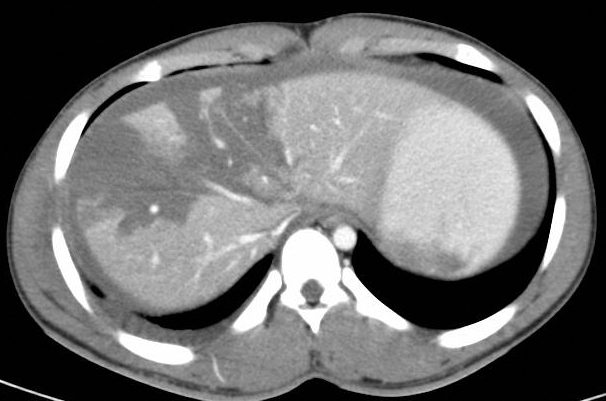
Fig. 1. Contrast-enhanced computed tomography scan showing shattered right lobe and segment 4 of the liver.
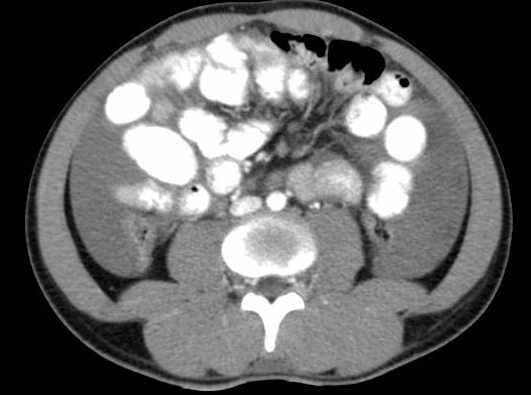
Fig. 2. Contrast-enhanced computed tomography scan showing free fluid in the peritoneum (hemoperitoneum).
Four days after admission, his abdomen gradually became distended, and this was associated with tachypnea and tachycardia. Ultrasonography revealed an increased collection of intraperitoneal fluid. Intra-abdominal pressure measured indirectly with a transurethral bladder catheter was 26 mm Hg. Based on the clinical features, findings on ultrasonography and intra-abdominal pressure measurement, we diagnosed ACS.
Under ultrasonographic guidance, we inserted an 18-gauge puncture needle into the right paracolic gutter. After serial dilatations over an Amplatz Super Stiff Wire (Boston Scientific), a 16-French pigtail catheter was inserted into the right paracolic gutter. Another 16-French pigtail drainage tube was placed into the left paracolic gutter. About 3 L of altered blood was collected in the next hour. Intra-abdominal pressure dropped to 8 mm Hg. The patient recovered within 2 weeks with conservative management.
DISCUSSION
ACS is a life-threatening disorder in critically ill patients caused by rapidly increasing intra-abdominal pressure (> 12 mm Hg), which may result in multiorgan dysfunction and possibly death. This syndrome is most common in the setting of severe abdominal trauma and after re-exploration of the abdomen after major abdominal surgeries.2 Other clinical conditions associated with this syndrome include massive intra-abdominal or retroperitoneal hemorrhage, severe intestinal edema or intestinal obstruction, and ascites under pressure.3 Increased intra-abdominal pressure causes venous stasis and arterial malperfusion of all intra-and extra-abdominal organs, resulting in ischemia, hypoxia and necrosis. In parallel, respiratory, cardiocirculatory, renal, intestinal and cerebral decompensation can be seen.1
The diagnosis of this syndrome is difficult. A number of radiologic features have been described to aid in the diagnosis. Computed tomography features associated with ACS include compression of the inferior vena cava, round belly sign, solid organ compression, bowel-wall thickening with enhancement and bilateral inguinal herniation.4 The treatment of choice in ACS is surgical decompression. When surgical decompression is not feasible, alternative treatment like percutaneous drainage should be considered.5 Our patient was hemodynamically stable, and the only indication for intervention was respiratory distress.
Ultrasound-guided percutaneous catheter drainage is simple and cost-effective. It can be done at the bedside using a portable scanner. In conditions such as ACS, this procedure can be life-saving.
Competing interests: None declared.
Correspondence to: Dr. K.S. Amitha Vikrama Department of Radiology CMC Hospital Vellore 632004 India fax 0416-2232035 amithavikrama@gmail.com
References
- 1.Standl T. Abdominal compartment syndrome. A still underestimated problem? Anasthesiol Intensivmed Notfallmed Schmerzther 2007;42:500-3. [DOI] [PubMed]
- 2.Sanda RB. Abdominal compartment syndrome. Ann Saudi Med 2007;27:183-90. [DOI] [PMC free article] [PubMed]
- 3.De Backer D. Abdominal compartment syndrome. Crit Care 1999;3: R103-4.
- 4.Pickhardt PJ, Shimony JS, Heiken JP, et al. The abdominal compartment syndrome: CT findings. AJR Am J Roentgenol 1999;173:575-9. [DOI] [PubMed]
- 5.Reckard JM, Chung MH, Varma MK, et al. Management of intraabdominal hypertension by percutaneous catheter drainage. J Vasc Interv Radiol 2005;16:1019-21. [DOI] [PubMed]