

Abstract
Despite mounting evidence on the importance of pain management in preterm infants, clinical use of analgesics in this population is limited. Our previous studies have shown that neonatal inflammation results in long-term alterations in adult somatosensory thresholds, characterized by decreased baseline nociceptive sensitivity, and enhanced hyperalgesia following a subsequent inflammatory insult. The present studies were conducted to determine if pre-emptive morphine attenuates these negative consequences. At P0, pups received an injection of morphine sulfate (MS) before an intraplantar injection of 1% carrageenan (CGN). Control pups received either saline (SAL) followed by intraplantar CGN, MS followed by intraplantar SAL, or SAL followed by intraplantar SAL. Pre-emptive morphine significantly attenuated neonatal injury-induced hypoalgesia in adolescence and adulthood. Similarly, morphine pre-treated animals displayed significantly less hyperalgesia and recovered faster from a subsequent inflammatory insult compared to controls. Neonatal morphine had no significant effect on morphine analgesia in adulthood. Interestingly, neonatally injured animals that did not receive morphine displayed a significant rightward shift in the morphine dose response curve in the absence of peripheral inflammation. Together, these results demonstrate that pre-emptive morphine significantly attenuates the long-term behavioral impact of neonatal inflammatory injury.
Keywords: morphine, pain, premature infant, opioid analgesia, neonate
Until the late 1980’s, many in the medical community believed that neonates were incapable of experiencing pain (1). It is now well established, however, that premature infants are highly responsive to noxious stimulation (2, 3) and generate developmentally specific and distinct responses to noxious stimuli (4, 5). Nociceptive responses to noxious stimulation have been demonstrated in preterm neonates using an array of physiological, biochemical and behavioral measures (6, 7). Cortical activation has also been reported in response to noxious stimulation in preterm neonates at 25 weeks, suggesting the potential for higher-level processing of pain (8, 9).
Accumulating evidence indicates that exposure to invasive procedures during the neonatal period leads to both short and long-term alterations in nociceptive processing (10-13). For example, a higher frequency of invasive procedures in preterm infants has been associated with dampened pain responses at 32 weeks of age (14). Decreased facial responsiveness to immunization at 4 and 8 months (15), and blunted pain sensitivity has also been reported in former preterm neonates (10).
Animal studies have also reported that neonatal injury induces long-term alterations in somatic and visceral sensitivity (12, 13, 16). In particular, animals that received intraplantar carrageenan (CGN) at birth display significant hypoalgesia in the previously injured and uninjured paws in adulthood (12, 13). Similar changes in nociceptive sensitivity have also been reported using intraplantar formalin (17). Neonatal injury also results in enhanced hyperalgesia following a subsequent insult in adulthood and significantly decreases the rate of recovery (12, 13).
The use of opioid analgesics in the treatment of neonatal pain is widely debated. Accumulating data, however, suggest that premature infants undergoing invasive procedures benefit from the use of opioid analgesics (18, 19). For example, altered pain responses in former preterm neonates can be predicted by the number of previous painful procedures and are normalized by the use of morphine (14). Moreover, post-operative morphine in preterm and full-term infants reduces behavioral and hormonal stress responses (20, 21), and is associated with decreased mortality (18).
There is evidence that opioid analgesics are efficacious in neonatal rodents (22). Few studies, however, have examined whether opioid analgesics can be used to prevent the consequences of neonatal injury (23). Therefore, the present studies were conducted to determine whether neonatal morphine 1) attenuates neonatal injury-induced hypoalgesia in adulthood; 2) reduces enhanced hyperalgesia observed following adult inflammation and impacts the rate of recovery; and 3) alters the response to morphine in adulthood.
METHODS
Animals
Time-pregnant Sprague-Dawley rats were obtained on the 14th day of gestation (E14) (Zivic Miller) and housed individually. Animals were maintained on a 12:12h light:dark cycle, with food and water available ad libitum. Offspring from the litters were combined on the day of birth, divided up equally, and randomly assigned to a neonatal treatment condition and dam. All litters were reared identically, weaned at P21, and housed with same-sex littermates in groups of 2-3. All experiments were approved by the Georgia State University Animal Care and Use Committee and were conducted in compliance with the guidelines established by the International Association for the Study of Pain (IASP).
Early Life Manipulations
On the day of birth (P0), male and female rat pups received morphine sulfate (MS; 2 mg/kg, ip) or saline (SAL) 15 minutes before a unilateral intraplantar injection of 1% carrageenan (CGN; 5ul) or SAL. This dose of morphine was chosen based on previous studies (22, 24). In preliminary studies, we noted that paw inflammation peaked at 5 hours post-CGN. Therefore, at 5 hours post-CGN or SAL, a second dose of either MS or SAL was administered. This resulted in a total of 4 groups: MS+SAL, MS+CGN, SAL+CGN, and SAL+SAL. All pups within a litter received the same neonatal treatment.
Maternal Behavior
Maternal behavior was observed daily at 18:00 hours for 60 minutes from P0-P7. Maternal observations were conducted by both direct observations and by videotape for later offline analysis. Specific maternal behaviors were recorded including pup licking/grooming, nursing posture (crouching), pup retrieval, nest construction, eating/drinking, exploring, inactive/napping and self-grooming. Observations were conducted by an individual blind to the neonatal group assignment.
Baseline Nociceptive Behavior
On postnatal days 40 and 60 (P40 and P60), baseline paw withdrawal (PWL) and tail flick (TFL) latencies in response to noxious thermal and mechanical stimuli were determined. Thermal testing was conducted using the Paw Thermal Stimulator (UCSD, CA). In this test, animals were placed in a clear plastic testing chamber on a glass surface and allowed to acclimate for 30 minutes before testing. A radiant beam of light beneath the glass base was directed at the plantar surface of the each hindpaw or 1.5 inches from the distal end of the tail, and the withdrawal latency was electronically measured (25). To avoid potential tissue damage, a 20-second automatic termination of the heat stimulus was imposed if withdrawal did not occur. Mechanical testing was conducted using a Dynamic Plantar Aesthesiometer (Ugo Basile, Italy). Animals were placed in Plexiglas chambers above a wire mesh, and allowed to acclimate for 30 minutes before testing. A metal probe was directed at the hind paw and the force applied electronically increased until paw withdrawal occurred. Both time and force were recorded, with an automatic cut off of 60 seconds and 50 grams, respectively. Male and female rats were tested separately. For both tests, the average response of 3 trials was taken; all trials were separated by a 5-minute inter-trial interval.
Nociceptive Behavior Following Re-Inflammation
Following baseline PWL determination at P60, animals received an intraplantar injection of Complete Freund’s adjuvant (CFA; 1:1 CFA:saline soln; 200ul; Sigma) into the neonatally injured hindpaw. CFA was used for re-injury as neonatally injured animals may potentially develop antibodies against CGN, thereby limiting its potency for use as an inflammatory agent. 24 hours following CFA, paw diameter and PWLs were tested as described above.
Recovery Following Re-Inflammation
Paw diameter and PWLs were determined at 7, 14, and 21 days following CFA re-inflammation (P60) to determine the impact of morphine pre-treatment on the response to recovery from a subsequent insult in adulthood.
Response to Morphine in Adulthood Following Neonatal Morphine Exposure
The effect of neonatal morphine on adult morphine responses was tested in the absence of peripheral inflammation. Following baseline PWL determination, animals were administered increasing cumulative doses of morphine (1.8, 1.4, 2.4, 2.4, 2.0, and 8.0 mg/kg s.c. resulting in quarter log doses of 1.8, 3.2, 5.6, 8.0, 10.0, and 18.0 mg/kg; Sigma) (26). PWLs were determined 15 minutes after each injection, followed by administration of the subsequent injection 5 minutes later.
Mu Opioid Receptor Western Blot Analysis
Western blot analysis was conducted to confirm that mu opioid receptors (MOR) are present centrally and peripherally on P0. Five hours after birth, rat pups were rapidly decapitated and brain, spinal cord, and paw tissue were removed and collected on dry ice. Dams were decapitated and maternal blood samples taken. Tissue and blood were stored at -80 degrees. Tissue samples were homogenized in Homogenization Buffer (50mM HEPES pH 7.4, 1mM EDTA, and 0.001% Protease Inhibitor Cocktail; Sigma USA) on ice. The samples underwent freeze/thawing 3 times on dry ice and 37°C waterbath, respectively, and were stored at -80°C. Sample protein concentrations were determined with a BCA Protein Assay Kit (Pierce) against a BSA standard curve. Next, 20μg of each sample was run on 12% acrylamide gels, and transferred to PVDF membranes (Bio-Rad). PVDF membranes were blocked in 5% nonfat dry milk in TTBS (0.1% Tween in 20 mM Tris-HCl; pH 7.5, 175 mM NaCl) overnight at 4°C. PVDF membranes were washed 3 times with TTBS, 10 min each, then incubated with rabbit anti-MOR (1:50,000; Sigma) and rabbit anti-GAPDH (1:300,000; Covance) in 2% nonfat dry milk in TTBS overnight at 4°C. Membranes were washed 3 times with TTBS, 10 min each, and incubated with anti-rabbit HRP conjugated antibodies (1:3000; Cell Signaling) for 1 hour. Membranes were subsequently washed with TTBS 3 times, 10 min each, and washed in TBS (20 mM Tris-HCl pH 7.5, 175 mM NaCl) for 30 min. Bands were visualized via chemiluminescence using LumiGLO (KPL). To confirm that the mu opioid receptor protein observed in the tissue samples was not the result of mu receptors located on maternal immune cells, western blot analysis was also conducted on maternal blood samples.
Statistical Analysis
Data are expressed as either raw withdrawal latencies or mean difference scores. All values are reported as Mean ± S.E.M. Data were analyzed for significant main effects of neonatal treatment and sex using ANOVA and repeated-measures ANOVA was used to analyze recovery post-CFA data; p< 0.05 was considered statistically significant. A priori specified post-hoc tests were conducted using the method of Sheffe as warranted to determine significant mean differences. Where multiple comparisons were made, p values were adjusted accordingly using the Bonferroni method. Morphine dose-response curves were plotted and the half maximal effective doses (ED50) were calculated using percent maximal possible effect (%MPE) data, defined as [(Dose mg/kg-baseline PWL)/(20.0-baseline PWL)]100 (GraphPad, Prism). Analysis of variance was used to compare differences between ED50 values.
RESULTS
Neonatal Morphine Attenuates Hypoalgesia In Adulthood
Pre-emptive morphine significantly attenuated both thermal (Figure 1) and mechanical (Figure 2) hypoalgesia induced by neonatal inflammation at P60. Animals that received SAL+CGN displayed significant thermal hypoalgesia in both the injured and uninjured paws, with females displaying PWLs of approximately 14 seconds and males 11.5 seconds (p<.05 treatment; p<.05 sex), versus PWLs of 10 seconds in SAL+SAL animals. In contrast, morphine pre-treated animals (MS+CGN) were not significantly different from uninjured controls. Consistent with our previous study (13), a significant main effect of sex on injury-induced thermal hypoalgesia was noted (Figure 1A and 1B). Morphine also reduced the injury-induced hypoalgesia present in the tail at P60 (Figure 1C) (P<.05). Furthermore, a significant reduction in the mechanical force threshold was present in morphine pre-treated animals in both paws in adulthood (P60) (Figure 2A and 2B) (p<.05). Significant morphine attenuation of the inflammation-induced hypoalgesia was also observed at P40 (data not shown).
Figure 1. Morphine attenuates thermal hypoalgesia in adulthood.

MS+CGN animals displayed significantly shorter PWLs compared to SAL+CGN in response to thermal stimulation applied to the (A) uninjured paw [F(3,73)=61.330,p<.0001]; (B) injured paw [F(3,73)=80.066,p<.0001]. (C) MS+CGN animals displayed significantly reduced TFLs compared to SAL+CGN animals [F(3,73)=5.879,p=.0012]. Neonatally injured females displayed significantly longer PWLs compared to males; uninjured paw [F(1,73)=8.912,p=.0039] and injured paw [F(1,73)=16.914,p<.0001]. N=5-15 rats per group/per sex; * significant main effect of treatment; ** significant main effect of sex; male: ■; female: □.
Figure 2. Morphine attenuates mechanical hypoalgesia in adulthood.

MS+CGN displayed significantly reduced force (g) to withdrawal compared to SAL+CGN in response to mechanical stimulation applied to the (A) uninjured paw [F(3,40)=50.604,p<.0001]; (B) injured paw [F(3,40)=56.898,p<.0001]. N=5-15 rats per group/per sex; * significant main effect of treatment; male: ■; female: □.
Neonatal Morphine Alters The Response To Re-injury And Recovery
Neonatal morphine significantly attenuated CFA-induced hyperalgesia at 24 hours compared to controls (Figure 3A) (p<.05). At 24 hours post-CFA, PWLs for SAL+CGN animals were approximately 2 seconds in females (mean difference score, MDS, of 12 seconds), and approximately 3.5 seconds in males (MDS 8.5 seconds). Neonatally injured females displayed significantly enhanced thermal hyperalgesia (i.e. greater MDS) at 24 hours following intraplantar CFA compared to males as previously reported (p<.05; Figure 3A) (13). The rate of recovery was also significantly reduced in morphine pre-treated compared to control animals (Figure 3B). SAL+CGN animals continued to show signs of hyperalgesia at 14 days (p<.05; MDS of 1 second in males and 3 seconds in females). In contrast, MS+CGN animals had completely recovered at this time point (MDS of 0), similar to control animals (p<.05). Furthermore, a significantly decreased rate of recovery was noted in injured females compared to injured males; where females displayed greater MDS at 7 and 14 days post-CFA (p<.05).
Figure 3. Morphine attenuates the hyperalgesia following re-inflammation and increases the rate of recovery.

MS+SAL animals displayed significantly lower mean difference scores (MDS) (i.e. reduced hyperalgesia) compared to SAL+CGN animals (A) 24-hours post-CFA [F(3,36)=22.524,p<.0001]; male: ■; female: □. (B) At 7, 14 and 21 days post-CFA, SAL+CGN animals displayed a significantly higher MDS (i.e. reduced rate of recovery) compared to controls [F(6,76)=10.644,p<.0001]. Females displayed significantly higher MDS (i.e. recovered slower) compared to males [F(2,76)=3.240,p<.05]. N=5-7 rats per group/per sex; * significant main effect of treatment; ** significant main effect of sex; male: ■; female: □(MS+SAL-Δ; MS+CGN-□; SAL+CGN-○; SAL+SAL-▽)
Neonatal Morphine Does Not Affect Morphine Analgesia In Adulthood
Neonatal morphine did not significantly alter morphine’s antinociceptive effects in adulthood in males or females (Figures 4A and 4B). As summarized in Table 1, morphine pre-treated females (MS+CGN) displayed similar ED50 values as morphine (MS+SAL) and saline (SAL+SAL) control females. Interestingly, a significant shift in ED50 was noted in neonatally injured females (SAL+CGN) that did not receive morphine (p<.05). Similarly, neonatal morphine in injured males did not alter adult morphine responses (Figure 4B). Nevertheless, SAL+CGN males also displayed a significant shift in ED50 compared to MS+CGN and control males. Finally, females had significantly higher ED50 values compared to males (p<.05; Table 1), as previously reported (27).
Figure 4. Neonatal morphine has no effect on morphine analgesia.

Neonatal morphine had no effect on morphine potency in (A) females; or (B) males in adulthood. Neonatal injury (SAL+CGN) (- - -) produced a significant shift in the morphine dose-response curve in (A) females [F(3,250)=2.982,p=0.03]; and (B) males [F(3,208)=2.979,p=0.03] compared to control animals (-----). N=6-13 rats per group/per sex; MS+CGN-■; SAL+SAL-○; MS+SAL-□; SAL+CGN-●.
Table 1.
Morphine ED50 Values
| Treatment | Female | 95% C.I | Male | 95% C.I |
|---|---|---|---|---|
| MS+CGN | 5.49 | 4.82-6.26 | 4.17** | 3.70-4.71 |
| SAL+SAL | 4.69 | 4.16-5.29 | 3.74** | 3.41-4.11 |
| MS+SAL | 5.28 | 4.77-5.84 | 4.22** | 3.76-4.74 |
| SAL+CGN | 6.60* | 5.54-7.86 | 5.24**/* | 4.35-6.32 |
p<.05 significant effect of treatment
p<.05 significant effect of sex
C.I.=Confidence interrval
Mu Opioid Receptors Are Present At Birth
As shown in Figure 5, MOR-like immunoreactivity (LI) is present on P0 in the brain, spinal cord, and right hindpaw tissue. To control for the presence of MOR on maternal immune cells, we assessed the presence of MOR-LI on maternal blood samples taken at 5 hours post parturition. MOR-LI was undetectable in maternal whole blood or serum (data not shown).
Figure 5. MOR is present centrally and peripherally on P0.
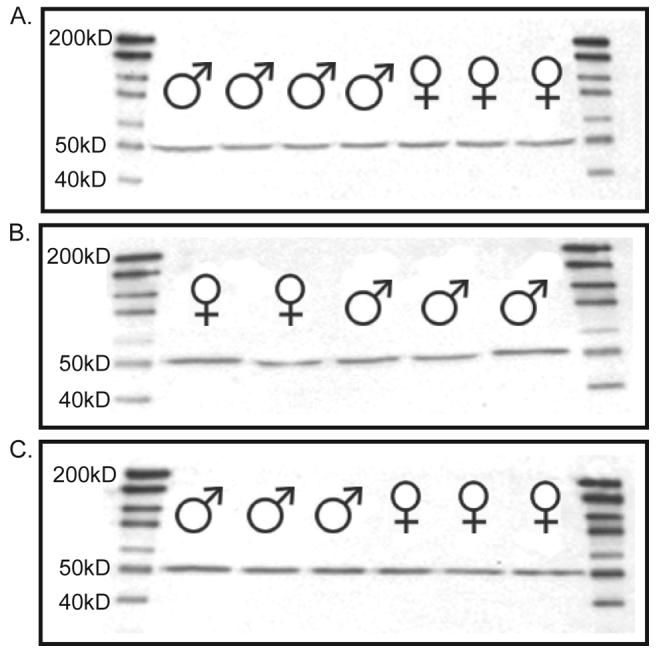
Following western blot analysis, mu opioid receptor protein was present in the (A) brain; (B) spinal cord; (C) hind paw on P0.
Neonatal Injury Has No Impact On Maternal Care
There were no significant differences in maternal behavior between morphine pre-treated and control animals in the amount of time the dam spent on/with pups (Figure 6). Similarly, no differences were noted in the amount of time the dam spent off/without pups or in the amount of time spent licking/grooming pups (Figure 6).
Figure 6. Neonatal injury has no impact on maternal care.

Neonatal injury had no effect on the duration of time the dam spent (A) on/with her litter F(3,13)=.734,p=.5503, (B) away from her litter F(3,13)=.393,p=.7600, (C) licking and grooming pups F(3,13)=1.883,p=.1822. N= 3-6 litters per group.
DISCUSSION
Our principal findings are as follows: (1) morphine pre-treatment attenuates neonatal injury-induced hypoalgesia in adolescent and adult rats; (2) neonatal morphine reduces hyperalgesia following a subsequent inflammation in adulthood; (3) neonatal morphine increases the rate of recovery; (4) neonatal morphine does not affect morphine analgesia in adulthood; (5) neonatal injury significantly reduces morphine potency.
Neonatal Morphine Attenuates The Consequences Of Neonatal Injury
The present studies are the first to demonstrate that pre-emptive morphine attenuates the long-term behavioral consequences associated with neonatal intraplantar CGN in rodents. Morphine blocked thermal and mechanical hypoalgesia in the injured and uninjured paws in adolescence and adulthood in both sexes. This is consistent with previous studies in rodents that report daily morphine administration prior to intraplantar formalin during the first week of life significantly reduces the long-term effects of repetitive pain (22). Similarly, previous studies in humans have reported that morphine ameliorates the effects of early repetitive noxious stimuli in pre-term infants at 4 months of age (14). Moreover, children who had minor neonatal operations and received pre-emptive analgesia responded to immunization pain in a similar manner as controls (28).
There is ample evidence that the hypoalgesia observed following neonatal inflammation might be mediated by a potentiation in descending endogenous opioid tone. Studies have shown that the functional activity of endogenous opioid systems is enhanced following noxious inflammatory stimulation (29, 30). Furthermore, increased endogenous opioid peptide expression and release in the periaqueductal gray (PAG) following peripheral inflammation has been reported, and is associated with decreased nociceptive sensitivity (31). Moreover, we have reported that systemic naloxone attenuates behavioral deficits in pain responsiveness associated with neonatal inflammation, suggesting that alterations in opioid tone may underlie the observed hypoalgesia (13). Our recent studies have demonstrated that injury-induced alterations in opioid tone primarily involve mu and delta opioid receptors in the PAG (LaPrairie J 2007 SFN poster). These results are consistent with findings in former pre-term infants (32, 33) and rodents treated neonatally with capsaicin (34) that early life trauma may impair the proper development of endogenous inhibitory systems in the CNS. In the present study, the ability of pre-emptive morphine to block the hypoalgesia may indeed occur through direct modulation of primary afferent drive into the spinal cord, thereby inhibiting the central relay of inflammatory pain and preventing the subsequent increase in descending endogenous opioid tone.
We cannot rule out alterations in the HPA axis as a contributing factor to the observed hypoalgesia. Nociception is one element in a broader context of stress reactivity (35, 36), and experimental studies have shown that exposure to early life stressors can permanently increase nociceptive thresholds and decrease the behavioral and physiological responses to stress in adult rodents (36-38). Data from human preterm infants also suggest that neonatal exposure to noxious stimuli may alter future pain responses. Ex-preterm infants exposed to four weeks of NICU care display reduced pain responsiveness following heel lance (39). In addition, pre-term birth is associated with increased salivary cortisol in response to vaccination at 6 months of age (40).
Neonatal Morphine Reduces Inflammatory Hyperalgesia And Increases The Rate Of Recovery Following Re-injury
In the present study, morphine pre-treatment significantly attenuated CFA-induced hyperalgesia and increased the rate of recovery, such that both males and females recovered 7 days faster than non- pre-treated animals. Interestingly, preliminary anatomical studies in our laboratory suggest that neonatal inflammation results in increased primary afferent innervation of the dorsal horn reflected by increased expression of CGRP and substance P immunoreactivity (LaPrairie JL, Murphy AZ, SfN abstract, 2005), which may account for our observed hyperalgesia. Our working hypothesis is that re-inflammation in adulthood results in an enhanced dorsal horn release of CGRP and/or substance P due to increased primary afferent input. Increased release of these pro-nociceptive peptides would be predicted to result in an enhanced hyperalgesic response.
Clinical reports demonstrate that at 32 weeks, preterm infants experience a reduced rate of recovery to skin breaking procedures (41), and exhibit subtle differences in ability to recover from finger lance at 4 months compared to controls (15). There are no reports on the impact of pre-emptive morphine on recovery rates in premature neonates, however, our data suggest that morphine analgesia may in fact significantly increase the rate of recovery following procedural pain in NICU infants. Neonatal pre-treatment with morphine may prevent the injury-induced increase in primary afferent innervation in the spinal cord, thereby blocking the susceptibility of re-inflammation to produce enhanced hyperalgesia and increasing the rate of recovery.
Neonatal Morphine Does Not Affect Morphine Analgesia In Adulthood
Our original hypothesis was that exposure to morphine during neonatal development may alter opioid receptor number and/or affinity, thereby altering morphine’s antinociceptive effects in adulthood. This hypothesis was based on previous studies that report a 60-fold shift in the morphine dose response curve in adult rats that received repeated neonatal morphine in the absence of pain (17). Nevertheless, we show that neonatal morphine did not affect morphine analgesia in adult animals (i.e. no significant shift in ED50 values). In contrast to the previous reports, however, neonatal morphine administration was associated with peripheral inflammation and was only provided on P0 in the present study.
Interestingly, neonatal injury alone resulted in a significant decrease in morphine potency in both males and females in adulthood. These results have serious clinical implications. Previous studies have reported that pre-term infants that experience surgery during the first three months of life have significantly higher peri- and post-operative analgesic requirements in response to surgery in the same or different dermatome compared to control infants (21, 40). Similarly, mice exposed to chronic noxious stimulation display increased TFLs compared to controls, and a significant two-fold increase in the ED50 of morphine in response to abdominal constriction (42). As noxious stimulation during the neonatal period leads to increased activation of opioid systems in a manner analogous to the repeated application of exogenous opiates, these studies provide evidence that neonatal injury produces cross-tolerance to the analgesic effects of morphine thereby decreasing the subsequent effectiveness of morphine (43, 44). Again interestingly, exposure to morphine neonatally did not result in a significant shift in ED50 values. Therefore, we believe that opioid cross tolerance is associated with neonatal injury-induced chronic exposure to endogenous opioids resulting from a potentiation of the descending inhibitory circuit, and not a result of exposure to morphine on P0. Alternatively, neonatal stress associated with maternal separation and repeated handling is also associated with reduced opioid analgesia (36, 37). This suggests that alterations in opioid analgesia may reflect a combined effect of neonatal nociceptive experience as well as early life stress, and therefore may involve altered responsiveness of endogenous analgesia circuits and the hypothalamic-pituitary-adrenal axis.
Acknowledgments
Financial Support: This work was supported by National Institute of Health grants DA16272 and AR49555 awarded to Anne Z. Murphy, the Center for Behavioral Neuroscience NSF: IBN 9876754, and the Georgia State University Brains and Behavior Program.
Abbreviations
- CFA
Complete Freund’s adjuvant
- CGN
carrageenan
- MDS
mean difference score
- MOR
mu opioid receptor
- MOR
LI-mu opioid receptor-like immunoreactivity
- MS
morphine sulfate
- P
postnatal day
- PWL
paw withdrawal latency
- SAL
saline
References
- 1.Tibboel D, Anand KJ, van den Anker JN. The pharmacological treatment of neonatal pain. Semin Fetal Neonatal Med. 2005;10:195–205. doi: 10.1016/j.siny.2004.11.002. [DOI] [PubMed] [Google Scholar]
- 2.Andrews K, Fitzgerald M. Cutaneous flexion reflex in human neonates: a quantitative study of threshold and stimulus-response characteristics after single and repeated stimuli. Dev Med Child Neurol. 1999;41:696–703. doi: 10.1017/s0012162299001425. [DOI] [PubMed] [Google Scholar]
- 3.Smith RP, Gitau R, Glover V, Fisk NM. Pain and stress in the human fetus. Eur J Obstet Gynecol Reprod Biol. 2000;92:161–165. doi: 10.1016/s0301-2115(00)00441-3. [DOI] [PubMed] [Google Scholar]
- 4.Giannakoulopoulos X, Teixeira J, Fisk N, Glover V. Human fetal and maternal noradrenaline responses to invasive procedures. Pediatr Res. 1999;45:494–499. doi: 10.1203/00006450-199904010-00007. [DOI] [PubMed] [Google Scholar]
- 5.Anand KJ, Carr DB. The neuroanatomy, neurophysiology, and neurochemistry of pain, stress, and analgesia in newborns and children. Pediatr Clin North Am. 1989;36:795–822. doi: 10.1016/s0031-3955(16)36722-0. [DOI] [PubMed] [Google Scholar]
- 6.Franck LS, Greenberg CS, Stevens B. Pain assessment in infants and children. Pediatr Clin North Am. 2000;47:487–512. doi: 10.1016/s0031-3955(05)70222-4. [DOI] [PubMed] [Google Scholar]
- 7.McNair C, Ballantyne M, Dionne K, Stephens D, Stevens B. Postoperative pain assessment in the neonatal intensive care unit. Arch Dis Child Fetal Neonatal Ed. 2004;89:F537–F541. doi: 10.1136/adc.2003.032961. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Slater R, Cantarella A, Gallella S, Worley A, Boyd S, Meek J, Fitzgerald M. Cortical pain responses in human infants. J Neurosci. 2006;26:3662–3666. doi: 10.1523/JNEUROSCI.0348-06.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 9.Bartocci M, Bergqvist LL, Lagercrantz H, Anand KJ. Pain activates cortical areas in the preterm newborn brain. Pain. 2006;122:109–117. doi: 10.1016/j.pain.2006.01.015. [DOI] [PubMed] [Google Scholar]
- 10.Grunau RV, Whitfield MF, Petrie JH. Pain sensitivity and temperament in extremely low-birth-weight premature toddlers and preterm and full-term controls. Pain. 1994;58:341–346. doi: 10.1016/0304-3959(94)90128-7. [DOI] [PubMed] [Google Scholar]
- 11.Bhutta AT, Cleves MA, Casey PH, Cradock MM, Anand KJ. Cognitive and behavioral outcomes of school-aged children who were born preterm: a meta-analysis. JAMA. 2002;288:728–737. doi: 10.1001/jama.288.6.728. [DOI] [PubMed] [Google Scholar]
- 12.Lidow MS, Song ZM, Ren K. Long-term effects of short-lasting early local inflammatory insult. Neuroreport. 2001;12:399–403. doi: 10.1097/00001756-200102120-00042. [DOI] [PubMed] [Google Scholar]
- 13.LaPrairie JL, Murphy AZ. Female rats are more vulnerable to the long-term consequences of neonatal inflammatory injury. Pain. 2007;132:S124–S133. doi: 10.1016/j.pain.2007.08.010. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 14.Grunau RE, Oberlander TF, Whitfield MF, Fitzgerald C, Lee SK. Demographic and therapeutic determinants of pain reactivity in very low birth weight neonates at 32 Weeks’ postconceptional Age. Pediatrics. 2001;107:105–112. doi: 10.1542/peds.107.1.105. [DOI] [PubMed] [Google Scholar]
- 15.Oberlander TF, Grunau RE, Whitfield MF, Fitzgerald C, Pitfield S, Saul JP. Biobehavioral pain responses in former extremely low birth weight infants at four months’ corrected age. Pediatrics. 2000;105:e6. doi: 10.1542/peds.105.1.e6. [DOI] [PubMed] [Google Scholar]
- 16.Wang G, Ji Y, Lidow MS, Traub RJ. Neonatal hind paw injury alters processing of visceral and somatic nociceptive stimuli in the adult rat. J Pain. 2004;5:440–449. doi: 10.1016/j.jpain.2004.07.003. [DOI] [PubMed] [Google Scholar]
- 17.Bhutta AT, Rovnaghi C, Simpson PM, Gossett JM, Scalzo FM, Anand KJ. Interactions of inflammatory pain and morphine in infant rats: long-term behavioral effects. Physiol Behav. 2001;73:51–58. doi: 10.1016/s0031-9384(01)00432-2. [DOI] [PubMed] [Google Scholar]
- 18.Anand KJ, Hickey PR. Halothane-morphine compared with high-dose sufentanil for anesthesia and postoperative analgesia in neonatal cardiac surgery. N Engl J Med. 1992;326:1–9. doi: 10.1056/NEJM199201023260101. [DOI] [PubMed] [Google Scholar]
- 19.Yaster M, Deshpande JK. Management of pediatric pain with opioid analgesics. J Pediatr. 1988;113:421–429. doi: 10.1016/s0022-3476(88)80622-x. [DOI] [PubMed] [Google Scholar]
- 20.Bouwmeester NJ, Anand KJ, van Dijk M, Hop WC, Boomsma F, Tibboel D. Hormonal and metabolic stress responses after major surgery in children aged 0-3 years: a double-blind, randomized trial comparing the effects of continuous versus intermittent morphine. Br J Anaesth. 2001;87:390–399. doi: 10.1093/bja/87.3.390. [DOI] [PubMed] [Google Scholar]
- 21.Bouwmeester NJ, Hop WC, van Dijk M, Anand KJ, van den Anker JN, Tibboel D. Postoperative pain in the neonate: age-related differences in morphine requirements and metabolism. Intensive Care Med. 2003;29:2009–2015. doi: 10.1007/s00134-003-1899-4. [DOI] [PubMed] [Google Scholar]
- 22.Abbott FV, Guy ER. Effects of morphine, pentobarbital and amphetamine on formalin-induced behaviours in infant rats: sedation versus specific suppression of pain. Pain. 1995;62:303–312. doi: 10.1016/0304-3959(94)00277-L. [DOI] [PubMed] [Google Scholar]
- 23.Sternberg WF, Scorr L, Smith LD, Ridgway CG, Stout M. Long-term effects of neonatal surgery on adulthood pain behavior. Pain. 2005;113:347–353. doi: 10.1016/j.pain.2004.11.013. [DOI] [PubMed] [Google Scholar]
- 24.Nandi R, Beacham D, Middleton J, Koltzenburg M, Howard RF, Fitzgerald M. The functional expression of mu opioid receptors on sensory neurons is developmentally regulated; morphine analgesia is less selective in the neonate. Pain. 2004;111:38–50. doi: 10.1016/j.pain.2004.05.025. [DOI] [PubMed] [Google Scholar]
- 25.Hargreaves K, Dubner R, Brown F, Flores C, Joris J. A new and sensitive method for measuring thermal nociception in cutaneous hyperalgesia. Pain. 1988;32:77–88. doi: 10.1016/0304-3959(88)90026-7. [DOI] [PubMed] [Google Scholar]
- 26.Morgan MM, Fossum EN, Stalding BM, King MM. Morphine antinociceptive potency on chemical, mechanical, and thermal nociceptive tests in the rat. J Pain. 2006;7:358–366. doi: 10.1016/j.jpain.2005.12.009. [DOI] [PubMed] [Google Scholar]
- 27.Wang X, Traub RJ, Murphy AZ. Persistent pain model reveals sex difference in morphine potency. Am J Physiol Regul Integr Comp Physiol. 2006;291:R300–R306. doi: 10.1152/ajpregu.00022.2006. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 28.Peters JW, Koot HM, de Boer JB, Passchier J, Bueno-de-Mesquita JM, de Jong FH, Duivenvoorden HJ, Tibboel D. Major surgery within the first 3 months of life and subsequent biobehavioral pain responses to immunization at later age: a case comparison study. Pediatrics. 2003;111:129–135. doi: 10.1542/peds.111.1.129. [DOI] [PubMed] [Google Scholar]
- 29.Iadarola MJ, Douglass J, Civelli O, Naranjo JR. Differential activation of spinal cord dynorphin and enkephalin neurons during hyperalgesia: evidence using cDNA hybridization. Brain Res. 1988;455:205–212. doi: 10.1016/0006-8993(88)90078-9. [DOI] [PubMed] [Google Scholar]
- 30.Noguchi K, Morita Y, Kiyama H, Sato M, Ono K, Tohyama M. Preproenkephalin gene expression in the rat spinal cord after noxious stimuli. Brain Res Mol Brain Res. 1989;5:227–234. doi: 10.1016/0169-328x(89)90039-9. [DOI] [PubMed] [Google Scholar]
- 31.Williams FG, Mullet MA, Beitz AJ. Basal release of Met-enkephalin and neurotensin in the ventrolateral periaqueductal gray matter of the rat: a microdialysis study of antinociceptive circuits. Brain Res. 1995;690:207–216. doi: 10.1016/0006-8993(95)00554-4. [DOI] [PubMed] [Google Scholar]
- 32.Goffaux P, Lafrenaye S, Morin M, Patural H, Demers G, Marchand S. Preterm births: Can neonatal pain alter the development of endogenous gating systems? Eur J Pain. 2008 doi: 10.1016/j.ejpain.2008.01.003. in press. [DOI] [PubMed] [Google Scholar]
- 33.Hermann C, Hohmeister J, Demirakca S, Zohsel K, Flor H. Long-term alteration of pain sensitivity in school-aged children with early pain experiences. Pain. 2006;125:278–285. doi: 10.1016/j.pain.2006.08.026. [DOI] [PubMed] [Google Scholar]
- 34.Cervero F, Plenderleith MB. C-fibre excitation and tonic descending inhibition of dorsal horn neurones in adult rats treated at birth with capsaicin. J Physiol. 1985;365:223–237. doi: 10.1113/jphysiol.1985.sp015768. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 35.Grunau RE, Holsti L, Haley DW, Oberlander T, Weinberg J, Solimano A, Whitfield MF, Fitzgerald C, Yu W. Neonatal procedural pain exposure predicts lower cortisol and behavioral reactivity in preterm infants in the NICU. Pain. 2005;113:293–300. doi: 10.1016/j.pain.2004.10.020. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 36.Sternberg WF, Ridgway CG. Effects of gestational stress and neonatal handling on pain, analgesia, and stress behavior of adult mice. Physiol Behav. 2003;78:375–383. doi: 10.1016/s0031-9384(03)00015-5. [DOI] [PubMed] [Google Scholar]
- 37.Coutinho SV, Plotsky PM, Sablad M, Miller JC, Zhou H, Bayati AI, McRoberts JA, Mayer EA. Neonatal maternal separation alters stress-induced responses to viscerosomatic nociceptive stimuli in rat. Am J Physiol Gastrointest Liver Physiol. 2002;282:G307–G316. doi: 10.1152/ajpgi.00240.2001. [DOI] [PubMed] [Google Scholar]
- 38.Pieretti S, d’Amore A, Loizzo A. Long-term changes induced by developmental handling on pain threshold: effects of morphine and naloxone. Behav Neurosci. 1991;105:215–218. doi: 10.1037//0735-7044.105.1.215. [DOI] [PubMed] [Google Scholar]
- 39.Johnston CC, Stevens BJ. Experience in a neonatal intensive care unit affects pain response. Pediatrics. 1996;98:925–930. [PubMed] [Google Scholar]
- 40.Peters JW, Schouw R, Anand KJ, van Dijk M, Duivenvoorden HJ, Tibboel D. Does neonatal surgery lead to increased pain sensitivity in later childhood? Pain. 2005;114:444–454. doi: 10.1016/j.pain.2005.01.014. [DOI] [PubMed] [Google Scholar]
- 41.Morison SJ, Holsti L, Grunau RE, Whitfield MF, Oberlander TF, Chan HW, Williams L. Are there developmentally distinct motor indicators of pain in preterm infants? Early Hum Dev. 2003;72:131–146. doi: 10.1016/s0378-3782(03)00044-6. [DOI] [PubMed] [Google Scholar]
- 42.Christie MJ, Trisdikoon P, Chesher GB. Tolerance and cross tolerance with morphine resulting from physiological release of endogenous opiates. Life Sci. 1982;31:839–845. doi: 10.1016/0024-3205(82)90538-0. [DOI] [PubMed] [Google Scholar]
- 43.Lett BT, Grant VL, Koh MT, Flynn G. Prior experience with wheel running produces cross-tolerance to the rewarding effect of morphine. Pharmacol Biochem Behav. 2002;72:101–105. doi: 10.1016/s0091-3057(01)00722-5. [DOI] [PubMed] [Google Scholar]
- 44.Stoller DC, Thornton SR, Smith FL. Loss of antinociceptive efficacy in rat pups infused with morphine from osmotic minipumps. Pharmacology. 2002;66:11–18. doi: 10.1159/000063250. [DOI] [PubMed] [Google Scholar]