

Summary
Although there are numerous publications in the literature describing the wide range of diagnosis, classifications and treatment of malformations of the hearing apparatus, even more variations can be found in clinical practice. Indeed, each individual case is unique as far as concerns pathogenesis, clinical course and treatment. The case reported herein describes a 12-year-old boy affected by cranio-facial dysmorphism and monolateral conductive hearing loss in the right ear: followed from radiological diagnosis – carried out to study a malformation of the ear pinna – to surgical treatment.
Keywords: Middle ear malformations, Cranio-facial dysplasia, Conductive hearing loss, Surgical treatment
Riassunto
Vi sono, in letteratura, numerose pubblicazioni concernenti diagnosi, classificazione e terapia delle malformazioni a carico dell’apparato uditivo, ma ancora più numerose sono le possibili varianti riscontrabili nella pratica clinica. Ogni singolo caso è, per patogenesi, decorso clinico e possibilità terapeutiche, peculiare. Il presente lavoro è l’analisi del caso di un bambino di 12 anni affetto da dismorfismo cranico e ipoacusia trasmissiva destra: lo si seguirà dalla diagnosi radiologica – avvenuta in seguito ad accertamenti effettuati per una malformazione del padiglione auricolare – al trattamento chirurgico.
Case report
J.R. was first seen when he was 12 years old for hearing problems noticed by his mother.
He was born of a 30-year-old mother and a 35-year-old father: both parents were in good health and there was no family history of malformations.
The child was the product of a normal pregnancy, labour and delivery and there was no evidence of foetal infections during the pregnancy. Audiometrically, the patient was found to have a monolateral conductive hearing loss in the right ear. This impairment was more severe for frequencies between 125 and 2000 Hz. He pronounced his first words when he was 12 months old and started walking at 18 months. When he was a year old, he underwent surgery, to remove a cartilaginous formation in the region of the right ear tragus, at 5 he underwent adenoidectomy, and, at 10 appendicectomy. Speech and language milestones were essentially age-appropriate, and there was no evidence of cognitive or behavioural impairment. There was no family history of hearing loss. External inspection revealed a cranio-facial dysmorphism. Computed tomography (CT) scan of the petrous pyramid and mastoid revealed anomalies of the middle and internal ear: “asymmetry of the bony structures at the basis of the skull, particularly of the right petrous pyramid that is dysmorphic, anteriorly displaced and rotated. There is a hypoplasia of the epitympanum; the ossicles are in place with not well-identified stapes” (Figs. 1, 2).
Fig. 1.
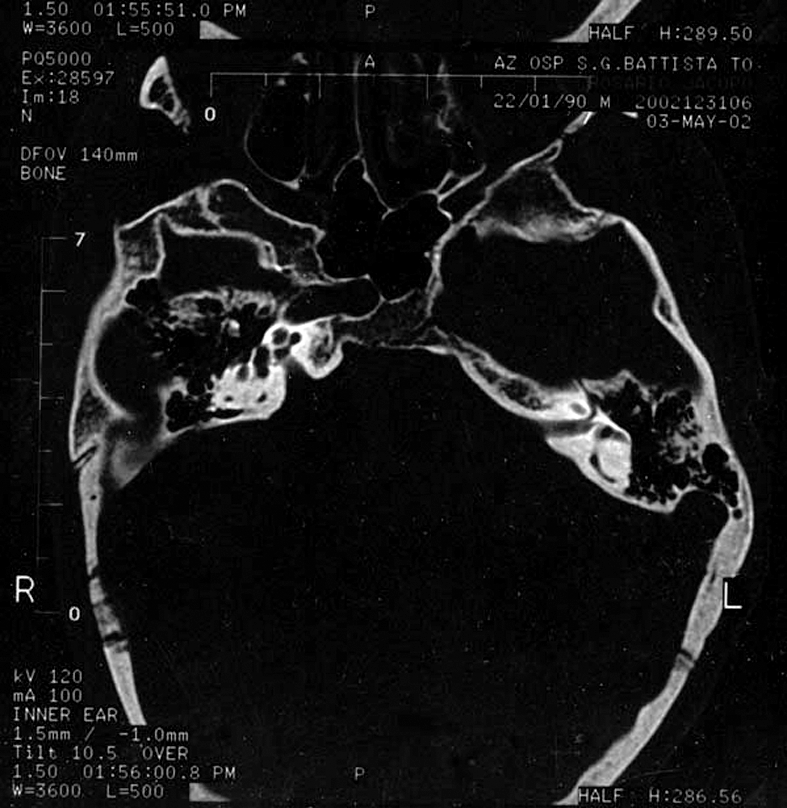
Axial CT scan showing the asymmetry of the bony structures of the basis of the skull, particularly of the right petrous pyramid that is dysmorphic, anteriorly displaced and rotated. It has to be pointed out the direction of the internal auditory canal of the right side: nearly 90° in comparison to the left one.
Fig. 2.

Coronal CT scan showing hypoplasy of the right epithympanum and a not well identified right stapes. Impossible to have both the petrous bones on the same section.
Noteworthy was the internal acoustic canal: i.e., the longitudinal axis was normal in the left ear, while it was rotated by about 90° in the right ear. Mandibular condyles were of different volume and were not at the same level in the frontal section.
Having taken into consideration all these elements, it was decided to proceed with surgical treatment.
Surgical procedure
Given the young age of the patient, an anterior tympanotomy was performed under general anaesthesia.
Following incision of the skin between the tragus and helix, the external ear canal was enlarged to allow a better view of the postero-inferior portion of the tympanic membrane that was partially hidden by the abnormal curvature of the canal floor.
The chorda tympani was preserved and the middle ear cavity normal.
The ossicular chain was present, but the stapes had a fixed footplate, a hypoplasic posterior crus and no anterior crus. The malleus handle was displaced anteriorly, while the anterior apophysis of the incus was also hypoplasic.
It was difficult to explore the posterior portion of the oval window as the bony anulus and facial canal were overhanging.
Extensive drilling was performed in the anterior portion of the oval window niche, after which a hole was drilled in order to place a fluoroplastic piston-type prosthesis. The tympanomeatal flap was replaced and the external meatus sutured.
The post-operative course was uneventful and an acceptable threshold was observed at one month, which was subjectively better than the instrumental (Figs. 3, 4).
Fig. 3.

Pre-operative audiogram showing a right conductive hearing loss for every frequency of the tonal field. The left ear presents an hearing function in the normal values range.
Fig. 4.

Audiogram performed three months after the operation. The right ear presents an improvement of the hearing function for all the frequencies. Particularly, the diagram shows good results for the frequencies between 1 and 4 kHz that are the ones mostly interested in the oral communication.
Discussion
The labyrinth has an embryologic origin which is quite separate from that of the middle and external ear. The inner ear or labyrinth develops from the ectoderm by the invagination of the otic placode. The external and middle ears, as well as the ossicles, develop from the first branchial cleft, the first pharyngeal pouch and the adjacent regions of the first and second branchial arch. Due to their separate origins, anomalies tend to be either of the inner or middle and external ear. Although anomalies of both regions are rare they do occasionally occur in certain syndromes and chromosomal anomalies. Combination anomalies also occur in cases of toxin exposure during early gestation.
The inner ear: the anomalies that affect the bony structure of the inner ear result from problems in the first trimester of pregnancy. The bony inner ear is essentially completely developed by this time. Initially, a small invagination of surface ectoderm forms a small vesicle, which becomes separate from the external surface. The vesicle, called the otocyst, is at first almost round, but soon small pouches form that elongate and further differentiate to form the cochlea, vestibule and semicircular canals. Congenital anomalies may mimic stages in this differentiation or may reflect absence or failure of this differentiation 1.
Middle and external ear: the first pharyngeal pouch extends from the primitive gut to form the eustachian tube and middle ear “en route” to the mastoid region. The branchial cleft extends inward from the external surface of the embryo and joins the pouch in the region of the tympanic membrane. The mesenchyme of the first and second branchial arches, which border the first cleft, form the ossicular chain, their muscles and ligaments. Anomalies often affect both areas due to the intimate relationship of formation of the middle and external ear 2–7.
Numerous studies on embryogenesis of the hearing system structure 8–10 have shown that it differs greatly from one individual to another: indeed, leading to the statement that “no two ears are the same” 11.
Despite this great physiological variability, reports of cases have appeared in the literature in which this difference becomes clinically relevant and, at times, truly pathological 12–16.
A malformation of the ear can be suspected in the presence of a deep conductive hearing loss without any evident damage in the middle or external ear. When this is the case, as in some microdysplasias (i.e., of the ossicular chain) are not detected either by CT scan 17 11 or X-ray examination 18 19, then explorative tympanotomy is necessary 20–24.
There are numerous reports on congenital malformations of the hearing apparatus25,26: from cases of synostosis between the malleus and incus 27, to congenital absence of the incus 28–32, lack of the incudostapedial joint 33–35, or stapedial malformations 36–39. These malformations are often related to malformations of the external ear. However, it is rare to find reports of malformations with an association of the external, middle or inner ear, such as that described here, in which cranial-facial-somatic dysmorphism with an evident asymmetry of the petrous bones is also present.
It is noteworthy that despite a malformation of the inner ear, there is no sensorineural hearing loss.
The peculiarity of this case resides in the particular distribution of the middle ear structures. Indeed, the surgical procedure routinely used for the fixed stapes in the case of microdysplasia of the ossicular chain was not feasible and, in fact, the surgeon had to try to find a “new” way to perform platinotomy.
Rotation of the whole petrous bone caused a radical alteration in the anatomic relationships between the ossicular chain and the medial wall of the tympanic cavity, resulting in the position of the oval window niche being moved posteriorly/superiorly which meant the surgeon had to enter into the anterior pole in the vestibule.
As the apophysis of the incus and malleus were also displaced anteriorly, it was possible, on account of its elasticity, to use the standard fluoroplastic prosthesis for stapedectomy.
The decision to perform surgery, even in the absence of indications, from a functional point of view (i.e., normal hearing in the other ear), was taken on the basis of the radiological findings (distorted middle ear, but potentially still correctable). Moreover, the family was in favour of all attempts to improve the child’s hearing.
If a less favourable outcome is suspected, due to a more severe malformation (dangerous surgery), especially in a patient with monolateral deafness, it is preferable to delay surgery until the patient is of age and able to give his/her own consent or make decisions regarding the “costs/benefits” of the treatment 40–45.
References
- 1.Jackler RK, Luxford WM, House WF. Congenital malformation of the inner ear: a classification based on embryogenesis. Laryngoscope 1987;97:2-14. [DOI] [PubMed] [Google Scholar]
- 2.Cousins VC, Milton CM. Congenital ossicular abnormalities: a review of 68 cases. Am J Otol 1988;9:76-80. [PubMed] [Google Scholar]
- 3.Jahrsdörfer RA. The facial nerve in congenital ear malformations. Laryngoscope 1981;91:1217-25. [DOI] [PubMed] [Google Scholar]
- 4.Neame JH. Anomalies of the ossicular chain. J Laryngol Otol 1962;76:596-600. [DOI] [PubMed] [Google Scholar]
- 5.Nomura Y, Nagao Y, Fukaya T. Anomalies of the middle ear. Laryngoscope 1988;98:390-3. [DOI] [PubMed] [Google Scholar]
- 6.Teunissen B, Cremers WR. Classification of congenital middle ear anomalies. Report on 144 ears. Ann Otol Rhinol Laryngol 1993;102:606-12. [DOI] [PubMed] [Google Scholar]
- 7.Wilmot TJ. Hereditary conductive deafness due to incus-stapes abnormalities and associated with pinna deformity. J Laryngol Otol 1970;84:469-79. [DOI] [PubMed] [Google Scholar]
- 8.Anson BJ, Hanson JS, Richany SF. Early embryology of the auditory ossicles and associated structures in relation to certain anomalies observed clinically. Ann Otol Rhinol Laryngol 1960;69:427-47. [DOI] [PubMed] [Google Scholar]
- 9.Hanson JR, Anson BJ, Strickland EM. Branchial sources of the auditory ossicles in man. Arch Otolaryngol 1962;76:100-22. [DOI] [PubMed] [Google Scholar]
- 10.Strickland EM, Hanson JR, Anson BJ. Branchial sources of the auditory ossicles in man. Arch Otolaryngol 1962;76:200-15. [DOI] [PubMed] [Google Scholar]
- 11.Hough JVD. Congenital malformations of the middle ear. Arch Otolaryngol Head Neck Surg 1963;78:335-43. [DOI] [PubMed] [Google Scholar]
- 12.Gerhardt HJ. One hundred and seventy-five surgically treated malformations of the external and middle ear: findings and results. Auris Nasus Larynx 1988;15:81-7. [DOI] [PubMed] [Google Scholar]
- 13.Henner R. Congenital middle ear malformations. Arch Otolaryngol 1960;71:454-8. [DOI] [PubMed] [Google Scholar]
- 14.Jahrsdörfer R. Congenital malformations of the ear. Analysis of 94 operations. Ann Otol Rhinol Laryngol 1980;89:348-52. [DOI] [PubMed] [Google Scholar]
- 15.Kraus P, Ziv M. Incus fixation due to congenital anomaly of the chorda tympani. Acta Otolaryngol 1971;72:358-60. [DOI] [PubMed] [Google Scholar]
- 16.Plester D. The promontorial window. Acta Otorhinolaryngol Belg 1989;43:105-8. [PubMed] [Google Scholar]
- 17.Hough JVD. Malformations and anatomical variations seen in the middle ear during the operation for mobilization of the stapes. Laryngoscope 1958;68:1337-79. [DOI] [PubMed] [Google Scholar]
- 18.Curtin HD. Congenital malformations of the ear. Otolaryngol Clin North Am 1988;21:317-35. [PubMed] [Google Scholar]
- 19.Sennaroglu L, Saatci I. A new classification for cochleovestibular malformations. Laryngoscope 2002;112:2230-41. [DOI] [PubMed] [Google Scholar]
- 20.House HP. Differential diagnosis between otosclerosis and congenital footplate fixation. Ann Otol Rhinol Laryngol 1958;67:848-57. [DOI] [PubMed] [Google Scholar]
- 21.House HP, House WF, Hildyard VH. Congenital stapes footplate fixation: a preliminary report of twenty-three operated cases. Laryngoscope 1958;68:1389-402. [DOI] [PubMed] [Google Scholar]
- 22.House HP. Congenital fixation of the stapes footplate: hearing loss-problems in diagnosis and treatment. Otolaryngol Clin North Am 1969;2:35-51. [Google Scholar]
- 23.Lund WS. The surgery of congenital deafness. The Oxford, England series of 235 ears. Acta Otorhinolaryngol Belg 1988;42:5-11. [PubMed] [Google Scholar]
- 24.Scheer AA. Correction of congenital middle ear deformities. Arch Otolaryngol 1967;85:55-63. [DOI] [PubMed] [Google Scholar]
- 25.Plester D. Congenital malformations of the middle ear. Acta Otorhinolaryngol Belg 1971;25:877-84. [PubMed] [Google Scholar]
- 26.Rahbar R, Neault MW, Kenna MA. Congenital absence of the incus bilaterally without other otologic anomalies: a new case report. Ear Nose Throat J 2002;81:274-6, 278. [PubMed] [Google Scholar]
- 27.Henner R, Buckingham R. The recognition and surgical treatment of congenital ossicular defects. Laryngoscope 1956;66:526-39. [DOI] [PubMed] [Google Scholar]
- 28.Parsed U, Chin YH. Bilateral congenital absence of incus. J Laryngol Otol 1975;89:1265-9. [DOI] [PubMed] [Google Scholar]
- 29.Shea III JJ, Shea JJ, Orchik DJ, Emmett JR. Congenital absence of the incus: a novel method of reconstruction. Otolaryngol Head Neck Surg 1987;97:413-5. [DOI] [PubMed] [Google Scholar]
- 30.Sooy FA. The management of middle ear lesions simulating otosclerosis. Ann Otol Rhinol Laryngol 1960;69:540-58. [DOI] [PubMed] [Google Scholar]
- 31.Tolan JF, Wilson HL. Anomalies of the middle ear. Arch Otolaryngol 1958;68:384-7. [DOI] [PubMed] [Google Scholar]
- 32.Wehrs RE. Congenital absence of the long process of the incus. Laryngoscope 1999;109:192-7. [DOI] [PubMed] [Google Scholar]
- 33.Escher F, Hirt H. Dominant hereditary conductive deafness through lack of incus-stapes junction. Acta Otolaryngol (Stockh) 1968;65:25-32. [DOI] [PubMed] [Google Scholar]
- 34.Funasaka S. Congenital ossicular anomalies without malformations of the external ear. Arch Otorhinolaryngol 1979;224:231-40. [DOI] [PubMed] [Google Scholar]
- 35.Hough JVD. Incudostapedial joint separation: etiology, treatment and significance. Laryngoscope 1959;69:644-64. [DOI] [PubMed] [Google Scholar]
- 36.Boone R, Dornhoffer J. Stapedotomy above the facial nerve in a congenitally malformed ear: a case report. Otolaryngol Head Neck Surg 2002;127:342-5. [DOI] [PubMed] [Google Scholar]
- 37.Caparosa RJ, Klassen D. Congenital anomalies of the stapes and facial nerve. Arch Otolaryngol 1966;83:420-1. [DOI] [PubMed] [Google Scholar]
- 38.Gundersen T. Congenital malformations of the stapes footplate. Arch Otolaryngol 1967;85:171-6. [DOI] [PubMed] [Google Scholar]
- 39.Teunissen B, Cremers WR, Huygen PL, Pouwels TP. Isolated congenital stapes ankylosis: surgical results in 32 ears and a review of the literature. Laryngoscope 1990;100:1331-6. [DOI] [PubMed] [Google Scholar]
- 40.Cole JM, Bartels LJ, Beresny GM. Long-term effect of otosclerosis on bone conduction. Laryngoscope 1979;89:1053-9. [PubMed] [Google Scholar]
- 41.Cole JM. Surgery for otosclerosis in children. Laryngoscope 1982;92:859-62. [PubMed] [Google Scholar]
- 42.De la Cruz A, Angeli S, Slattery WH. Stapedectomy in children. Otolaryngol Head Neck Surg 1999;120:487-92. [DOI] [PubMed] [Google Scholar]
- 43.House JW, Sheehy JL, Antunez JC. Stapedectomy in children. Laryngoscope 1980;90:1804-9. [DOI] [PubMed] [Google Scholar]
- 44.Robinson M. Juvenile otosclerosis. A 20-year study. Ann Otol Rhinol Laryngol 1983;92:561-5. [DOI] [PubMed] [Google Scholar]
- 45.Vincent R, Oates J, Sperling NM. Stapedotomy for tympanosclerotic stapes fixation: is it safe and efficient? A review of 68 cases. Otol Neurotol 2002;23:866-72. [DOI] [PubMed] [Google Scholar]