

“I should like, in my old age, to be involved, by a group of young people, in their activities, in choral work, in which also an old man could be useful, if for nothing else but to tell stories and remember History”
V. Andreoli
Dear Colleagues, Ladies and Gentlemen,
In one of his more recent books entitled “Letter to an Adolescent”, the well-known psychiatrist Vittorino Andreoli expresses his wish, cited here, a wish with which I whole-heartedly agree. Thus, I accepted, with great pleasure, the invitation to introduce the topics of the Meeting delivering a speech of a historical nature, first of all because Dr. Franzetti invited me, second because the topic is related both to stories and to History, which is apt for a person of my age. For a Lecture, with an informal and personal touch, somewhat unlike those usually presented on these occasions, which are full of dates and names, I plan to speak about events in Otology during the second half of the 20th Century, attempting, at the same time, to tell you about the people I have known, the events I have witnessed. The 40’s and 50’s were the crucial years for the change from the old to new Otology; I spent that era on the stage of the most important Italian ORL Clinics of the time, that of the University of Milan, a forerunner of those changes.
Audiological diagnostics
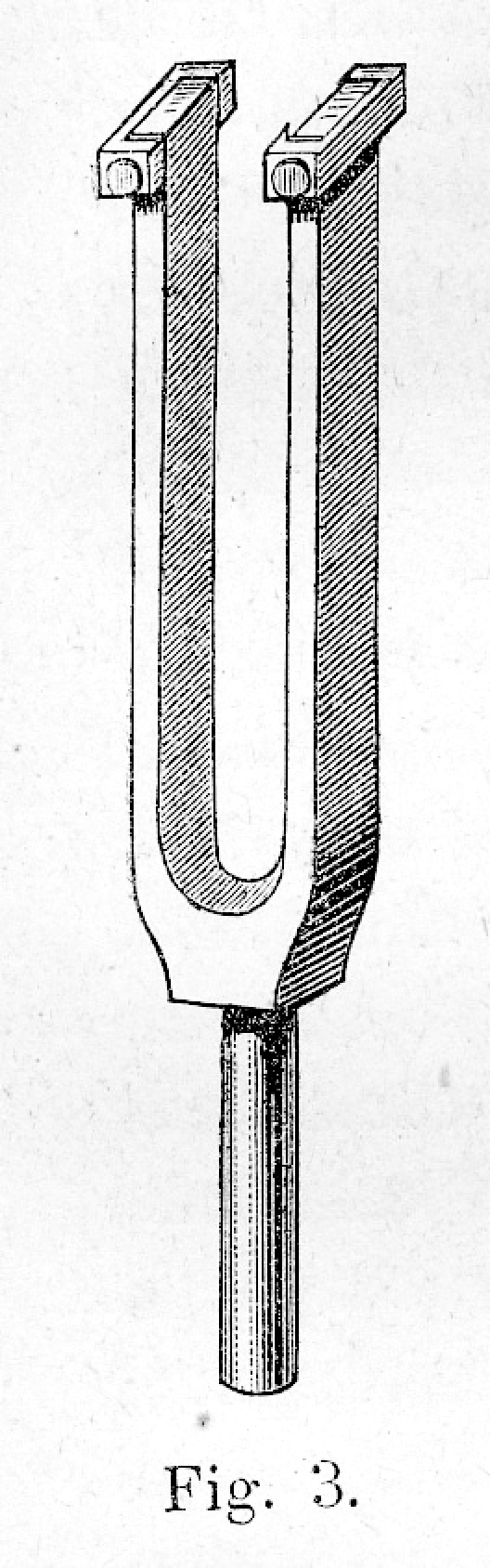
At the end of World War II, when I first began to take an interest in Otorhinolaryngology, diagnosis of hearing loss was still based, for the quantitative evaluations, on the use of a whispering or spoken voice and a watch, and, for a qualitative evaluation, on the use of a tuning fork (Fig. 1). There were also other instruments: Politzer’s acumeter (Fig. 2). Galton’s whistle (Fig. 3) which emitted tones > 6000 Hertz, Struycken-Schaefer’s monochord, a kind of violin to assess the upper limit of hearing, but these were less frequently employed. Cochlear reflexes were studied: cochlear-phonatory reflex (Lombard’s test), cochlear-eyelid (for newborns) or galvanic reflex for assessment of the eighth nerve. Tube function was evaluated by means of Politzer inflator and with Valsalva’s manoeuvre.
Fig. 1.
Tuning fork.
Fig. 2.
Politzer’s tuning fork.
Fig. 3.
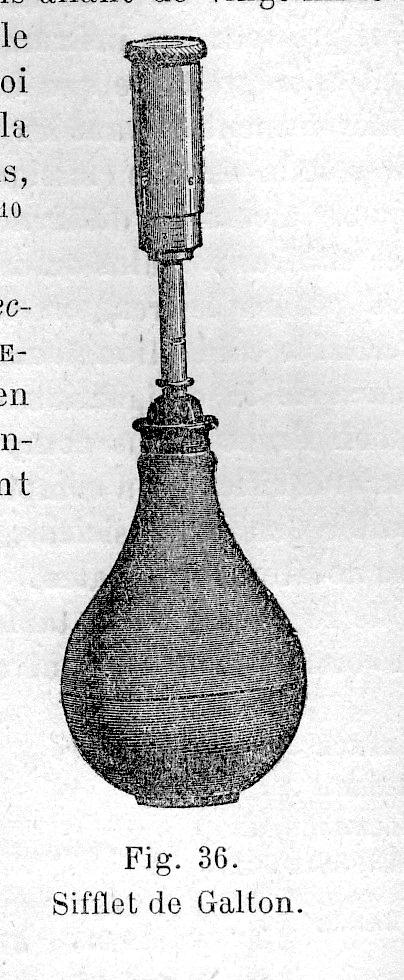
Galton’s whistle.
Audiometers already existed having been imported from America, electronic instruments which produced pure tones, enabling quantitative and qualitative examinations of hearing function to be carried out simultaneously, but they were to be found in only a few of the more important hospital centres and were used to integrate the above-mentioned instruments, particularly the tuning-fork. The need began to be expressed to carry out hearing assessments in a soundproof cabin, but very few research centres actually had one. In the ORL Division of the Ospedale Civile in Venice which I attended as a student, hearing function was assessed in the outpatient department, with the patient at a distance of five or six metres from the physician for the voice test. The examination with the tuning-fork was integrated with the detection of the Schwabach, Bing, Rinne, Weber and Gellè signs, requesting all those present to remain silent.
The audiometer was in a separate room, but was used in special cases. The manufacturer which had supplied the instrument was MAICO, Head of which was Dr. Buchwald who, every so often would make his presence felt either with a telephone call or by sending his consultant, Dr. Azzo Azzi with the intent to have us purchase the soundproof cabin imported from Minneapolis (Minnesota), USA.
If we look at documents of the end of the 1800’s-early 1900’s, for example, the “Manuale di Otologia” prepared by V. Grazzi in 1886 (Fig. 4) or the “Précis des Maladies de l’Oreille, du Nez, du Pharynx et du Larynx” by M. Lannois, 1908, or again the small volume “Otites et surdités de guerre” written by H. Bourgeois and M. Sourdille in 1917, we will find very similar descriptions to those mentioned above as far as concerns the methods used in investigations on hearing function at that time. The electronic audiometer had not yet been invented, however electro-telephonic audiometers existed (combination of a tuning-fork, as the source of sound, and of a telephone as the means of transmission), one of which was that of Cozzolino (Fig. 5). These instruments were, however, more for the personal use of the inventor than for generalized use. The first electronic audiometers were used in America during the period of the First World War, particularly in the care of the military.
Fig. 4.

The Manual prepared by V. Grazzi, 1886.
Fig. 5.

Cozzolino’s electro-telephonic audiometer.
But let us go back to that mythical era of World War II. From the United States, which had become the most qualified core of scientific and technical research, we began, through scientific journals and the early congresses, to receive news in Europe about the latest studies on the physiology of hearing.
On the strength of this, L. Fiori-Ratti, a Clinician, and A. Manfredi, an Engineer, both from Rome, presented an Official Report, entitled “Electrophysiology of Hearing”, at the 36th Congress of the Italian Society of ORL, held in Genoa, October, 1947, thus bringing to the attention of Italian specialists in ORL, the state of the art of the most advanced American experimental research and stimulating the clinicians’ interest in eventual practical applications of the US results. They discussed the masking effect of sound, hearing fatigue due to prolonged exposure of the hearing organ, of cochlear potentials, the cochlear microphonic effect, nerve and trunk potentials, electrical activity of the cortex and names were mentioned that, for my generation, were irreplaceable reference points: Wever and Bray, Adrian, Davis and Saul, Hallpike, Lorente de Nò, von Békésy. This was a completely new way of interpreting the physiology of hearing which was to take the place of the old theories of Helmholtz.
At this point, allow me to make a personal comment which will help to understand how I was able to become a direct witness of the enormous transformations that were taking shape, at that time. I got my degree in 1948 and, at that point, Professor Fausto Brunetti, Head of the ORL Unit of the Hospital in Venice said to me, words to the effect: “I am old and my appointment as Head is coming close to the end; you are young and you need to be part of a stimulating atmosphere. There is one such place in Italy: the ORL Clinic of the University of Milan, of which my friend Luigi Pietrantoni (Fig. 6) has just been appointed Head and he is, at present, the best Otorhinolaryngologist in our country. You should transfer to Milan, enrol in the Specialization School, follow the Course and learn the very most of what that place and that Maestro can give you”. That was how it came about and from then on was the start of that very exciting period of my professional and human formation which lasted until 1960, the year that marked the premature death of the Maestro.
Fig. 6.
Professor Luigi Pietrantoni.
Ettore Bocca and Carlo Agazzi were the right and left arm of Prof. Pietrantoni. Bocca was literally bursting all over with geniality, Agazzi was the expression of rationality and order. The Clinic was divided into various Services, a complete Department ante litteram, a Head was appointed responsible for each Service. Bocca was responsible for the Audiology Service, which had been called by the name of another Maestro from the Milanese School: Francesco Lasagna, a study and research centre that, in little more that ten years, was to produce results of world renown. I was, therefore, bound by great admiration and friendship to those colleagues that worked with Bocca: Amedeo Pellegrini, Giulio Pestalozza, Giovanni Zanotti, Carlo Calearo and, later, Giampiero Teatini and Antonio Antonelli. In the Audiology Service, there were the Maico audiometer, Peters imported from England and commercialised by Acousticon belonging to Engineer Otello Giovacchini, the Elit developed by Engineer Savelli and distributed by Amplifon belonging to Engineer Charles Holland; there was also Manfredi’s audiometer which worked with steps of one db, whilst all other audiometers had steps of 10 db, offering a scrupulous evaluation of hearing function. An excellent piece of equipment both for routine use and research. It was there that I learned the techniques to differentiate transmission deafness, perception deafness and mixed forms, the significance of recruitment described by Fowler in 1936 and the proof to be able to reveal it, the masking etc.
A large number of research projects were carried out by that group of great brains, allow me to recall some of the most important:
vocal audiometry with the first lists of phonetically balanced words and the logatomi (fragments of senseless words), which were added to the tonal audiometry;
study of central deafness based upon the use of lists of phrases pronounced with accelerated voice, with a distorted voice (by means of various big or low pass filters), the interrupted voice, prepared in order to make the perception of the spoken messages more difficult.
Pestalozza, who in 1954 had gone to work with H. Davis in Saint Louis and where he remained for one year, published an article in the American Journal of Physiology entitled Electric responses of the guinea pig ear to high audio-frequencies, after which he presented an official report on The adapting phenomena of the hearing apparatus presented together with E. Pirodda at the meeting of the Italian Society of Phonetics, Phoniatrics and Audiology, in 1960. He also carried out studies on professional deafness for the European Community of Coal and Steel, a topic that was later to be made into a film.
A Course on Audiology was held in the Clinic, in 1951, with an international cast of Professors. The lessons were later published, the topics ranging from the physiology of hearing to audiological diagnostics and surgical treatment of otosclerosis.
Meanwhile, paediatric audiometry had appeared on the scene. This was particularly important for the diagnosis of severe deafness in children. Games including sound were used, the Borel-Maisony test without words, the Dix and Hallpike test, the so-called peep-show and, when possible, even von Békésy’s objective audiometry. Later, the Boel test came into general use for children up to 10 months of age, conditioned reflex audiometry with the Suzuki and Ogiba theatre, and objective audiometry by measuring impedance and assessment of evoked potentials. Besides individual examinations, collective examinations were introduced which took place in the nursery and junior schools with the use of various tests: Massachusetts hearing test, Balayage des frequences, and others.
The various steps in the following stages of audiologic diagnostics included: assessment of acoustic impedance, recording of evoked potentials at nerve and trunk levels, evaluation of acoustic otoemissions.
Acoustic impedance
One of the first authors to focus on the detection, for diagnostic purposes, of resistance to the transmission of sound across the structures of the middle ear, was Ernest Gellé who, in the second half of the 1800’s, contributed with his test to make the diagnosis of otosclerosis easier. K. Terkildsen and K.A. Thomsen in Copenhagen (1959) were the first to describe the reliable tympanograms; this was followed by the realisation of the first impedancemeters for clinical use thanks above all to Scandinavian authors (1960). These began to be used in the differential diagnosis between the various disorders of the middle ear. Tympanogram findings and stapedial reflex then became part of the routine diagnostic workup in every ORL outpatient unit.
Evoked potentials
As far as concerns evoked potentials, studies first began at the time of research on the electrophysiology of hearing and the first practical applications date back to the 70’s. This technique is currently used in the diagnostic workup of hearing disorders of peripheral and central pathways.
Acoustic otoemissions
Acoustic otoemissions were first mentioned in 1978, when Kemp discovered that the external ciliate cells possess a spontaneous electric activity (thus quite independent from the action of a sound stimulation, as occurs with the cochlear microphonic effect), detectable with the proper recording techniques. In the 1980’s, this phenomenon was adopted for practical diagnostic purposes in the study of cochlear lesions (toxic, traumatic or metabolic applications) and was used in particular in the screening of deafness in infants. Acoustic otoemission findings are also used in adults to monitor progressive cochlear impairments.
Treatment
As already mentioned, once the way had been paved for the diagnostic work-up of hearing loss, the development then began, immediately after the end of World War II, of medical and surgical treatment, thanks to the discovery of antibiotics, cortisone, anti-histamines, mucolytics etc. and the use of the surgical microscope.
The discovery of penicillin was followed by that of streptomycin, aureomycin, terramycin, bacitracin. The pharmaceutical industry was first engaged in the production of these substances by means of fermentation, and thereafter by means of synthesis, producing, by means of molecular modifications, drugs with a wider range of use or with a delayed action or improved biodisponibility. An identical process of chemical manipulation was applied to cortisone, the anti-histamines and the mucolytics, of which I should like to recall the forerunners: trypsin and chymotrypsin produced by Sieroterapico Milanese, in the study of which we contributed personally.
Thanks to these discoveries, the picture of infectious diseases underwent substantial changes: the acute forms were generally resolved, as well as the recurrence of the chronic forms. The eso- and endo-cranial complications which, in the past, had had a marked adverse effect on the fate of the patient and, from a professional viewpoint, was the most interesting and complex field of this specialty, rapidly disappeared. However, the situation that emerged, if, on the one hand, had reduced the contents of the specialty, had, on the other, created the favourable conditions to better study and extend this practice to other fields which, until then, had been neglected: vascular, degenerative and neoplastic disorders, the incidence of which, in the meantime, had increased.
In the field of ORL, an important technical tool first appeared on the scene at the end of the 40’s which was to have a great influence on the surgical aspects of this specialty, namely the Zeiss surgical microscope. This instrument (which offered the possibility of enlarging the surgical field reaching 40 diameters and presented a mean focal distance of 25 cm), together with the antibiotics used to fight infection, enabled otological surgery to adopt a functional approach, i.e., respecting the residual anatomic structures of the ear which were no longer treated as components of a chronic inflammatory process to be totally removed, but were conserved according to their integrity and function. A new era was about to begin.
Serous otitis media
One pathological condition upon which attention was focused, at that time, was catarrhal otitis media or gelatinous (glue ear), particularly in childhood: a pathological disorder with serious consequences, even tympanosclerosis. This disease had been treated in the past using the Politzer inflator, tubal catheterisation, inhalation therapy. Now, treatment was taking on new characteristics, with studies focusing on the immunology, physiology and pathophysiology of tympanic tube drainage which had, in the meantime, been introduced. Modern pharmacological therapy included thermal treatment (inhalation, nebulization, humage, crenotherapy), corticosteroids, mucolytics, decongestive antihistamines. As from 1954, if the case was not resolved, B.W. Armstrong proceded with surgical evacuation of the middle ear fluid and permanent drainage by means of a small tube introduced by paracentesis. This was left in situ for several months. This surgical procedure was widely used in the 70’s; it was later criticised as being the cause of tympanic alterations. According to Pestalozza, who, for many years, was Director of the Paediatric Otorhinolaryngology Unit of the Children’s Hospital in Milan, the earlier the procedure was performed, and the closer the child’s age was within the 3-7 years range, the better the long-term results. The treatment, as already mentioned, should be associated with pharmacological support.
Surgery in otosclerosis
Labyrinthine fenestration
The era of surgery for deafness began in the 30’s, with the attempts at labyrinthine fenestration, for otosclerosis, by Holmgren and his pupil Sourdille. Sourdille was a Lecturer at the French Congress of ORL, in 1935, speaking on the surgical procedure of fenestration of the horizontal semicircular canal and covering the fistula with a tympano-meatal flap. Surgery was performed in two steps. It was Lempert, in 1938, who defined the fenestration technique and in one stage only, displacing, as far as possible, the opening towards the ampulla, a technique which was to become adopted throughout the world. Shambaugh, Popper, as well as others, made slight changes to the procedure. Pietrantoni, in order to avoid serrous labyrinthitis associated with closure of the window with the tympano-meatal flap, soon began to use a free flap according to Thiersh. Thiersh flaps were also used to cover the mastoid cavity as this was often the cause of suppuration.
The first labyrinthine fenestrations in Italy were performed with the loupe, magnifying glasses, but the Zeiss microscope soon appeared and the technique immediately became not only more precise but also more elegant This reminds me of a small anecdote: one day, while Prof. Pietrantoni was performing surgery for otosclerosis, I was standing directly behind him watching the movement of his hands. At a certain point, the Professor raised his eyes from the microscope and with the expression of a person clearly satisfied with the work he was doing, said: “There you are, Otorhinolaryngology has overcome its past history of surgery of suppurations and clumsy handling, to become a technique of precision in a sterile field, with elective indications. This is a great step forward achieved by our Specialisation”. Whilst until then, the otosclerotic patient had been advised to postpone surgery for fear of a deterioration in the hearing function, he/she was now being advised to attempt surgery in order to regain the function. And, besides otosclerosis, chronic otitis was taken into consideration, as well as other pathological conditions related to the ear and thus new techniques in the field of functional surgery began to be invented. But a completely new approach was about to revolutionize the surgical treatment of otosclerosis: i.e., stapes surgery.
Stapes surgery
The first attempts at stapes surgery date back to the 19th Century. There was the procedure of stapedectomy according to Kessel (1876), drilling of the promontorium of Passow (1894), paracentesis of the round window of our own De Rossi (1882) albeit the lack of fine surgical instruments, but above all the risk of suppurative complications at labyrinthine and meningeal level, had prevented the development and widespread use of these techniques. Stapedectomy was later used again, in Italy, by Faraci, Masini and later also by Cornelli, but always with disappointing results because these authors left the oval window open and did not ensure continuity of the chain. The procedure could not, therefore, lead to a functional improvement in the patient and could become the cause of infection of the inner ear, leading to total deafness. Albeit, at the end of the 40’s, an American, Samuel Rosen, proposed a new operation, respecting the anatomical integrity of the chain: the mobilisation of the stapes and went around the world several times to promote the technique. When he was cordially approached by people, he would give them a small model of the stapes made of synthetic material (Fig. 7).
Fig. 7.

A model of S. Rosen stapes.
Rosen’s procedure was criticized because, after a few months, the stapes again became blocked, but this stimulated improvements of otosclerosis surgery by way of the oval window.
After this mobilization, total stapedectomy followed by closure of the window with flaps from various sites (vein, perichondrium) and effecting continuity, between the flap and the long incus apophysis by means of insertion of a small tube made of synthetic material. The last step of the stapedectomy technique was a procedure, still widely used to-day, limited to removal of the branches of the stapes, to perforation of the foot plate, introduction of a small piston made of teflon connected to the long apophysis of the incus. In expert hands, this procedure is performed in 15-30 minutes.
Chronic otitis surgery
The widespread use of antibiotics, as already pointed out, has drastically modified the pattern of this disorder and increased, in a totally unexpected fashion, the possibility of performing surgery. Acute otitis was resolved in just a few days and complications related to otitis almost totally disappeared from the clinical panorama. Mastoidectomy, from a routine procedure, became a rare occurrence while procedures for other complications, such as petrositis, meningitis, cerebral abscess and thrombophlebitis, etc. became exceptional.
In the first half of the Century, surgery performed for chronic purulence of the ear consisted in a procedure aimed at petro-mastoid emptying, also referred to as radical (Stake’s operation) which, since it was radical, did not take into consideration the damage caused to the function. Also limited procedures existed: atticotomy, ossiculectomy, but indications were rare. After the war, the term conservative radical began to be used. Caliceti and Pietrantoni, at the “International Medico-Surgical Meetings” in Turin, in 1951, spoke of their early results of function-sparing surgery. But the big change came immediately afterwards with Zollner and Wullstein who proposed to the international otological world, the tympanoplasty procedure (TPL). This was to be the beginning of a conceptual revolution: stop indiscriminately attacking the ear without paying attention to the function! It was necessary, instead, to focus on preserving the structures of the middle ear that could be saved, in order to reconstruct with the precision of a watchmaker, a container which was to be in as functional as possible! It is the duty of the otologist, prior to any surgical manoeuvre on the ear to check for the presence of adenoid tissue, chronic tonsillitis, nasal stenosis etc, attempting to eliminate them in order to re-establish conditions of passage through the tubo-tympanic area. It would be worthwhile making the insertion test, in the preliminary audiological investigation, as this is the only manoeuvre able to reliably predict the functional outcome of the operation.
Five types of TPL were initially proposed by Wullstein:
Type I = Myringoplasty;
Type II = Tympanoplasty with integral and functioning chain;
Type III = Tympanoplasty with discontinuous chain, but with mobile stapes;
Type IV = Tympanoplasty with discontinuous chain and damaged or absent stapes, which can be resolved with small middle ear cavity surgery including the oval window, both free and mobile;
Type V = Tympanoplasty with discontinuous chain and no stapes, which can be resolved with a small middle ear cavity introduced at the lower edge of the oval window and fenestration on the lateral semicircular canal.
During those years, Willstein came several times to our Clinic in Milan to promote his personal procedure, enjoying the opportunity not only to witness the appreciation demonstrated by the Italian colleagues but also to become better acquainted with their experience.
After those early years, in about 1954-55, the TPL operation was simplified as outlined below:
TPL with continuous chain;
TPL a discontinuous chain with stapes present and mobile onto which a bone fragment is introduced in order to regain the size of the earlier middle ear cavity considered to be a fundamental condition for a successful operation;
TPL with no stapes and attempt to achieve myringo-platinopexy.
It became obvious that the key to success of TPL was to maintain a sufficiently large and aerated middle ear cavity; thus in the event of destruction of the chain, every effort had to be made to reconstruct it, even simplifying it. An interesting and useful discovery in those years of surgical activity was the identification of the spontaneous TPL. This event is, sometimes, associated with the presence of cholesteatoma, which in its process of growth is able to modify, in various ways, the relationships between the structures of the middle ear, giving rise to a variety of anatomical and functional changes. Use of the small middle ear cavity was completely abandoned since it ended in tympanosclerosis. Myringoplasty proceeded with various solutions, as far as concerns both the type of approach, and the materials used. The technique was brought to perfection and the underlay and overlay techniques appeared.
But the need to tidy up the TPL techniques after the 50’s and 60’s led to the report that Clerici, Felisati, Pellegrini and Pestalozza presented in Fiuggi, at the XXI AOOI National Congress in 1968, entitled “Present clinical and surgical aspects of chronic purulent otitis media”. Attention was focused, together with other aspects, on the problem of the open technique and the closed technique (Jansen), which had later given rise to discussion, together with the problem of surgery of the angle of the antrum threshold. During those years, it had emerged that purulence of the mastoid cavity, widely open and drained externally, was present in almost 50% of the cases operated and the solutions with flaps of varying origin (skin, periostium) were unable to modify the prognosis.
In the years that followed, several reports and papers focused on the topic of functional surgery in chronic otitis: E. Bocca et al. on Tympanosclerosis in 1969, C. Zini in 1972 on Transplants and implants in ORL, M. De Benedetto on Myringoplasty in 1996, C.A. Leone in 1999 on Cholesteatoma Surgery and the AOOI publication in May 2004 by C.A. Leone on Tympanoplasty, as well as the numerous and admirable publications in journals and communications at Congresses.
Surgery of VIII nerve
In the second half of the 20th Century, attention was focused on other aspects of functional surgery, together with that of chronic otitis: Malformations of the ear which involved also the plastic surgeons, but due to the limited number of cases, it became a marginal topic. Great interest and energy was applied, on the other hand, to surgery of the VIII nerve. H. Cushing and W.E. Dandy had already dealt with this procedure, in the neuro-surgical setting, in the period between the two wars; Olivecrona dedicated his attention to this area after the war. The aim was to cure the neoplastic pathology of the nerve. In 1959, William House in Los Angeles, as an otologist, focused attention on the VIII and VII nerves (neoplasias, particularly neurinoma in the otologic phase, peripheral vestibular vertigo, paralysis of the VII), initiating surgery of the internal hearing canal, by way of the transmeatal, retro-labyrinthine, trans-labyrinthine access. House published two treatises on these topics in 1964 and 1968. He can, therefore, be considered the founder of internal hearing canal surgery, which was soon extended to the ponto-cerebellar angle. Thus Oto-neuro-surgery was born. In Italy, in the 70’s, Antonio Mazzoni, a pupil of Bocca, in Ferrara, after a two-year stay in the United States, in Los Angeles with House and in Memphis with J. Shea, practised and promoted this procedure, creating a school which continues his work. His Report at the 64th National Congress of the Italian Society of ORL (S.I.L.O.R.), in S. Margherita Ligure in 1977, entitled: Internal hearing canal surgery - clinical and diagnostic aspects is the first important contribution of the Italian School on this topic. Mazzoni was joined by C. Zini, M. Sanna, as well as others, who brought, not only to Italy, but also abroad, the fruits of their research and personal experience in this new area of O.R.L. surgery. In Milan, in one of the Meetings of the Centro Studi e Ricerche L. Pietrantoni, which we organized in 1989, Iannetta, from USA, gave a Lecture on Neuro-vascular conflicts.
Cochlear implants
Our excursus on otologic surgery in the 20th Century comes to a close focusing on a conquest that we have witnessed over the last 10 years, namely, cochlear implants. At the World Congress of ORL organized by M. Arslan and held in Venice Lido, in 1973, W. House addressed the Meeting at Palazzo del Cinema, giving the Opening Session on the first monocanal cochlear implants which he personally had performed. The participants were absolutely fascinated and, at the same time, perturbed by such courage and by the problems those early operations had caused. Many years have passed since then and a lot of ground has been covered: the multi-channel cochlear implants now play a well-deserved part in the more sophisticated techniques used in otological rehabilitation surgery. Yet another evolution was applications of the implants at midbrain level. At present, for the transmissive forms, osteo-integrated implants are used which appear to offer a valid alternative to the traditional prosthesis. At the same time, a logopedic re-education method was being developed which, associated with the implant technique, improved the functional outcome, resulting in this procedure becoming a first choice tool in the rehabilitation programme of children presenting severe deafness.
Prevention and rehabilitation
In post-war Italy, social medicine, took a great step forward. Means became available to combat infectious diseases, work-related disorders, hereditary and congenital conditions and there were already talks of prevention of tumours and degenerative diseases. The concept of prevention was better defined by way of a description of the three components: primary, secondary and tertiary. Rehabilitation, thanks also to the possibilities offered by electronic devices, led to the availability of new instruments for the restoration of the impaired function.
In the otological field, a whole series of steps were taken, aimed at the prevention of hearing defects in children, related especially to pre- and post-natal disorders, and, in the adult, disorders related primarily to lesions caused by noise (occupational deafness).
In 1945, the ORL Clinic in Turin, started a dépistage campaign for deaf children, by means of screening in schools. The local authorities in Milan and several other areas in Lombardia, Veneto, Emilia-Romagna, as well as other Regions, set up a similar campaign, offering suitable support and organizing meetings for this type of activity.
In 1954, G. Moretto reported interesting epidemiological data on the percentage of hard-of-hearing cases in the population: this was evaluated, at that time, to be approximately 5-6%, with even considerable differences related to the area, social status of the population examined, etc. Over the next few years, this percentage dropped to around 2-3%, thanks to the campaign for the prevention of genetic and congenital deafness, to improvements in living conditions, to the early diagnosis of the disorders and the improvement of the rhinopharyngeal status. The percentage of severely deaf children, destined to become deaf and dumb, remained at approximately 1% and even less. Together with Marialuisa Marenzi, Responsible for the Audiological Centre for Infants of the City and Province of Milan, we took part, in 1969, in the Congress “Social and Preventive Medicine Services”, a joint promotion by the Authorities of the Provinces of Lombardia, Piemonte, Liguria and Veneto, presenting a Lecture referring to our personal experience in this field. In 1980, Amedeo Pellegrini held a Meeting, in his hospital in Saronno, on “Duties and organisation of an Audio-phonology Service for the Local Health Unit during which the Audiological Clinic of the University of Milan, presented a project for the organization of an Audio-phonological Service for a population of half a million inhabitants.
At that same time, collaboration was started with the Clinic for Work-related diseases, campaigns for: the screening of occupational deafness, the use of equipment to protect hearing; prevention of existing damage becoming more serious.
Coming back to the first post-war era, from where we began, it is worthwhile mentioning another step forward of a technical nature: the introduction of electronic acoustic prostheses. The carbon prosthesis of the early 1900’s, which had taken the place of the acoustic horns used in the 1700’s and early 1800’s (Fig. 8), were unable to offer sufficient amplification to correct a hearing deficit > 50-60 db. Distortion was so marked, at times, that it became unbearable for the patient; furthermore, these instruments were extremely cumbersome. Electronic amplification employed in the new prostheses, using high and low pass filters, reach an amplification of 60 db, with negligible distortion phenomena. At first, the dimensions of the prosthesis, were less than those of a packet of cigarettes, it was usually carried in the pocket of the patient’s jacket, Later, it was even reduced in size and it was possible to hide the amplifier behind the ear or in a pair of glasses. More recently, endoauricular prostheses have become available.
Fig. 8.
Ear trumpets (Y. Guerrier and P. Mounier-Kuhn).
A large of number of hard-of-hearing people, of all ages and regardless of the origin of the defect, have been able take advantage of the electronic prostheses. These also paved the way to the possibility to recuperate a severely deaf child with the new teaching techniques based upon the early use of binaural prostheses, on logopedic rehabilitation, as well as the chance for the child to attend a normal school. As already mentioned, the cochlear implants which first appeared in the early seventies, marked the beginning of a new era for the rehabilitation of deaf children, to the point that the old schools in which sign language was taught were no longer important and were used for other purposes. For example, in Padova, in 1958, the State Professional Institute for Industry and Craftmanship for the Deaf “Tommaso Pendola” in which a course for dental technicians was organized.
Dear Colleagues, Ladies and Gentlemen
Many years have gone by since 1948 when, after getting my degree, I transferred to Milan. I worked for 6 years as a Voluntary Assistant in the Clinic in Via Commenda. Upon the death of Professor Pietrantoni (1960), the School dispersed in the various hospitals in Lombardia. Despite the difficulties, I lived those years with great passion and dedication to my work. There were times when I felt hesitant but I also had great faith in the future, but, and above all, esteem and admiration towards the Maestro. Not many young people to-day would perhaps be prepared to make similar sacrifices, but the fault lies in the fact that times have changed: we had just come through the war years which had severely affected us from a socio-economic point of view and had left us with a country to be rebuilt. Young people today live in a well-to-do society and look to the future with few ideals and little hope. And maybe, the fault lies also with the Maestri who have failed to stimulate enthusiasm and energy in the young of today.
These are the reflections, in this is respect, of Professor Pietrantoni:
“Someone once reprimanded me for having big ideas, for envisaging work programmes that were too great for me. I accepted the scolding because my great desire to work, rather than a sin of presumption in my modest strength, is above all and first of all an act of deep faith in the young people around me, in their intelligence, their capacity to work and to achieve important goals, faith in the young which, in the School and in the Clinic, is rewarded every day by that sense of a life of fulfilment and fruitfulness that only they know how, and can, give”.
Lecture delivered at the Opening of the Congress “Understand and Live Deafness in the Third Millenium” organized by Dr. Andrea Franzetti, Head of the Otorhinolaryngology Division of the E. Bassini Hospital, Cinisello Balsamo – Milan, Italy and held at the Cosmo Hotel Palace in Cinisello Balsamo on 8th October 2004.
Selected Reading
Proceedings of a Meeting organized by the Unioni Regionali delle Provincie Lombarde, Piemontesi, Liguri e Venete on: “I Servizi di medicina sociale preventiva e l’articolazione territoriale della medicina pubblica nell’ambito della Regione”. Milan, 28-30 November, 1969.
- Arslan M. Otorinolaringoiatria. Padua: Ed. CEDAM; 1945. [Google Scholar]
- Aubry M. La chirurgie de la surdité. Paris: Ed. Masson; 1959. [Google Scholar]
- Bourgeois H, Sourdille M. Otites et surdités de guerre. Paris: Ed. Masson; 1917. [Google Scholar]
- Burdo S. Impianto coclearie multicanale. Milan, Paris, Barcellona: Ed. Masson; 1994. [Google Scholar]
- Calogero B. Audiologia. Bologna: Ed. Monduzzi; 1983. [Google Scholar]
- Del Bo M. Manuale di Audiologia. Milano: Ed Masson Italia; 1980. [Google Scholar]
- Fiori Ratti L, Manfredi A. Elettrofisiologia dell’udito. Relazione Ufficiale al XXXVI Congresso della Soc. It. di Laring. Otol. e Rinol., Genova, 24-29 October, 1947. [Google Scholar]
- Grazzi V. Manuale di Otologia. Florence: Carlo Collini; 1886. [Google Scholar]
- Lannois M. Précis des Maladies de l’oreille, du nez, du pharynx et du larynx. Collection Testut, Ed. Paris: Octave Doin; 1908. [Google Scholar]
- Guerrier Y, Mounier-Kuhn P. Histoire des maladies de l’oreille, du nez e de la gorge. Paris: Dacosta; 1980. [Google Scholar]
- Moretto G. Nozioni di Audiologia. Turin: Libreria Ed. Univ., 1954. [Google Scholar]
- Moure J, Liébault G, Canuyt G. Technique chirurgicale oto-rhino-laryngologique. L’oreille et ses annexes. Paris: O. Doin; 1922. [Google Scholar]
- Motta G. La protesizzazione acustica oggi. Centro Ricerche e Studi Amplifon; 1988. [Google Scholar]
- Pellegrini A. Compiti e organizzazione di un Servizio di Audiofonologia per il Territorio di una USSL. Milan: Ed. Amplifon; 1980. [Google Scholar]
- Pestalozza G, Cusmano G. Trattamento chirurgico dell’otite media secretiva a timpano chiuso. In: Catalano GB, Pinelli V, editors. Problemi di chirurgia otologica in età pediatrica. Relazione al V Congresso Società Italiana di Otorinolaringologia Pediatrica, Catania 5-7 dicembre 1980. Rome: Luigi Pozzi; 1980. [Google Scholar]
- Pietrantoni L. Nuovi sviluppi e nuovi orientamenti della Clinica Otorinolaringologica. Prolusione al Corso di Clinica ORL all’Università di Milano, 30 January, 1950. Arch It ORL 1950. p. 214-33. [PubMed] [Google Scholar]
- Pietrantoni L. La moderna concezione dell’Audiologia. In: Corso di Audiologia tenuto all’Università di Milano, 13-21 January, 1951. Milan: IDOS (Istituto Milano per la diffusione di opere scientifiche); 1951. p. 3-11. [Google Scholar]
- Pietrantoni L. Il trattamento chirurgico dell’otosclerosi. In: Corso di Audiologia tenuto all’Università di Milano, 13-21 January, 1951. Milan: IDOS (Istituto per la diffusione di opere scientifiche); 1951. p. 393-423. [Google Scholar]
- Quaranta A. Epidemiologia dei problemi uditivi nella popolazione adulta in Italia (EPUPAI). Dal Centro di Audiologia e Otologia, Università degli Studi di Bari/Centro Pilota di Audiologia e Otologia per i Paesi dell’Area del Mediterraneo, Bari. [Google Scholar]
- Sperati G, Felisati D. Mostra di strumenti d’epoca riguardanti la storia dell’Otorinolaringoiatria. Roma: 90° Congresso Nazionale della Società Italiana di Otorinolaringoiatria e Chirurgia Cervico-Facciale; 28-31 May, 2003. [Google Scholar]
- Willemot J, Dafydd Stephens S. L’impedancemetrie. In: Willemot J, editor. Histoire de l’ORL. Acta Belgica 1981;35:(Suppl IV)1417. [Google Scholar]