

Abstract
We examined the feasibility of brief outpatient detoxification as a treatment for prescription opioid (PO) abusers. Fifteen PO-dependent adults were enrolled to receive buprenorphine stabilization, a 2-week buprenorphine taper, and subsequent naltrexone for those who completed the taper. Subjects also received behavioral therapy, urinalysis monitoring, and double-blind drug administration. Subjects provided 83.8%, 91.7% and 31.2% opioid-negative samples during stabilization, taper and naltrexone phases, respectively. Inspection of individual subject data revealed systematic differences in whether subjects successfully completed the taper without resumption of illicit opioid use. Post-hoc analyses were used to examine the characteristics of subjects who successfully completed the taper (Responders, n=5) versus those who failed to do so (Nonresponders, n=9). These pilot data suggest a subset of PO abusers may respond to brief buprenorphine detoxification, though future efforts should aim to improve outcomes, investigate individual differences in treatment response and identify characteristics that may predict those for whom longer-term agonist treatment is warranted.
Keywords: Prescription opioid abuse, Oxycodone, Opioid detoxification, Buprenorphine, Naltrexone
1. Introduction
Abuse of prescription opioids (POs) has become a significant public health problem in recent years (Cicero et al., 2005; Compton & Volkow, 2006; Zacny et al., 2003). Incidence of abuse and dependence on POs, such as oxycodone (e.g., OxyContin®, Percocet®), hydrocodone (e.g., Vicodin®) and hydromorphone (e.g., Dilaudid®), increased by more than 400% between 1990 and 2000 (SAMHSA, 2003) and the most recent National Survey on Drug Use and Health reports that an estimated 5.2 million people abused POs in 2006 (SAMHSA, 2007a). These trends are not limited to adults; similar increases in PO abuse have been noted among adolescents and young adults (Johnston et al., 2002; McCabe et al., 2005a, 2005b, 2007; Sung et al., 2005). The alarming increase in PO abuse is also evident in data on drug-related emergency department (ED) visits. For example, PO-related ED visits increased by 408% between 1994 and 2002 (DAWN, 2003) and by 2006 they represented 33% of all drug-related ED visits (DAWN, 2007).
Perhaps not surprisingly, increases have also been noted in the number of individuals seeking treatment for PO abuse and dependence (Carise et al., 2007; Rosenblum et al., 2007; SAMHSA, 2007b). Despite this, the demographic and drug use characteristics and potential treatment needs of this group have gone largely unexamined. A position paper from the College of Problems on Drug Dependence highlighted the urgent need for both an improved understanding of PO abusers and development of effective treatments for this form of drug abuse (Zacny et al., 2003). Some early data have suggested that PO abusers may possess several demographic and drug use characteristics that may predict favorable treatment outcome, particularly as compared to historical groups of heroin users. For example, PO-dependent individuals may use a smaller amount of opioids daily and report a shorter duration of regular opioid use, later age of opioid-use onset, less intravenous drug use, less use of other drugs, and possibly greater social stability (Brands et al., 2004; Moore et al., 2007; Rosenblum et al., 2007; Sigmon, 2006; TEDS, 2004). Such differences in prior studies with drug abusers have been associated with more favorable treatment outcome (e.g., Alterman et al., 1997; Iguchi & Stitzer, 1991; Kampman et al., 2004; Preston et al., 1998; Soyka et al, 2008).
These data suggest that at least a subset of PO abusers may not require extended agonist maintenance in order to achieve abstinence from illicit opioids. If this is indeed the case, an initial effort at a relatively brief opioid detoxification in combination with antagonist and behavioral therapies may be a prudent course to investigate. The possibility of identifying a subset of the PO-abusing population who might be responsive to a taper rather than long-term maintenance would be a valuable contribution for several reasons. First, the increasing numbers of PO-abusing adolescents and young adults warrants exploring potential alternatives to long-term opioid maintenance, especially considering that recent research suggests that good outcomes can be obtained using brief opioid tapers with these younger patients (e.g., Marsch et al., 2005). Many PO abusers also are likely to shun agonist maintenance programs due to the stigma associated with them (Knudsen, 2007; Zacny et al., 2003), and maintenance treatments are highly restricted by federal regulation (SAMHSA, 2001) such that patients with less severe or brief opioid histories like those noted above may be ineligible for treatment. Finally, opioid maintenance programs can be difficult for patients to access in rural areas, which are also geographical regions where PO abuse is particularly prevalent (Cicero et al., 2007; O’Connor et al., 1997). While extended or maintenance therapies may eventually be deemed necessary for treating PO abuse, that should be determined empirically rather than assumed.
The present study represents a first step toward systematically developing and evaluating a brief outpatient detoxification for PO-dependent adults. Towards this end, buprenorphine was chosen as the detoxification agent. The partial mu-agonist has been used in numerous outpatient detoxification studies (e.g., Becker et al., 2001; Bickel et al., 1988; Diamant et al., 1998; Johnson et al., 1992; Kosten et al., 1989; Ling et al, 2005; Lintzeris et al., 2002) and has several features that lend toward its use in a detoxification paradigm. Buprenorphine is characterized by a long plasma half-life and slow dissociation from the receptor (Bullingham et al., 1980; Hambrook & Rance, 1976) and its discontinuation is associated with a more limited withdrawal syndrome relative to full agonists like methadone (Bickel et al., 1988; Fudala et al., 1990; Jasinski et al., 1978). In outpatient detoxification studies, buprenorphine also has produced rates of opioid abstinence and treatment retention that are favorable to clonidine (Ling et al., 2005; Lintzeris et al., 2002; Marsch et al., 2005; O’Conner et al., 1997) and comparable to methadone (Bickel et al., 1988; Gerra et al., 2004). Finally, PO abusers have been shown to respond favorably to buprenorphine treatment, showing increased treatment retention and opioid-negative urines when compared to heroin abusers (Moore et al., 2007).
Subjects in this study who completed the buprenorphine taper without resumption of illicit opioid use were subsequently transitioned to oral naltrexone. Naltrexone is a long-acting competitive opioid antagonist that, when taken regularly in sufficient doses, can block the reinforcing effects of opioids and markedly diminish or eliminate opioid self-administration and subjective effects (Gonzalez & Brogden, 1988; Martin et al., 1973; Mello et al., 1981). The ability of naltrexone to block the reinforcing effects of opioids was an important feature of this treatment in that it could provide protection for subjects should they have a lapse to opioid use following the taper. In anticipation of the challenges often associated with detoxification and naltrexone therapy (e.g., relapse to opioid use, poor adherence to naltrexone regimen), an intensive behavioral therapy based on the Community Reinforcement Approach (CRA) was provided as the platform counseling with all subjects. CRA was originally developed as an efficacious treatment for alcohol-dependent patients (Azrin et al., 1982; Hunt & Azrin, 1973) and has been demonstrated efficacious with cocaine- (Higgins et al., 2003) and opioid-dependent (Abbott et al., 1998; Bickel et al., 1997) outpatients. CRA also has been shown previously to enhance disulfiram therapy, which is another substance abuse treatment medication with a notoriously poor record of patient adherence (Azrin, 1976).
Overall, in this study we aimed to examine the feasibility of a brief outpatient detoxification to treat PO-dependent outpatients. The study included three general phases: brief buprenorphine stabilization (1-2 weeks), a 2-week buprenorphine taper, and subsequent naltrexone for those who successfully tapered. All participants received a platform of individual behavioral therapy and urine toxicology testing. While participants were not randomized into the 2-week taper condition and there was no control comparison group, this pilot trial did incorporate several methodological strengths with the aim of establishing these procedures prior to conducting a large-scale randomized trial. These included comprehensive assessment of opioid withdrawal (via self-report measures, observer ratings and pupillometer) and double-blind, double-dummy administration of study medications (i.e., provision of active and/or placebo forms of both buprenorphine and naltrexone throughout the duration study to minimize any influence of staff or participant expectations).
2. Materials and methods
2.1. Participants
Fifteen participants were recruited via mailings to local medical offices, flyers posted in the community, and newspaper advertisements. Eligible subjects had to be ≥ 18 years old, meet DSM-IV criteria for opioid dependence, provide an opioid-positive urine at intake, and be seeking or willing to accept opioid detoxification. They had to report a PO (e.g., oxycodone, hydrocodone) as their primary drug of abuse and be using the PO illicitly (e.g., without a valid prescription for a medical problem). Individuals who required ongoing opioid therapy for pain or other chronic medical conditions were excluded, as were individuals with an active psychiatric disorder that may interfere with consent or participation, with significant medical illness or those who were pregnant or nursing. The study was approved by the local institutional review board. Subjects were informed that, following a brief buprenorphine stabilization, they would receive a 2-week buprenorphine taper followed by a transition to naltrexone if they did not resume opioid use. Subjects also were informed of all other study procedures (e.g., double-blind dosing, withdrawal assessments, ancillary medications, urinalysis testing, behavior therapy and follow-up assessments). Each subject provided written informed consent prior to participating.
2.2. General procedures
The study was 12 weeks in duration (not including the initial 1-2 weeks of buprenorphine stabilization). Subjects attended the clinic daily until Study Week 6 when visits were reduced to thrice weekly (MWF). All subjects received individual behavioral therapy twice weekly and urinalysis testing thrice weekly (MWF) throughout the study. During stabilization, doses were titrated to achieve withdrawal suppression without intoxication or sedation using procedures based on recommended guidelines (Johnson et al., 2003). The mean duration of the stabilization phase was 12 (range 9-17) days and the mean ending stabilization dose of buprenorphine was 9 (range 4-16) mg.
Once stabilized, participants began the 2-week taper, during which buprenorphine dose reductions occurred in a graded fashion with the stabilization dose being decreased by 2 mg steps down to 2 mg, followed by a 1-mg dose, until 0 mg was reached by the end of Week 2. Throughout the study, non-opioid ancillary medications were made available to alleviate withdrawal symptomatology (e.g., clonidine, hydroxyzine, ibuprofen). Subjects who successfully tapered from buprenorphine and received placebo without relapsing were then transitioned to oral naltrexone therapy for the remainder of the study. To ensure safe induction without precipitating opioid withdrawal, subjects were required to provide an opioid-negative urine specimen and to self-report no opioid use in the past 24 hrs prior to initiating naltrexone therapy. Using the buprenorphine test strip (described below), it typically took 2-3 placebo doses before urine levels fell below the 10-ng/ml cutoff and were considered buprenorphine-negative. Induction onto naltrexone began with a low 12.5-mg dose on Day 1 of the naltrexone regimen, 25 mg on Days 2 and 3, and 50 mg on Day 4. Daily administration of 50 mg continued through Week 5 (Kosten et al., 1991; O’Connor et al., 1997; Umbricht et al., 1999). At Week 6 study visits were reduced from daily to thrice weekly and naltrexone doses of 100 mg, 100 mg, and 150 mg were ingested on Mondays, Wednesdays and Fridays, respectively (e.g., Carroll et al., 2002; Preston et al. 1999; Verebey, 1976).
Throughout the study, dosing was conducted in a double-blind, double-dummy manner. While such rigorous methods were not required for this uncontrolled pilot study, it served as an opportunity to develop and refine the dosing procedures that would be used in the subsequent randomized controlled trial comparing multiple taper durations. Subjects received a total of 5.5 tablets and 3 capsules at each clinic visit; the 5.5 tablets contained a combination of active and/or placebo buprenorphine and the 3 capsules a combination of active and/or placebo naltrexone, depending on study day. These procedures prevented subjects and staff from knowing the stabilization dose, the details of the buprenorphine taper, and the point at which an individual transitioned to naltrexone. At the end of the study, subjects were offered aftercare consisting of continued counseling and urinalysis monitoring at a less frequent schedule; those who were interested in continuing naltrexone following study completion were assisted with accessing a prescription from their primary care physician. Three consecutive missed doses or urine samples resulted in discharge from the study and referral to a local treatment program.
2.3. Study medications
Buprenorphine/naloxone and color-matched placebo sublingual tablets were provided by Reckitt Benckiser Pharmaceuticals, Inc. (Richmond, VA) through the National Institute on Drug Abuse (Rockville, MD). Doses (placebo, 1, 2, 4, 6, 8, 10, 12, 14 and 16 mg) were prepared by the investigational pharmacy and packaged in blind, letter-coded cassettes. All doses were administered sublingually under staff observation. Subjects were administered 5.5 tablets sublingual tablets, containing a combination of active and/or color-matched placebo buprenorphine, at each study visit throughout the study to preserve the double-blind nature of the dosing procedures.
Naltrexone (12.5, 25, 50, 100 and 150 mg) capsules (size 0, opaque hard gelatin) were prepared by the investigational pharmacy using naltrexone hydrochloride and powdered lactose. Identical placebo capsules were prepared using only powdered lactose. Doses were packaged in letter-coded plastic envelopes to ensure that research staff and subjects remained blind to the dose being administered. Subjects ingested orally 3 capsules, containing a combination of naltrexone and/or placebo, depending on study day, at each study visit under staff observation (e.g., subjects ingested all placebo capsules throughout the buprenorphine stabilization and taper phases).
2.4. Urinalysis Testing
Urine samples were collected under same-sex staff observation thrice weekly (MWF) and tested immediately for opioids. Enzyme multiplied immunoassay assays (Syva, San Jose, C.A.) on a VIVA-E analyzer (Dade Behring, Cupertino, CA) were used to test for opioids (300 ng/ml cutoff), methadone (150 ng/ml cutoff) and propoxyphene (300 ng/ml cutoff). ACON One Step lateral flow immunoassay test strips (ACON Laboratories, San Diego, CA) were used to test for oxycodone (100 ng/ml cutoff) and buprenorphine (10 ng/ml cutoff). Since buprenorphine was being administered during stabilization and taper phases, buprenorphine-positive results were expected and therefore not considered as opioid-positive. Beginning on Day 15 (the day immediately following the end of the 2-week taper), a buprenorphine-positive result was considered as positive for illicit opioid use. If a subject failed to provide a scheduled urine sample at any time in the study, it was considered opioid positive. Samples were also tested on a once-weekly, random schedule for the presence of cocaine, amphetamines, benzodiazepines, marijuana and barbiturates.
2.5. Assessments
At intake, subjects completed an assessment battery that included the following instruments: a Demographic and Drug History Questionnaire developed by our clinic, the psychoactive substance dependence section of the DSM-IV (Feingold & Rounsaville, 1995), the Addiction Severity Index (ASI, McLellan et al., 1985); the Beck Anxiety Inventory (BAI, Beck et al, 1988); the Beck Depression Inventory (BDI-II, Beck et al, 1961) and the Michigan Alcoholism Screening Test (MAST, Selzer, 1971). Subjects also received a comprehensive medical evaluation (e.g., detailed medical history, physical examination, blood chemistry, hematology, urinalysis) to confirm they were healthy to participate, and all were compensated $35 for completing the intake screening.
At each clinic visit, assessments of opioid withdrawal and agonist effects were conducted via self-report, observer-rated and physiological measures. Self-report ratings were collected using a 37-item adjective checklist that included a 21-item Withdrawal Adjective and a 16-item Agonist Rating Scale (Preston et al., 1988). Subjects also completed visual analog scales consisting of seven items: “Do you feel any withdrawal discomfort right now?,” “How high are you?,” “Do you feel any good effects?,” “Do you feel any bad effects?,” “Do you like the way you feel?,” “Do you feel sick?,” and “Do you crave opiates right now?”. Subjects responded by drawing a mark along a 100-mm line labeled at either end with “Not at all” and “Extremely” to yield a score between 0 and 100. Observer ratings of withdrawal were made by research nurses using a modified Himmelsbach (1941) withdrawal severity scale (Eissenberg et al., 1996), which assessed the presence or absence of 6 opioid withdrawal symptoms (i.e., lacrimation, rhinorrhea, yawning, perspiration, piloerection, and restlessness) and had a possible score range of 0-12. Nurses also completed the Clinical Institute Narcotic Assessment (CINA, Peachey & Lei, 1988), a commonly-used 12-item clinical instrument that yields a withdrawal severity score from a combination of self-report and observer ratings. Finally, pupil diameter, a physiological measure of withdrawal, was assessed in constant ambient lighting via pupillometer (NeurOptics, San Clemente, CA), a handheld, cordless device that uses infrared technology to estimate pupil diameter over a 3-second period.
2.6. Behavioral therapy
All subjects received individual behavioral counseling twice-weekly with a master’s level therapist. The CRA therapy was based on that developed for cocaine dependence (Budney & Higgins, 1998) but adapted to accommodate a PO-dependent population undergoing detoxification. Topics included identifying antecedents to drug use and relapse prevention, developing new recreational activities and social networks, and addressing practical needs such as employment, education and health insurance. Additional components were tailored to an individual’s unique needs (e.g., money management, insomnia, assertiveness training, depression, anger management). Finally, several mandatory sessions were conducted on coping with opioid withdrawal, medication management, and HIV/hepatitis education. The therapist completed extensive training in this manual-based therapy and received weekly clinical supervision.
2.7. Analyses
Analyses were performed on the 14 subjects who completed stabilization and began the taper phase independent of early dropout, noncompliance, etc., consistent with an intent-to-treat approach to clinical trials (Armitage, 1983). Any missing urine samples were considered as opioid-positive for all analyses. Descriptive statistics were used to characterize baseline demographic and drug use variables, the percent of urine specimens testing negative for opioids for the entire study and for each study phase and the percent of subjects testing opioid negative at the end of the taper, ingesting at least one 50 mg dose of naltrexone and being retained through the end of the study. Similar analyses were used to describe assessments of withdrawal during the study. Post-hoc comparisons of Responders and Nonresponders (defined below) were performed on opioid abstinence, retention, and baseline demographic and drug use characteristics using t-tests, chi-square and Wilcoxon rank sum tests for continuous measures or Fisher’s exact tests for percentages. Analyses were performed using SAS 9.1 (SAS Institute, Inc., Cary, NC). Statistical significance was determined using α=.05.
3. Results
3.1. Demographic and drug use characteristics
Of the 15 subjects consented, one dropped out prior to completing the stabilization phase; therefore, results are based on the 14 (8 males, 6 females) who completed stabilization and entered the taper phase. Demographic and drug use characteristics are shown in Table 1. Briefly, subjects reported using opioids on 24.6 ± 4.2 of the 30 days prior to intake and using opioids regularly for 2.8± 1.4 years. An oxycodone product (e.g., OxyContin, Percocet) was the primary drug for all subjects. Seventy-nine percent reported intranasal as the primary route of administration and 21% reported the oral route. Subjects reported using 79.3 ± 29.5 mg oxycodone per day and spending $439 ± 230 on POs per week. While oxycodone was the most commonly-used drug, subjects reported using a wide range of other opioids, including illicit buprenorphine (86%), hydrocodone (71%), hydromorphone (65%), methadone (57%), morphine (50%), codeine (43%), meperidine (21%) and d-propoxyphene (21%), with 43% also reporting lifetime use of heroin. Twenty-nine percent of subjects reported a prior treatment episode for opioid abuse. In addition to opioid dependence, 50%, 21% and 7% met DSM criteria for nicotine, cannabis and alcohol dependence, respectively.
Table 1.
Baseline Demographic and Drug Use Characteristics
| n=14 | |
|---|---|
| Demographic Characteristics | |
| % Female | 43 |
| % Caucasian | 100 |
| Mean age (yrs) | 30.5 ± 10.4 |
| Mean years of education | 12.7 ± 0.4 |
| Drug Use Characteristics | |
| Primary opioid in past month | |
| % OxyContin | 93 |
| % Percocet | 7 |
| % Primary Oral Administration | 21 |
| % Primary Intranasal Administration | 79 |
| % Used IV | 7 |
| % Used Heroin | 43 |
| Mean opioids used per day (mgs) | 79.3 ± 29.5 |
| Mean days used opioids in past 30 days | 24.6 ± 4.2 |
| Mean duration of regular opioid use (yrs) | 2.8 ± 1.4 |
| Mean longest period of abstinence (days) | 67 (1.5, 180)a |
| % Reporting prior opioid treatment | 29 |
| DSM-IV Criteria | |
| % Meeting DSM-IV Dependence Criteria | |
| Alcohol | 7 |
| Cannabis | 21 |
| Cocaine | 0 |
| Nicotine | 50 |
| Opioid | 100 |
| Baseline Questionnaire Outcomes | |
| Addiction Severity Index (ASI)b | |
| Alcohol | 0.05 ± 0.07 |
| Drug | 0.37 ± 0.05 |
| Employment | 0.33 ± 0.28 |
| Family | 0.19 ± 0.29 |
| Legal | 0.04 ± 0.09 |
| Medical | 0.08 ± 0.15 |
| Psychiatric | 0.19 ± 0.22 |
| Beck Anxiety Inventory (range 0 - 63) | 13.1 ± 7.7 |
| Beck Depression Inventory (range 0 - 54) | 22.9 ± 12.4 |
| Michigan Alcohol Screening Inventory (range 0 - 53) | 9.6 ± 8.4 |
Values represent average ± SD unless otherwise indicated.
Represents interquartile range
ASI scores represent composite scores, range 0-1.
3.2. Opioid Abstinence
During stabilization, 83.8% of scheduled urine samples tested negative for illicit opioid use (with missing samples treated as opioid-positive); in the subsequent 2-week taper phase, 91.7% of samples tested negative for illicit opioids (Figure 1, upper panel). While these outcomes of the stabilization and taper phases were favorable, those following the taper were more modest, with 31.2% of samples testing negative from all opioids during the 10-week naltrexone phase (Figure 1, upper panel).
Figure 1. Opioid Abstinence.
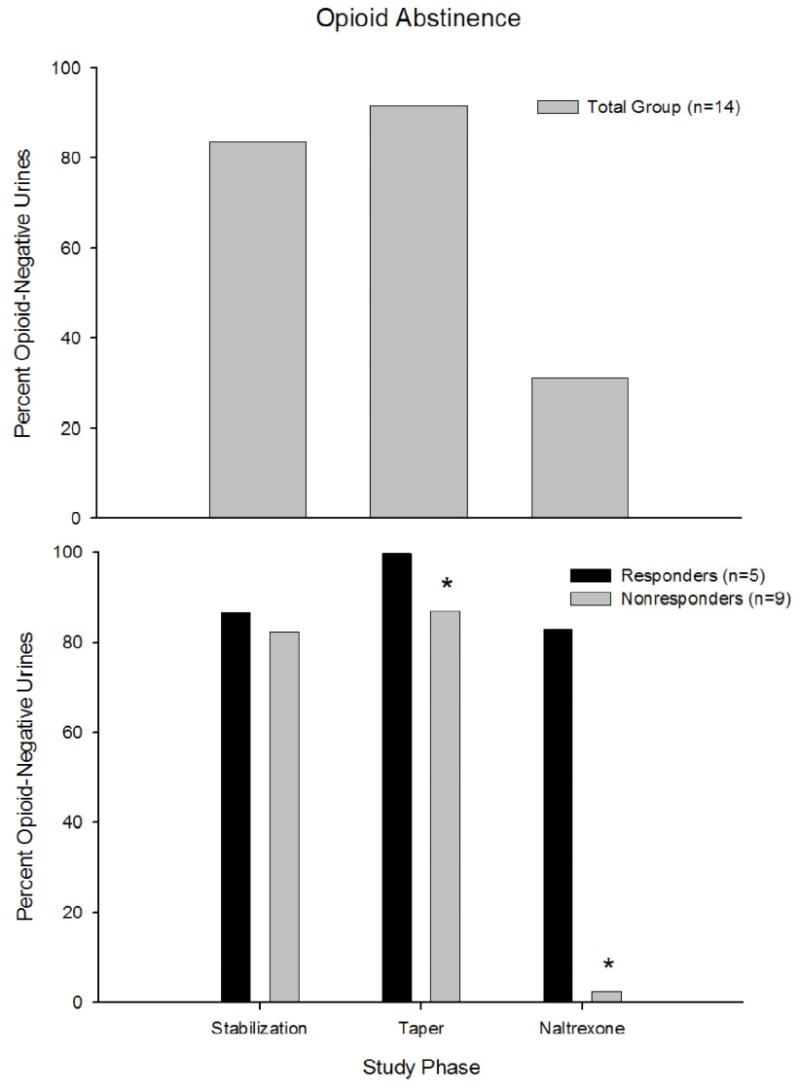
Percent opioid-negative urine samples submitted by all participants (n=14; upper panel) and by Responders (n=5) and Nonresponders (n=9; lower panel) during the stabilization, taper and naltrexone study phases. Asterisks indicate significant (p<.05) differences between the Responders and Nonresponders during the taper and naltrexone study phases.
Inspection of individual subject data at the end of the 2-week taper revealed systematic differences in whether subjects successfully completed the taper without resumption of illicit opioid use. More specifically, subjects were dichotomized using the criterion of whether they tested negative for all illicit opioids (including buprenorphine) on the day following the 2-week taper (Responder) or positive for any opioid (Nonresponder). Using this definition, 36% (n=5) of subjects met criteria for being a Responder and 64% (n=9) were Nonresponders. Responders provided numerically more opioid-negative samples than Nonresponders during stabilization (86.7% vs. 82.2%, respectively; p=.75) and significantly more during taper (100% vs. 87%, respectively; p=.04) and naltrexone (82.9% vs. 2.4%, respectively; p<.01) phases (Figure 1, lower panel). Other measures showed a similar pattern, with more Responders achieving complete opioid abstinence for the entire study (40% vs. 0%; p=.11) and Responders submitting more consecutive opioid-negative urines (38 vs. 10; p=.02) than Nonresponders, respectively. A greater percent of Responders also ingested at least one 50 mg dose of naltrexone (100% vs. 11%; p<.01) and were retained through the end of the study (60% vs. 0%; p=.03) compared to Nonresponders. Responders and Nonresponders did not significantly differ on demographic or drug use characteristics except for the Alcohol subscale of the ASI, on which Nonresponders had higher scores than Responders (0.08 vs. 0.00, respectively, p=.05).
3.3. Opioid Withdrawal
Analyses of withdrawal data were limited to Responders as relapse to illicit opioid use among Nonresponders would have confounded our evaluation of withdrawal. Participants presented with modestly-elevated CINA scores upon entry into the study, which then gradually decreased during buprenorphine stabilization (Figure 2, upper left panel). Mean CINA scores increased again during the 2-week taper, though they did not reach peak levels until several days following the end of the taper. CINA scores did not fully return to pre-taper levels until approximately 8-10 weeks following the end of the buprenorphine taper. Subject and observer ratings showed patterns similar to the CINA, including the VAS item “Do you feel any withdrawal discomfort right now” (upper right), the Withdrawal Adjective Rating Scale score (lower left) and observer ratings on the modified Himmelsbach (lower right).
Figure 2. Opioid Withdrawal.
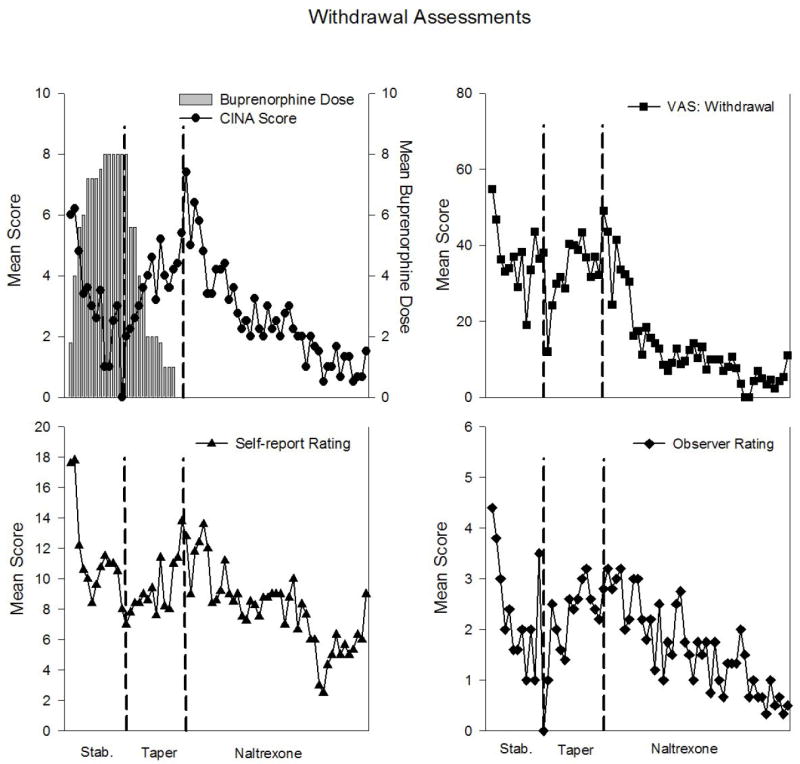
Data represent mean withdrawal measures among Responders (n=5), collected immediately prior to administration of study medication. Vertical lines distinguish stabilization, taper and naltrexone phases. Upper left panel: Mean CINA scores (range 0 – 30; left y-axis) and mean buprenorphine doses (mg; right y-axis) across consecutive study visits. Upper right panel: Mean score on self-report visual analog (range 0 – 100) item “Do you feel any withdrawal discomfort right now?” Lower left panel: Mean score on self-report Withdrawal Adjective Rating Scale (range 0 – 84). Lower right panel: Mean withdrawal severity score on observer-rated modified Himmelsbach assessment (range 0 – 12).
4. Discussion
In this pilot trial, we sought to examine the feasibility of a brief outpatient detoxification for treating PO-dependent outpatients. Overall, participants achieved high rates of opioid abstinence during the stabilization and taper phases but poor to modest rates following the taper. These data suggest that a brief 2-week outpatient taper may be effective with a subset of the PO-abusing sample. These results are comparable to outcomes seen in other studies using outpatient buprenorphine detoxification of similar durations with general populations of illicit opioid abusers (Diamant et al., 1998; Lintzeris, 2002; Lintzeris et al., 2002; Ling et al., 2005). Overall, a careful and systematic scientific effort will be necessary to develop a medication-assisted detoxification protocol that prevents the poor retention and high relapse rates that can plague detoxification programs (Amass et al., 1994; Bickel et al., 1988; Kosten et al., 1991; O’Connor et al., 1997; Resnick, 1983). Future research by our group will explore additional ways to enhance treatment outcome in this population, including longer taper durations as well as the possibility of incorporating innovative components like sustained-release formulations of pharmacotherapies and contingency management.
A two-week opioid taper does not appear to be sufficient for the majority of PO abusers, at least among the participants in the present study. The between-subject differences in outcome seen in this study are not unique to the PO-abusing population and are commonly observed with substance abuse treatments in general (e.g., Silverman et al., 1999). When baseline characteristics were compared between Responders and Nonresponders, the two groups in this study were largely similar. The only difference observed in this sample was that Nonresponders reported more severe alcohol-related problems at treatment intake than Responders. While this finding is provocative, it is also the case that the ASI score themselves were generally low (0.00 vs. 0.08, respectively, out of a possible range of 0-1) and there were no group differences on the MAST. Overall, the limited sample size in this pilot trial is insufficient to address this issue definitively. It will be important for future studies to more thoroughly investigate, using larger sample sizes, whether baseline alcohol severity may influence treatment outcome among PO abusers, as well other individual differences in response to specific treatments for PO abuse. Also important will be efforts to prospectively identify the demographic or drug use characteristics which may predict who will do well with a taper versus those who may need longer-term opioid maintenance and whether a longer-duration taper may produce higher success rates.
While the primary goal of this study was to begin to develop a treatment for PO abuse, it also included a comprehensive evaluation of opioid withdrawal using instruments derived from both clinical and research settings. Assessments were conducted at a high frequency over an extended duration (e.g., daily until Week 6, thrice weekly through Week 12) and under relatively rigorous experimental conditions (e.g., double-blind, double-dummy medication administration). Participants presented with modestly elevated withdrawal severity, which gradually decreased as they became stabilized on buprenorphine. Withdrawal scores increased again during the taper, though they generally did not reach peak magnitude until approximately 3.5 (range 3-5) days after the last buprenorphine dose. In addition to this delayed peak, it is also interesting to note that withdrawal scores did not fully return to pre-taper levels until the final weeks of the study (e.g., 8-10 weeks after the last buprenorphine dose). These data are consistent with prior reports suggesting a slightly delayed emergence of peak buprenorphine withdrawal symptoms (Assadi et al., 2004; Fudala et al., 1990). A more complete characterization of withdrawal timecourse and severity in PO abusers will be reported in a future report that also will include a larger sample size and double-blind randomization to multiple taper durations. Overall, developing a full understanding of the parameters of buprenorphine withdrawal is important, particularly as use of this medication becomes increasingly common in clinical settings for treatment of opioid dependence.
Several limitations of this study should be noted. First, the primary limitation is that this was an unrandomized pilot trial with a limited sample size. A large-scale, double-blind randomized clinical trial is currently underway to evaluate multiple taper durations using a more rigorous scientific design. However, the present study did possess several methodological strengths, including rigorous dosing procedures, comprehensive withdrawal assessments, on-site observed urinalysis testing, and a manual-based empirically-supported behavioral therapy. As such, it represents a good first step towards investigating the potential feasibility of an outpatient buprenorphine detoxification in treating PO abuse. Second, there was no effort in this study to dismantle or isolate the effects of the behavioral therapy compared to the other treatment components and, as a result, the contribution of the counseling to outcomes is unknown. Future efforts to experimentally examine the type of therapy used with this population may be warranted. Third, all participants were Caucasian and endorsed an oxycodone product as their primary drug of abuse, both of which may limit the generality of our results to the larger population of PO abusers. Our large-scale randomized trial will include subjects who use a wider range of primary opioids, which will allow us to examine the generality of these findings to PO abusers who use opioids other than oxycodone. However, it is also worth noting that recent reports have indicated that PO users tend to be overwhelmingly Caucasian (e.g., McCabe et al., 2005a, 2005b; Moore et al., 2007; NSDUH, 2005; Rosenblum et al., 2007). Further, recent reports indicate that oxycodone is one of the most commonly-abused POs (Cicero et al., 2005; DAWN, 2007) and it is among the most-commonly diverted pharmaceuticals in many areas of the country (ONDCP, 2008). Finally, as the primary focus of this study was to develop an efficacious intervention for PO abuse that employs an opioid taper and subsequent naltrexone maintenance, individuals who required ongoing opioid therapy for pain or other chronic medical conditions were excluded from participating. While this may limit the generality of our findings, it also seems reasonable to expect that PO abusers with significant pain issues also are not likely to be the most appropriate candidates for opioid detoxification and antagonist therapy.
Overall, results from this pilot study suggest that a subset of PO abusers may respond to an outpatient treatment that includes brief buprenorphine detoxification and intensive behavioral therapy. Identifying these individuals is important, particularly for those who may be able to achieve good outcomes without long-term maintenance, and certainly the increasing numbers of PO-abusing adolescents and young adults warrant exploring potential alternatives to long-term opioid maintenance. That said, the majority did not respond to the intervention. Additional controlled studies will be important to better understand the parameters for developing efficacious treatments for PO abuse, as well as to identify individual patient characteristics that may predict whether short- versus longer-term treatments are warranted. Overall, this new information should inform efforts to develop efficacious treatments for the emerging population of PO abusers.
Acknowledgments
This study was supported by research grant R01-DA019989 (S.C. Sigmon, Principal Investigator) and training grant T32 DA007242 from the National Institute on Drug Abuse. Buprenorphine/naloxone and color-matched placebo sublingual tablets were provided by Reckitt Benckiser Pharmaceuticals, Inc. (Richmond, VA) through the National Institute on Drug Abuse (Rockville, MD). We thank Betsy Bahrenburg, Bruce Brown, Allison Newth and Dana Wohl for their assistance conducting this study and Colleen Thomas for statistical support.
Footnotes
Publisher's Disclaimer: This is a PDF file of an unedited manuscript that has been accepted for publication. As a service to our customers we are providing this early version of the manuscript. The manuscript will undergo copyediting, typesetting, and review of the resulting proof before it is published in its final citable form. Please note that during the production process errors may be discovered which could affect the content, and all legal disclaimers that apply to the journal pertain.
References
- Abbott PJ, Moore BA, Weller SB, Delaney HD. AIDS risk behavior in opioid dependent patients treated with community reinforcement approach and relationships with psychiatric disorders. Journal of Addictive Diseases. 1998;14(4):33–48. doi: 10.1300/J069v17n04_04. [DOI] [PubMed] [Google Scholar]
- Alterman AI, Kampman K, Boardman CR, Cacciola JS, Rutherford MJ, McKay JR, Maany I. A cocaine-positive baseline urine predicts outpatient treatment attrition and failure to attain initial abstinence. Drug and Alcohol Dependence. 1997;46(12):79–85. doi: 10.1016/s0376-8716(97)00049-5. [DOI] [PubMed] [Google Scholar]
- Amass L, Bickel WK, Higgins S, Hughes JR. A preliminary investigation of outcome following gradual or rapid buprenorphine detoxification. Journal of Addictive Diseases. 1994;13(3):33–45. doi: 10.1300/j069v13n03_04. [DOI] [PubMed] [Google Scholar]
- Armitage P. Exclusions, losses to follow-up, and withdrawals in clinical trials. In: Shapiro SH, Lewis TA, editors. Clinical trials Issues and approaches. New York; Marcel Dekker, Inc: 1983. pp. 99–113. [Google Scholar]
- Assadi SM, Hafezi M, Mokri A, Razzaghi E, Pharm PG. Opioid detoxification using high doses of buprenorphine in 24 hours: A randomized, double-blind, controlled clinical trial. Journal of Substance Abuse Treatment. 2004;27(1):75–82. doi: 10.1016/j.jsat.2004.05.002. [DOI] [PubMed] [Google Scholar]
- Azrin NH. Improvements in the community-reinforcement approach to alcoholism. Behavior Research and Therapy. 1976;14(5):339–38. doi: 10.1016/0005-7967(76)90021-8. [DOI] [PubMed] [Google Scholar]
- Azrin NH, Sisson RW, Meyers R, Godley M. Alcoholism treated by disulfiram and community reinforcement therapy. Journal of Behavior Therapy and Experimental Psychiatry. 1982;13(2):105–121. doi: 10.1016/0005-7916(82)90050-7. [DOI] [PubMed] [Google Scholar]
- Beck AT, Epstein N, Brown G, Steer RA. An inventory for measuring clinical anxiety: Psychometric properties. Journal of Consulting and Clinical Psychology. 1988;56(6):893–897. doi: 10.1037//0022-006x.56.6.893. [DOI] [PubMed] [Google Scholar]
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Archives of General Psychiatry. 1961;4:561–571. doi: 10.1001/archpsyc.1961.01710120031004. [DOI] [PubMed] [Google Scholar]
- Becker AB, Strain EC, Bigelow GE, Stitzer ML, Johnson RE. Gradual dose taper following chronic buprenorphine. The American Journal on Addictions. 2001;10(2):111–121. doi: 10.1080/105504901750227778. [DOI] [PubMed] [Google Scholar]
- Bickel WK, Amass L, Higgins ST, Badger GJ, Esch RA. Effects of adding behavioral treatment to opioid detoxification with buprenorphine. Journal of Consulting and Clinical Psychology. 1997;65(5):803–810. doi: 10.1037//0022-006x.65.5.803. [DOI] [PubMed] [Google Scholar]
- Bickel WK, Stitzer ML, Bigelow GE, Liebson IA, Jasinski DR, Johnson RE. A clinical trial of buprenorphine: Comparison with methadone in the detoxification of heroin addicts. Clinical Pharmacological Therapeutics. 1988;43(3):72–78. doi: 10.1038/clpt.1988.13. [DOI] [PubMed] [Google Scholar]
- Brands B, Blake J, Sproule B, Gourlay D, Busto U. Prescription opioid abuse in patients presenting for methadone maintenance treatment. Drug and Alcohol Dependence. 2004;73(2):199–207. doi: 10.1016/j.drugalcdep.2003.10.012. [DOI] [PubMed] [Google Scholar]
- Budney AJ, Higgins ST. A community reinforcement plus vouchers approach Treating cocaine addiction. Rockville, MD: Department of Health and Human Services, National Institute on Drug Abuse; 1998. [Google Scholar]
- Bullingham RE, McQuay HJ, Moore A, Bennett MR. Buprenorphine kinetics. Clinical Pharmacology and Therapeutics. 1980;28(5):667–672. doi: 10.1038/clpt.1980.219. [DOI] [PubMed] [Google Scholar]
- Carise D, Dugosh KL, McLellan AT, Camilleri A, Woody GE, Lynch KG. Prescription OxyContin abuse among patients entering addiction treatment. American Journal of Psychiatry. 2007;164(11):1750–1756. doi: 10.1176/appi.ajp.07050252. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Carroll KM, Sinha R, Nich C, Babuscio T, Rounsaville BJ. Contingency management to enhance naltrexone treatment of opioid dependence: a randomized clinical trial of reinforcement magnitude. Experimental and Clinical Psychopharmacology. 2002;10(1):54–63. doi: 10.1037//1064-1297.10.1.54. [DOI] [PubMed] [Google Scholar]
- Cicero TJ, Inciardi JA, Munoz A. Trends in abuse of OxyContin and other opioid analgesics in the United States: 2002-2004. The Journal of Pain. 2005;6(10):662–672. doi: 10.1016/j.jpain.2005.05.004. [DOI] [PubMed] [Google Scholar]
- Cicero TJ, Surratt H, Inciardi JA, Munoz A. Relationship between therapeutic use and abuse of opioid analgesics in rural, suburban, and urban locations in the United States. Phamacoepidemiology and Drug Safety. 2007;16(8):827–840. doi: 10.1002/pds.1452. [DOI] [PubMed] [Google Scholar]
- Compton WM, Volkow ND. Major increases in opioid analgesic abuse in the United States: Concerns and strategies. Drug and Alcohol Dependence. 2006;81(2):103–107. doi: 10.1016/j.drugalcdep.2005.05.009. [DOI] [PubMed] [Google Scholar]
- Diamant K, Fischer G, Schneider C, Lenzinger E, Pezawas L, Schindler S, Eder H. Outpatient opiate detoxification treatment with buprenorphine. Preliminary Investigation. European Addiction Research. 1998;4(4):198–202. doi: 10.1159/000018953. [DOI] [PubMed] [Google Scholar]
- Drug Abuse Warning Network (DAWN) The DAWN Report. Rockville, MD: 2003. Substance Abuse and Mental Health Services Administration Office of Applied Studies: Trends in drug-related emergency department visits 1994-2002 at a glance. [PubMed] [Google Scholar]
- Drug Abuse Warning Network (DAWN) DAWN Series D-29, DHHS Publication No (SMA) 07-4256. Rockville, MD: 2007. Substance Abuse and Mental Health Services Administration Office of Applied Studies National Estimates of Drug-Related Emergency Department Visits 2005. [Google Scholar]
- Eissenberg T, Greenwald MK, Johnson RE, Liebson IA, Bigelow GE, Stitzer ML. Buprenorphine’s physical dependence potential: antagonist-precipitated withdrawal in humans. Journal of Pharmacology and Experimental Therapeutics. 1996;276(2):449–459. [PubMed] [Google Scholar]
- Feingold A, Rounsaville B. Construct validity of the dependence syndrome as measured by DSM-IV for different psychoactive substances. Addiction. 1995;90(2):1661–1669. doi: 10.1046/j.1360-0443.1995.901216618.x. [DOI] [PubMed] [Google Scholar]
- Fudala PJ, Jaffe JH, Dax EM, Johnson RE. Use of buprenorphine in the treatment of opioid addiction. II. Physiologic and behavioral effects of daily and alternate-day administration and abrupt withdrawal. Clinical Pharmacology and Therapeutics. 1990;47(4):525–534. doi: 10.1038/clpt.1990.67. [DOI] [PubMed] [Google Scholar]
- Gerra G, Borella F, Zaimovic A, Moi G, Bussandri M, Bubici C, Bertacca S. Buprenorphine versus methadone for opioid dependence: predictor variables for treatment outcome. Drug and Alcohol Dependence. 2004;75(1):37–45. doi: 10.1016/j.drugalcdep.2003.11.017. [DOI] [PubMed] [Google Scholar]
- Gonzalez JP, Brogden RN. Naltrexone. A review of its pharmacodynamic and pharmacokinetic properties and therapeutic efficacy in the management of opioid dependence. Drugs. 1988;35(3):192–213. doi: 10.2165/00003495-198835030-00002. [DOI] [PubMed] [Google Scholar]
- Hambrook JM, Rance MJ. The interaction of buprenorphine with the opiate receptor: Lipophilicity as a determining factor in drug-receptor kinetics. In: Kosterlitz HW, editor. Opiates and Endogenous Opioid Peptides. Amsterdam: Elsevier/North Holland, Biomedical Press; 1976. pp. 295–301. [Google Scholar]
- Higgins ST, Sigmon SC, Wong CJ, Heil SH, Badger GJ, Donham R, Dantona RL, Anthony S. Community-reinforcement therapy for cocaine-dependent outpatients. Archives of General Psychiatry. 2003;60(10):1043–1052. doi: 10.1001/archpsyc.60.9.1043. [DOI] [PubMed] [Google Scholar]
- Himmelsbach CK. The morphine abstinence syndrome, its nature and treatment. Annals of Internal Medicine. 1941;15:829–839. [Google Scholar]
- Hunt GM, Azrin NH. A community-reinforcement approach to alcoholism. Behaviour Research and Therapy. 1973;11(1):91–104. doi: 10.1016/0005-7967(73)90072-7. [DOI] [PubMed] [Google Scholar]
- Iguchi MY, Stitzer ML. Predictors of opiate drug abuse during a 90-day methadone detoxification. American Journal of Drug and Alcohol Abuse. 1991;17:279–294. doi: 10.3109/00952999109027552. [DOI] [PubMed] [Google Scholar]
- Jasinski DR, Pevnick JS, Griffith JD. Human pharmacology and abuse potential of the analgesic buprenorphine: a potential agent for treating narcotic addiction. Archives of General Psychiatry. 1978;35(4):501–516. doi: 10.1001/archpsyc.1978.01770280111012. [DOI] [PubMed] [Google Scholar]
- Johnson RE, Jaffe JH, Fudala PJ. A controlled trial of buprenorphine treatment for opioid dependence. Journal of the American Medical Association. 1992;267(10):2750–2755. [PubMed] [Google Scholar]
- Johnston LD, O’Malley PM, Bachman JG. NIH Publication No 02-5105. National Institute on Drug Abuse; Bethesda, MD: 2002. Monitoring the Future National Results on Adolescent Drug Use: Overview of Key Findings, 2001. [Google Scholar]
- Kampman KM, Pettinati HM, Volpicelli JR, Oslin DM, Lipkin C, Sparkman T, O’Brien CP. Cocaine dependence severity predicts outcome in outpatient detoxification from cocaine and alcohol. American Journal of Addiction. 2004;13(1):74–82. doi: 10.1080/10550490490265389. [DOI] [PubMed] [Google Scholar]
- Knudsen HK, Ducharme LJ, Roman PM. Controlled-release oxycodone admissions in public and private substance abuse treatment: Associations with organizational characteristics. Journal of Addictive Diseases. 2007;26(1):41–50. doi: 10.1300/J069v26n01_06. [DOI] [PubMed] [Google Scholar]
- Kosten TR, Kleber HD. Buprenorphine detoxification from opioid dependence: A pilot study. Life Sciences. 1989;42(2):635–641. doi: 10.1016/0024-3205(88)90454-7. [DOI] [PubMed] [Google Scholar]
- Kosten TR, Morgan C, Kleber HD. Treatment of heroin addicts using buprenorphine. American Journal on Drug and Alcohol Abuse. 1991;17(2):119–128. doi: 10.3109/00952999108992815. [DOI] [PubMed] [Google Scholar]
- Ling W, Amass L, Shoptaw S, Annon JJ, Hillhoise M, Babcock D, Brigham G, Harrer J, Reid M, Muir J, Buchan B, Orr D, Woody G, Krejci J, Ziedonis D Buprenorphine Study Protocol Group. A multi-center randomized trial of buprenorphine-naloxone versus clonidine for opioid detoxification: findings from the National Institute on Drug Abuse Clinical Trials Network. Addiction. 2005;100(8):1090–1100. doi: 10.1111/j.1360-0443.2005.01154.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Lintzeris N. Buprenorphine dosing regime in the management of out-patient heroin withdrawal. Drug and Alcohol Review. 2002;21(1):39–45. doi: 10.1080/09595230220119309. [DOI] [PubMed] [Google Scholar]
- Lintzeris N, Bell J, Bammer G, Jolley DJ, Rushworth L. A randomized controlled trial of buprenorphine in the management of short-term ambulatory heroin withdrawal. Addiction. 2002;97(11):1395–1404. doi: 10.1046/j.1360-0443.2002.00215.x. [DOI] [PubMed] [Google Scholar]
- Marsch L, Bickel WK, Badger GJ, Stothart ME, Quesnel KJ, Stanger C, Brooklyn J. Comparison of pharmacological treatments for opioid-dependent adolescents. Archives of General Psychiatry. 2005;62(10):1157–1164. doi: 10.1001/archpsyc.62.10.1157. [DOI] [PubMed] [Google Scholar]
- Martin WR, Jasinski DR, Mansky PA. Naltrexone, an antagonist for the treatment of heroin dependence. Effects in man. Archives in General Psychiatry. 1973;28(6):784–791. doi: 10.1001/archpsyc.1973.01750360022003. [DOI] [PubMed] [Google Scholar]
- McCabe SE, Boyd CJ, Teter CJ. Illicit use of opioid analgesics by high school seniors. Journal of Substance Abuse Treatment. 2005a;28(3):225–230. doi: 10.1016/j.jsat.2004.12.009. [DOI] [PubMed] [Google Scholar]
- McCabe SE, Boyd CJ, Young A. Medical and nonmedical use of prescription drugs among secondary school students. Journal of Adolescent Health. 2007;40(1):76–83. doi: 10.1016/j.jadohealth.2006.07.016. [DOI] [PMC free article] [PubMed] [Google Scholar]
- McCabe SE, Teter CJ, Boyd CJ, Knight JR, Wechsler H. Nonmedical use of prescription opioids among U.S. college students: Prevalence and correlates from a national study. Addictive Behaviors. 2005b;30(4):798–805. doi: 10.1016/j.addbeh.2004.08.024. [DOI] [PubMed] [Google Scholar]
- McLellan AT, Luborsky L, Cacciola J. New data from the Addiction Severity Index: Reliability and validity in three centers. Journal of Nervous and Mental Disease. 1985;173(7):412–423. doi: 10.1097/00005053-198507000-00005. [DOI] [PubMed] [Google Scholar]
- Mello NK, Mendelson JH, Kuehnle JC, Sellers MS. Operant analysis of human heroin self-administration and the effects of naltrexone. Journal of Pharmacology and Experimental Therapeutics. 1981;216(1):45–54. [PubMed] [Google Scholar]
- Moore B, Fiellin DA, Barry DT, Sullivan LE, Chawarski MC, O’Connor PG, Shottenfeld RS. Primary care office-based buprenorphine treatment: Comparison of heroin and prescription opioid dependent patients. Journal of General Internal Medicine. 2007;22(4):527–530. doi: 10.1007/s11606-007-0129-0. [DOI] [PMC free article] [PubMed] [Google Scholar]
- National Survey on Drug Use and Health (NSDUH) report. Nonmedical oxycodone users A comparison with heroin users Office of Applied Studies publication. 2005 available online at http://www.oas.samhsa.gov.
- O’Connor PG, Carroll KM, Shi JM, Schottenfeld RS, Kosten TR, Rounsaville BJ. Three methods of opioid detoxification in a primary care setting. Annals of Internal Medicine. 1997;127(7):526–530. doi: 10.7326/0003-4819-127-7-199710010-00004. [DOI] [PubMed] [Google Scholar]
- Office of National Drug Control Policy (ONDCP) State of Vermont: Profile of Drug Indicators. Drug Policy Information Clearinghouse; Rockville, MD: 2008. [Google Scholar]
- Peachey JE, Lei H. Assessment of opioid dependence with naloxone. British Journal of Addiction. 1988;83(2):193–201. doi: 10.1111/j.1360-0443.1988.tb03981.x. [DOI] [PubMed] [Google Scholar]
- Preston KL, Bigelow GE, Liebson IA. Buprenorphine and naloxone alone and in combination in opioid-dependent humans. Psychopharmacology. 1988;94:484–490. doi: 10.1007/BF00212842. [DOI] [PubMed] [Google Scholar]
- Preston KL, Silverman K, Higgins ST, Brooner RK, Montoya I, Schuster CR, Cone EJ. Cocaine use early in treatment predicts outcome in a behavioral treatment program. Journal of Consulting and Clinical Psychology. 1998;66(4):691–696. doi: 10.1037//0022-006x.66.4.691. [DOI] [PubMed] [Google Scholar]
- Resnick R. Methadone detoxification from illicit opiates and methadone maintenance. In: Cooper JR, Altman F, Brown BS, Czechowicz D, editors. Research on the Treatment of Narcotic Addiction State of the Art NIDA Treatment Research Monograph Series no 83-1281. Washington, DC: US Government Printing Office; 1983. pp. 160–167. [Google Scholar]
- Rosenblum A, Parrino M, Schnoll SH, Fong C, Maxwell C, Cleland CM, Magura S, Haddox JD. Prescription opioid abuse among enrollees into methadone maintenance treatment. Drug and Alcohol Dependence. 2007;90(1):64–71. doi: 10.1016/j.drugalcdep.2007.02.012. [DOI] [PubMed] [Google Scholar]
- Selzer ML. The Michigan Alcoholism Screening Test: The quest for a new diagnostic instrument. American Journal of Psychiatry. 1971;127(12):1653–1658. doi: 10.1176/ajp.127.12.1653. [DOI] [PubMed] [Google Scholar]
- Sigmon SC. Characterizing the emerging population of prescription opioid abusers. The American Journal on Addictions. 2006;15(3):208–212. doi: 10.1080/10550490600625624. [DOI] [PubMed] [Google Scholar]
- Silverman K, Chutuape MA, Bigelow GE, Stitzer ML. Voucher-based reinforcement of cocaine abstinence in treatment-resistant methadone patients: effects of reinforcement magnitude. Psychopharmacology. 1999;146(2):128–138. doi: 10.1007/s002130051098. [DOI] [PubMed] [Google Scholar]
- Soyka M, Zingg C, Koller G, Kuefner H. Retention rate and substance use in methadone and buprenorphine maintenance therapy and predictors of outcome: Results from a randomized study. International Journal of Neuropsychopharmacology. 2008;11:641–653. doi: 10.1017/S146114570700836X. [DOI] [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) 21 CFR Part 29 142 CFR Part 8. Department of Health and Human Services; Rockville, MD: 2001. Federal Register Opioid Drugs in Maintenance and Detoxification Treatment of Opiate Addiction Final Rule. [PubMed] [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) NHSDA Series H-22, DHHS Publication No (SMA) 03–3836. Rockville, MD: 2003. Office of Applied Studies Results from the 2002 National Survey on Drug Use and Health National Findings. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) Office of Applied Studies NSDUH Series H-32, DHHS Publication No SMA 07-4293. Rockville, MD: 2007a. Results from the 2006 National Survey on Drug Use and Health National Findings. [Google Scholar]
- Substance Abuse and Mental Health Services Administration (SAMHSA) Office of Applied Studies Series #S-40, DHHS Publication No (SMA) 08-4313. Rockville, MD: 2007b. Treatment Episode Data Set (TEDS) Highlights - 2006 National Admissions to Substance Abuse Treatment Services. [Google Scholar]
- Sung H-E, Richter L, Vaughan R, Johnson P, Thom B. Nonmedical use of prescription opioids among teenagers in the United States: Trends and correlates. Journal of Adolescent Health. 2005;37(1):44–51. doi: 10.1016/j.jadohealth.2005.02.013. [DOI] [PubMed] [Google Scholar]
- Treatment Episode Data Set (TEDS) DASIS Series S-23, DHHS Publication No (SMA) 04-3965. Rockville, MD: 2004. National Admissions to Substance Abuse Treatment Services 1992-2002. [Google Scholar]
- Umbricht A, Montoya ID, Hoover DR, Demuth KL, Chiang CT, Preston KL. Naltrexone shortened opioid detoxification with buprenorphine. Drug and Alcohol Dependence. 1999;56(3):181–190. doi: 10.1016/s0376-8716(99)00033-2. [DOI] [PubMed] [Google Scholar]
- Verebey K, Volavka J, Mule SJ, Resnick RB. Naltrexone: disposition, metabolism, and effects after acute and chronic dosing. Clinical Pharmacology and Therapeutics. 1976;20(3):315–328. doi: 10.1002/cpt1976203315. [DOI] [PubMed] [Google Scholar]
- Zacny J, Bigelow G, Compton P, Foley K, Iguchi M, Sannerud C. College on Problems of Drug Dependence taskforce on prescription opioid non-medical use and abuse: position statement. Drug and Alcohol Dependence. 2003;69(3):215–232. doi: 10.1016/s0376-8716(03)00003-6. [DOI] [PubMed] [Google Scholar]