

Abstract
Background
Hemodialysis patients experience a high degree of psychosocial impairment.
Methods
The psychosocial status of hemodialysis patients after Hurricane Katrina was evaluated using the Hurricane Coping Self-Efficacy (HCSE) measure, the Short Form-12 Health Survey (physical component summary [PCS] and mental component summary [MCS]), and the Center for Epidemiologic Studies Short Depression Scale (CES-D). These scales were administered to 391 hemodialysis patients (86% participation rate), 7 to 14 months after Hurricane Katrina.
Results
The mean score (standard deviation) was 36.2 (9.6) for the HCSE scale, 37.1 (10.9) and 46.7 (12.7) for the PCS and MCS, respectively, and 10.0 (6.5) on the CES-D. Symptoms of depression (CES-D scores ≥10) were present in 45.5% of patients. After age, race and gender adjustment, evacuating less than 2 days prior to Hurricane Katrina making landfall and more fear of dying were associated with less favorable scores on the HCSE, MCS and CES-D scales. Patients placed in a shelter and with a longer displacement had significantly lower MCS scores and more depressive symptoms. More depressive symptoms were observed among patients hospitalized in the month following the storm. Those who evacuated to a hotel, with more fear of dying and who were hospitalized in the month following Hurricane Katrina had lower scores on the PCS.
Conclusions
Impaired psychosocial status was common among dialysis patients surviving Hurricane Katrina and associated with reduced coping. These data demonstrate the need for screening and management of psychosocial issues in hemodialysis patients after disasters.
Keywords: hemodialysis, natural disasters, psychosocial status
INTRODUCTION
Hurricane Katrina made landfall on August 29, 2005 near New Orleans, LA as one of the deadliest storms in United States history.1 Individuals with chronic conditions comprised 25% of evacuees from this storm and, due to their reliance on continuity of health care, may constitute a large population warranting special considerations during and after an evacuation.2 Among this population were dialysis-dependent end-stage renal disease (ESRD) patients, requiring regular treatment, symptom monitoring, and dietary and fluid restrictions. These factors, along with knowledge of a shortened life expectancy and severely reduced mobility, can influence the psychosocial health of patients with ESRD.
Several previous studies have reported high rates of depression and reduced quality of life among hemodialysis patients in the non-disaster setting compared to the general population and patients who have received kidney transplantation.3-6 Following a natural disaster, these differences in psychosocial status may persist. The primary aim of the current study was to characterize the psychosocial status of hemodialysis patients impacted by Hurricane Katrina.
METHODS
Study Population
Participants in the current study were identified from the rosters, prior to Hurricane Katrina, for 9 dialysis facilities in New Orleans and four surrounding parishes. All of these clinics were closed during the immediate aftermath of Hurricane Katrina and 2 remained closed throughout the conduct of the study in 2006. To be eligible for the current study, patients had to be receiving hemodialysis treatment for ESRD at one of the 9 participating facilities during the week of August 23-27, 2005 (N=593). Among this population, 24 patients were excluded and 112 died prior to being contacted for the current study leaving 457 patients eligible for participation. Study interviews were completed with 391 patients between April 1, 2006 and October 30, 2006 yielding a participation rate of 85.6%. Additional details about the study population have been previously published.7
Conceptual Model
A conceptual model of the psychosocial adaptation of hemodialysis patients following a traumatic event such as a natural disaster is illustrated in Figure 1. The schema proposes interactions between medical, psychosocial, neurobiologic and disaster-related factors in the development of symptoms of depression in hemodialysis patients in the aftermath of a traumatic event. The current analysis examines the integral roles of coping factors, quality of life and depression in this model, as well as the influence of evacuation and displacement factors in the post-disaster setting.
Figure 1.
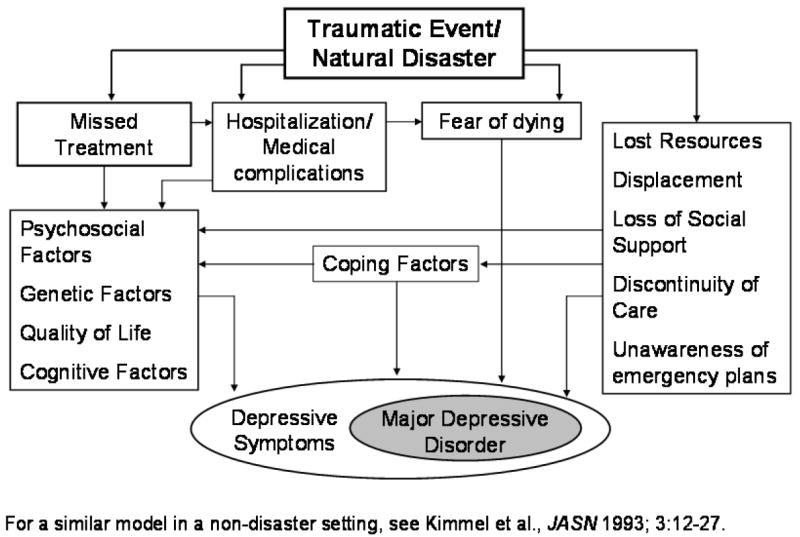
Conceptual model of the impact of trauma on the psychosocial status of hemodialysis patient
Data Collection
Study questionnaires were administered over the telephone by trained interviewers using a standardized script. In addition to the validated instruments detailed below, evacuation and displacement characteristics of patients were collected through questions developed by the study investigators.
The Hurricane Coping Self-Efficacy (HCSE) measure is a validated 7-item tool designed to assess coping self-efficacy after major hurricanes.8;9 Response options for each HCSE item ranged from 1 to 7 on a Likert scale, with 1, 4 and 7 anchored as “not at all capable,” “moderately capable,” and “totally capable,” respectively. Participants were asked to rate how confident they felt in successfully dealing with situations related to Hurricane Katrina and the subsequent flooding in New Orleans, and instructed to respond with any number between 1 and 7. The 7 items were summed to produce an overall HCSE score, with a possible range from 7 to 49. Higher scores indicate greater coping self-efficacy.
To measure perceived health status, the validated second version of the Medical Outcomes Study 12-Item Short-Form Health Survey (SF-12) was administered.10;11 Individual items on the SF-12 compose 8 scales which are aggregated to produce summary measures of physical (physical component summary [PCS]) and mental health (mental component summary [MCS]). The PCS and MCS are normalized to a general population mean of 50 and an SD of 10 with higher scores indicating better perceived health status.11
Symptoms of depression were evaluated using the validated 10-item Center for Epidemiologic Studies Short Depression Form (CES-D).12 This scale is used to assess the frequency of symptoms of depression over the past week. Points for response options are 0 for “rarely or none of the time,” 1 for “some or a little of the time,” 2 for “occasionally or a moderate amount of time,” and 3 for “all of the time,” with positively phrased items reverse-coded. Overall scores are obtained through the summation of the 10 items with higher scores representing greater depressive symptomatology. The presence of symptoms of depression was defined by a score ≥10.3;12
In summary, higher scores for the HCSE, PCS and MCS are interpreted as reflecting better self-reported status, while lower scores on the CES-D indicate less depressive symptomatology. All aspects of the current study were approved by the Institutional Review Boards of Tulane University and the Ochsner Health System. Verbal informed consent was obtained from all patients.
Statistical Analysis
Correlations between psychosocial scales were examined using Spearman’s rank correlation coefficients to account for their non-normal distributions. Next, the age, race, and gender-standardized mean HCSE, PCS, MCS and CES-D scale scores were computed overall and by demographics and dialysis- and evacuation-related characteristics. Differences in mean scores across sub-grouping were assessed by t-tests using least squares estimation methods. In addition, the percentage of patients with depressive symptoms was calculated overall and by sub-grouping with the statistical significance of differences across sub-groups determined using maximum likelihood methods. Robust variance estimates for all analyses were calculated to account for within-clinic correlation of patients. Percentages within categories may not sum to 100% due to missing values. Less than 5% of data was missing for any variable. We performed all analyses using SAS 9.1 (Cary, NC) and SUDAAN 9.0.1 (Research Triangle Park, NC).
RESULTS
Significant pairwise associations were observed between the CES-D, PCS, MCS and HCSE with the exception of the correlation between PCS and MCS (each p<0.001; Table 1). The overall mean (SD) score was 36.2 (9.6) for HCSE, 37.1 (10.9) and 46.7 (12.7) for the PCS and MCS, respectively, and 10.0 (6.5) for the CES-D (Table 2). Symptoms of depression were identified in 45.5% of patients. Lower HCSE scores were observed among women and those living alone before the hurricane, while patients living with a roommate before the storm had lower scores on the MCS and higher scores on the CES-D scale. After adjustment for gender and race, patients ≥50 years of age had lower PCS scores. Patients more recently (<5 years prior) initiating treatment for ESRD had lower MCS, and higher CES-D scores after adjustment for age, race and gender.
Table 1.
Correlation coefficients between depression, physical and mental quality of life and coping self-efficacy scores among dialysis patients following Hurricane Katrina
| Correlation between factorsa | ||||
|---|---|---|---|---|
| CES-D | PCS | MCS | HCSE | |
| CES-D | 1.00 | - | - | - |
| PCS | -0.19b | 1.00 | - | - |
| MCS | -0.76b | -0.005 | 1.00 | - |
| HCSE | -0.43b | 0.27b | 0.32b | 1.00 |
CES-D –Center for Epidemiologic Studies Short Depression Scale, HCSE – Hurricane Coping Self-Efficacy Scale, MCS – mental component score, PCS – physical component score
Spearman correlation coefficients are reported due to the non-normality of some of the scale scores.
P<0.001
Table 2.
Age, race, gender-standardized mean psychosocial scale scores and percentage with symptoms of depression overall, and by demographic and dialysis-related characteristics of hemodialysis patients following Hurricane Katrina
| % of study participantse (N=391) | Standardized mean (SE) scored |
% (SE) with symptoms of depression | ||||
|---|---|---|---|---|---|---|
| HCSE | PCS | MCS | CES-D | |||
| Overall | 100.0 | 36.2 (0.5) | 37.1 (0.8) | 46.7 (0.6) | 10.0 (0.3) | 45.5 (2.5) |
| Age group, years | ||||||
| < 50 | 31.0 | 36.7 (0.8) | 39.6 (1.6) | 47.1 (0.6) | 9.8 (0.6) | 44.6 (5.3) |
| 50-64 | 36.8 | 35.3 (0.6) | 35.5 (1.0)b | 46.0 (1.2) | 10.8 (0.4) | 52.1 (2.5) |
| ≥65 | 32.2 | 36.9 (0.8) | 36.6 (0.7) | 47.3 (0.8) | 9.1 (0.7) | 38.9 (5.3) |
| Gender | ||||||
| Men | 51.7 | 37.1 (0.6) | 37.8 (0.9) | 47.5 (0.6) | 9.8 (0.3) | 45.1 (4.4) |
| Women | 48.3 | 35.3 (0.7)a | 36.4 (1.0) | 45.9 (0.8) | 10.1 (0.3) | 46.0 (3.2) |
| Race/ethnicity | ||||||
| White | 28.6 | 37.1 (0.7) | 35.9 (1.6) | 46.9 (1.6) | 9.8 (0.3) | 44.6 (3.7) |
| Black | 70.1 | 36.0 (0.5) | 37.7 (0.8) | 46.8 (0.8) | 10.0 (0.4) | 46.4 (3.5) |
| Time since initiation of ESRD treatment | ||||||
| ≥5 years | 34.5 | 35.8 (0.4) | 36.3 (1.4) | 49.4 (0.9) | 8.6 (0.5) | 41.5 (4.1) |
| 2-4 years | 31.2 | 36.6 (0.7) | 37.7 (0.9) | 45.2 (1.4)a | 11.0 (0.6)a | 48.4 (4.7) |
| <2 years | 34.3 | 36.4 (1.1) | 37.5 (1.3) | 45.4 (1.3) | 10.4 (0.4)a | 47.0 (2.2) |
| Cohabitation before Hurricane Katrina | ||||||
| Lived w/ spouse or partner | 39.9 | 37.3 (0.7) | 37.4 (1.1) | 47.1 (1.4) | 9.1 (0.6) | 39.1 (5.6) |
| Lived w/ family members | 37.1 | 35.8 (0.7) | 38.0 (0.9) | 46.5 (1.5) | 9.9 (0.7) | 46.2 (7.0) |
| Lived w/ roommate | 5.1 | 33.2 (2.0) | 34.6 (4.8) | 40.7 (2.7)a | 15.4 (1.1)b | 80.0 (5.4)c |
| Lived alone | 17.7 | 35.5 (1.0) | 34.9 (1.1) | 47.9 (1.4) | 10.5 (0.6) | 49.3 (4.8) |
CES-D –Center for Epidemiologic Studies Short Depression Scale, ESRD – end-stage renal disease, HCSE – Hurricane Coping Self-Efficacy Scale, MCS – mental component score, PCS – physical component score, SE – standard error
P<0.05;
P<0.01;
P<0.001
All scores except the overall are standardized to the age, race, and gender distribution of the overall study population.
Percentages within categories may not sum to 100% due to missing values (e.g., lack of patient recall).
Most participants evacuated prior to Hurricane Katrina making landfall on August 29, 2005, and 49.9% were displaced by the storm for at least 3 months (Table 3). A later evacuation from Hurricane Katrina was associated with lower scores on the HCSE and MCS, and higher scores on the CES-D. Patients who initially evacuated to a hotel had lower scores on the PCS, while those who evacuated to a shelter had lower MCS scores and a higher prevalence of depressive symptoms. Patients’ awareness of their dialysis unit’s evacuation plans was associated with a higher HCSE, and a lower CES-D score. Fear of dying during the week following the hurricane was associated with less favorable scores on all psychosocial measures. Patients who were hospitalized in the month after the storm reported lower scores on the PCS and higher scores on the CES-D scale. A longer displacement was associated with lower MCS scores and a higher prevalence of depressive symptoms.
Table 3.
Age, race, gender-standardized mean psychosocial scale scores and percentage with symptoms of depression by evacuation characteristics of hemodialysis patients following Hurricane Katrina
| % of study participantsg (N=391) | Standardized mean (SE) scored |
% (SE) with symptoms of depression | ||||
|---|---|---|---|---|---|---|
| HCSE | PCS | MCS | CES-D | |||
| Date of evacuation due to Hurricane Katrinae | ||||||
| On/before Aug 27, 2005 | 27.9 | 37.2 (0.6) | 37.6 (1.3) | 49.1 (1.0) | 8.2 (0.5) | 33.0 (4.5) |
| August 28, 2005 | 45.1 | 36.2 (0.8) | 37.3 (1.4) | 45.9 (1.0) | 10.3 (0.5)a | 48.2 (4.8)a |
| On/after Aug 29, 2005 | 22.0 | 34.8 (1.0) | 37.3 (0.8) | 45.3 (0.9)a | 11.2 (0.6)b | 55.7 (3.6)c |
| First evacuation locatione | ||||||
| Hotelf | 42.1 | 36.7 (0.9) | 35.8 (1.4) | 48.2 (1.0) | 9.2 (0.5) | 40.4 (3.0) |
| Shelter | 14.5 | 34.7 (1.2) | 38.6 (1.0)a | 43.0 (1.3)a | 11.6 (1.3) | 57.7 (4.6)b |
| Relative’s house | 34.8 | 36.1 (0.7) | 37.5 (1.1) | 46.2 (1.4) | 10.4 (0.6) | 46.4 (5.7) |
| Friend’s house | 8.1 | 35.5 (1.2) | 39.9 (1.5)a | 46.5 (3.2) | 9.8 (1.3) | 41.4 (6.7) |
| Aware of dialysis clinic’s evacuation plans | ||||||
| No | 37.9 | 35.1 (0.6) | 36.9 (1.4) | 45.9 (0.5) | 10.7 (0.3) | 47.3 (3.7) |
| Yes | 62.2 | 36.9 (0.5)b | 37.3 (0.6) | 47.3 (0.9) | 9.5 (0.3)a | 44.4 (3.1) |
| Fear of dying during one week after Hurricane Katrina | ||||||
| Not afraid at all | 56.5 | 38.4 (0.3) | 38.0 (1.1) | 49.5 (0.9) | 8.4 (0.4) | 36.7 (2.2) |
| Somewhat afraid | 17.4 | 35.5 (1.2)a | 37.7 (0.8) | 47.4 (1.4) | 9.4 (0.7) | 42.7 (5.2) |
| Moderately afraid | 10.5 | 33.3 (1.7)a | 35.0 (2.2) | 43.0 (2.2)a | 12.0 (1.0)a | 61.0 (7.1)c |
| Extremely afraid | 14.8 | 31.1 (2.0)b | 34.4 (0.8)b | 37.6 (1.7)c | 15.0 (1.0)b | 74.1 (5.4)c |
| Hospitalized one month after Hurricane Katrina | ||||||
| No | 76.0 | 36.7 (0.3) | 38.2 (0.8) | 47.2 (0.7) | 9.3 (0.2) | 43.1 (2.5) |
| Yes | 23.3 | 34.8 (1.6) | 33.7 (1.0)c | 45.9 (1.0) | 11.8 (0.6)b | 52.8 (4.7)a |
| Length of displacement | ||||||
| <3 months | 42.5 | 36.6 (1.0) | 36.7 (1.6) | 48.6 (1.1) | 9.0 (0.6) | 38.6 (4.0) |
| ≥3 months | 49.9 | 35.7 (0.7) | 37.6 (0.5) | 45.2 (1.0) | 10.8 (0.5) | 50.8 (4.2)a |
| Never displaced | 7.4 | 37.5 (2.0) | 36.9 (2.2) | 46.6 (0.9) | 9.8 (0.8) | 51.7 (4.6) |
| Still displaced at time of study interview | ||||||
| No | 65.7 | 36.5 (0.8) | 37.2 (1.2) | 47.7 (0.6) | 9.6 (0.3) | 42.8 (2.2) |
| Yes | 34.3 | 35.8 (0.8) | 36.9 (0.8) | 44.8 (0.7)c | 10.6 (0.5) | 50.8 (5.1) |
CES-D –Center for Epidemiologic Studies Short Depression Scale, HCSE – Hurricane Coping Self-Efficacy Scale, MCS – mental component score, PCS – physical component score, SE – standard error
P<0.05;
P<0.01;
P<0.001
Standardized to the age, race, and gender distribution of the overall study population.
Among study participants who evacuated.
This category includes patients whose first evacuation location was unspecified.
Percentages within categories may not sum to 100% due to missing values (e.g., lack of patient recall).
DISCUSSION
The current study identified several groups of hemodialysis patients with deficits in psychosocial adaptation after Hurricane Katrina. Symptoms of depression were common and associated with impaired coping skills. Evacuation and displacement characteristics were associated with poor psychosocial status, of which the most consistent predictors were a later evacuation and fear of dying during the week following the hurricane.
The unique interaction of medical and psychological factors in the development of depression in hemodialysis patients was posited by Kimmel and colleagues in the non-disaster setting.13 In the current study, we demonstrate that many of the same medical and psychosocial factors may interact with aspects of an evacuation and coping abilities with greater degrees of depressive symptomatology among hemodialysis patients facing a traumatic event.
Significant differences in mean scores across groups of hemodialysis patients may not universally correlate to clinically meaningful disparities in psychosocial status. However, there is evidence that differences in the current study are clinically important, as similar differences in scores on these instruments have been associated with adverse outcomes, including death, in other populations of hemodialysis patients.3;14 The mean coping self-efficacy scale scores among hemodialysis patients who survived Hurricane Katrina were lower, indicating lower coping self-efficacy, than previously reported estimates derived from the general population who survived Hurricanes Andrew and Opal in Florida.9 This difference is noteworthy as significant associations have been reported between coping self-efficacy and psychosocial outcomes including quality of life and depression in hemodialysis patients.15;16
Previous studies including large samples of dialysis patients reported mean PCS scores between 32.7 and 35.2 and mean MCS scores between 46.9 and 47.9.17-19 Differences in PCS and MCS scores between previous studies and the current findings may be attributable to characteristics beyond the disaster setting such as dialysis-related characteristics and stressors. Nonetheless, it is interesting to note the current study population had a higher mean PCS and a lower mean MCS, possibly revealing the better self-rated physical, but not mental, state of Hurricane Katrina survivors. The finding of a higher mean PCS could indicate a survivor effect among participants in the current study, with patients of poorer health not surviving until the time of interview. Depressive scores and symptom prevalence were higher in the current study (mean=10.0, SD=6.5 and prevalence of depressive symptoms=45.5%) than among hemodialysis patients in the Dialysis Outcomes and Practice Patterns Study (DOPPS) (mean=8.7, SD=5.6 and prevalence of depressive symptoms=39.2%).3 Given the lack of data on patients’ depressive symptoms prior to Hurricane Katrina, assessing changes in symptoms of depression from before to after the event was not possible.
Several evacuation-related characteristics were associated with impaired psychosocial status during the study period. The current study demonstrated that a delayed evacuation, placement in a shelter, lack of evacuation plan awareness and a longer displacement were related to poor psychosocial health in the aftermath of the disaster. Findings from the current study point to the importance of coping processes in the recovery from a natural disaster and support the structure of the proposed conceptual model. A randomized, controlled trial demonstrated that an empowerment program significantly improved dialysis patients’ self-efficacy and reduced symptoms of depression.20 Similar programs designed within the context of a post-disaster setting may help alleviate stress responses in the hemodialysis population and improve long-term outcomes following disasters of the future.
Several limitations of this study are acknowledged. No pre-disaster data from this region were available, so assessments of changes in psychosocial health were not possible. Study interviews were conducted seven to fourteen months after Hurricane Katrina, and previous recommendations for use of the HCSE measure indicate that the scale may be best suited for assessments during the acute phase of recovery (<5 months post-disaster).9 However, given the widespread damage and long-lasting interruption of services in the affected area, exposure to the hurricane and flooding extended beyond the short timeline of the event itself. Despite these limitations, the current study has several noteworthy strengths. Almost 400 hemodialysis patients (participation rate=85.6%) completed the study interview, and were similar to all hemodialysis patients impacted by Hurricane Katrina.7 The current study utilized validated instruments and is the first, to our knowledge, to report on multiple psychosocial domains for hemodialysis patients following a natural disaster.
A high degree of depressive symptoms and reduced perceived health status was observed in hemodialysis patients following Hurricane Katrina. Psychosocial adaptation to this disaster was mediated by coping skills, and specific patient groups including those more recently initiating ESRD treatment and patients who lived alone or with a roommate prior to the storm reporting more impaired psychosocial functioning. The importance of an early evacuation, evacuating to a location other than a shelter, awareness of evacuation plans and a shorter displacement in the psychological recovery from a large disaster was noted. Targeted coping programs and interventions aimed at improving psychosocial health may improve the recovery of hemodialysis patients after future disasters.
Acknowledgments
This study was supported by a subcontract to Tulane University from the National Institutes of Health contract N01-DK-1-2471. The interpretation and reporting of the data presented here are the responsibility of the authors and in no way should be seen as an official policy or interpretation of the United States government.
Sources of Support: Subcontract from the National Institutes of Health: N01-DK-1-2471
References
- 1.Johnson DL. Silver Spring, MD: US Department of Commerce National Oceanic and Atmospheric Administration, National Weather Service; 2006. [July 9, 2006]. Service Assessment: Hurricane Katrina, August 23-31, 2005. at: http://www.nws.noaa.gov/om/assessments/pdfs/Katrina.pdf. [Google Scholar]
- 2.Ford ES, Mokdad AH, Link MW, et al. Chronic disease in health emergencies: in the eye of the hurricane. Prev Chronic Dis. 2006;3:A46. [PMC free article] [PubMed] [Google Scholar]
- 3.Lopes AA, Albert JM, Young EW, et al. Screening for depression in hemodialysis patients: associations with diagnosis, treatment, and outcomes in the DOPPS. Kidney Int. 2004;66:2047–53. doi: 10.1111/j.1523-1755.2004.00977.x. [DOI] [PubMed] [Google Scholar]
- 4.Kimmel PL, Cukor D, Cohen SD, et al. Depression in end-stage renal disease patients: a critical review. Adv Chronic Kidney Dis. 2007;14:328–34. doi: 10.1053/j.ackd.2007.07.007. [DOI] [PubMed] [Google Scholar]
- 5.Kimmel PL, Patel SS. Quality of life in patients with chronic kidney disease: focus on end-stage renal disease treated with hemodialysis. Semin Nephrol. 2006;26:68–79. doi: 10.1016/j.semnephrol.2005.06.015. [DOI] [PubMed] [Google Scholar]
- 6.Cameron JI, Whiteside C, Katz J, et al. Differences in quality of life across renal replacement therapies: a meta-analytic comparison. Am J Kidney Dis. 2000;35:629–37. doi: 10.1016/s0272-6386(00)70009-6. [DOI] [PubMed] [Google Scholar]
- 7.Hyre AD, Cohen AJ, Kutner NG, et al. Prevalence and predictors of post-traumatic stress disorder among hemodialysis patients following Hurricane Katrina. Am J Kidney Dis. 2007;50:585–93. doi: 10.1053/j.ajkd.2007.07.013. [DOI] [PubMed] [Google Scholar]
- 8.Benight CC, Harper ML. Coping self-efficacy perceptions as a mediator between acute stress response and long-term distress following natural disasters. J Trauma Stress. 2002;15:177–86. doi: 10.1023/A:1015295025950. [DOI] [PubMed] [Google Scholar]
- 9.Benight CC, Ironson G, Durham RL. Psychometric properties of a hurricane coping self-efficacy measure. J Trauma Stress. 1999;12:379–86. doi: 10.1023/A:1024792913301. [DOI] [PubMed] [Google Scholar]
- 10.Ware J, Jr, Kosinski M, Keller SD. A 12-Item Short-Form Health Survey: construction of scales and preliminary tests of reliability and validity. Med Care. 1996;34:220–33. doi: 10.1097/00005650-199603000-00003. [DOI] [PubMed] [Google Scholar]
- 11.Ware J, Jr, Kosinski M, Turner-Bowker DM, et al. How to score version 2 of the SF-12 health survey (with a supplement documenting version 1) Lincoln, RI: QualityMetric,Incorporated; 2002. [Google Scholar]
- 12.Andresen EM, Malmgren JA, Carter WB, et al. Screening for depression in well older adults: evaluation of a short form of the CES-D (Center for Epidemiologic Studies Depression Scale) Am J Prev Med. 1994;10:77–84. [PubMed] [Google Scholar]
- 13.Kimmel PL, Weihs K, Peterson RA. Survival in hemodialysis patients: the role of depression. J Am Soc Nephrol. 1993;4:12–27. doi: 10.1681/ASN.V4112. [DOI] [PubMed] [Google Scholar]
- 14.Kalantar-Zadeh K, Kopple JD, Block G, et al. Association among SF36 quality of life measures and nutrition, hospitalization, and mortality in hemodialysis. J Am Soc Nephrol. 2001;12:2797–806. doi: 10.1681/ASN.V12122797. [DOI] [PubMed] [Google Scholar]
- 15.Tsay SL, Healstead M. Self-care self-efficacy, depression, and quality of life among patients receiving hemodialysis in Taiwan. Int J Nurs Stud. 2002;39:245–51. doi: 10.1016/s0020-7489(01)00030-x. [DOI] [PubMed] [Google Scholar]
- 16.Tovbin D, Gidron Y, Jean T, et al. Relative importance and interrelations between psychosocial factors and individualized quality of life of hemodialysis patients. Qual Life Res. 2003;12:709–17. doi: 10.1023/a:1025101601822. [DOI] [PubMed] [Google Scholar]
- 17.Lowrie EG, Curtin RB, LePain N, et al. Medical outcomes study short form-36: a consistent and powerful predictor of morbidity and mortality in dialysis patients. Am J Kidney Dis. 2003;41:1286–92. doi: 10.1016/s0272-6386(03)00361-5. [DOI] [PubMed] [Google Scholar]
- 18.Curtin RB, Klag MJ, Bultman DC, et al. Renal rehabilitation and improved patient outcomes in Texas dialysis facilities. Am J Kidney Dis. 2002;40:331–8. doi: 10.1053/ajkd.2002.34517. [DOI] [PubMed] [Google Scholar]
- 19.DeOreo PB. Hemodialysis patient-assessed functional health status predicts continued survival, hospitalization, and dialysis-attendance compliance. Am J Kidney Dis. 1997;30:204–12. doi: 10.1016/s0272-6386(97)90053-6. [DOI] [PubMed] [Google Scholar]
- 20.Tsay SL, Hung LO. Empowerment of patients with end-stage renal disease--a randomized controlled trial. Int J Nurs Stud. 2004;41:59–65. doi: 10.1016/s0020-7489(03)00095-6. [DOI] [PubMed] [Google Scholar]