

Abstract
Intracerebral hemorrhage is by far the most destructive form of stroke. The clinical presentation is characterized by a rapidly deteriorating neurological exam coupled with signs and symptoms of elevated intracranial pressure. The diagnosis is easily established by the use of computed tomography or magnetic resonance imaging. Ventilatory support, blood pressure control, reversal of any preexisting coagulopathy, intracranial pressure monitoring, osmotherapy, fever control, seizure prophylaxis, treatment of hyerglycemia, and nutritional supplementation are the cornerstones of supportive care in the intensive care unit. Dexamethasone and other glucocorticoids should be avoided. Ventricular drainage should be performed urgently in all stuporous or comatose patients with intraventricular blood and acute hydrocephalus. Emergent surgical evacuation or hemicraniectomy should be considered for patients with large (>3 cm) cerebellar hemorrhages, and in those with large lobar hemorrhages, significant mass effect, and a deteriorating neurological exam. Apart from management in a specialized stroke or neurological intensive care unit, no specific medical therapies have been shown to consistently improve outcome after intracerebral hemorrhage.
Introduction
Intracerebral hemorrhage (ICH) is defined as the spontaneous extravasation of blood into the brain parenchyma. Non-traumatic forms of ICH account for 10% to 30% of all stroke hospital admissions [1], leading to catastrophic disability, morbidity, and a mortality of 30% to 50% at 30 days [1]. Death at 1 year varies by different location: 51% for deep, 57% for lobar, 42% for cerebellar and 65% for brain stem hemorrhages [2]. In a recent population-based study, the overall incidence of ICH was estimated to be 12 to 15 cases per 100,000 population [3]. The cost of ICH alone is estimated to be USD $125,000 per person per year, with a total cost of USD $6 billion per year in the United States alone [4,5] related to both acute and chronic medical care costs, as well as the loss of productivity.
Depending on the underlying cause of hemorrhage, ICH may be classified as primary when it originates from the spontaneous rupture of small arterioles damaged by chronic hypertension or cerebral amyloid angiopathy, representing at least 85% of all cases; or secondary when associated with vascular malformations, bleeding related to an ischemic stroke, tumors, abnormal coagulation [6,7], trauma [8], or vasculitis. In approximately 40% of the cases, blood may also extend into the ventricles – intra-ventricular hemorrhage (IVH) – potentially leading to neurological death related to acute obstructive hydrocephalus resulting in a substantial worsening of the prognosis.
Despite ongoing attempts to find effective interventions based on the physiopathological understanding of this disease, options are limited, and outcomes remain poor. Evidence-based medical therapies for ICH are limited to guidelines or options regarding blood pressure (BP) reduction, intracranial pressure (ICP) monitoring, osmotherapy with adequate fluid resuscitation, fever and glycemic control, seizure prophylaxis, and care in a specialized stroke or neurological intensive care unit (ICU) [9]. Recently published guidelines for the management of spontaneous ICH in adults [2] provide a helpful set of evidence-based recommendations for the management of this form of stroke. This review summarizes current therapeutic options for ICH based on the American Heart Association Guidelines. A summary of the methods for the classification of the level of evidence is shown in Table 1[10].
Table 1.
Definition of classes and levels of evidence used in AHA recommendations
| Class I | Conditions for which there is evidence for and/or general agreement that the procedure or treatment is useful and effective |
| Class II | Conditions for which there is conflicting evidence and/or a divergence of opinion about the usefulness/efficacy of a procedure or treatment |
| Class IIa | Weight of evidence or opinion is in favor of the procedure or treatment |
| Class IIb | Usefulness/efficacy is less well established by evidence or opinion |
| Class III | Conditions for which there is evidence and/or general agreement that the procedure or treatment is not useful/effective and in some cases may be harmful |
| Level of Evidence A | Data derived from multiple randomized trials |
| Level of Evidence B | Data derived from a single randomized trial or non-randomized trials |
| Level of Evidence C | Expert Opinion or case studies |
From [10].
Risk factors
Hypertension is the most important and prevalent risk factor for ICH [11]. In a study of 331 patients, hypertension increased the risk of ICH by more than two-fold, especially in patients younger than 55 years of age who stopped anti-hypertensive treatment [12]. Hypertension causes a chronic small-vessel vasculopathy characterized by fragmentation, degeneration, and the eventual rupture of small penetrating vessels within the brain (lipohyalinosis) [13]. Commonly affected structures include the basal ganglia and thalamus (50%), lobar regions (33%), and brainstem and cerebellum (17%) [6,14].
Low cholesterol levels have been implicated as a risk factor for primary ICH. There is controversy regarding this association as the results from case-control and cohort studies have suggested that lower cholesterol levels imparted an increased risk of ICH [15-17]. The results of additional cohort-studies [18] and recent cardiac trials that have evaluated the effects of statin therapy have failed to confirm this association [19]. However, the more recent results of the Stroke Prevention by Aggressive Reduction in Cholesterol Levels Study (SPARCL) showed that in patients with recent stroke or transient ischemic attack, 80 mg of atorvastatin per day reduced the overall incidence of strokes and of cardiovascular events for over 5 years, despite a small increase in the incidence of hemorrhagic stroke [20].
Heavy alcohol intake has been implicated as a risk factor for ICH in recent case-control studies [21-25]. This effect may be mediated in part by hypertension, but those studies that controlled for it have supported an independent association. In theory, alcohol may affect platelet function, coagulation physiology, and enhance vascular fragility [23].
Cigarette smoking has not been linked to an increased risk of ICH. However, a retrospective study found that smokers with hypertension have an increased risk of ICH [12], an effect that is mediated by hypertension and not by tobacco abuse per se. Similarly, ICH may be a complication of incidental or chronic cocaine use [26-28].
Non-modifiable risk factors for ICH include advanced age [29,30], male gender, and African-American or Japanese race/ethnicity [28,31]. Cerebral amyloid angiopathy is an important risk factor for ICH in the elderly. It is characterized by the deposition of β-amyloid protein in small- to medium-sized blood vessels of the brain and leptomeninges, which may undergo fibrinoid necrosis. It can occur as a sporadic disorder, in association with Alzheimer's disease, or with certain familial syndromes (apolipoprotein ε2 and ε4 allele) [7].
Initial approach
Diagnosis
Widespread use of non-enhancing computed tomography (CT) scan of the brain has dramatically changed the diagnostic approach of this disease, making it the method of choice to evaluate the presence of ICH (Figure 1). CT scan evaluates the size and location of the hematoma, extension into the ventricular system, degree of surrounding edema, and anatomical disruption (Class I, Level of Evidence A). Hematoma volume may be easily calculated from CT scan images by use of the ABC÷2 method, a derived formula from the calculation of the volume of the sphere [32,33].
Figure 1.
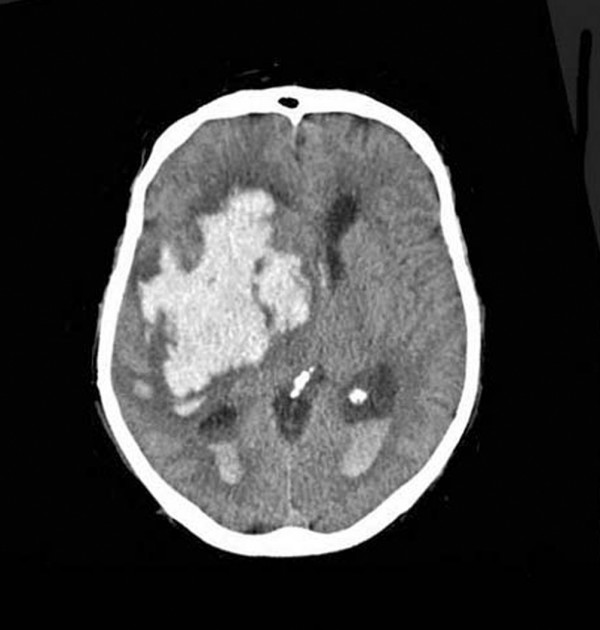
Computed tomography scan of patient with intracerebral hemorrhage.
CT-angiography is not routinely performed in most centers, but may prove helpful in predicting hematoma expansion and outcomes [34,35]. In a recent prospective study of 39 patients with spontaneous ICH, focal enhancing foci (contrast extravasation, 'spot sign') seen in initial CT-angiography were associated with the presence and extent of hematoma progression with good sensitivity (91%) and negative predictive value (96%) (Figure 2) [36]. Magnetic resonance imaging (MRI) techniques, such as gradient-echo (GRE, T2*), are highly sensitive for the diagnosis of ICH as well. Sensitivity of MRI for ICH is 100%. In the HEME Study, MRI and CT were equivalent for the detection of acute ICH but MRI was significantly more accurate than CT for the detection of chronic ICH [37].
Figure 2.

Contrast extravasation seen in the hematoma of a patient with acute coagulopathic intracerebral hemorrhage (white arrows).
Conventional diagnostic cerebral angiography should be reserved for patients in whom secondary causes of ICH are suspected, such as aneurysms, arteriovenous malformations, cortical vein or dural sinus thrombosis, or vasculitis. Findings on CT scan or MRI that should prompt angiographic study include the presence of subarachnoid hemorrhage, IVH, underlying calcification, or lobar hemorrhage in non-hypertensive younger patients. The role of angiography after ICH has been addressed by two studies. Zhu and colleagues [38] reported abnormalities on angiography in 48% of patients who were normotensive and younger than 45 years of age, 49% of patients with lobar hemorrhages, 65% with isolated IVH, and no abnormalities in patients older than 45 years who had a history of hypertension with subcortical ICH. In a second study, Halpin and colleagues [39] reported finding an underlying lesion in 84% of patients that appeared to have a structural abnormality seen previously on brain imaging. Diagnostic catheter angiography should be strongly considered in all patients with primary IVH and younger non-hypertensive patients with lobar ICH.
Airway control, breathing, and circulation
Rapid neurological deterioration and ensuing loss of consciousness with impairment of reflexes that maintain the airway mandate permanent airway control (Figure 3) [40] (Class I, Level of Evidence B). Failure to recognize imminent airway loss may result in complications, such as aspiration, hypoxemia, and hypercapnia. Preferred induction agents for rapid sequence intubation (RSI) in the setting of ICH include propofol [41] and etomidate [42] (Table 2), both of which are short-acting agents that will not obscure the neurological exam for a prolonged period of time (Class IIA, Level of Evidence B). Adverse effects of propofol include drug-induced hypotension that usually responds to fluid infusion [42]. Adverse effects of etomidate include nausea, vomiting, myoclonic movements, lowering of seizure threshold [42], and adrenal suppression [43]. Unfavorable effects on the ICP have been reported with the use of midazolam [41,44]. In certain circumstances, neuromuscular paralysis may be needed as part of RSI. Succinylcholine is the most commonly administered muscle relaxant for RSI, owing to its rapidity of onset (30 to 60 s) and short duration (5 to 15 minutes) [45]. However, side effects of succinylcholine include hyperkalemia, cardiac arrhythmias, exacerbation of neuropathy or myopathy, malignant hyperthermia, and elevation of intracranial pressure in patients with intracranial mass lesions [42,46]. For this reason, in neurological patients, non-depolarizing neuromuscular blocking agents, such as cisatracurium [47], rocuronium [42], or vecuronium, are preferred [48] (Class IIA, Level of Evidence B). In patients with increased ICP, pre-medication with intravenous lidocaine for RSI is of questionable use [49].
Figure 3.
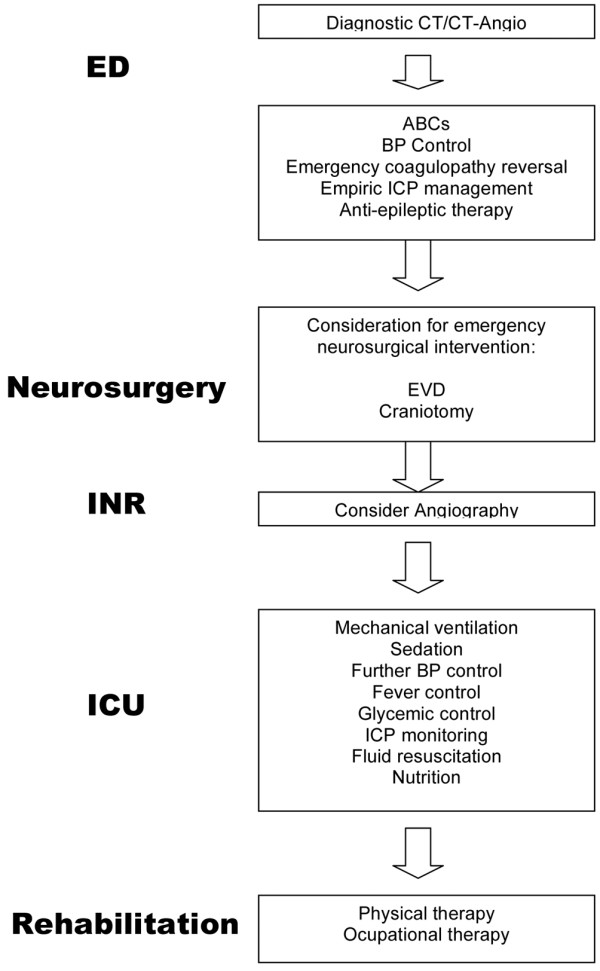
Approach to intracerebral hemorrhage from the emergency department to the intensive care unit.
Table 2.
Intravenous antihypertensive agents for acute intracerebral hemorrhage
| Drug | Mechanism | Dose | Cautions |
| Labetalol | Alpha-1, beta-1, beta-2 receptor antagonist | 20–80 mg bolus every 10 minutes, up to 300 mg; 0.5 to 2.0 mg/minute infusion | Bradycardia, congestive heart failure, bronchospasm, hypotension |
| Esmolol | Beta-1 receptor antagonist | 0.5 mg/kg bolus; 50 to 300 μg/kg/minute | Bradycardia, congestive heart failure, bronchospasm |
| Nicardipine | L-type calcium channel blocker (dihydropyridine) | 5 to 15 mg/h infusion | Severe aortic stenosis, myocardial ischemia, hypotension |
| Enalaprilat | ACE inhibitor | 0.625 mg bolus; 1.25 to 5 mg every 6 h | Variable response, precipitous fall in blood pressure with high-renin states |
| Fenoldopam | Dopamine-1 receptor agonist | 0.1 to 0.3 μg/kg/minute | Tachycardia, headache, nausea, flushing, glaucoma, portal hypertension |
| Nitroprusside* | Nitrovasodilator (arterial and venous) | 0.25 to 10 μg/kg/minute | Increased intracranial pressure, variable response, myocardial ischemia, thiocyanate and cyanide toxicity, hypotension |
*Nitroprusside is not recommended for use in acute intracerebral hemorrhage because of its tendency to increase intracranial pressure. Modified with permission from Mayer SA, Rincon F: Management of intracerebral hemorrhage. Lancet Neurol 2005, 4: 662–672. ACE, angiotensin-converting enzyme.
Isotonic fluid resuscitation and vasopressors are indicated for patients in shock [2]. Dextrose-containing solutions should be avoided as hyperglycemia may be detrimental to the injured brain [50] (Class III, Level of Evidence C). Additionally, a thorough laboratory panel should be obtained, including hematological, biochemical, coagulation profiles, echocradiogram and chest X-rays.
Blood pressure control
Extreme levels of BP after ICH should be aggressively but carefully treated to reduce the risk of hematoma expansion and to keep and maintain cerebral perfusion pressure (CPP; CPP = mean arterial pressure (MAP) – ICP). Controversy exists about the initial treatment of high BP in patients with ICH. An expanding hematoma may result from persistent bleeding and/or re-bleeding from a single arteriolar rupture. Some studies have reported evidence of hematoma growth from bleeding into an ischemic penumbra zone surrounding the hematoma [51,52] but other reports have not confirmed the existence of ischemia at the hypoperfused area in the periphery of the hematoma.
In the study by Brott and colleagues [53], no association was demonstrated between hematoma growth and levels of BP, but the use of anti-hypertensive agents may have negatively confounded this association. Similarly, initial BP was not associated with hematoma growth in the Recombinant Activated Factor VII ICH Trial [54]. Moreover, aggressive blood pressure reduction after ICH may predispose to an abrupt drop in CPP and ischemia, which, in turn, may be accompanied by elevations of ICP and further neurological damage. In a recent pilot trial of BP reduction after ICH, 14 patients with supratentorial ICH were randomized to receive either labetalol or nicardipine within 22 hours of onset to lower the MAP by 15%. Cerebral blood flow (CBF) studies were performed before and after treatment with positron emission tomography and [15O] water. No changes in global or peri-hematoma CBF were observed [55]. Two additional studies have demonstrated that a controlled, pharmacologically based reduction in BP has no adverse effects on CBF in humans or animals [56,57]. BP level has been correlated with increases in the ICP and volume of the hematoma but it has been very difficult to explain if hypertension is the cause of hematoma growth or if this is just a response to elevated ICP in the setting of large volume ICH to maintain cerebral perfusion.
In general, the American Heart Association Guidelines indicate that systolic blood pressures exceeding 180 mmHg or MAP exceeding 130 mmHg should be managed with continuous infusion antihypertensive agents such as labetalol, esmolol, or nicardipine [2] (Class IIB, Level of Evidence C). Urapidil, a sympatholytic agent with vasodilator properties is an alternative but it is currently not approved for use in the US. Use of nitroprusside has drawbacks since this agent may exacerbate cerebral edema and intracranial pressure [58].
Oral and sub-lingual agents are not preferred, because of the need for immediate and precise BP control. There are few, if any, comparative or randomized trials providing definitive conclusions about the efficacy and safety of comparative agents.
In comatose patients, it is recommended to monitor ICP and to titrate vasopressors to maintain CPP in the range 70 to 90 mmHg. Use of brain tissue oxygen and thermodilution CBF probes to detect reductions in perfusion related to excessive lowering of BP is gaining in popularity. In general, no matter how high the BP is, the MAP should not be reduced beyond 15% to 30% over the first 24 hours [56]. In the setting of impaired blood flow autoregulation, excessive blood pressure reduction may exacerbate ischemia in the area surrounding the hematoma and worsen peri-hematomal brain injury [59,60] (Table 2; Figure 3). In fact transcranial doppler velocities become positively correlated with CPP when CPP drops below the left side of the autoregulation curve [61].
Whether more aggressive BP reduction after ICH is safe is the matter of the ongoing National Institute of Neurological Diseases and Stroke supported Antihypertensive Treatment in Acute Cerebral Hemorrhage (ATACH) pilot study [62]. Additionally, the ongoing phase III Intensive Blood Pressure Reduction in Acute Cerebral Hemorrhage Trial (INTERACT) will test the hypothesis that lowering BP acutely after ICH will reduce the chances of dying or surviving with long-term disability [63].
Though no prospective study has addressed the timing of conversion from intravenous to oral anti-hypertensive management, this process can generally be started after 24 to 72 hours, as long as the patient's condition has stabilized [6].
Initial emergency intracranial pressure management
Emergency measures for ICP control are appropriate for stuporous or comatose patients, or those who present acutely with clinical signs of brain stem herniation (that is, pupillary abnormalities or motor posturing; Figure 3). The head should be elevated to 30 degrees, 1.0 to 1.5 g/kg of 20% mannitol should be administered by a rapid infusion, and the patient should be hyperventilated to a pCO2 of 26 to 30 mmHg (Class IIA, Level of Evidence B). As a second line therapy, or if the patient is relatively hypotensive, 0.5 to 2.0 ml/kg of 23.4% saline solution can be administered through a central venous line [64] (Class IIA, Level of Evidence B). These measures are designed to lower ICP as quickly and effectively as possible, in order to 'buy time' before a definitive neurosurgical procedure (craniotomy, ventriculostomy (Class IIA, Level of Evidence B), or placement of an ICP monitor) can be performed (Table 3). Corticosteroids are contraindicated based on the results of randomized trials that have failed to demonstrate their efficacy in ICH [65,66] (Class III, Level of Evidence B). Neurosurgical consultation is warranted for those patients with rapidly declining mental status and hydrocephalus with IVH seen in the initial CT scan. Early placement of a ventricular drain in this case may be life-saving [67] (Class IIA, Level of Evidence B; Figure 3).
Table 3.
Stepwise treatment protocol for elevated intracranial pressure* in a monitored patient in the intensive care unit
| 1. Surgical decompression | Consider repeat CT scanning, and definitive surgical intervention or ventricular drainage |
| 2. Sedation | Intravenous sedation to attain a motionless, quiet state |
| 3. CPP optimization | Vasopressor infusion if CPP is <70 mmHg, or reduction of blood pressure if CPP is >110 mmHg (preferred agents are phenylephrine, vasopressin, nor-epinephrine) |
| 4. Osmotherapy | Mannitol 0.25 to 1.5 g/kg IV or 0.5 to 2.0 ml/kg 23.4% hypertonic saline (repeat every 1 to 6 hours as needed) |
| 5. Controlled hyperventilation | Target PaCO2 levels of 26 to 30 mmHg |
| 6. High dose pentobarbital therapy | Load with 5 to 20 mg/kg, infuse 1 to 4 mg/kg/h |
| 7. Hypothermia | Cool core body temperature to 32 to 33°C |
*Elevated intracranial pressure ≥20 mmHg. Adapted from Mayer SA, Chong J: Critical care management of increased intracranial pressure. J Int Care Med 2002, 17: 55–67. CPP, cerebral perfusion pressure; CT, computed tomography; IV, intravenous; PaCO2 = arterial partial pressure of carbon dioxide.
Hemostatic therapy
Hematoma size is an important determinant of mortality after ICH and early hematoma growth, which is the increase in hematoma size within 6 hours after onset, is consistently associated with poor clinical outcomes [53,68-70] and an increased mortality rate [70]. As a corollary, hematoma growth occurs in only 5% of patients who are initially scanned beyond 6 hours of symptom onset. Similarly, significantly greater reductions in the Glasgow Coma Scale (GCS) and National Institute of Health Stroke Scale (NIHSS) have been reported among patients with documented hematoma growth on 1-hour follow-up CT scans, versus those without growth [53]. These observations suggest that the reduction in hematoma growth may be an important strategy for improvement of survival and outcome after ICH.
To be effective, hematostatic therapy must be given early after the onset of ICH. Even if a hemostatic intervention is completely effective, substantial hematoma enlargement (that is, a >33% increase from baseline) would be expected to occur in 10%, 17% and 21% of patients after a 15-, 30-, or 45-minute treatment delay following the baseline scan [53]. Underlying this principle is the fact that the only consistently identified predictor of early hematoma growth is the interval from the onset of symptoms to CT: the earlier the first scan is obtained, the more likely subsequent bleeding will be detected on a follow-up scan [53,69,70]. Importantly, hematoma growth occurs in only 5% of patients who are initially scanned beyond 6 hours of symptom onset [53,69,70].
Recombinant factor VII (rFVIIa, Novoseven®, Novo Nordisk) is a powerful initiator of hemostasis that is currently approved for the treatment of bleeding in patients with hemophilia who are resistant to factor VIII replacement therapy. Considerable evidence exists suggesting that rFVIIa may enhance hemostasis in patients with normal coagulation systems as well. In a randomized, double blind, placebo controlled study, 399 patients with spontaneous ICH received treatment with rFVIIa at doses of 40, 80, or 160 μg/kg within 4 hours after ICH onset. The primary outcome of the study was change in hematoma volume at 24 hours, a direct measure of hematoma growth. Secondary outcomes included clinical outcome at three months as measured by Modified Ranking Scale, Barthel Index, Extended GCS and NIHSS. Use of rFVIIa was associated with a 38% reduction in mortality and significantly improved functional outcomes at 90 days, despite a 5% increase in the frequency of arterial thromboembolic adverse events [71]. A similar pilot trial of epsilon aminocaproic acid, an anti-fibrinolytic agent, has been conducted with negative results [72].
In May of 2008, the results of the phase III Factor VIIa for Acute Hemorrhagic Stroke Trial (FAST) were published. This study compared doses of 80 and 20 μg/kg of rFVIIa with placebo in an overall trial population of 841 patients. No significant difference was found in the main outcome measure, which was the proportion of patients suffering death or with severe disability according to the modified Rankin scale at 90 days (score of 5 or 6) but the hemostatic effect and side effect profiles were confirmed [73]. On the basis of these results, routine use of rFVIIa as a hemostatic therapy for all patients with ICH within a 4-hour time window cannot be recommended (Class III, Level of Evidence B). Future studies to test rFVIIa in younger patients who present within an earlier time-frame are needed.
Reversal of anticoagulation
Anticoagulation with warfarin increases the risk of ICH by 5-to 10-fold in the general population [74], and approximately 15% of ICH cases overall are associated with its use. Among ICH patients, warfarin increases the risk of progressive bleeding and clinical deterioration, and doubles the risk of mortality [75]. Failure to rapidly normalize the international normalized ratio (INR) to below 1.4 further increases these risks [76]. Patients with ICH receiving warfarin should be reversed immediately with fresh frozen plasma (FFP; Class IIB, Level of Evidence B) or prothrombin-complex concentrate [77,78] (Class IIB, Level of Evidence B), and vitamin K (Class I, Level of Evidence B) [79] (Table 4). Treatment should never be delayed in order to check coagulation tests. Unfortunately, normalization of the INR with this approach usually takes several hours, and clinical results are often poor. The associated volume load with FFP may also cause congestive heat failure in the setting of cardiac or renal disease. Prothrombin complex concentrate contains vitamin K-dependent coagulation factors II, VII, IX, and X, normalizes the INR more rapidly than FFP, and can be given in smaller volumes, but carries a higher risk for developing disseminated intra-vascular coagulation [76].
Table 4.
Emergency management of the coagulopathic intracerebral hemorrhage patient
| Scenario | Agent | Dose | Comments | Level of Evidence* |
| Warfarin | Fresh frozen plasma | 15 ml/kg | Usually 4 to 6 units (200 ml) each are given | B |
| or | ||||
| Prothrombin complex concentrate | 15 to 30 U/kg | Works faster than fresh frozen plasma, but carries risk of disseminated intravascular coagulation | B | |
| and | ||||
| Intravenous vitamin K | 10 mg | Can take up to 24 hours to normalize international normalized ratio | B | |
| Warfarin and emergency neurosurgical intervention | Above plus rFVIIa | 20 to 80 μg/kg | Contraindicated in acute thromboembolic disease | C |
| Unfractionated or low molecular weight heparin† | Protamine sulfate | 1 mg per 100 units of heparin, or 1 mg of enoxaparin | Can cause flushing, bradycardia, or hypotension, anticoagulation | C |
| Platelet dysfunction or thrombocytopenia | Platelet transfusion | 6 units | Range 4 to 8 units based on size; transfuse to >100,000 | C |
| and/or | ||||
| Desmopressin (DDAVP) | 0.3 μg/kg | Single dose required | C |
*See Table 1 for descriptions of Levels of Evidence. †Protamine has minimal efficacy against danaparoid or fondaparinux. Reproduced with permission from Mayer SA, Rincon F: Management of intracerebral hemorrhage. Lancet Neurol 2005, 4: 662–672. rFVIIa, recombinant factor VII.
Recent reports have described the use of rFVIIa to speed the reversal of warfarin anticoagulation in ICH patients [80]. A single intravenous dose of rFVIIa can normalize the INR within minutes, with larger doses producing a longer duration of effect, a response seen in healthy volunteers [81]. Doses of rFVIIa ranging from 10 to 90 μg/kg have been used to reverse the effects of warfarin in acute ICH in order to expedite acute neurosurgical interventions with good clinical results (Class IIB, Level of Evidence C) [80,82]. When this approach is used, rFVIIa should be used as an adjunct to coagulation factor replacement and vitamin K, since its effect lasts only several hours. Patients with ICH who have been anticoagulated with unfractionated or low-molecular weight heparin should be reversed with protamine sulfate [83] (Class I, Level of Evidence B) and patients with thrombocytopenia or platelet dysfunction can be treated with a single dose of desmopressin, platelet transfusions, or both [84] (Class IIB, Level of Evidence C) (Table 4). Re-starting anticoagulation in patients with a strong indication, such as a mechanical heart valve or atrial fibrillation with a history of cardioembolic stroke, can be safely implemented after 10 days [85].
Intensive care unit management
Observation in an ICU or similar setting is strongly recommended for at least the first 24 hours after ictus (Class I, Level of Evidence B), since the risk of neurological deterioration is highest during this period [86] and because the majority of patients with brain stem or cerebellar hemorrhage have depressed levels of consciousness requiring ventilatory support [40] (Figure 3). Measurements in the ICU indicated for the optimal cardiovascular monitoring of ICH patients include invasive arterial blood pressure, central venous pressure, and, if required, pulmonary artery catheter monitoring. An external ventricular drain should be placed in patients with a depressed level of consciousness (GCS score ≤ 8), signs of acute hydrocephalus or intracranial mass effect on CT, and a prognosis that warrants aggressive ICU care [87].
Outcomes after ICH are better when patients are cared for in specialized ICUs. In a large administrative database, Diringer and colleagues [88] demonstrated that mortality after ICH was associated with lower GCS scores, higher age, and admission to a general medical-surgical, as opposed to specialty neurological, ICU. In this study a clear impact on outcomes was seen when patients were admitted and cared for by a specialized neurocritical care team. Similarly, in the study by Mirski and colleagues [89], mortality and disposition at discharge in ICH patients treated in a neuro-ICU compared to a similar cohort treated 2 years earlier in a general ICU setting. Although the exact reason why improved outcomes occur with treatment in a dedicated neuro-ICU remains unclear, much attention has focused recently on the major role that therapeutic nihilism and self-fulfilling prophesies of doom can have in determining outcome after ICH [90,91].
Patient positioning
To minimize ICP and reduce the risk of ventilator-associated pneumonia in mechanically ventilated patients, the head should be elevated 30 degrees (Class IIA, Level of Evidence B). In mechanically ventilated patients, further need for head elevation should be guided by changing of pulmonary and volume needs.
Fluids
Isotonic fluids such as 0.9% saline at a rate of approximately 1 ml/kg/h should be given as the standard intravenous replacement fluid for patients with ICH and optimized to achieve euvolemic balance and an hourly diuresis of >0.5 cc/kg (Class I, Level of Evidence B). Free water given in the form of 0.45% saline or 5% dextrose in water can exacerbate cerebral edema and increase ICP because it flows down its osmotic gradient into injured brain tissue (Class III, Level of Evidence C) [50]. Systemic hypo-osmolality (<280 mOsm/L) should be aggressively treated with mannitol or 3% hypertonic saline (Class IIA, Level of Evidence B). A state of euvolemia should be maintained by monitoring fluid balance and body weight, and by maintaining a normal central venous pressure (range 5 to 8 mmHg). Careful interpretation of the central venous pressure should be done when analyzing its value in the setting of positive end-expiratory pressure (PEEP).
The use of hypertonic saline in the form of a 2% or 3% sodium/chloride-acetate solution (1 ml/kg/h) has become an increasingly popular alternative to normal saline as a resuscitation fluid for patients with significant peri-hematomal edema and mass effect after ICH (Class IIA, Level of Evidence B). The goal is to establish and maintain a baseline state of hyper-osmolality (300 to 320 mOsms/L) and hypernatremia (150 to 155 mEq/L), which may reduce cellular swelling and the number of ICP crises. Potential complications of hypertonic saline use are fluid overload, pulmonary edema, hypokalemia, cardiac arrhythmias, hyperchloremic metabolic acidosis, and dilutional coagulopathy, [92]. Hypertonic saline should be gradually tapered and the serum sodium level should never be allowed to drop more than 12 mEq/L over 24 hours, to avoid rebound cerebral edema and increased ICP [92,93].
Prevention of seizures
Acute seizures should be treated with intravenous lorazepam (0.05 to 0.1 mg/kg) followed by a loading dose of phenytoin or fosphenytoin (20 mg/kg) (Class I, Level of Evidence B; Figure 3). An alternative to phenytoin infusion is levetiracetam (500 mg q12h, adjusted for renal insufficiency). Side effects of phenytin infusions include rash, hypotension, arrhythmias, and severe hypocalcemia for the phosphenytoin presentation. Patients with ICH may benefit from prophylactic anti-epileptic drug therapy, but no randomized trial has addressed the efficacy of this approach. The American Heart Association Guidelines have recommended anti-epileptic medication for up to one month, after which therapy should be discontinued in the absence of seizures [94]. This recommendation is supported by the results of a recent study that showed that the risk of early seizures was reduced by prophylactic anti-epileptic drug therapy [95]. The 30-day risk for convulsive seizures after ICH is approximately 8%, and the risk of overt status epilepticus is 1% to 2% [95]. Lobar location and small hematomas are independent predictors of early seizures [95]. The argument for prophylactic anticonvulsant therapy in stuporous or comatose ICH patients is bolstered by the fact that continuous electroencephalogram monitoring demonstrates electrographic seizure activity in approximately 25% of these patients, despite prophylactic anti-epileptic drug therapy [96,97]. The risk of late seizures or epilepsy among survivors of ICH is 5% to 27% [95].
Temperature control
Fever (temperature >38.3°C) after ICH is common, particularly with IVH [98], and should be treated aggressively (Figure 3; Class I, Level of Evidence C). Sustained fever after ICH has been shown to be independently associated with poor outcome after ICH [99]. A large body of experimental evidence indicates that even small degrees of hyperthermia can worsen ischemic brain injury by exacerbating excitotoxic neurotransmitter release, proteolysis, free radical and cyto-kine production, blood-brain barrier compromise, and apop-tosis [100,101]. Brain temperature elevations have also been associated with hyperemia, exacerbation of cerebral edema, and elevated intracranial pressure [102,103].
As a general standard, acetaminophen and cooling blankets are recommended for almost all patients with sustained fever in excess of 38.3°C (101.0°F), despite the lack of prospective randomized controlled trials supporting this approach [104,105]. Acetaminophen should be used with caution in patients with hepatic dysfunction. Newer adhesive surface cooling systems and endovascular heat exchange catheters have been shown to be much more effective for maintaining normothermia [106,107]; however, it remains to be seen if these measures can improve clinical outcome.
Management of hyperglycemia
Admission hyperglycemia is a potent predictor of 30-day mortality in both diabetic and non-diabetic patients with ICH [108]. The detrimental effect of hyperglycemia has been well studied in acute vascular syndromes. In ischemic stroke, hyperglycemia occurs in 20% to 40% of patients and is associated with infarct expansion, worse functional outcome, longer hospital stays, higher medical costs, and an increased risk of death [109-111] and it is felt to be secondary to a catecholamine surge and generalized stress response [110].
In the critically ill population, hyperglycemia seems much more acutely toxic than in healthy individuals, for whom cells can protect themselves by down-regulation of glucose transporters [112]. The acute toxicity of high levels of glucose in critical illness might be explained by an accelerated cellular glucose overload and more pronounced toxic side effects of glycolysis and oxidative phosphorylation [113]. Neurons and several other cell types are insulin independent for glucose uptake, which is mediated by transporters such as GLUT-1, GLUT-2, and GLUT-3 [114]. These transporters are up-regulated by hypoxia and inflammatory mediators such as angio-tensin-II, endothelin-1, vascular endothelial growth factor, and transforming growth factor-β among others. These transporters facilitate glucose entry into the neuron where intra-cellular hyperglycemia can lead to oxidative stress and exaggerated production of superoxide species [114]. Peroxy-nitrite, superoxide, and other reactive oxygen species lead to inhibition of the glycolytic enzyme glyceraldhyde phosphate dehydrogenase and mitochondrial complexes I and IV, the basis of mitochondrial dysfunction likely to induce end-organ failure and cellular death [114].
Strict glucose control after ICH is recommended (Class IIA, Level of Evidence C). This approach has been linked to reductions in intracranial pressure, duration of mechanical ventilation, and seizures in an heterogeneous cohort of critically ill patients [115].
Elevated intracranial pressure management
Large volume ICH carries the risk of developing cerebral edema and high ICP (≥ 15 mmHg or 20 ≥ mmH2O), and the presence of IVH further increases the risk of mortality [116,117] (Figure 3). This effect is primarily related to the development of obstructive hydrocephalus and alterations of normal cerebrospinal fluid flow-dynamics. Patients with large volume ICH, intracranial mass effect, and coma may benefit from ICP monitoring, though this intervention has not been proved to benefit outcomes after ICH [118,119]. We recommend a stepwise protocol for addressing intracranial hypertension in the ICU setting.
Cerebrospinal fluid drainage
Initial cerebrospinal fluid drainage may be a life-saving procedure particularly in the setting of hydrocephalus and IVH [67] (Class IIA, Level of Evidence B). This technique allows for rapid clearance of cerebrospinal fluid, release of ICP, and ICP/CPP monitoring. As a general rule, an ICP monitor or external ventricular drain (EVD) should be placed in all comatose ICH patients (GCS score of 8 or less) with the goal of maintaining ICP less than 20 mmH2O (<15 mmHg) and CPP at greater than 70 mmHg, unless their condition is so dismal that aggressive ICU care is not warranted. Compared to parenchymal monitors, EVDs carry the therapeutic advantage of allowing cerebrospinal fluid drainage, and the disadvantage of a substantial risk of infection (approximately 10% during the first 10 days) [120]. A small retrospective study failed to show any relationship between changes in ventricular size and level of consciousness in ICH patients treated with EVDs [121].
Sedation
Sedation should be used to minimize pain, agitation, and decrease surges in ICP (Class IIA, Level of Evidence B). Agitation must be avoided, because it can aggravate ICP elevation through straining (increasing thoracic, jugular venous, and systemic BP), increased cerebral metabolic rate of oxygen, and also may cause uncontrolled hyper-/hypo-ventilation, which both can be detrimental. During an ICP spike, sedation may be all that is necessary to control the ICP. The goal of sedation should be a calm, comfortable, and cooperative state in patients with ICP that is well-controlled, and a quiet, motionless state in patients where ICP elevation requires active management. The preferred regimen is the combination of a short-acting opioid, such as fentanyl (1 to 3 μg/kg/h) or remifentanyl (0.03 to 0.25 μg/kg/minute), to provide analgesia, and propofol (0.3 to 3 mg/kg/h) because of its extremely short half-life, which makes it ideal for periodic interruption for neurological assessments, which should be performed on a daily basis unless the patient has demonstrated that the ICP is too unstable (frequent ICP crisis in the setting of awakening, position changes, fever, and so on) to tolerate this. Bolus injections of opioids should be used with caution in patients with elevated ICP because they can transiently lower MAP and increase ICP due to autoregulatory vasodilation of cerebral vessels [122]. Compared to an opiod-based sedation regimen, in one trial propofol was associated with lower ICP and fewer ICP interventions in patients with severe traumatic brain injury [123]. However, propofol has been associated with mithocondrial dysfunction and multi-organ failure (propofol infusion syndrome). Predisposing factors include young age, severe critical illness of central nervous system or respiratory origin, exogenous catecholamine or glucocorticoid administration, inadequate carbohydrate intake and subclinical mitochondrial disease [124].
Cerebral perfusion pressure optimization
Two prevailing management strategies for the management of elevated ICP have evolved from the experience in traumatic brain injury. The 'Lund concept' assumes a disruption of the blood brain barrier and recommends manipulations to decrease the hydrostatic BP and increase osmotic pressures to minimize cerebral blood volume and vasogenic edema by improving perfusion and oxygenation to the injured areas of the brain [125]. This is achieved in theory by maintaining an euvolemic state with normal hemoglobin, hematocrit, plasma protein concentrations, and by antagonizing vasoconstriction through reduction of catecholamine concentration in plasma and sympathetic outflow. These therapeutic measures attempt to normalize all essential hemodynamic parameters (blood pressure, plasma oncotic pressure, plasma and erythrocyte volumes, arterial partial pressure of oxygen (PaO2), and arterial partial pressure of carbon dioxide (PaCO2)). The introduction of microdialysis with novel physiological targets may optimize the goals of the original Lund protocol. The 'Rosner concept' emphasizes maintaining a high CPP to minimize reflex vasodilatation or ischemia [126,127] at the expense of added cardiopulmonary stress (Class IIA, Level of Evidence B). Computerized bedside graphical displays (ICU Pilot®, CMA Micodialysis, Solna, Sweden) can allow clinicians to identify whether ICP and MAP are positively correlated, in which case a low CPP would be preferable, or negatively correlated, in which case a higher CPP would be desirable.
Hyperosmolar therapy
Hyperosmolar therapy [128] should be used after sedation and CPP optimization fail to normalize ICP (Class IIA, Level of Evidence B). The initial dose of mannitol is 1 to 1.5 g/kg of a 20% solution, followed by bolus doses of 0.25 to 1.0 g/kg as needed to a target osmolality of 300 to 320 mOsm/kg. Additional doses can be given as frequently as once an hour, based on the initial response to therapy with the anticipation of a transient drop in BP. There is little to recommend the use of standing mannitol in patients with normal ICP. In a recent trial of mannitol for ICH, 128 patients were randomized to receive low-dose mannitol (100 ml of 20% solution) or sham therapy every 4 hours for 5 days with a rapid dose tapering schedule over 48 hours. The 1-month mortality rate was 25% in both groups and disability scores at 3 months were not significantly different between groups [129]. Hypertonic saline, such as 23.4% saline solution, can be used as an alternative to mannitol, particularly when CPP augmentation is desirable (Class IIA, Level of Evidence B). However, care should be taken to avoid fluid overload in the setting of heart or kidney failure. Additional side effects of hyperosmolar therapy include kidney failure, rebound ICP, electrolytic imbalance (hypo-/hyper-natremia), and acid/base disturbances. Despite clinical and animal model support [64], many issues remain to be clarified, including the exact mechanism of action, best mode and timing of administration, and the most appropriate concentration.
Hyperventilation
Forced hyperventilation is generally used sparingly in the ICU and, for brief periods, in monitored patients, because its effect on ICP tends to last for only a few hours (Class IIA, Level of Evidence B). Good long term outcomes can occur when the combination of osmotherapy and hyperventilation is successfully used to reverse transtentorial herniation [130]. Overly aggressive hyperventilation to pCO2 levels <25 mmHg may cause excessive vasoconstriction and exacerbation of ischemia during the acute phase of ICH and should be avoided. Controlled hyperventilation therapy can be optimized by saturation of jugular vein oxygen and partial brain tissue oxygenation monitoring.
Barbiturates
For cases of severe and intractable intracranial hypertension, barbiturates can control ICP by decreasing cerebral metabolic activity, which translates into a reduction of the CBF and cerebral blood volume (Class IIB, level of Evidence B). Pentobarbital can be given in repeated 5 mg/kg boluses every 15 to 30 minutes until ICP is controlled (usually 10 to 20 mg/kg is required), and then continuously infused at 1 to 4 mg/kg/h. An electroencephalogram should be continuously recorded, and the pentobarbital titrated to produce a burst-suppression pattern, with approximately 6 to 8 second interbursts, to avoid excessive sedation.
Hypothermia
If pentobarbital fails to control ICP, induced hypothermia to 32 to 34°C can effectively lower otherwise refractory ICP (Class IIB, Level of Evidence C) [131]. Hypothermia can be achieved using various surface and endovascular cooling systems coupled to a rectal, esophageal, pulmonary artery, or bladder thermometer. Complications of hypothermia include nosocomial infection, hypotension, cardiac arrhythmias, coagulopathy, shivering, hyperkalemia, hyperglycemia, and ileus. Because these risks increase with the depth and duration of cooling, some advocate for the induction of mild hypothermia (34 to 36°C) if temperature reduction is required for a prolonged period of time to control ICP [104,132,133].
Intraventricular thrombolytic therapy
IVH commonly results from extension of ICH into the cerebral ventricular system, and is an independent predictor of mortality after ICH [134]. Commonly, hydrocephalus and IVH are managed with an EVD, but outcomes remain poor [9]. Intraventricular administration of the plasminogen activator urokinase every 12 hours may reduce hematoma size and the expected mortality rate at 1 month [135]. Several small studies have reported the successful use of urokinase or tissue plasminogen activator (t-PA) for the treatment of IVH, with the goal of accelerating the clearance of IVH and improving clinical outcome [136]. A Cochrane systematic review published in 2002 summarized the experience of several case series providing evidence of safety but no definitive efficacy [137]. No randomized prospective controlled trial has addressed the efficacy of intraventricular thrombolysis after ICH. The ongoing Clear IVH Trial (Clot Lysis Evaluating Accelerated Resoution of Intra Ventricular Hemorrhage), a phase II multicenter study evaluating recombinant t-PA treatment of patients with IVH, is designed to investigate the optimum dose and frequency of recombinant t-PA administered via an intraventricular catheter to safely and effectively treat IVH and will soon provide some insight into this issue [138]. When used off-label, a dose of 1 mg of t-PA every 8 hours (followed by clamping of the EVD for 1 hour) is reasonable until clearance of blood from the third ventricle has been achieved [139]. Doses of 3 mg or more of t-PA for IVH thrombolysis have been associated with an unacceptably high bleeding rate (Daniel Hanley, MD, personal communication).
Deep venous thrombosis prophylaxis
Patients with ICH are at high risk for deep vein thrombosis and pulmonary embolism, a potentially fatal complication, due to limb paresis and prolonged immobilization. Dynamic compression stockings should be placed on admission [140] (Class I, Level of Evidence B). A small prospective trial has shown that low dose subcutaneous heparin (5000 U BID) starting after the second day significantly reduces the frequency of venous thromboembolism, with no increase in intracranial bleeding (Class IIB, Level of Evidence B) [141]. Treatment with low molecular weight heparin (enoxaparin 40 mg daily) is a reasonable alternative if renal function is normal (Class IIB, Level of Evidence C).
Nutrition
As is the case with all critically ill neurological patients, enteral feeding should be started within 48 hours to avoid protein catabolism and malnutrition. A small-bore nasoduo-denal feeding tube may reduce the risk of aspiration events.
Surgical intervention for intracerebral hemorrhage
Craniotomy has been the most studied intervention for the surgical management of ICH but the results have been discouraging. Two earlier smaller trials showed that for patients presenting with moderate alterations in the state of consciousness, surgery reduced the risk of death without improving the functional outcome [142] and that ultra-early evacuation might improve the 3-month NIHSS [143]. Nevertheless, in a meta-analysis of all prior trials of surgical intervention for supratentorial ICH, no benefit was demonstrated [144].
The International Surgical Trial in Intracerebral Haemorrhage (STICH) study, a landmark trial of over 1,000 ICH patients, showed that emergent surgical hematoma evacuation via craniotomy within 72 hours of onset fails to improve outcome compared to a policy of initial medical management [145]. Although the STICH has rightfully dampened the enthusiasm of neurosurgeons for performing surgery, it must be remembered that the trial was based on the principle of clinical equipoise and patients who the local investigator felt would most likely benefit from emergency surgery were not enrolled into the study. In a post hoc analysis of the STICH, the subgroup of patients with superficial hematomas and no IVH had better outcomes in the surgical arm [146]. This observation provided support for the STICH-II, which is currently enrolling patients [147]. In contrast to supratentorial ICH, there is much better evidence that cerebellar hemorrhages exceeding 3 cm in diameter benefit from emergent surgical evacuation as abrupt and dramatic deterioration to coma can occur within the first 24 hours of onset in these patients (Class I, Level of evidence B) [148]. For this reason, it is generally unwise to defer surgery in these patients until further clinical deterioration occurs.
As emergent craniotomy has been unable to improve neurological outcome after ICH, the role of other surgical techniques such as minimally invasive surgery have gained importance over the past decade. The advantages of minimally invasive surgery over conventional craniotomy include reduced operative time, the possibility of performance under local anesthesia, and reduced surgical trauma. Endoscopic aspiration of supratentorial ICH was studied in a small single-center randomized controlled trial (Class IIB, Level of Evidence B) [149]. The study showed that this technique provided a reduction of mortality rate at 6 months in the surgical group but surgery was more effective in superficial hematomas and in younger patients (<60 years).
Thrombolytic therapy and surgical removal of hematomas is another technique that has been studied in a single center randomized clinical trial (Class IIB, Level of Evidence B) [143]. Patients in the surgical group had better outcome scores than the medically treated group. Finally, a multi-center randomized control trial examined the utility of sterotactic urokinase infusion when administered within 72 hours to patients with GCS score ≥ 5 and hematomas ≥ 10 ml [150]; this provided significant reduction in hematoma size and mortality rate at the expense of higher rates of re-bleeding but no significant differences in outcomes measures was seen.
Hemicraniectomy with duraplasty has been proposed as a life-saving intervention for several neurological catastrophes, such as malignant middle cerebral artery infarction and poor grade subarachnoid hemorrhage. No randomized controlled trial has been conducted in patients with ICH. In a recent report of 12 consecutive patients with hypertensive ICH and treated with hemicraniectomy, 11 (92%) survived at discharge and 6 of them (54.5%) had a good functional outcome (modified Rankin Score 0 to 3) [151]. These preliminary data support the need for better controlled studies addressing the role of this surgical technique in ICH patients (Class IIB, Level of Evidence B).
Conclusion
Despite a long history of devastating outcomes and high mortality, there is optimism that the management of ICH will change in the future based on new insights into the acute pathophysiology of this disease. A better understanding of the dynamic process of hematoma growth, importance of inflammation triggered by coagulation and products of blood degradation, and the deleterious effects of fever and hyperglycemia may provide feasible targets for future interventions. A recent setback in the form of a negative phase III trial evaluating ultra-early hemostatic therapy with rFVIIa for acute ICH has led researchers to investigate CT angiography as a method for identifying patients with contrast extravasation and an increased risk of active bleeding. Other promising approaches that deserve further study include thrombolytic therapy for IVH [138], minimally invasive surgery for clot lysis [152], and the development of novel anti-inflammatory agents that target coagulation-induced peri-hematomal brain injury, such as thrombin, hemoglobin, matrix metalloproteinases, and vascular endothelial growth factor [153]. These advances will hopefully lead to new optimism for what has historically been one of the most devastating illnesses in clinical medicine, and establish ICH as a medically treatable condition worthy of aggressive ICU support.
Note
This article is part of a review series on Stroke, edited by David Menon.
Other articles in the series can be found online at http://ccforum.com/series/CC_Stroke
Abbreviations
BP: blood pressure; CBF: cerebral blood flow; CPP: cerebral perfusion pressure; CT: computed tomography; EVD: external ventricular drain; FFP: fresh frozen plasma; GCS: Glasgow Coma Scale; ICH: intracerebral hemorrhage; ICP: intracranial pressure; ICU: intensive care unit; INR: international normalized ratio; IVH: intraventricular hemorrhage; MAP: mean arterial pressure; MRI: magnetic resonance imaging; NIHSS: National Institute of Health Stroke Scale; rFVIIa: recombinant factor VII; RSI: rapid sequence intubation; t-PA: tissue plasminogen activator.
Competing interests
SAM has received research grant support, unrestricted educational grants, consulting fees, and speaking honoraria from Novo Nordisk A/S; and unrestricted educational grants, consulting fees, speaking honoraria from PDL BioPharma and EKR therapeutics. FR has no potential conflicts of interest to report.
References
- Sacco RL, Mayer SA. Epidemiology of intracerebral hemorrhage. In: Feldmann E, editor. Intracerebral Hemorrhage. Armonk, NY: Futura Publishing Co; 1994. pp. 3–23. [Google Scholar]
- Broderick J, Connolly S, Feldmann E, Hanley D, Kase C, Krieger D, Mayberg M, Morgenstern L, Ogilvy CS, Vespa P, Zuccarello M, American Heart Association; American Stroke Association Stroke Council; High Blood Pressure Research Council; Quality of Care and Outcomes in Research Interdisciplinary Working Group Guidelines for the management of spontaneous intracerebral hemorrhage in adults: 2007 update: a guideline from the American Heart Association/American Stroke Association Stroke Council, High Blood Pressure Research Council, and the Quality of Care and Outcomes in Research Interdisciplinary Working Group. Stroke. 2007;38:2001–2023. doi: 10.1161/STROKEAHA.107.183689. [DOI] [PubMed] [Google Scholar]
- Gebel JM, Broderick JP. Intracerebral hemorrhage. Neurol Clin. 2000;18:419–438. doi: 10.1016/s0733-8619(05)70200-0. [DOI] [PubMed] [Google Scholar]
- Holloway RG, Witter DM, Jr, Lawton KB, Lipscomb J, Samsa G. Inpatient costs of specific cerebrovascular events at five academic medical centers. Neurology. 1996;46:854–860. [PubMed] [Google Scholar]
- Taylor TN, Davis PH, Torner JC, Holmes J, Meyer JW, Jacobson MF. Lifetime cost of stroke in the United States. Stroke. 1996;27:1459–1466. doi: 10.1161/01.str.27.9.1459. [DOI] [PubMed] [Google Scholar]
- Qureshi AI, Tuhrim S, Broderick JP, Batjer HH, Hondo H, Hanley DF. Spontaneous intracerebral hemorrhage. N Engl J Med. 2001;344:1450–1460. doi: 10.1056/NEJM200105103441907. [DOI] [PubMed] [Google Scholar]
- Skidmore CT, Andrefsky J. Spontaneous intracerebral hemorrhage: epidemiology, pathophysiology, and medical management. Neurosurg Clin N Am. 2002;13:281–288. doi: 10.1016/s1042-3680(02)00019-0. v. [DOI] [PubMed] [Google Scholar]
- Siddique MS, Gregson BA, Fernandes HM, Barnes J, Treadwell L, Wooldridge TD, Mendelow AD. Comparative study of traumatic and spontaneous intracerebral hemorrhage. J Neurosurg. 2002;96:86–89. doi: 10.3171/jns.2002.96.1.0086. [DOI] [PubMed] [Google Scholar]
- Mayer SA, Rincon F. Treatment of intracerebral haemorrhage. Lancet Neurol. 2005;4:662–672. doi: 10.1016/S1474-4422(05)70195-2. [DOI] [PubMed] [Google Scholar]
- Measuring and improving quality of care: a report from the American Heart Association/American College of Cardiology First Scientific Forum on Assessment of Healthcare Quality in Cardiovascular Disease and Stroke. Circulation. 2000;101:1483–1493. doi: 10.1161/01.cir.101.12.1483. [DOI] [PubMed] [Google Scholar]
- Brott T, Thalinger K, Hertzberg V. Hypertension as a risk factor for spontaneous intracerebral hemorrhage. Stroke. 1986;17:1078–1083. doi: 10.1161/01.str.17.6.1078. [DOI] [PubMed] [Google Scholar]
- Thrift AG, McNeil JJ, Forbes A, Donnan GA. Three important subgroups of hypertensive persons at greater risk of intracerebral hemorrhage. Melbourne Risk Factor Study Group. Hypertension. 1998;31:1223–1229. doi: 10.1161/01.hyp.31.6.1223. [DOI] [PubMed] [Google Scholar]
- Fisher C. Pathological observations in hypertensive intracerebral hemorrhage. J Neuropathol Exp Neurol. 1971;30:536–550. doi: 10.1097/00005072-197107000-00015. [DOI] [PubMed] [Google Scholar]
- Kase CS, Williams JP, Wyatt DA, Mohr JP. Lobar intracerebral hematomas: clinical and CT analysis of 22 cases. Neurology. 1982;32:1146–1150. doi: 10.1212/wnl.32.10.1146. [DOI] [PubMed] [Google Scholar]
- Segal AZ, Chiu RI, Eggleston-Sexton PM, Beiser A, Greenberg SM. Low cholesterol as a risk factor for primary intracerebral hemorrhage: A case-control study. Neuroepidemiology. 1999;18:185–193. doi: 10.1159/000026210. [DOI] [PubMed] [Google Scholar]
- Iso H, Jacobs DR, Jr, Wentworth D, Neaton JD, Cohen JD. Serum cholesterol levels and six-year mortality from stroke in 350,977 men screened for the multiple risk factor intervention trial. N Engl J Med. 1989;320:904–910. doi: 10.1056/NEJM198904063201405. [DOI] [PubMed] [Google Scholar]
- Yano K, Reed DM, MacLean CJ. Serum cholesterol and hemorrhagic stroke in the Honolulu Heart Program. Stroke. 1989;20:1460–1465. doi: 10.1161/01.str.20.11.1460. [DOI] [PubMed] [Google Scholar]
- Iribarren C, Jacobs DR, Sadler M, Claxton AJ, Sidney S. Low total serum cholesterol and intracerebral hemorrhagic stroke: is the association confined to elderly men? The Kaiser Permanente Medical Care Program. Stroke. 1996;27:1993–1998. doi: 10.1161/01.str.27.11.1993. [DOI] [PubMed] [Google Scholar]
- Plehn JF, Davis BR, Sacks FM, Rouleau JL, Pfeffer MA, Bernstein V, Cuddy TE, Moyé LA, Piller LB, Rutherford J, Simpson LM, Braunwald E. Reduction of stroke incidence after myocardial infarction with pravastatin: the Cholesterol and Recurrent Events (CARE) study. The Care Investigators. Circulation. 1999;99:216–223. doi: 10.1161/01.cir.99.2.216. [DOI] [PubMed] [Google Scholar]
- Amarenco P, Bogousslavsky J, Callahan A, 3rd, Goldstein LB, Hennerici M, Rudolph AE, Sillesen H, Simunovic L, Szarek M, Welch KM, Zivin JA, Stroke Prevention by Aggressive Reduction in Cholesterol Levels (SPARCL) Investigators High-dose ator-vastatin after stroke or transient ischemic attack. N Engl J Med. 2006;355:549–559. doi: 10.1056/NEJMoa061894. [DOI] [PubMed] [Google Scholar]
- Gill JS, Shipley MJ, Tsementzis SA, Hornby RS, Gill SK, Hitchcock ER, Beevers DG. Alcohol consumption – a risk factor for hemorrhagic and non-hemorrhagic stroke. Am J Med. 1991;90:489–497. [PubMed] [Google Scholar]
- Gill JS, Zezulka AV, Shipley MJ, Gill SK, Beevers DG. Stroke and alcohol consumption. N Engl J Med. 1986;315:1041–1046. doi: 10.1056/NEJM198610233151701. [DOI] [PubMed] [Google Scholar]
- Gorelick PB. Alcohol and stroke. Stroke. 1987;18:268–271. doi: 10.1161/01.str.18.1.268. [DOI] [PubMed] [Google Scholar]
- Klatsky AL, Armstrong MA, Friedman GD. Alcohol use and subsequent cerebrovascular disease hospitalizations. Stroke. 1989;20:741–746. doi: 10.1161/01.str.20.6.741. [DOI] [PubMed] [Google Scholar]
- Thrift AG, Donnan GA, McNeil JJ. Heavy drinking, but not moderate or intermediate drinking, increases the risk of intracerebral hemorrhage. Epidemiology. 1999;10:307–312. [PubMed] [Google Scholar]
- Levine SR, Brust JC, Futrell N, Ho KL, Blake D, Millikan CH, Brass LM, Fayad P, Schultz LR, Selwa JF, et al. Cerebrovascular complications of the use of the "crack" form of alkaloidal cocaine. N Engl J Med. 1990;323:699–704. doi: 10.1056/NEJM199009133231102. [DOI] [PubMed] [Google Scholar]
- Ariesen MJ, Claus SP, Rinkel GJ, Algra A. Risk factors for intracerebral hemorrhage in the general population: a systematic review. Stroke. 2003;34:2060–2065. doi: 10.1161/01.STR.0000080678.09344.8D. [DOI] [PubMed] [Google Scholar]
- Qureshi AI, Mohammad Y, Suri MF, Braimah J, Janardhan V, Guterman LR, Hopkins LN, Frankel MR. Cocaine use and hypertension are major risk factors for intracerebral hemorrhage in young African Americans. Ethn Dis. 2001;11:311–319. [PubMed] [Google Scholar]
- Arboix A, Vall-Llosera A, Garcia-Eroles L, Massons J, Oliveres M, Targa C. Clinical features and functional outcome of intracerebral hemorrhage in patients aged 85 and older. J Am Geriatr Soc. 2002;50:449–454. doi: 10.1046/j.1532-5415.2002.50109.x. [DOI] [PubMed] [Google Scholar]
- Daverat P, Castel JP, Dartigues JF, Orgogozo JM. Death and functional outcome after spontaneous intracerebral hemorrhage. A prospective study of 166 cases using multivariate analysis. Stroke. 1991;22:1–6. doi: 10.1161/01.str.22.1.1. [DOI] [PubMed] [Google Scholar]
- Broderick JP, Brott T, Tomsick T, Miller R, Huster G. Intracerebral hemorrhage more than twice as common as subarachnoid hemorrhage. J Neurosurg. 1993;78:188–191. doi: 10.3171/jns.1993.78.2.0188. [DOI] [PubMed] [Google Scholar]
- Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, Khoury J. The ABCs of measuring intracerebral hemorrhage volumes. Stroke. 1996;27:1304–1305. doi: 10.1161/01.str.27.8.1304. [DOI] [PubMed] [Google Scholar]
- Newman GC. Clarification of abc/2 rule for ICH volume. Stroke. 2007;38:862. doi: 10.1161/01.STR.0000257309.50643.0a. [DOI] [PubMed] [Google Scholar]
- Becker KJ, Baxter AB, Bybee HM, Tirschwell DL, Abouelsaad T, Cohen WA. Extravasation of radiographic contrast is an independent predictor of death in primary intracerebral hemorrhage. Stroke. 1999;30:2025–2032. doi: 10.1161/01.str.30.10.2025. [DOI] [PubMed] [Google Scholar]
- Goldstein JN, Fazen LE, Snider R, Schwab K, Greenberg SM, Smith EE, Lev MH, Rosand J. Contrast extravasation on CT angiography predicts hematoma expansion in intracerebral hemorrhage. Neurology. 2007;68:889–894. doi: 10.1212/01.wnl.0000257087.22852.21. [DOI] [PubMed] [Google Scholar]
- Wada R, Aviv RI, Fox AJ, Sahlas DJ, Gladstone DJ, Tomlinson G, Symons SP. CT angiography "spot sign" predicts hematoma expansion in acute intracerebral hemorrhage. Stroke. 2007;38:1257–1262. doi: 10.1161/01.STR.0000259633.59404.f3. [DOI] [PubMed] [Google Scholar]
- Kidwell CS, Chalela JA, Saver JL, Starkman S, Hill MD, Demchuk AM, Butman JA, Patronas N, Alger JR, Latour LL, Luby ML, Baird AE, Leary MC, Tremwel M, Ovbiagele B, Fredieu A, Suzuki S, Villablanca JP, Davis S, Dunn B, Todd JW, Ezzeddine MA, Haymore J, Lynch JK, Davis L, Warach S. Comparison of MRI and CT for detection of acute intracerebral hemorrhage. JAMA. 2004;292:1823–1830. doi: 10.1001/jama.292.15.1823. [DOI] [PubMed] [Google Scholar]
- Zhu XL, Chan MS, Poon WS. Spontaneous intracranial hemorrhage: which patients need diagnostic cerebral angiography? A prospective study of 206 cases and review of the literature. Stroke. 1997;28:1406–1409. doi: 10.1161/01.str.28.7.1406. [DOI] [PubMed] [Google Scholar]
- Halpin SF, Britton JA, Byrne JV, Clifton A, Hart G, Moore A. Prospective evaluation of cerebral angiography and computed tomography in cerebral haematoma. J Neurol Neurosurg Psychiatry. 1994;57:1180–1186. doi: 10.1136/jnnp.57.10.1180. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Gujjar AR, Deibert E, Manno EM, Duff S, Diringer MN. Mechanical ventilation for ischemic stroke and intracerebral hemorrhage: indications, timing, and outcome. Neurology. 1998;51:447–451. doi: 10.1212/wnl.51.2.447. [DOI] [PubMed] [Google Scholar]
- Diringer MN. Intracerebral hemorrhage: pathophysiology and management. Crit Care Med. 1993;21:152–157. doi: 10.1097/00003246-199310000-00032. [DOI] [PubMed] [Google Scholar]
- Reynolds SF, Heffner J. Airway management of the critically ill patient: rapid-sequence intubation. Chest. 2005;127:1397–1412. doi: 10.1378/chest.127.4.1397. [DOI] [PubMed] [Google Scholar]
- Fellows IW, Bastow MD, Byrne AJ, Allison SP. Adrenocortical suppression in multiply injured patients: a complication of etomidate treatment. Br Med J (Clin Res Ed) 1983;287:1835–1837. doi: 10.1136/bmj.287.6408.1835. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Papazian L, Albanese J, Thirion X, Perrin G, Durbec O, Martin C. Effect of bolus doses of midazolam on intracranial pressure and cerebral perfusion pressure in patients with severe head injury. Br J Anaesth. 1993;71:267–271. doi: 10.1093/bja/71.2.267. [DOI] [PubMed] [Google Scholar]
- Orebaugh SL. Succinylcholine: adverse effects and alternatives in emergency medicine. Am J Emerg Med. 1999;17:715–721. doi: 10.1016/s0735-6757(99)90168-7. [DOI] [PubMed] [Google Scholar]
- Booij LH. Is succinylcholine appropriate or obsolete in the intensive care unit? Crit Care. 2001;5:245–246. doi: 10.1186/cc1039. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schramm WM, Jesenko R, Bartunek A, Gilly H. Effects of cisatracurium on cerebral and cardiovascular hemodynamics in patients with severe brain injury. Acta Anaesthesiol Scand. 1997;41:1319–1323. doi: 10.1111/j.1399-6576.1997.tb04651.x. [DOI] [PubMed] [Google Scholar]
- Schramm WM, Strasser K, Bartunek A, Gilly H, Spiss CK. Effects of rocuronium and vecuronium on intracranial pressure, mean arterial pressure and heart rate in neurosurgical patients. Br J Anaesth. 1996;77:607–611. doi: 10.1093/bja/77.5.607. [DOI] [PubMed] [Google Scholar]
- Robinson N, Clancy M. In patients with head injury undergoing rapid sequence intubation, does pretreatment with intravenous lignocaine/lidocaine lead to an improved neurological outcome? A review of the literature. Emerg Med J. 2001;18:453–457. doi: 10.1136/emj.18.6.453. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Passero S, Ciacci G, Ulivelli M. The influence of diabetes and hyperglycemia on clinical course after intracerebral hemorrhage. Neurology. 2003;61:1351–1356. doi: 10.1212/01.wnl.0000094326.30791.2d. [DOI] [PubMed] [Google Scholar]
- Siddique MS, Fernandes HM, Wooldridge TD, Fenwick JD, Slomka P, Mendelow AD. Reversible ischemia around intracerebral hemorrhage: a single-photon emission computerized tomography study. J Neurosurg. 2002;96:736–741. doi: 10.3171/jns.2002.96.4.0736. [DOI] [PubMed] [Google Scholar]
- Rosand J, Eskey C, Chang Y, Gonzalez RG, Greenberg SM, Koroshetz WJ. Dynamic single-section CT demonstrates reduced cerebral blood flow in acute intracerebral hemorrhage. Cerebrovasc Dis. 2002;14:214–220. doi: 10.1159/000065681. [DOI] [PubMed] [Google Scholar]
- Brott T, Broderick J, Kothari R, Barsan W, Tomsick T, Sauerbeck L, Spilker J, Duldner J, Khoury J. Early hemorrhage growth in patients with intracerebral hemorrhage. Stroke. 1997;28:1–5. doi: 10.1161/01.str.28.1.1. [DOI] [PubMed] [Google Scholar]
- Broderick JP, Diringer MN, Hill MD, Brun NC, Mayer SA, Steiner T, Skolnick BE, Davis SM. Determinants of intracerebral hemorrhage growth: an exploratory analysis. Stroke. 2007;38:1072–1075. doi: 10.1161/01.STR.0000258078.35316.30. [DOI] [PubMed] [Google Scholar]
- Powers WJ, Zazulia AR, Videen TO, Adams RE, Yundt KD, Aiyagari V, Grubb RL, Jr, Diringer MN. Autoregulation of cerebral blood flow surrounding acute (6 to 22 hours) intracerebral hemorrhage. Neurology. 2001;57:18–24. doi: 10.1212/wnl.57.1.18. [DOI] [PubMed] [Google Scholar]
- Powers WJ, Adams RE, Yundt KD. Acute pharmacological hypotension after intracerebral hemorrhage does not change cerebral blood flow. Stroke. 1999;30:242. [Google Scholar]
- Qureshi AI, Wilson DA, Hanley DF, Traystman RJ. Pharmacologic reduction of mean arterial pressure does not adversely affect regional cerebral blood flow and intracranial pressure in experimental intracerebral hemorrhage. Crit Care Med. 1999;27:965–971. doi: 10.1097/00003246-199905000-00036. [DOI] [PubMed] [Google Scholar]
- Rose JC, Mayer SA. Optimizing blood pressure in neurological emergencies. Neurocritical Care. 2004;1:287–299. doi: 10.1385/NCC:1:3:287. [DOI] [PubMed] [Google Scholar]
- Kuwata N, Kuroda K, Funayama M, Sato N, Kubo N, Ogawa A. Dysautoregulation in patients with hypertensive intracerebral hemorrhage. A SPECT study. Neurosurg Rev. 1995;18:237–245. doi: 10.1007/BF00383874. [DOI] [PubMed] [Google Scholar]
- Mayer SA, Lignelli A, Fink ME, Kessler DB, Thomas CE, Swarup R, Van Heertum RL. Perilesional blood flow and edema formation in acute intracerebral hemorrhage: a SPECT study. Stroke. 1998;29:1791–1798. doi: 10.1161/01.str.29.9.1791. [DOI] [PubMed] [Google Scholar]
- Lang EW, Lagopoulos J, Griffith J, Yip K, Mudaliar Y, Mehdorn HM, Dorsch NW. Noninvasive cerebrovascular autoregulation assessment in traumatic brain injury: validation and utility. J Neurotrauma. 2003;20:69–75. doi: 10.1089/08977150360517191. [DOI] [PubMed] [Google Scholar]
- Antihypertensive Treatment in Acute Cerebral Hemorrhage http://www.strokecenter.org/trials/TrialDetail.aspx?tid=602
- Intensive Blood Pressure Reduction in Acute Cerebral Haemorrhage http://www.clinicaltrials.gov/ct/show/NCT00226096?order=1
- Qureshi AI, Wilson DA, Traystman RJ. Treatment of transtentorial herniation unresponsive to hyperventilation using hypertonic saline in dogs: effect on cerebral blood flow and metabolism. J Neurosurg Anesthesiol. 2002;14:22–30. doi: 10.1097/00008506-200201000-00005. [DOI] [PubMed] [Google Scholar]
- Poungvarin N, Bhoopat W, Viriyavejakul A, Rodprasert P, Buranasiri P, Sukondhabhant S, Hensley MJ, Strom BL. Effects of dexamethasone in primary supratentorial intracerebral hemorrhage. N Engl J Med. 1987;316:1229–1233. doi: 10.1056/NEJM198705143162001. [DOI] [PubMed] [Google Scholar]
- Tellez H, Bauer RB. Dexamethasone as treatment in cerebrovascular disease. 1. A controlled study in intracerebral hemorrhage. Stroke. 1973;4:541–546. doi: 10.1161/01.str.4.4.541. [DOI] [PubMed] [Google Scholar]
- Liliang PC, Liang CL, Lu CH, Chang HW, Cheng CH, Lee TC, Chen HJ. Hypertensive caudate hemorrhage prognostic predictor, outcome, and role of external ventricular drainage. Stroke. 2001;32:1195–1200. doi: 10.1161/01.str.32.5.1195. [DOI] [PubMed] [Google Scholar]
- Fujii Y, Takeuchi S, Sasaki O, Minakawa T, Tanaka R. Multivariate analysis of predictors of hematoma enlargement in spontaneous intracerebral hemorrhage. Stroke. 1998;29:1160–1166. doi: 10.1161/01.str.29.6.1160. [DOI] [PubMed] [Google Scholar]
- Fujii Y, Tanaka R, Takeuchi S, Koike T, Minakawa T, Sasaki O. Hematoma enlargement in spontaneous intracerebral hemorrhage. J Neurosurg. 1994;80:51–57. doi: 10.3171/jns.1994.80.1.0051. [DOI] [PubMed] [Google Scholar]
- Kazui S, Naritomi H, Yamamoto H, Sawada T, Yamaguchi T. Enlargement of spontaneous intracerebral hemorrhage. Incidence and time course. Stroke. 1996;27:1783–1787. doi: 10.1161/01.str.27.10.1783. [DOI] [PubMed] [Google Scholar]
- Mayer SA, Brun NC, Begtrup K, Broderick J, Davis S, Diringer MN, Skolnick BE, Steiner T. Recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2005;352:777–785. doi: 10.1056/NEJMoa042991. [DOI] [PubMed] [Google Scholar]
- Piriyawat PML, Yawn DH, Hall CE, Grotta JC. Treatment of Acute Intracerebral Hemorrhage with epsilon aminocaproic Acid: a pilot study. Neurocritical Care. 2004;1:47–51. doi: 10.1385/ncc:1:1:47. [DOI] [PubMed] [Google Scholar]
- Mayer SA, Brun NC, Begtrup K, Broderick J, Davis S, Diringer MN, Skolnick BE, Steiner T. Efficacy and safety of recombinant activated factor VII for acute intracerebral hemorrhage. N Engl J Med. 2008;358:2127–2137. doi: 10.1056/NEJMoa0707534. [DOI] [PubMed] [Google Scholar]
- Wintzen AR, de Jonge H, Loeliger EA, Bots GT. The risk of intracerebral hemorrhage during oral anticoagulant therapy: a population study. Ann Neurol. 1984;16:553–558. doi: 10.1002/ana.410160505. [DOI] [PubMed] [Google Scholar]
- Hart RG, Boop BS, Anderson DC. Oral anticoagulants and intracranial hemorrhage. Facts and hypotheses. Stroke. 1995;26:1471–1477. doi: 10.1161/01.str.26.8.1471. [DOI] [PubMed] [Google Scholar]
- Fredriksson K, Norrving B, Stromblad LG. Emergency reversal of anticoagulation after intracerebral hemorrhage. Stroke. 1992;23:972–977. doi: 10.1161/01.str.23.7.972. [DOI] [PubMed] [Google Scholar]
- Makris M, Greaves M, Phillips WS, Kitchen S, Rosendaal FR, Preston EF. Emergency oral anticoagulant reversal: the relative efficacy of infusions of fresh frozen plasma and clotting factor concentrate on correction of the coagulopathy. Thromb Haemost. 1997;77:477–480. [PubMed] [Google Scholar]
- Yasaka M, Sakata T, Minematsu K, Naritomi H. Correction of INR by prothrombin complex concentrate and vitamin K in patients with warfarin related hemorrhagic complication. Thromb Res. 2002;108:25–30. doi: 10.1016/s0049-3848(02)00402-4. [DOI] [PubMed] [Google Scholar]
- Heit JA. Perioperative management of the chronically anticoagulated patient. J Thromb Thrombolysis. 2001;12:81–87. doi: 10.1023/a:1012746729537. [DOI] [PubMed] [Google Scholar]
- Sorensen B, Johansen P, Nielsen GL, Sorensen JC, Ingerslev J. Reversal of the International Normalized Ratio with recombinant activated factor VII in central nervous system bleeding during warfarin thromboprophylaxis: clinical and biochemical aspects. Blood Coagul Fibrinolysis. 2003;14:469–477. doi: 10.1097/00001721-200307000-00007. [DOI] [PubMed] [Google Scholar]
- Erhardtsen E, Nony P, Dechavanne M, Ffrench P, Boissel JP, Hedner U. The effect of recombinant factor VIIa (NovoSeven) in healthy volunteers receiving acenocoumarol to an International Normalized Ratio above 2.0. Blood Coagul Fibrinolysis. 1998;9:741–748. doi: 10.1097/00001721-199811000-00003. [DOI] [PubMed] [Google Scholar]
- Freeman WD, Brott TG, Barrett KM, Castillo PR, Deen HG, Jr, Czervionke LF, Meschia JF. Recombinant factor VIIa for rapid reversal of warfarin anticoagulation in acute intracranial hemorrhage. Mayo Clin Proc. 2004;79:1495–1500. doi: 10.4065/79.12.1495. [DOI] [PubMed] [Google Scholar]
- Wakefield TW, Stanley JC. Intraoperative heparin anticoagulation and its reversal. Semin Vasc Surg. 1996;9:296–302. [PubMed] [Google Scholar]
- Mannucci PM, Remuzzi G, Pusineri F, Lombardi R, Valsecchi C, Mecca G, Zimmerman TS. Deamino-8-D-arginine vasopressin shortens the bleeding time in uremia. N Engl J Med. 1983;308:8–12. doi: 10.1056/NEJM198301063080102. [DOI] [PubMed] [Google Scholar]
- Ananthasubramaniam K, Beattie JN, Rosman HS, Jayam V, Borzak S. How safely and for how long can warfarin therapy be withheld in prosthetic heart valve patients hospitalized with a major hemorrhage? Chest. 2001;119:478–484. doi: 10.1378/chest.119.2.478. [DOI] [PubMed] [Google Scholar]
- Mayer SA, Sacco RL, Shi T, Mohr JP. Neurologic deterioration in noncomatose patients with supratentorial intracerebral hemorrhage. Neurology. 1994;44:1379–1384. doi: 10.1212/wnl.44.8.1379. [DOI] [PubMed] [Google Scholar]
- Mayer SA, Chong J. Critical care management of increased intracranial pressure. J Intensive Care Med. 2002;17:55–67. [Google Scholar]
- Diringer MN, Edwards DF. Admission to a neurologic/neurosurgical intensive care unit is associated with reduced mortality rate after intracerebral hemorrhage. Crit Care Med. 2001;29:635–640. doi: 10.1097/00003246-200103000-00031. [DOI] [PubMed] [Google Scholar]
- Mirski MA, Chang CW, Cowan R. Impact of a neuroscience intensive care unit on neurosurgical patient outcomes and cost of care: evidence-based support for an intensivist-directed specialty ICU model of care. J Neurosurg Anesthesiol. 2001;13:83–92. doi: 10.1097/00008506-200104000-00004. [DOI] [PubMed] [Google Scholar]
- Hemphill JC, 3rd, Newman J, Zhao S, Johnston SC. Hospital usage of early do-not-resuscitate orders and outcome after intracerebral hemorrhage. Stroke. 2004;35:1130–1134. doi: 10.1161/01.STR.0000125858.71051.ca. [DOI] [PubMed] [Google Scholar]
- Becker KJ, Baxter AB, Cohen WA, Bybee HM, Tirschwell DL, Newell DW, Winn HR, Longstreth WT., Jr Withdrawal of support in intracerebral hemorrhage may lead to self-fulfilling prophecies. Neurology. 2001;56:766–772. doi: 10.1212/wnl.56.6.766. [DOI] [PubMed] [Google Scholar]
- Ziai WC, Toung TJ, Bhardwaj A. Hypertonic saline: first-line therapy for cerebral edema? J Neurol Sci. 2007;261:157–166. doi: 10.1016/j.jns.2007.04.048. [DOI] [PubMed] [Google Scholar]
- Adrogue HJ, Madias NE. Hypernatremia. N Engl J Med. 2000;342:1493–1499. doi: 10.1056/NEJM200005183422006. [DOI] [PubMed] [Google Scholar]
- Broderick JP, Adams HP, Jr, Barsan W, Feinberg W, Feldmann E, Grotta J, Kase C, Krieger D, Mayberg M, Tilley B, Zabramski JM, Zuccarello M. Guidelines for the management of spontaneous intracerebral hemorrhage: A statement for healthcare professionals from a special writing group of the Stroke Council, American Heart Association. Stroke. 1999;30:905–915. doi: 10.1161/01.str.30.4.905. [DOI] [PubMed] [Google Scholar]
- Passero S, Rocchi R, Rossi S, Ulivelli M, Vatti G. Seizures after spontaneous supratentorial intracerebral hemorrhage. Epilepsia. 2002;43:1175–1180. doi: 10.1046/j.1528-1157.2002.00302.x. [DOI] [PubMed] [Google Scholar]
- Vespa PM, O'Phelan K, Shah M, Mirabelli J, Starkman S, Kidwell C, Saver J, Nuwer MR, Frazee JG, McArthur DA, Martin NA. Acute seizures after intracerebral hemorrhage: A factor in progressive midline shift and outcome. Neurology. 2003;60:1441–1446. doi: 10.1212/01.wnl.0000063316.47591.b4. [DOI] [PubMed] [Google Scholar]
- Claassen J, Jetté N, Chum F, Green R, Schmidt M, Choi H, Jirsch J, Frontera JA, Connolly ES, Emerson RG, Mayer SA, Hirsch LJ. Electrographic seizures and periodic discharges after intracerebral hemorrhage. Neurology. 2007;25:1356–1365. doi: 10.1212/01.wnl.0000281664.02615.6c. [DOI] [PubMed] [Google Scholar]
- Commichau C, Scarmeas N, Mayer SA. Risk factors for fever in the neurologic intensive care unit. Neurology. 2003;60:837–841. doi: 10.1212/01.wnl.0000047344.28843.eb. [DOI] [PubMed] [Google Scholar]
- Szczudlik A, Turaj W, Slowik A, Strojny J. Hyperthermia is not an independent predictor of greater mortality in patients with primary intracerebral hemorrhage. Med Sci Monit. 2002;8:CR702–707. [PubMed] [Google Scholar]
- Baena RC, Busto R, Dietrich WD, Globus MY, Ginsberg MD. Hyperthermia delayed by 24 hours aggravates neuronal damage in rat hippocampus following global ischemia. Neurology. 1997;48:768–773. doi: 10.1212/wnl.48.3.768. [DOI] [PubMed] [Google Scholar]
- Minamisawa H, Smith ML, Siesjo BK. The effect of mild hyperthermia and hypothermia on brain damage following 5, 10, and 15 minutes of forebrain ischemia. Ann Neurol. 1990;28:26–33. doi: 10.1002/ana.410280107. [DOI] [PubMed] [Google Scholar]
- Clasen RA, Pandolfi S, Laing I, Casey D., Jr Experimental study of relation of fever to cerebral edema. J Neurosurg. 1974;41:576–581. doi: 10.3171/jns.1974.41.5.0576. [DOI] [PubMed] [Google Scholar]
- Rossi S, Zanier ER, Mauri I, Columbo A, Stocchetti N. Brain temperature, body core temperature, and intracranial pressure in acute cerebral damage. J Neurol Neurosurg Psychiatry. 2001;71:448–454. doi: 10.1136/jnnp.71.4.448. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Schwab S, Georgiadis D, Berrouschot J, Schellinger PD, Graffagnino C, Mayer SA. Feasibility and safety of moderate hypothermia after massive hemispheric infarction. Stroke. 2001;32:2033–2035. doi: 10.1161/hs0901.095394. [DOI] [PubMed] [Google Scholar]
- Mayer S, Commichau C, Scarmeas N, Presciutti M, Bates J, Copeland D. Clinical trial of an air-circulating cooling blanket for fever control in critically ill neurologic patients. Neurology. 2001;56:292–298. doi: 10.1212/wnl.56.3.292. [DOI] [PubMed] [Google Scholar]
- Diringer MN. Treatment of fever in the neurologic intensive care unit with a catheter-based heat exchange system. Crit Care Med. 2004;32:559–564. doi: 10.1097/01.CCM.0000108868.97433.3F. [DOI] [PubMed] [Google Scholar]
- Mayer SA, Kowalski RG, Presciutti M, Ostapkovich ND, McGann E, Fitzsimmons BF, Yavagal DR, Du YE, Naidech AM, Janjua NA, Claassen J, Kreiter KT, Parra A, Commichau C. Clinical trial of a novel surface cooling system for fever control in neurocritical care patients. Crit Care Med. 2004;32:2508–2515. doi: 10.1097/01.ccm.0000147441.39670.37. [DOI] [PubMed] [Google Scholar]
- Fogelholm R, Murros K, Rissanen A, Avikainen S. Admission blood glucose and short term survival in primary intracerebral haemorrhage: a population based study. J Neurol Neurosurg Psychiatry. 2005;76:349–353. doi: 10.1136/jnnp.2003.034819. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Baird TA, Parsons MW, Phanh T, Butcher KS, Desmond PM, Tress BM, Colman PG, Chambers BR, Davis SM. Persistent poststroke hyperglycemia is independently associated with infarct expansion and worse clinical outcome. Stroke. 2003;34:2208–2214. doi: 10.1161/01.STR.0000085087.41330.FF. [DOI] [PubMed] [Google Scholar]
- Capes SE, Hunt D, Malmberg K, Pathak P, Gerstein HC. Stress hyperglycemia and prognosis of stroke in nondiabetic and diabetic patients: a systematic overview. Stroke. 2001;32:2426–2432. doi: 10.1161/hs1001.096194. [DOI] [PubMed] [Google Scholar]
- Williams LS, Rotich J, Qi R, Fineberg N, Espay A, Bruno A, Fineberg SE, Tierney WR. Effects of admission hyperglycemia on mortality and costs in acute ischemic stroke. Neurology. 2002;59:67–71. doi: 10.1212/wnl.59.1.67. [DOI] [PubMed] [Google Scholar]
- Klip A, Tsakiridis T, Marette A, Ortiz PA. Regulation of expression of glucose transporters by glucose: a review of studies in vivo and in cell cultures. Faseb J. 1994;8:43–53. doi: 10.1096/fasebj.8.1.8299889. [DOI] [PubMed] [Google Scholar]
- Berghe G Van den. How does blood glucose control with insulin save lives in intensive care? J Clin Invest. 2004;114:1187–1195. doi: 10.1172/JCI23506. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Langouche L, Berghe G Van den. Glucose metabolism and insulin therapy. Crit Care Clin. 2006;22:119–129. doi: 10.1016/j.ccc.2005.09.005. [DOI] [PubMed] [Google Scholar]
- Berghe G Van den, Schoonheydt K, Becx P, Bruyninckx F, Wouters PJ. Insulin therapy protects the central and peripheral nervous system of intensive care patients. Neurology. 2005;64:1348–1353. doi: 10.1212/01.WNL.0000158442.08857.FC. [DOI] [PubMed] [Google Scholar]
- Nilsson OG, Lindgren A, Brandt L, Saveland H. Prediction of death in patients with primary intracerebral hemorrhage: a prospective study of a defined population. J Neurosurg. 2002;97:531–536. doi: 10.3171/jns.2002.97.3.0531. [DOI] [PubMed] [Google Scholar]
- Tuhrim S, Horowitz DR, Sacher M, Godbold JH. Volume of ventricular blood is an important determinant of outcome in supratentorial intracerebral hemorrhage. Crit Care Med. 1999;27:617–621. doi: 10.1097/00003246-199903000-00045. [DOI] [PubMed] [Google Scholar]
- Bowers SA, Marshall LF. Outcome in 200 consecutive cases of severe head injury treated in San Diego County: a prospective analysis. Neurosurgery. 1980;6:237–242. [PubMed] [Google Scholar]
- Unwin DH, Giller CA, Kopitnik TA. Central nervous system monitoring: what helps, what does not. Surg Clin North Am. 1991;71:733–747. doi: 10.1016/s0039-6109(16)45483-6. [DOI] [PubMed] [Google Scholar]
- Lozier AP, Sciacca RR, Romagnoli MF, Connolly ES., Jr Ventriculostomy-related infections: a critical review of the literature. Neurosurgery. 2002;51:170–181. doi: 10.1097/00006123-200207000-00024. [DOI] [PubMed] [Google Scholar]
- Adams RE, Diringer MN. Response to external ventricular drainage in spontaneous intracerebral hemorrhage with hydrocephalus. Neurology. 1998;50:519–523. doi: 10.1212/wnl.50.2.519. [DOI] [PubMed] [Google Scholar]
- Albanese J, Durbec O, Viviand X, Potie F, Alliez B, Martin C. Sufentanil increases intracranial pressure in patients with head trauma. Anesthesiology. 1993;79:493–497. doi: 10.1097/00000542-199309000-00012. [DOI] [PubMed] [Google Scholar]
- Kelly DF, Goodale DB, Williams J, Herr DL, Chappell ET, Rosner MJ, Jacobson J, Levy ML, Croce MA, Maniker AH, Fulda GJ, Lovett JV, Mohan O, Narayan RK. Propofol in the treatment of moderate and severe head injury: a randomized, prospective double-blinded pilot trial. J Neurosurg. 1999;90:1042–1052. doi: 10.3171/jns.1999.90.6.1042. [DOI] [PubMed] [Google Scholar]
- Kam PC, Cardone D. Propofol infusion syndrome. Anaesthesia. 2007;62:690–701. doi: 10.1111/j.1365-2044.2007.05055.x. [DOI] [PubMed] [Google Scholar]
- Lundberg N. Continuous recording and control of ventricular fluid pressure in neurosurgical practice. Acta Psychiatr Scand Suppl. 1960;36:1–193. [PubMed] [Google Scholar]
- Chambers IR, Banister K, Mendelow AD. Intracranial pressure within a developing intracerebral haemorrhage. Br J Neurosurg. 2001;15:140–141. doi: 10.1080/02688690120036847. [DOI] [PubMed] [Google Scholar]
- Fernandes HM, Siddique S, Banister K, Chambers I, Wooldridge T, Gregson B, Mendelow AD. Continuous monitoring of ICP and CPP following ICH and its relationship to clinical, radiological and surgical parameters. Acta Neurochir Suppl. 2000;76:463–466. doi: 10.1007/978-3-7091-6346-7_96. [DOI] [PubMed] [Google Scholar]
- Qureshi AI, Suarez JI. Use of hypertonic saline solutions in treatment of cerebral edema and intracranial hypertension. Crit Care Med. 2000;28:3301–3313. doi: 10.1097/00003246-200009000-00032. [DOI] [PubMed] [Google Scholar]
- Misra UK, Kalita J, Ranjan P, Mandal SK. Mannitol in intracerebral hemorrhage: a randomized controlled study. J Neurol Sci. 2005;234:41–45. doi: 10.1016/j.jns.2005.03.038. [DOI] [PubMed] [Google Scholar]
- Qureshi AI, Geocadin RG, Suarez JI, Ulatowski JA. Long-term outcome after medical reversal of transtentorial herniation in patients with supratentorial mass lesions. Crit Care Med. 2000;28:1556–1564. doi: 10.1097/00003246-200005000-00049. [DOI] [PubMed] [Google Scholar]
- Shiozaki T, Sugimoto H, Taneda M, Yoshida H, Iwai A, Yoshioka T, Sugimoto T. Effect of mild hypothermia on uncontrollable intracranial hypertension after severe head injury. J Neurosurg. 1993;79:363–368. doi: 10.3171/jns.1993.79.3.0363. [DOI] [PubMed] [Google Scholar]
- Schwab S, Spranger M, Schwarz S, Hacke W. Barbiturate coma in severe hemispheric stroke: useful or obsolete? Neurology. 1997;48:1608–1613. doi: 10.1212/wnl.48.6.1608. [DOI] [PubMed] [Google Scholar]
- Rincon F, Mayer SA. Therapeutic hypothermia for brain injury after cardiac arrest. Semin Neurol. 2006;26:387–395. doi: 10.1055/s-2006-948319. [DOI] [PubMed] [Google Scholar]
- Hemphill JC, 3rd, Bonovich DC, Besmertis L, Manley GT, Johnston SC. The ICH score: a simple, reliable grading scale for intracerebral hemorrhage. Stroke. 2001;32:891–897. doi: 10.1161/01.str.32.4.891. [DOI] [PubMed] [Google Scholar]
- Naff NJ, Carhuapoma JR, Williams MA, Bhardwaj A, Ulatowski JA, Bederson J, Bullock R, Schmutzhard E, Pfausler B, Keyl PM, Tuhrim S, Hanley DF. Treatment of intraventricular hemorrhage with urokinase: effects on 30-day survival. Stroke. 2000;31:841–847. doi: 10.1161/01.str.31.4.841. [DOI] [PubMed] [Google Scholar]
- Coplin WM, Vinas FC, Agris JM, Buciuc R, Michael DB, Diaz FG, Muizelaar JP. A cohort study of the safety and feasibility of intraventricular urokinase for nonaneurysmal spontaneous intraventricular hemorrhage. Stroke. 1998;29:1573–1579. doi: 10.1161/01.str.29.8.1573. [DOI] [PubMed] [Google Scholar]
- Lapointe M, Haines S. Fibrinolytic therapy for intraventricular hemorrhage in adults. Cochrane Database Syst Rev. 2002:CD003692. doi: 10.1002/14651858.CD003692. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Evaluating Accelerated Resolution of Intraventricular Hemorrhage, rt-PA (Cathflo®) Treatment of Brain Hemorrhage http://www.strokecenter.org/trials/TrialDetail.aspx?tid=607
- Nyquist P, Hanley DF. The use of intraventricular thrombolytics in intraventricular hemorrhage. J Neurol Sci. 2007;261:84–88. doi: 10.1016/j.jns.2007.04.039. [DOI] [PubMed] [Google Scholar]
- Geerts WH, Pineo GF, Heit JA, Bergqvist D, Lassen MR, Colwell CW, Ray JG. Prevention of venous thromboembolism: the Seventh ACCP Conference on Antithrombotic and Thrombolytic Therapy. Chest. 2004;126(3 Suppl):338S–400S. doi: 10.1378/chest.126.3_suppl.338S. [DOI] [PubMed] [Google Scholar]
- Boeer A, Voth E, Henze T, Prange HW. Early heparin therapy in patients with spontaneous intracerebral haemorrhage. J Neurol Neurosurg Psychiatry. 1991;54:466–467. doi: 10.1136/jnnp.54.5.466. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Juvela S, Heiskanen O, Poranen A, Valtonen S, Kuurne T, Kaste M, Troupp H. The treatment of spontaneous intracerebral hemorrhage. A prospective randomized trial of surgical and conservative treatment. J Neurosurg. 1989;70:755–758. doi: 10.3171/jns.1989.70.5.0755. [DOI] [PubMed] [Google Scholar]
- Zuccarello M, Brott T, Derex L, Kothari R, Sauerbeck L, Tew J, Van Loveren H, Yeh HS, Tomsick T, Pancioli A, Khoury J, Broderick J. Early surgical treatment for supratentorial intracerebral hemorrhage: a randomized feasibility study. Stroke. 1999;30:1833–1839. doi: 10.1161/01.str.30.9.1833. [DOI] [PubMed] [Google Scholar]
- Fernandes HM, Gregson B, Siddique S, Mendelow AD. Surgery in intracerebral hemorrhage. The uncertainty continues. Stroke. 2000;31:2511–2516. doi: 10.1161/01.str.31.10.2511. [DOI] [PubMed] [Google Scholar]
- Mendelow AD, Gregson BA, Fernandes HM, Murray GD, Teasdale GM, Hope DT, Karimi A, Shaw MD, Barer DH. Early surgery versus initial conservative treatment in patients with spontaneous supratentorial intracerebral haematomas in the International Surgical Trial in Intracerebral Haemorrhage (STICH): a randomised trial. Lancet. 2005;365:387–397. doi: 10.1016/S0140-6736(05)17826-X. [DOI] [PubMed] [Google Scholar]
- Bhattathiri PS, Gregson B, Prasad KS, Mendelow AD. Intraventricular hemorrhage and hydrocephalus after spontaneous intracerebral hemorrhage: results from the STICH trial. Acta Neurochir Suppl. 2006;96:65–68. doi: 10.1007/3-211-30714-1_16. [DOI] [PubMed] [Google Scholar]
- STICH II Trial http://www.ncl.ac.uk/stich/
- Ott KH, Kase CS, Ojemann RG, Mohr JP. Cerebellar hemorrhage: diagnosis and treatment. A review of 56 cases. Arch Neurol. 1974;31:160–167. doi: 10.1001/archneur.1974.00490390042003. [DOI] [PubMed] [Google Scholar]
- Auer LM, Deinsberger W, Niederkorn K, Gell G, Kleinert R, Schneider G, Holzer P, Bone G, Mokry M, Korner E, et al. Endoscopic surgery versus medical treatment for spontaneous intracerebral hematoma: a randomized study. J Neurosurg. 1989;70:530–535. doi: 10.3171/jns.1989.70.4.0530. [DOI] [PubMed] [Google Scholar]
- Teernstra OP, Evers SM, Lodder J, Leffers P, Franke CL, Blaauw G. Stereotactic treatment of intracerebral hematoma by means of a plasminogen activator: a multicenter randomized controlled trial (SICHPA) Stroke. 2003;34:968–974. doi: 10.1161/01.STR.0000063367.52044.40. [DOI] [PubMed] [Google Scholar]
- Murthy JM, Chowdary GV, Murthy TV, Bhasha PS, Naryanan TJ. Decompressive craniectomy with clot evacuation in large hemispheric hypertensive intracerebral hemorrhage. Neurocritical care. 2005;2:258–262. doi: 10.1385/ncc:2:3:258. [DOI] [PubMed] [Google Scholar]
- Minimally Invasive Surgery Olus rtPA for Intracerebral Hemorrhage Evacuation (MISTIE) http://www.strokecenter.org/trials/TrialDetail.aspx?tid=690 [DOI] [PubMed]
- Rincon F, Mayer SA. Novel therapies for intracerebral hemorrhage. Curr Opin Crit Care. 2004;10:94–100. doi: 10.1097/00075198-200404000-00003. [DOI] [PubMed] [Google Scholar]