

Abstract
We report two cases in which the technique of fracture fixation using the Less Invasive Stabilisation System (LISS) has been successfully used in the management of distal femoral fractures in the child.
Keywords: Distal femoral fracture, Children, LISS plate
Fractures of the femoral shaft are one of the commonest major paediatric injuries managed by the orthopaedic surgeon. Definitive management decisions are influenced by fracture morphology, age, available resources, cost, associated injuries and surgical expertise. Traditionally, younger children have been treated conservatively using traction and cast immobilisation; in the older child, operative interventions including elastic nailing, plating and external fixation have been successfully utilised.1 Particular difficulty still exists with satisfactory treatment and outcomes of proximal and distal third femoral fractures.
The Less Invasive Stabilisation System (LISS) allows fracture fixation using a minimally invasive technique. In recent times, the LISS has been applied across a broad spectrum of fractures on either side of the knee joint2 and has proven itself to be a good alternative to more traditional stabilising techniques in the adult patient.3 We report two cases in which the technique of fracture fixation using the LISS has been successfully used in the management of distal femoral fractures in the child.
Case reports
A 13-year-old boy sustained a closed injury to his left femur after twisting it following a fall on the beach with his left foot anchored between two rocks. Radiographs revealed a spiral fracture of the distal third of the left femur extending distally to within 4 cm of the distal epiphysis (Fig. 1A). In the second case, a 12-year-old boy fell from a climbing frame landing directly onto his left leg sustaining a closed injury to his left distal femur (Fig. 2A). Radiographs revealed a similar complex spiral fracture of the distal third of the left femur extending almost to the physis.
Figure 1.

(A) Admission AP film showing a spiral fracture of the distal third of the left femur. (B) LISS plate construct in situ at 3 weeks with early callus formation. (C) Healed fracture at 10 weeks.
Figure 2.
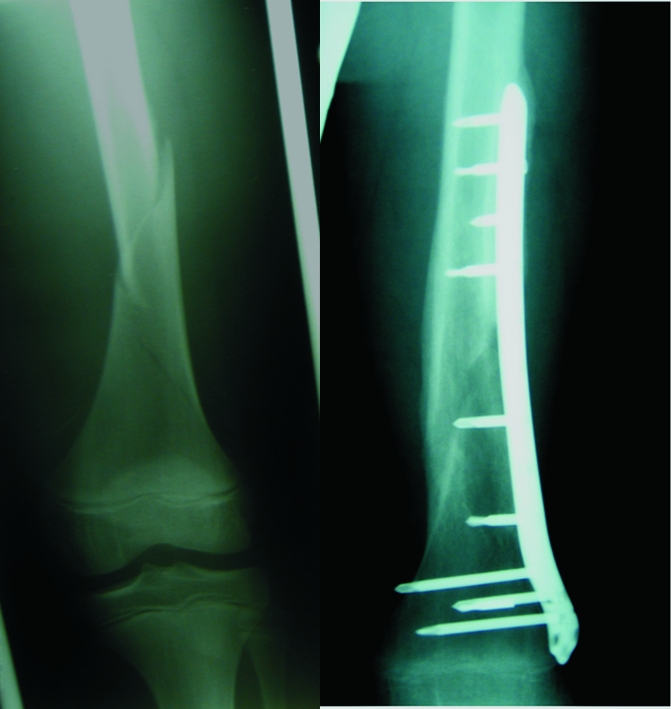
(A) Admission AP film showing a spiral fracture extending down to the distal femoral physis. (B) Fracture united at 4 months post fixation.
Due to the distal extent of the fractures, it was decided that conventional compression plating or intramedullary fixation would not give satisfactory control of the distal fragment, and external fixation could result in knee stiffness or intra-articular infection. The LISS was, therefore, employed to provide a minimally invasive stable internal construct (Fig. 1B).
Following fixation, both patients were mobilised non-weight bearing and were discharged on days 14 and 9 postoperatively. By 8 weeks there was adequate callus formation to allow partial weight bearing and, over the following 4 weeks, they both proceeded to full unassisted weight bearing correlating with clinical and radiological union (Figs 1C and 2B). By 3 months, both boys had been discharged from the care of the physiotherapy department having achieved full, pain-free mobility and a full range of movement in the knee comparable with the unaffected side. Both were back to participating in a full range of daily activities. No formal objective assessment of outcome using validated scoring systems was undertaken.
Discussion
The ideal treatment for femoral fractures in children is one that controls alignment, length and rotation, minimises joint stiffness, is comfortable and convenient for the child and family, and causes the least negative psychological impact possible. In the older adolescent child, operative intervention is usually preferred and numerous techniques have been described.1 Each has its own place in the management of these fractures and good results have been reported with flexible intramedullary nails, locked intramedullary devices, bridge compression plating, and external fixation.4 These techniques are, however, most applicable in mid-shaft fractures, and the proximal and distal third fractures remain a problem.
The Less Invasive Stabilisation System (LISS) was designed to combine the advantages of a locked intramedullary nailing technique and a ‘biological’ locked plating technique into one system.5 Since its conception, it has been applied to a broad range of clinical situations in adults with successful results.5 The two cases described above illustrate that this technique is also applicable to paediatric femoral fractures especially those in the adolescent child. In particular, it is useful in those fractures which extend distally towards the distal epiphysis where other, more conventional, techniques will not achieve adequate control of the distal fragment, offer adequate fixation or may encroach on the growth plate with its associated complications.
In our two cases, both patients had sustained long spiral fractures with a large surface area which allows rapid fracture healing. Following indirect freehand reduction under radiographic screening, the LISS plate was inserted percutaneously in the submuscular plane via a lateral approach. In these cases, ensuring correct fracture alignment is more important than achieving full anatomical reduction and, due to the design of the LISS plate, there is also no need for compression of the fracture. It is important to use at least four locking screws either side of the fracture to achieve adequate control. Consideration must be given to placement of the distal cluster of screws, as they do not sit perpendicular to the plate and instead diverge distally. If placed too close to the distal physis, these screws may inadvertently penetrate. In both of these cases, a 9-hole (236 mm) plate was used; however, 5-hole (156 mm) and 13-hole (316 mm) plates are available allowing assorted fracture configurations, in femurs of various lengths to be effectively spanned.
In these two cases, excellent recovery was seen and, by 3 months, both patients were back to full pre-morbid mobility. Full range of knee movement was regained. There was no valgus/varus or rotational malalignment as assessed by the alignment of the hip/knee/ankle axis, no leg-length discrepancy when compared to the uninjured leg, and no residual symptoms of pain or stiffness were described. Assessment was purely clinical and radiographic evaluation with long-leg films and comparative views of the uninjured leg were not performed.
The adaptation of a specialist plating system designed for use in complex peri-articular or metaphyseal fractures around the knee in the adult offers an excellent opportunity for fixation of fractures of the distal third of the paediatric femur. When faced with these difficult fractures, use of the LISS plate should be considered.
References
- 1.Hunter J. Femoral shaft fractures in children. Injury. 2005;36:S-A-86–93. doi: 10.1016/j.injury.2004.12.018. [DOI] [PubMed] [Google Scholar]
- 2.Schandelmaier P, Partheimer A, Koenemann B, Grun O, Krettek C. Distal femoral fractures and LISS stabilisation. Injury. 2001;32:S-C-55–63. doi: 10.1016/s0020-1383(01)00184-x. [DOI] [PubMed] [Google Scholar]
- 3.Kregor K, Stannard J, Zlowodski M, Cole P. Treatment of distal femoral fractures using the Less Invasive Stabilisation System: surgical experience and early clinical results in 103 fractures. J Orthop Trauma. 2004;18:509–20. doi: 10.1097/00005131-200409000-00006. [DOI] [PubMed] [Google Scholar]
- 4.Canale S. Campbell's Operative Orthopaedics. 9th edn. St Louis, MO: Mosby Year Book; 1998. pp. 2476–82. Chapter 50, Part XII. [Google Scholar]
- 5.Frigg R, Appenzeller A, Christensen R, Frenk A, Gilbert S, Schavan R. The development of the distal femur Less Invasive Stabilisation System (LISS) Injury. 2001;32:S-C-24–31. doi: 10.1016/s0020-1383(01)00181-4. [DOI] [PubMed] [Google Scholar]