

Abstract
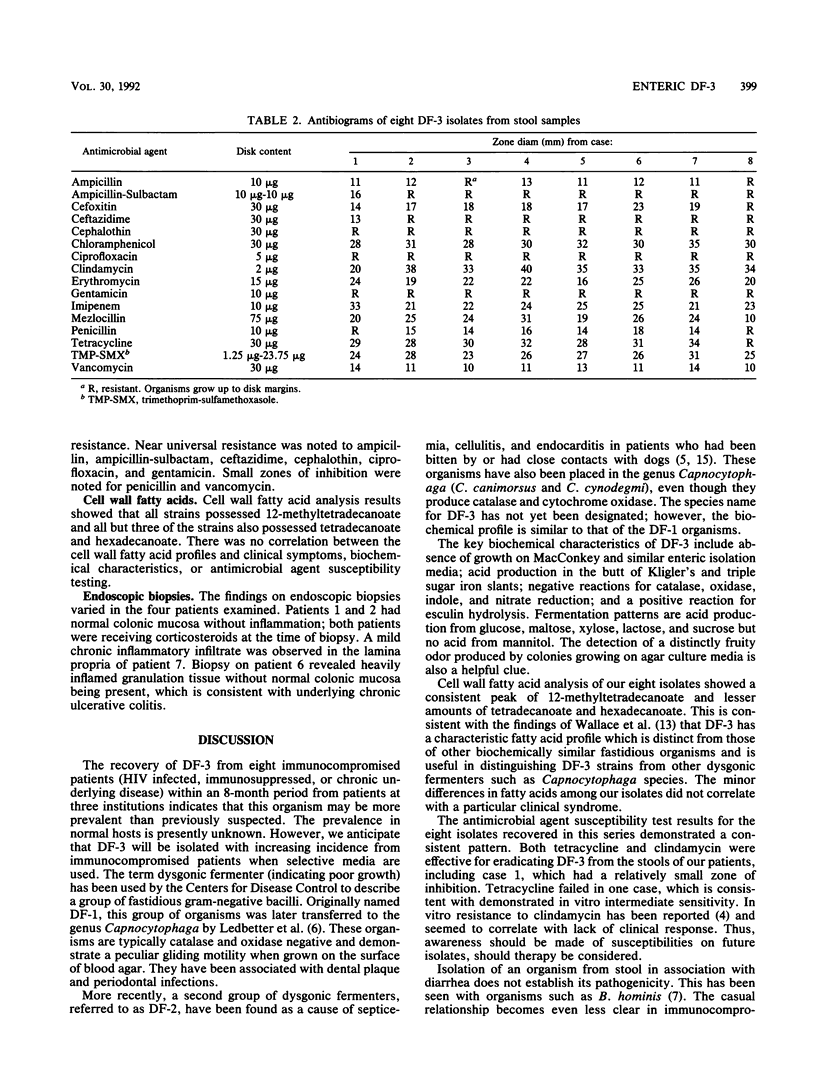
The clinical significance of the fastidious organism DF-3 isolated from stool cultures is unclear. We sought to improve our understanding of this organism and to further define its association with human disease. Stool cultures for DF-3 were obtained from three sources: an ongoing study of enteric pathogens in patients infected with the human immunodeficiency virus, a screening procedure in which all stool samples submitted for Clostridium difficile toxin assay were cultured for DF-3, and stool samples submitted specifically for DF-3 culture. Retrospective clinical data were obtained from chart reviews of patients with positive cultures. Antimicrobial susceptibility testing and cell wall fatty acid analysis were performed for each DF-3 isolated. Eight isolates of DF-3 were obtained over a period of 8 months. All patients either had severe underlying disease or were immunocompromised, including three patients coinfected with human immunodeficiency virus and two patients with inflammatory bowel disease. The spectrum of clinical disease ranged from chronic diarrhea with a well-defined response to therapy for DF-3 to an asymptomatic carrier state. Cell wall fatty acid analysis of these isolates demonstrated a consistent pattern with a large peak of 12-methyltetradecanoate. DF-3, a fastidious gram-negative coccobacillus, can be recovered from stool cultures of immunocompromised patients by using selective media. The presence of 12-methyltetradecanoate in cell wall fatty acid analysis assists in identification. The increased use of a selective medium-(cefoperazone-vancomycin-amphotericin B) in the evaluation of diarrhea in immunocompromised hosts, including persons with inflammatory bowel disease, may better define the association of DF-3 with human gastrointestinal disease.
Full text
PDF

Selected References
These references are in PubMed. This may not be the complete list of references from this article.
- Aronson N. E., Zbick C. J. Dysgonic fermenter 3 bacteremia in a neutropenic patient with acute lymphocytic leukemia. J Clin Microbiol. 1988 Oct;26(10):2213–2215. doi: 10.1128/jcm.26.10.2213-2215.1988. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Bangsborg J. M., Frederiksen W., Bruun B. Dysgonic fermenter 3-associated abscess in a diabetic patient. J Infect. 1990 May;20(3):237–240. doi: 10.1016/0163-4453(90)91194-i. [DOI] [PubMed] [Google Scholar]
- Bodey G. P., Fainstein V. Infections of the gastrointestinal tract in the immunocompromised patient. Annu Rev Med. 1986;37:271–281. doi: 10.1146/annurev.me.37.020186.001415. [DOI] [PubMed] [Google Scholar]
- Hicklin H., Verghese A., Alvarez S. Dysgonic fermenter 2 septicemia. Rev Infect Dis. 1987 Sep-Oct;9(5):884–890. doi: 10.1093/clinids/9.5.884. [DOI] [PubMed] [Google Scholar]
- Leadbetter E. R., Holt S. C., Socransky S. S. Capnocytophaga: new genus of gram-negative gliding bacteria. I. General characteristics, taxonomic considerations and significance. Arch Microbiol. 1979 Jul;122(1):9–16. doi: 10.1007/BF00408040. [DOI] [PubMed] [Google Scholar]
- Markell E. K., Udkow M. P. Association of Blastocystis hominis with human disease? J Clin Microbiol. 1990 May;28(5):1085–1086. doi: 10.1128/jcm.28.5.1085-1086.1990. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Perlman D. M., Ampel N. M., Schifman R. B., Cohn D. L., Patton C. M., Aguirre M. L., Wang W. L., Blaser M. J. Persistent Campylobacter jejuni infections in patients infected with the human immunodeficiency virus (HIV). Ann Intern Med. 1988 Apr;108(4):540–546. doi: 10.7326/0003-4819-108-4-540. [DOI] [PubMed] [Google Scholar]
- René E., Marche C., Regnier B., Saimot A. G., Vilde J. L., Perrone C., Michon C., Wolf M., Chevalier T., Vallot T. Intestinal infections in patients with acquired immunodeficiency syndrome. A prospective study in 132 patients. Dig Dis Sci. 1989 May;34(5):773–780. doi: 10.1007/BF01540353. [DOI] [PubMed] [Google Scholar]
- Smith P. D., Lane H. C., Gill V. J., Manischewitz J. F., Quinnan G. V., Fauci A. S., Masur H. Intestinal infections in patients with the acquired immunodeficiency syndrome (AIDS). Etiology and response to therapy. Ann Intern Med. 1988 Mar;108(3):328–333. doi: 10.7326/0003-4819-108-3-328. [DOI] [PubMed] [Google Scholar]
- Wagner D. K., Wright J. J., Ansher A. F., Gill V. J. Dysgonic fermenter 3-associated gastrointestinal disease in a patient with common variable hypogammaglobulinemia. Am J Med. 1988 Feb;84(2):315–318. doi: 10.1016/0002-9343(88)90432-9. [DOI] [PubMed] [Google Scholar]
- Wallace P. L., Hollis D. G., Weaver R. E., Moss C. W. Characterization of CDC group DF-3 by cellular fatty acid analysis. J Clin Microbiol. 1989 Apr;27(4):735–737. doi: 10.1128/jcm.27.4.735-737.1989. [DOI] [PMC free article] [PubMed] [Google Scholar]
- Yolken R. H., Bishop C. A., Townsend T. R., Bolyard E. A., Bartlett J., Santos G. W., Saral R. Infectious gastroenteritis in bone-marrow-transplant recipients. N Engl J Med. 1982 Apr 29;306(17):1010–1012. doi: 10.1056/NEJM198204293061701. [DOI] [PubMed] [Google Scholar]
- Zumla A., Lipscomb G., Corbett M., McCarthy M. Dysgonic Fermenter-type 2: an emerging zoonosis. Report of two cases and review. Q J Med. 1988 Sep;68(257):741–752. [PubMed] [Google Scholar]