

Abstract
Background and aims
The occiput-wall distance (OWD), a measure of kyphosis, has been associated with postural instability, osteoporosis, disability and depression. The association between OWD and measures of physical performance was evaluated.
Methods
Data from the Invecchiare in Chianti (InCHIANTI) study on home-dwelling people were used. People younger than 65 years and with overt disability at baseline assessment were excluded. The sample population was divided into three groups according to the OWD distribution (1st quartile: short OWD; 2nd and 3rd quartiles: medium OWD; 4th quartile: long OWD). Performance scores were expressed as the percentage of the best performance in this population.
Results
783 persons (55% women) were studied. The mean age for men was 73.8 (SD 6.34) and 75.0 (SD 6.85) for women. In men, a longer OWD was associated with reduced balance and walking speed, but not with impaired performance at the chair standing test. Overall, the association between increased OWD and reduced physical function was weak. In women, OWD was associated with a reduced walking speed, expressed as a percentage of the best performance (mean [SD]: 77% [12], 72% [14], 66% [15] in short, medium and long OWD groups, respectively), and impaired balance (mean [SD]: 97% [11], 95% [13], 90% [21] for short, medium and long OWD groups, respectively).
Conclusions
Our findings suggest that OWD is an easily measurable marker of poor physical function in women. Further research should verify whether OWD predicts incident disability.
Keywords: Aged, kyphosis, physical performance
Introduction
Kyphosis is defined as a sagittal deviation in the spinal alignment, with a backward curve of the thoracic spine exceeding 20-40 degrees (1). The occiput-wall distance (OWD) is a surrogate measure of kyphosis. Although it cannot substitute highly accurate clinical measures of kyphosis such as Cobb's angle, OWD has been extensively used in epidemiological studies. It has been associated with depressed mood, postural instability, muscle weakness and disability in older women (2), and may account for a large percentage of the dyspnea and restrictive/obstructive respiratory dysfunction that often remains unexplained in older persons (3). In the Rancho-Bernardo study, OWD was found to be inversely related to several measures of physical performance, but it was not clear whether osteoporosis mediated this relationship to some extent (4). A qualitative measure of kyphosis was independently associated with increased time to walk 5 meters and to climb a flight of stairs, and with self-reported difficulties in performing heavy housework (5). Based on these findings, we hypothesized that OWD is an easily measurable marker of reduced physical function in older persons, and this study was performed to investigate its association with measures of physical performance (balance, gait speed, chair standing) in a population of community-dwelling people aged 65 years or older.
Methods
Study population
We used data from the Invecchiare in Chianti (InCHIANTI) study, a population-based study designed to investigate factors contributing to the decline in mobility in older persons (6). Study participants were randomly selected from the population of two towns in the Chianti region: Greve in Chianti and Bagno a Ripoli. Eligible subjects who agreed to participate were interviewed at their homes by trained study researchers using a structured questionnaire investigating the health status, physical and cognitive performance and other factors possibly related to loss of independence in late life. Interviews were followed by physical examinations at the study clinic. The InCHIANTI database includes 1453 persons who completed the home interview. Of these, 282 were excluded because they were younger than 65 years, 92 because they had overt disability (inability to perform without help one of the activities of daily living), and 160 because of missing values for OWD or height. The final sample included 783 subjects, of which 431 (55.0%) were women.
Occiput-wall distance measurement
OWD was measured during the clinical examination. A rigid measurement tape was used to measure the distance between the prominence of the 7th cervical vertebra and the wall, while the participant was standing with both heels and the sacrum against the wall, and with the lower orbital margin and upper margin of the acoustic meatus on the horizontal plane.
Measures of performance
The results of three performance-based tests were used in the analysis: balance, gait speed, and repeated chair stands (7). Balance was evaluated by asking participants to attempt to maintain their feet in the side-by-side, semi-tandem (heel of one foot against the big toe of the other foot), and tandem position for 10 seconds each. The ability to rise from a chair was evaluated by asking the participants to fold their arms over their chest and to stand up from a sitting position. If they were able to perform the task, they were asked to repeat the exercise five times, as quickly as possible. Walking speed was evaluated over a 4-meter distance, using the better of two trials. For each test, performance was expressed as the percentage of the best performance recorded in this sample. Best performance was defined as the 1st percentile of the distribution. In this way, the score for the balance test was calculated as performance/30, for the chair standing test as performance/6.6 sec, and for walking speed as performance/1.62 m*sec-1, yielding a score ranging from 0 (worst performance) to 1 (best performance) (8). A summary performance score was obtained by adding the three individual score and dividing by three.
Analytic approach
As the biomechanical effects of OWD are expected to change as a function of height, and OWD is expected to increase with increasing distance between the upper limit of the kyphotic curve and the occiput, we decided to express OWD as a percentage of height. On the basis of preliminary analyses, we considered outliers, and therefore excluded people with an OWD greater than 10 (99th centile of distribution; n=11). Also, a different effect of OWD was expected in men and women, and therefore all analyses were stratified by gender. Gender-specific percentiles were used to split OWD into three groups: <25th (short OWD group), between 25th and the 74th (medium OWD group), and equal to or above the 75th percentile (long OWD group). The cut-offs used were 2.39% and 3.55% of height in men, and 2.58% and 3.90% of height in women.
The physical performance scores was also dichotomized using the gender-specific median value for each test. The cut-offs used for men were 1 for performance in the test of balance, 0.67 for chair standing, 0.71 for walking speed, and 0.80 for the summary score. The corresponding cut-off values in women were 1, 0.58, 0.64, and 0.72.
Differences between OWD classes were described with respect to demographic and clinical characteristics, including medical conditions and depression. Disease diagnoses were based on a standard algorithm which considered information on medical history, physical examination, medical records, medications, and diagnostic tests performed during the evaluation. Bone density was evaluated by peripheral quantitative computed tomography of the tibia (XCT 2000, Stratec Medizintechnik, Pforzheim, Germany), implemented with software (BonAlyse, BonAlyse Oy, Jyvaskyla, Finland) which automatically identifies bone tissue (cortical and trabecular), to derive total, cortical and trabecular volumetric bone mass density. Osteoporosis was diagnosed when any of the following scores was below the normal range: trabecular bone density at 4% of tibial length, cortical bone density at 38% of tibial length, and bone area at 38% of tibial length. Calculations were performed separately for men and women. Depressive symptoms were evaluated by the Center for Epidemiologic Studies Depression Scale (CES-D) (9), with a cut-off of 16 to identify participants with depression (10).
Since kyphosis may be caused by osteoporosis, groups were compared with respect to bone density measured by a computerized tomography at the 38% of the tibia (11).
Statistical analysis
Contingency tables were used to analyze the relationship between OWD classes and variables of interest. Analysis of variance was applied to evaluate differences in performance scores across OWD classes. As our aim was to verify whether OWD could be used as a simple screening tool for reduced physical function, we did not expect the association to be independent of other variables, and therefore we based our analyses on crude associations. However, to better understand the mechanism linking increased OWD with our outcomes, analysis of co-variance was applied to verify an association taking into account potential confounders. All analyses were performed with SAS V8.0 for Windows (SAS Institute, Cary, NC).
Results
783 persons were studied, of whom 431 (55.0%) were women. The mean age for men was 73.8 (SD 6.34), and 75.0 (SD 6.85) for women.
Men
Table 1 (upper panel) shows the differences in clinical characteristics across OWD groups in men. Age was strongly correlated with OWD, and more than 50% of those with long OWD were aged 75 years or more, compared with 19.5% of those with short OWD. Increased OWD was associated with ischemic heart disease, cerebro-vascular disease, and heart failure.
Table 1. Clinical characteristics according to occiput-wall distance (OWD) in men and women.
| MEN (n=352) | |||
|---|---|---|---|
| OWD* | |||
| Short (n=87) % |
Medium (n=175) % |
Long (n=90) % |
|
| Age ≥75 years | 19.5 | 36.6 | 54.4 |
| Parkinson's Disease | 1.2 | 2.9 | 2.2 |
| Ischemic heart disease | 5.7 | 12.6 | 21.1 |
| Cerebrovascular disease | 3.4 | 5.7 | 11.1 |
| Heart failure | 19.5 | 20.0 | 36.7 |
| Diabetes mellitus | 11.5 | 16.6 | 12.2 |
| Chronic obstructive pulmonary disease | 19.5 | 16.6 | 17.8 |
| Hip fracture | 1.1 | 2.3 | 1.1 |
| Hip arthritis | 6.9 | 6.3 | 11.1 |
| Knee arthritis | 16.1 | 13.7 | 24.4 |
| Depressed mood | 19.5 | 13.8 | 16.8 |
| Osteoporosis | 52.9 | 57.8 | 65.1 |
| WOMEN (n=431) | |||
| OWD** | |||
|
Short (n=107) % |
Medium (n=217) % |
Long (n=107) % |
|
| Age ≥75 years | 22.4 | 44.7 | 64.5 |
| Parkinson's Disease | 0 | 2.30 | 1.87 |
| Ischemic heart disease | 3.7 | 13.8 | 9.3 |
| Cerebrovascular disease | 5.6 | 2.8 | 7.5 |
| Heart failure | 12.1 | 24.4 | 31.8 |
| Diabetes mellitus | 6.5 | 11.1 | 13.1 |
| Chronic obstructive pulmonary disease | 8.4 | 3.2 | 5.6 |
| Hip fracture | 4.7 | 1.8 | 2.8 |
| Hip arthritis | 23.4 | 16.1 | 21.5 |
| Knee arthritis | 41.1 | 34.1 | 39.2 |
| Depressed mood | 25.2 | 40.2 | 50.5 |
| Osteoporosis | 62.5 | 61.6 | 71.3 |
Short: OWD<2.39% of body height; Medium: OWD≥2.39% and <3.55% of body height; Long: OWD≥3.55% of body height.
Short: OWD<2.58% of body height; Medium: OWD≥2.58% and <3.90% of body height; Long: OWD≥3.90% of body height.
The upper panel of Figure 1 shows that there was no difference in bone density in the three groups.
Fig. 1. Distribution of bone mass density across OWD groups.
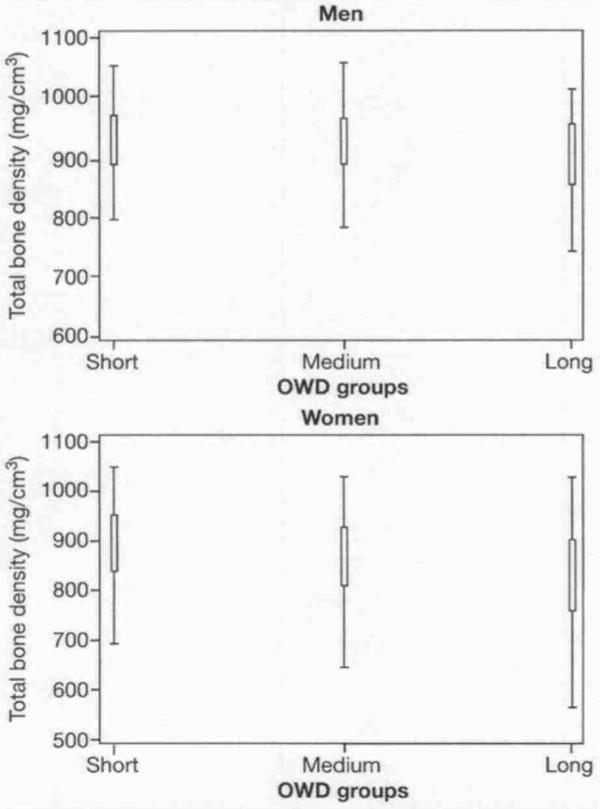
Table 2 (upper panel) shows mean performances in the three groups. Worse performances in balance, walking speed and overall performance were observed with increasing OWD, with no differences for the chair standing test. After correction for age and diagnosis of heart failure, ischemic heart disease and cerebro-vascular disease, only the association with reduced walking speed was confirmed (Table 3).
Table 2. Relationship between occiput-wall distance (OWD) groups and physical performance in men and women.
| MEN (n=352) | ||||
|---|---|---|---|---|
| OWD* | ||||
| Short (n=87) Mean (SD) |
Medium (n=175) Mean (SD) |
Long (n=90) Mean (SD) |
p | |
| Balance | 0.97 (0.11) | 0.95 (0.13) | 0.90 (0.21) | 0.009 |
| Chair standing test | 0.67 (0.15) | 0.66 (0.16) | 0.66 (0.20) | 0.790 |
| Walking speed | 0.77 (0.12) | 0.72 (0.14) | 0.66 (0.15) | <0.001 |
| Overall performance | 0.81 (0.08) | 0.78 (0.11) | 0.74 (0.16) | <0.001 |
| WOMEN (n=431) | ||||
| OWD | ||||
|
Short (n=107) Mean (SD) |
Medium (n=217) Mean (SD) |
Long (n=107) Mean (SD) |
p | |
| Balance | 0.96 (0.13) | 0.90 (0.18) | 0.77 (0.28) | <0.001 |
| Chair standing test | 0.60 (0.17) | 0.58 (0.19) | 0.51 (0.21) | 0.001 |
| Walking speed | 0.70 (0.12) | 0.61 (0.13) | 0.54 (0.18) | <0.001 |
| Overall performance | 0.75 (0.11) | 0.69 (0.14) | 0.61 (0.19) | <0.001 |
Short: OWD<2.39% of body height; Medium: OWD≥2.39% and <3.55% of body height; Long: OWD≥3.55% of body height.
Table 3. Analysis of covariance corrected for age, diagnosis of heart failure, ischemic heart disease, and cerebrovascular disease (men), and for age, diagnosis of heart failure, ischemic heart disease, depression, and bone density (women).
| MEN | ||
|---|---|---|
| F (df: 2) | p | |
| Balance | 0.8 | 0.449 |
| Chair standing | 1.74 | 0.176 |
| Walking speed | 6.00 | 0.003 |
| Overall performance | 0.95 | 0.387 |
| WOMEN | ||
| F (df: 2) | p | |
| Balance | 6.40 | 0.002 |
| Chair standing | 2.31 | 0.100 |
| Walking speed | 7.19 | <0.001 |
| Overall performance | 4.52 | 0.011 |
Women
Also in women, age was strongly associated with longer OWD. A linear association was also present with heart failure, whereas a non-linear association was evident for Parkinson's disease, ischemic heart disease, cerebro-vascular disease, and chronic obstructive pulmonary disease. The prevalence of knee arthritis decreased from 41.1% in women with short OWD to 29.2% in women with long OWD.
Figure 1 (lower panel) shows that bone density was lower in women with longer OWD. The analysis of variance confirmed this, with a statistically significant difference between the group with longer OWD compared with both groups with longer and medium OWD; there was no difference between the groups with short and medium OWD.
All performance measures showed a decline with increasing OWD, most evident for balance (mean score: 0,96 in short OWD group vs 0.77 in long OWD group, p<0.001) and walking speed (mean score: 0.70 in short OWD group vs 0.54 in long OWD group, p<0.001). Overall, the mean performance score decreased from 0.75 in short OWD group to 0.61 in long OWD group (p<0.001).
Corrections for age, heart failure, ischemic heart disease, depression, and bone density did not change the overall pattern, but variance in chair standing performance was not associated with OWD (Table 3).
Discussion
Using data from a large population-based sample of men and women, OWD was found to be associated with poor performance in tests of balance and gait. This association was stronger for women and was confirmed after correction for age and BMD. Thus, OWD is unlikely to qualify as a pure marker of osteoporosis.
Thoracic kyphosis, assessed using Cobb's angle, has been proved to be associated with poor physical fitness, osteoporosis, and the risk of falls (12, 13). However, measuring Cobb's angle requires radiologic equipment and therefore this measure is not easily performed. OWD cannot substitute for Cobb's angle because it does not directly measure the curvature of the spine at a given point, but quantifies the effect of altered curvature. Thus, OWD is unlikely to reflect kyphotic posture as accurately as Cobb's angle. Nevertheless, the well-recognized association with several measures of physical limitation confirmed here, makes OWD a valuable tool for epidemiological research.
The lower prevalence of functional impairment in men compared with women has been reported in other studies and has some biological plausibility (14). Greater muscle mass, testosterone and GH levels and the lesser propensity to dysregulation of the hypothalamic-adrenal axis and cortisol secretion may protect males from physical decline (15-19). A distinctive age-related change in the immune system probably makes men more vulnerable to infections and less prone to chronic conditions which are ultimately responsible for muscle loss (20, 21). Lastly, earlier mortality may eliminate men at greater risk of developing functional impairment (22).
In both men and women, walking speed and balance were found to be more severely compromised with higher OWD values. This relationship is probably explained by the biomechanical effects of changes in OWD: in particular, the kyphotic posture of the upper dorsal and cervical spine results in anterior displacement of the center of gravity, and is followed by compensatory widening of the base of support and lumbar hyperlordosis (23, 24). This adaptive strategy leads to the balance impairment shown in our study, and probably involves a consequent increase in the risk of falls. Changes in postural control may also account for reduced walking speed, since the cautious “small steps” gait characterized by reduced step length is an obvious response to postural instability (1). As both balance impairment and reduced walking speed are recognized risk factors for falls and hip fractures (25, 26), systematic measures of OWD may help to identify subjects at risk of falls, although this hypothesis needs to be evaluated prospectively.
The limitations of this study deserve consideration. First, because of its cross-sectional design, associations between different variables could be tested, but no cause-effect relationship could be verified. Prospective studies are needed to clarify whether OWD is causally related to some of the identified correlates. Second, we were unable to explain fully the causal pathway relating kyphosis with impaired performance in women but not in men. However, our finding strongly supports the hypothesis that OWD is a good screening tool for early detection of physical impairment and perhaps frailty in non-disabled older people. Third, our study population was on average in good health. It is probable that some of the observed relationships would be stronger even in males belonging to a less healthy population.
Conclusions
Our findings indicate that OWD is a potential marker of overall reduced physical function in women but not in men. To better define the rationale for its use in the clinical setting, further research should verify whether OWD increases in parallel with the development of frailty or whether it can predict incident frailty.
References
- 1.Tribus CB. Scheuermann's kyphosis in adolescents and adults: diagnosis and management. J Am Acad Orthop Surg. 1998;6:36–43. doi: 10.5435/00124635-199801000-00004. [DOI] [PubMed] [Google Scholar]
- 2.Balzini L, Vannucchi L, Benvenuti F, et al. Clinical characteristics of flexed posture in elderly women. J Am Geriatr Soc. 2003;51:1419–26. doi: 10.1046/j.1532-5415.2003.51460.x. [DOI] [PubMed] [Google Scholar]
- 3.Di Bari M, Chiarlone M, Matteuzzi D, et al. Thoracic kyphosis and ventilatory dysfunction in unselected older persons: an epidemiological study in Dicomano, Italy. J Am Geriatr Soc. 2004;52:909–15. doi: 10.1111/j.1532-5415.2004.52257.x. [DOI] [PubMed] [Google Scholar]
- 4.Kado DM, Huang MH, Barrett-Connor E, Greendale GA. Hyperkyphotic posture and poor physical functional ability in older community-dwelling men and women: the Rancho Bernardo study. J Gerontol. 2005;60:633–7. doi: 10.1093/gerona/60.5.633. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 5.Ryan SD, Fried LP. The impact of kyphosis on daily functioning. J Am Geriatr Soc. 1997;45:1479–86. doi: 10.1111/j.1532-5415.1997.tb03199.x. [DOI] [PubMed] [Google Scholar]
- 6.Guralnik JM, Ferrucci L, Pieper CF, et al. Lower extremity function and subsequent disability: consistency across studies, predictive models, and value of gait speed alone compared with the short physical performance battery. J Gerontol. 2000;55:M221–31. doi: 10.1093/gerona/55.4.m221. [DOI] [PubMed] [Google Scholar]
- 7.Guralnik JM, Ferrucci L, Simonsick EM, Salive ME, Wallace RB. Lower-extremity function in persons over the age of 70 years as a predictor of subsequent disability. N Engl J Med. 1995;332:556–62. doi: 10.1056/NEJM199503023320902. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 8.Onder G, Penninx BWJH, Lapuerta P, et al. Change in physical performance over time in older women: the Women's Health and Aging Study. J Gerontol. 2002;57:M289–93. doi: 10.1093/gerona/57.5.m289. [DOI] [PubMed] [Google Scholar]
- 9.Radloff LS. The CES-D scale: a self-report depression scale for research in the general population. Appl Psychol Meas. 1977;1:385–401. [Google Scholar]
- 10.Parikh RM, Eden DT, Price TR, Robinson RG. The sensitivity and specificity of the Center for Epidemiologic Studies Depression Scale in screening for post-stroke depression. Int J Psychiatry Med. 1988;18:169–81. doi: 10.2190/bh75-euya-4fm1-j7qa. [DOI] [PubMed] [Google Scholar]
- 11.Louis O, Boulpaep F, Willnecker J, Van den Winkel P, Osteaux M. Cortical mineral content of the radius assessed by peripheral QCT predicts compressive strength on biomechanical testing. Bone. 1995;16:375–9. doi: 10.1016/8756-3282(94)00050-6. [DOI] [PubMed] [Google Scholar]
- 12.Chow RK, Harrison JE. Relationship of kyphosis to physical fitness and bone mass in post-menopausal women. Am J Phys Med. 1987;66:219–27. [PubMed] [Google Scholar]
- 13.Sinaki M, Brey RH, Hughes CA, Larson DR, Kaufman KR. Balance disorder and increased risk of falls in osteoporosis and kyphosis: significance of kyphotic posture and muscle strength. Osteoporos Int. 2005;16:1004–10. doi: 10.1007/s00198-004-1791-2. [DOI] [PubMed] [Google Scholar]
- 14.Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol. 2001;56:M146–56. doi: 10.1093/gerona/56.3.m146. [DOI] [PubMed] [Google Scholar]
- 15.Metter EJ, Conwit R, Tobin J, Fozard JL. Age-associated loss of power and strength in the upper extremities in women and men. J Gerontol. 1997;52:B267–76. doi: 10.1093/gerona/52a.5.b267. [DOI] [PubMed] [Google Scholar]
- 16.Phillips SK, Rook KM, Siddle NC, Bruce SA, Woledge RC. Muscle weakness in women occurs at an earlier age than in men, but strength is preserved by hormone replacement therapy. Clin Sci (Lond) 1993;84:95–8. doi: 10.1042/cs0840095. [DOI] [PubMed] [Google Scholar]
- 17.Lamberts SW, van den Beld AW, van der Lely AJ. The endocrinology of aging. Science. 1997;278:419–24. doi: 10.1126/science.278.5337.419. [DOI] [PubMed] [Google Scholar]
- 18.O'Connor KG, Tobin JD, Harman SM, et al. Serum levels of insulin-like growth factor-I are related to age and not to body composition in healthy women and men. J Gerontol. 1998;53:M176–82. doi: 10.1093/gerona/53a.3.m176. [DOI] [PubMed] [Google Scholar]
- 19.Van Cauter E, Leproult R, Kupfer DJ. Effects of gender and age on the levels and circadian rhythmicity of plasma cortisol. J Clin Endocrinol Metab. 1996;81:2468–73. doi: 10.1210/jcem.81.7.8675562. [DOI] [PubMed] [Google Scholar]
- 20.Albrecht AE, Hartmann BW, Scholten C, Huber JC, Kalinowska W, Zielinski CC. Effect of estrogen replacement therapy on natural killer cell activity in postmenopausal women. Maturitas. 1996;25:217–22. doi: 10.1016/s0378-5122(96)01063-8. [DOI] [PubMed] [Google Scholar]
- 21.Kanda N, Tsuchida T, Tamaki K. Testosterone inhibits immunoglobulin production by human peripheral blood mononuclear cells. Clin Exp Immunol. 1996;106:410–5. doi: 10.1046/j.1365-2249.1996.d01-842.x. [DOI] [PMC free article] [PubMed] [Google Scholar]
- 22.Hazzard WR. The gender differential in longevity. In: Hazzard WR, Bierman EL, Blass JP, Ettinger WHJ, Halter JB, editors. Principles of Geriatric Medicine and Gerontology. New York, NY: McGraw-Hill; 1994. pp. 37–47. [Google Scholar]
- 23.Lynn SG, Sinaki M, Westerlind KC. Balance characteristics of persons with osteoporosis. Arch Phys Med Rehabil. 1997;78:273–7. doi: 10.1016/s0003-9993(97)90033-2. [DOI] [PubMed] [Google Scholar]
- 24.O'Brien K, Culham E, Pickles B. Balance and skeletal alignment in a group of elderly female fallers and nonfallers. J Gerontol. 1997;52:B221–6. doi: 10.1093/gerona/52a.4.b221. [DOI] [PubMed] [Google Scholar]
- 25.Tinetti ME. Preventing falls in elderly persons. N Engl J Med. 2003;348:42–9. doi: 10.1056/NEJMcp020719. [DOI] [PubMed] [Google Scholar]
- 26.de Rekeneire N, Visser M, Peila R, et al. Is a fall just a fall: correlates of falling in healthy older persons, the health, aging and body composition study. J Am Geriatr Soc. 2003;51:841–6. doi: 10.1046/j.1365-2389.2003.51267.x. [DOI] [PubMed] [Google Scholar]