

Abstract
Purpose
The purpose of this study was to compare the biomechanical stability generated when utilizing increasing sizes of titanium (Ti) flexible nails for fixation of simulated comminuted femur fractures.
Methods
Five synthetic adolescent-sized femur models were reamed to create a 9-mm canal. A 2-cm section was removed in the mid-diaphysis to simulate comminution. Each femur was first stabilized with bilateral, retrograde 3.0-mm titanium elastic nails. Femurs were tested in axial rotation and axial compression. The constructs were removed, and femurs were re-nailed with 3.5-mm nails. Identical testing was conducted. These nails were then removed, and femurs were re-nailed with 4.0-mm nails. This provided data on “canal fill” representing 67, 78 and 89% of the reamed canal diameter. Data for axial rotation (degrees) and failure load (N) required to produce 5 mm of fracture shortening were analyzed with a one-way ANOVA (P < 0.05) and a Tukey’s post-hoc test for multiple comparisons.
Results
For axial rotation, there were statistically significant improvements in rotational control for each increase in nail size. For axial stability, each increase in nail size resulted in increased axial failure loads to 5 mm, although these data were not statistically different. A specific comparison between 3.0- and 3.5-mm nails for compressive stability found significantly greater stability afforded by using 3.5-mm nails.
Conclusions
Data from this study demonstrate that increasing the amount of canal fill provides significant improvements in rotational control. The largest improvement was seen when increasing from 3.0- to 3.5-mm nails. While increasing the nail size from 3.5 to 4.0 mm again provided greater stability, larger nails may be more difficult to insert. Thus, increasing the nail size for femoral fracture fixation should be considered after measuring the diameter of the canal and evaluating the potential difficulty of insertion as well as specific demands of the fracture pattern.
Keywords: Simulated femur fracture, Comminution, Titanium, Increasing nail diameter, Percent canal fill
Introduction
The treating orthopedic surgeon has many options available for the treatment of pediatric femur fractures [1–15]. Over the last 10 years the use of flexible intramedullary nails has dramatically increased [1, 3–11, 13, 15, 16]. The benefits of flexible intramedullary nails include excellent fracture union rates and early fracture stabilization, allowing a short hospital stay and minimal postoperative bracing. The antegrade approach holds reduced risk of femoral head osteonecrosis and proximal femoral physeal damage, while the retrograde approach avoids both of these sequelae of rigid intramedullary nails [12, 14, 15, 17]. The technique is relatively simple and requires minimal surgical exposure.
Most complications of flexible intramedullary nailing are minor and include leg length inequality (<2 cm), malalignment and nail site irritation. Recently, authors have defined complications and technical points for the surgeon to consider lessening the incidence of these minor but troublesome complications. Several investigators have recommended using the largest nail diameter possible; however, the larger the nail, the more difficult it is to contour and insert. The recommended use of two flexible nails each with a diameter, i.e., 40% of the medullary canal diameter will yield a “canal fill” of 80% [4, 9, 10]. A recent study found that an 80% canal fill improved the overall biomechanical stability of the fractured femur, but often resulted in malreduction with posterior gapping [18]. These authors advocated the potential use of multiple smaller nails (i.e., 2 mm) to achieve the dimension of a single larger rod (4 mm). However, the use of more than two nails, some of which may be dimensionally asymmetric, is not recommended by the manufacturer and has not gained clinical acceptance [18].
While both stainless steel [11] and titanium [6, 9] nails have gained clinical acceptance, titanium has demonstrated improved biomechanical stability compared to stainless steel [19]. A recent report of 230 femur fractures treated with titanium elastic nails found poor outcomes in 10% of cases, with unacceptable angulation and fracture shortening representing the most common failures [16]. Titanium nails of different sizes were used at surgeon discretion. In that study, poor outcomes were significantly correlated to older children (>11 years old) and larger children (>49 kg). With larger children, it would be intuitively desirable to maximize the diameter of the nails used to achieve optimal fracture fixation. Thus, the purpose of this study was to compare the biomechanical performance of different diameter titanium flexible intramedullary nails in stabilizing femoral fractures loaded in torsion and axial compression.
Methods
Five adolescent-sized (38-cm length) two-part composite synthetic femora (polyurethane foam core with glass-filled epoxy shell) (Pacific Research Laboratories, Vashon, WA) were used for the biomechanical testing. A reamer was used to create a 9-mm canal diameter in each femur. Each femur was then placed in a custom cutting rig to cut and remove an identical 2-cm section from the central diaphysis. This defect was created in order to simulate comminution in an unstable fracture. Titanium nail diameters of 3.0, 3.5 and 4.0 mm (Synthes, Paoli, PA) were cut and precontoured into matching “C” patterns. The femora were stabilized utilizing retrograde insertion of flexible nails with entry points 2 cm proximal to the metaphyseal flare. The five femoral models were first stabilized with two 3.0-mm titanium (Ti) flexible nails. This size represents a canal fill of 67%. Once stabilized, the femora underwent testing in conditions of torsion and axial compression. Each specimen was placed into a form-fit epoxy mold for testing with an servohydraulic MTS 858 Mini-Bionix machine (MTS, Co., Eden Prairie, MN). For both torsion and compressive testing the specimens were tested along their mechanical axis running through the center of the femoral head to the midpoint between the femoral condyles (Fig. 1). For torsional testing, cyclic torques between ±2 Nm were applied at 0.5° per second over five cycles while maintaining 20N of compressive load to simulate passive muscle tension. For compression testing, a single test ramped to 5 mm of displacement (fracture gap shortening) was performed at 0.5 mm per second. Angle (°), torque (Nm), displacement (mm) and force (N) were recorded at 10 Hz during each test. The range of motion (degrees) was calculated during torsion tests, and the force values (N) required for shortening of 5 mm of compression were calculated. The 3.0-mm nails were then removed and replaced with 3.5-mm nails. Fracture reduction was again accomplished on the benchtop and a section of the previously resected mid-diaphysis placed at the level of the comminution to ensure an identical fracture pattern. Following fixation, this piece was removed. Identical testing was conducted using the bilateral 3.5-mm nails representing a canal fill of 78%. After this round of testing, nails were again removed and upsized to the 4.0-mm nails (using identical fracture reduction techniques). The bilateral 4.0-mm nails represent a canal fill of 89%. Data for range of motion (degrees) and load to 5-mm compression (N) were compared between groups using a one-way ANOVA (P < 0.05) and a Tukey’s post-hoc test for multiple comparisons.
Fig. 1.
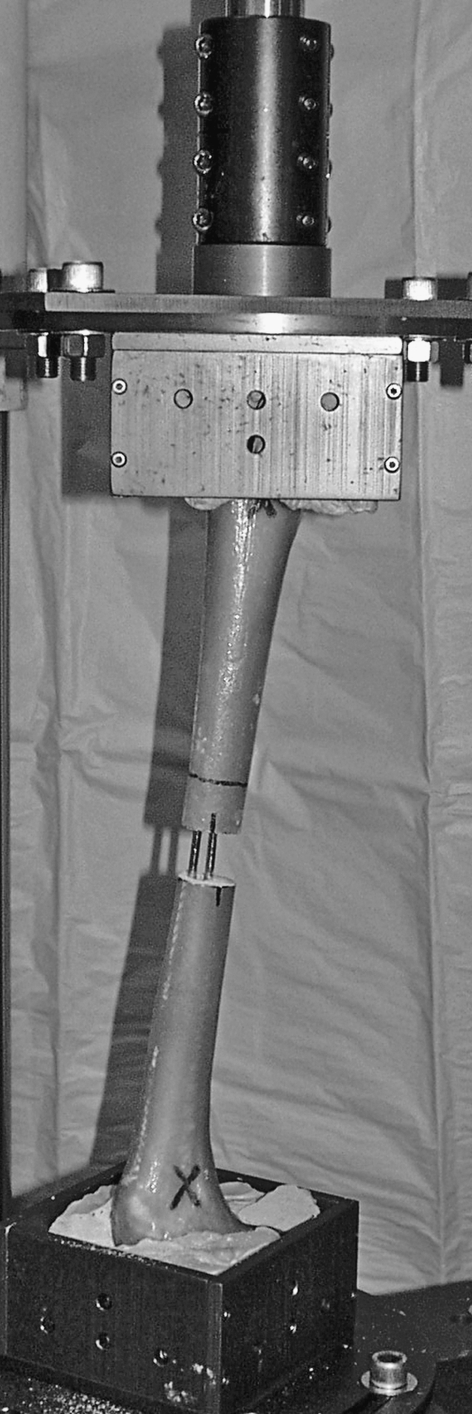
Mechanical test setup for torsion and compression testing
Results
Torsion
The stability provided by using increasing nail sizes was found to be statistically greater as larger nails were used (P < 0.0002). The 3.0-mm nails provided little support as the torsional range of motion was 163° ± 5°. The largest jump in increased stability (72%) was seen when moving to 3.5-mm nails (46° ± 6°), and this was statistically significant (P < 0.002). Moving to 4.0-mm nails (21° ± 4°) demonstrated significantly increased rotational stability (P < 0.002) compared to 3.5-mm nails, although this improvement was not quite as large (54%) (Fig. 2).
Fig. 2.

Range of motion during torsion testing between ±2 Nm
Axial compression
The loads required to create 5 mm of fracture gap shortening were found to approach significance (P = 0.06) across each nail diameter. The 3.0-mm nails were found to have the lowest load (103 ± 55 N). Using 3.5-mm nails improved the axial compressive stability by 156% (265 ± 91 N). Moving to 4.0-mm nails (305 ± 189 N) only generated a modest improvement in axial compressive stability (14%). Upon review of these data, a specific t test comparison was made between the 3.0- and 3.5-mm nail construct data, which found a statistically significant improvement in axial compressive stability when using 3.5-mm nails (P < 0.01) (Fig. 3).
Fig. 3.

Axial forces during compression testing at 5-mm shortening
Discussion
In the treatment of pediatric femoral shaft fractures, flexible intramedullary nails provide an internal splint that allows early mobilization with minimal surgical dissection and minimal risk to the growth plates or femoral head blood supply. The general guidelines for nail selection are based upon anecdotal evidence. Several authors describe using two nails with a combined diameter that is 80% of the intramedullary canal at its narrowest width [4, 10]. However, smaller nails are easier to place than larger nails. Therefore, the goal of this study was to evaluate the validity of using increasing nail sizes as a clinical guideline in instrumentation selection by testing constructs that “bound” 80%. Using a synthetic femur model, three different two-nail constructs were tested: titanium nails of 3.0-, 3.5- and 4.0-mm diameter. Data indicate that when increasing the canal fill from 67% (3.0 mm) to 78% (3.5 mm), increases in biomechanical stability are seen in axial rotation and in axial compressive stability. Moving to the maximum nail size of 89% (4.0 mm) only improved the rotation stability.
Inadequate stabilization can result in limb shortening, a described complication of flexible intramedullary nails. In previous prospective evaluations, the investigators found that 10–15% of fractures stabilized by flexible nails were at least 5 mm shorter than the other limb after fracture healing [4, 6]. None of these investigators described a correlation between nail size and limb shortening. However, in their retrospective evaluation of pediatric femoral fractures treated with titanium elastic nails, Luhmann et al. [10] and coworkers describe a case of hypertrophic non-union in which undersized nails (2.0 mm) were used. The non-union resolved within 8 weeks of exchanging these 2.0-mm nails for larger 3.5-mm nails [10]. These clinical reports support the findings of the present study that approaching 80% of canal fill results in greater stability during biomechanical testing.
In addition to limb shortening, an inadequate sized nail may back out and can cause irritation at the nail insertion site. Insertion site pain and prominence were some of the most common minor complications cited in clinical studies. The incidence of nail site morbidity ranged from 7 to 65% with a few patients having nail erosion through the skin or even deep wound infection [4, 9, 10]. Although some of these cases are a result of leaving too much implant length outside of the bone intraoperatively, a significant portion of these nail problems may result from failure under compressive loading leading to nail back out. Thus, using a larger nail diameter and achieving ~80% canal fill as described in this biomechanical study may lessen the chance of back out and resulting nail prominence.
Another complication described in clinical studies is angulation at the fracture site. In their study of 123 fractures treated by flexible intramedullary nailing, Ligier et al. [9] reported 14 fractures (11%) had angulation at the fracture site that ranged from 5° to 10°. In a study of 78 femoral fractures fixed by Ender nails, Heinrich et al. [6] stated that 11% had at least 5° of coronal angulation and 8% had at least 5° of sagittal angulation at the fracture site at the time of healing. Flynn et al. [4] reported that 6 of their 58 fractures fixed with titanium elastic nails had more than 5° of angulation. In the Luhmann et al. [10] study of 43 fractures treated with flexible titanium nail fixation, coronal and sagittal angulation averaged 4.7° and 4.2°, respectively. The authors found a significant negative correlation between coronal angulation and nail size and a trend toward a correlation between increasing sagittal angulation and decreasing nail size [10]. These clinical findings support the findings of the current study in that increasing nail sizes should provide greater biomechanical stability. Maximizing nail size may also be desirable in older, larger children, which may reduce the poor outcomes (10%) of unacceptable angulation and fracture shortening reported in a series of 230 femur fractures [16].
Titanium nails have gained increasing popularity in the past 10 years. Since the early 1980s, French surgeons have pioneered the use of titanium elastic nails asserting that stainless steel nails are “not elastic enough for treating children” [9]. A recent biomechanical analysis by Mahar et al. [19] compared fracture fixation with 3.5-mm stainless steel nails and 3.5-mm titanium nails in a divergent “C” configuration in an adolescent femur model. The titanium constructs had significantly greater rotational stability and compression stiffness than the stainless steel constructs. The authors theorized that the more flexible titanium nails were able to conform to the medullary canal walls and attain more nail/bone contact, thus providing more resistance to motion, especially compression. Conversely, the less flexible stainless steel nails do not conform as well once in the medullary canal. Therefore, stainless steel constructs rely upon the surgeon “prebending” them to get as much medullary canal wall contact as possible; however, this prebend may be lost during nail insertion [19].
Further clinical evaluation should be conducted to answer questions about intraoperative issues and treatment outcomes; however, the current study yields important information about the biomechanical qualities of flexible nail constructs of varying nail diameters. Using an adolescent femur model with a 9-mm canal, the benefit of increasing the nail diameter from 3.0 mm (67% canal fill) to 3.5 mm (78% canal fill) to 4.0 mm (89% canal fill) was significant. The increase in nail size from 3.0 to 3.5 mm provided the greatest improvements in fracture stabilization for both axial torsion and axial compression. The 4.0-mm nails did improve stability compared to 3.5-mm nails. The improvement in stabilization from 3.5- to 4.0-mm nails must be balanced between the ease of insertion (and reduced risk for extension of the fracture). The differences in biomechanical stability across nail sizes also reinforce the importance of proper canal diameter measurement by the surgeon prior to nail size selection.
With regards to some of the limitations of the study, the use of synthetic femur models may be of concern. The synthetic models have reported mechanical properties similar to that of human bone [20, 21]. It was thus hoped the bone–implant interaction would be similar, although there would be no effects related to blood, marrow or other fluids. Also, these models provide inherently similar “specimens” with which to assess varying fixation constructs. In addition, the loading the femur experiences between the knee and hip are extremely complex, and the current methods were an attempt to use simplified yet physiological mechanical inputs. Finally, the femurs were sequentially nailed with increasing nail diameters. The material composition certainly would not degrade with sequential testing although nail insertion may remove part of the synthetic medullary wall. This minimal loss of material was not considered to have a biomechanical effect on the fixation constructs. It was felt that, by increasing nail diameter, the fixation would be less susceptible to loosening than if smaller nails were inserted following the larger nails.
Data from this study demonstrates a combined nail diameter of ~80% of the canal diameter led to the greatest increases in biomechanical stability for both axial torsion and axial compression. The largest improvement was seen when increasing from 3.0- to 3.5-mm nails. While increasing the nail size from 3.5 to 4.0 mm again provided greater stability, larger nails may be more difficult to contour and insert. Thus, increasing the nail size for femoral fracture fixation could be considered after measuring the diameter of the canal and evaluating the potential difficulty of insertion as well as specific demands of the fracture pattern.
Acknowledgments
This research was funded by a restricted research grant from the Denver Children’s Hospital Orthopedic Education and Research Fund. None of the authors received financial support for this study.
References
- 1.Bar-On E, Sagiv S, Porat S (1997) External fixation or flexible intramedullary nailing for femoral shaft fractures in children. A prospective, randomised study. J Bone Joint Surg Br 79:975–978 [DOI] [PubMed]
- 2.Caird MS, Mueller KA, Puryear A, Farley FA (2003) Compression plating of pediatric femoral shaft fractures. J Pediatr Orthop 23:448–452 [DOI] [PubMed]
- 3.Carey TP, Galpin RD (1996) Flexible intramedullary nail fixation of pediatric femoral fractures. Clin Orthop 332:110–118 [DOI] [PubMed]
- 4.Flynn JM, Hresko T, Reynolds RA, Blasier RD, Davidson R, Kasser J (2001) Titanium elastic nails for pediatric femur fractures: a multicenter study of early results with analysis of complications. J Pediatr Orthop 21:4–8 [DOI] [PubMed]
- 5.Gregory P, Sullivan JA, Herndon WA (1995) Adolescent femoral shaft fractures: rigid versus flexible nails. Orthopedics 18:645–649 [DOI] [PubMed]
- 6.Heinrich SD, Drvaric DM, Darr K, MacEwen GD(1994) The operative stabilization of pediatric diaphyseal femur fractures with flexible intramedullary nails: a prospective analysis. J Pediatr Orthop 14:501–507 [DOI] [PubMed]
- 7.Huber RI, Keller HW, Huber PM, Rehm KE (1996) Flexible intramedullary nailing as fracture treatment in children. J Pediatr Orthop 16:602–605 [DOI] [PubMed]
- 8.Kissel EU, Miller ME (1989) Closed Ender nailing of femur fractures in older children. J Trauma 29:1585–1588 [DOI] [PubMed]
- 9.Ligier JN, Metaizeau JP, Prevot J, Lascombes P (1988) Elastic stable intramedullary nailing of femoral shaft fractures in children. J Bone Joint Surg B 70:74–77 [DOI] [PubMed]
- 10.Luhmann SJ, Schootman M, Schoenecker PL, Dobbs MB, Gordon JE (2003) Complications of titanium elastic nails for pediatric femoral shaft fractures. J Pediatr Orthop 23:443–447 [DOI] [PubMed]
- 11.Mann DC, Weddington J, Davenport K (1986) Closed Ender nailing of femoral shaft fractures in adolescents. J Pediatr Orthop 6:651–655 [DOI] [PubMed]
- 12.O’Malley DE, Mazur JM, Cummings RJ (1995) Femoral head avascular necrosis associated with intramedullary nailing in an adolescent. J Pediatr Orthop 15:21–23 [DOI] [PubMed]
- 13.Ozdemir HM, Yensel U, Senaran H, Mutlu M, Kutlu A (2003) Immediate percutaneous intramedullary fixation and functional bracing for the treatment of pediatric femoral shaft fracture. J Pediatr Orthop 23:453–457 [DOI] [PubMed]
- 14.Raney EM, Ogden JA, Grogan DP (1993) Premature greater trochanteric epiphysiodesis secondary to intramedullary femoral rodding. J Pediatr Orthop 13:516–520 [DOI] [PubMed]
- 15.Stans AA, Morrissy RT, Renwick SE (1999) Femoral shaft fracture treatment in patients age 6 to 16 years. J Pediatr Orthop 19:222–228 [DOI] [PubMed]
- 16.Moroz LA, Launay F, Kocher MS, Newton PO, Frick SL, Sponseller PD, Flynn JM (2006) Titanium elastic nailing of fractures of the femur in children. Predictors of complications and poor outcome. J Bone Joint Surg Br 88:1361–1366 [DOI] [PubMed]
- 17.Gonzalez-Herranz P, Burgos-Flores J, Rapariz JM, Lopez-Mondejar JA, Ocete JG, Amaya S (1995) Intramedullary nailing of the femur in children. Effects on its proximal end. J Bone Joint Surg Br 77:262–266 [PubMed]
- 18.Green JK, Werner FW, Dhawan R, Evans PJ, Kelley S, Webster DA (2005) A biomechanical study on flexible intramedullary nails used to treat pediatric femoral fractures. J Orthop Res 23:1315–1320 [DOI] [PubMed]
- 19.Mahar AT, Lee SS, Lalonde FD, Impelluso T, Newton PO (2004) Biomechanical comparison of stainless steel and titanium nails for fixation of simulated femoral fractures. J Pediatr Orthop 24:638–641 [DOI] [PubMed]
- 20.Cristofolini L, Viceconti M, Cappello A, Toni A (1996) Mechanical validation of whole bone composite femur models. J Biomech 29:525–535 [DOI] [PubMed]
- 21.Heiner A, Brown T (2001) Structural properties of a new design of composite replicate femurs and tibias. J Biomech 34:777–781 [DOI] [PubMed]