

Abstract
Purpose
The ligamentum teres has primarily been considered as an obstruction to reduction in children with developmental dislocation of the hip (DDH). In the early surgical descriptions of both the medial (Ludloff) approach and the anterior (Salter) approach to the hip, it was generally accepted that the ligamentum teres was an obstruction to reduction and was excised (similar to the discarding of menisci for knee surgery in our orthopedic history). Because of the known propensity for early re-dislocation following open reduction, we developed surgical methods for maintaining the ligamentum teres when performing open reduction for hip dislocation in young children. This study presents the surgical methods developed for ligament maintenance and transfer, and analyzes the early clinical and radiographic results in a study group.
Methods
The techniques for open reduction by both the medial Ludloff approach and the anterior open reduction were developed and refined. Twenty-one children (23 hips) had ligamentum teres shortening and transfer performed as part of either a medial Ludloff or anterior open reduction for hip dislocation. Complete pre-operative and post-operative clinical and radiographic analysis was performed.
Results
All patients had stable hips at follow-up. The transferred ligamentum teres appeared to provide additional stability to prevent repeat dislocation. We noted no apparent loss of hip motion or other adverse events. One patient had avascular necrosis (AVN).
Conclusions
In this series of 23 hips, in which ligamentum teres transfer/tenodesis was utilized, we found no residual subluxation or dislocation in either the medial Ludloff or the anterior open reduction groups. Based on these early positive results, we recommend the method for children treated with the Ludloff open reduction procedure. Although we have less experience with it, the technique presented for ligamentum maintenance and transfer in anterior open reduction may provide similar added stability. This is an early follow-up study, and long-term follow-up will be required to confirm the ultimate femoral head and acetabular development.
Keywords: Developmental dysplasia of the hip, Ligamentum teres, Avoiding re-dislocation, Open reduction, Surgical technique
Introduction
The ligamentum teres, also known as the ligamentum capitis femoris, has been well-characterized in normal and pathologic hips [1–5]. The ligament has a broad-based origin from the cotyloid notch of the acetabulum and the transverse acetabular ligament, with a distinct insertion into the fovea of the femoral head.
Despite numerous studies of the anatomy and histology of the ligamentum teres, its role in hip stability remains poorly understood [4, 5]. Previous animal studies have documented a lower rate of hip dislocation with an intact ligamentum teres [6, 7]. In addition, a recent biomechanical animal study by Wenger et al. [8] demonstrated the strength of the ligamentum teres, clarifying its mechanical characteristics and strength similar to the anterior cruciate ligament of the knee (Fig. 1). Although the exact role of this ligament in pediatric hip instability remains unknown, these findings suggest that it may be an important stabilizer.
Fig. 1.
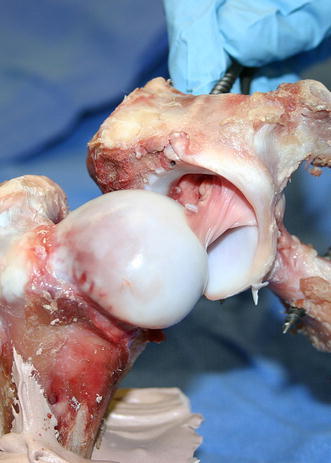
Lateral view of a right hip porcine model used for biomechanical testing. The size, strength, and orientation of fibers in this model is similar to that noted in the infant human and suggests a functional role
In developmental dysplasia of the hip (DDH), the ligamentum teres has primarily been considered to be a potential obstruction to reduction. Numerous authors have described excision of the ligamentum teres as a part of open hip reduction in DDH [9–11]. This may parallel past thinking in meniscal surgery—the “problem” tissue was discarded. Weinstein and Ponseti [11] have demonstrated that the ligamentum teres in DDH is longer and thicker than normal, and can, indeed, serve as an obstruction to reduction, particularly with a medial Ludloff-type approach [3]. Excision of the ligamentum teres has also been described during open reduction (combined with femoral and acetabular osteotomy) for hip dislocations in cerebral palsy (CP) and myelomeningocele [12].
Even with modern surgical techniques, residual instability and re-dislocation after open hip reduction remains a problem in DDH patients who have reduction by a medial (Ludloff) approach or by anterior open reduction with capsulorrhaphy [13–16]. A review of the literature by Tonnis [17] reported that a failure to obtain a stable concentric reduction after open operation occurred in 5–14% of medial approaches and approximately 3% of procedures performed through an anterior approach. Residual subluxation and repeat dislocation also remain problematic after open reduction in CP [18].
Noting the frequency of re-dislocation following open reduction, even in the hands of experienced surgeons, we began to consider the ligamentum teres as an additional stabilizer. After studying the size and strength of the ligamentum teres [8], we initiated a clinical series in which the ligamentum teres was left attached to the femoral head, shortened, and then re-attached (on the acetabular side) as part of the hip reconstruction.
We first maintained and transferred the ligament during medial (Ludloff) open reduction for DDH, where retention of the ligament is easiest [11, 19]. After noting greatly improved stability of reduction in these cases, we then developed techniques to maintain the ligament in anterior open reduction.
The purpose of this paper is to present surgical techniques for ligamentum teres maintenance and transfer as part of the surgical treatment for childhood hip dislocation. The early results of a patient series are also described.
Materials and methods
Inclusion criteria for this retrospective study included all children who underwent open reduction plus ligamentum teres transfer for a dislocated hip in our institution from 1999 to 2007.
The 21 children (23 hips) were classified according to the underlying cause of their hip instability and their medical records were referenced to ascertain birth history, risk factors, management prior to open reduction, operative findings, early postoperative complications, and the need for additional procedures. Clinical parameters recorded at the latest follow-up included pain in the affected hip, the presence or absence of a limp, and range of motion.
Radiographic evaluation included pre-operative and post-operative anterior-posterior (AP) and frog-lateral pelvis radiographs evaluated for post-operative subluxation, dislocation, and avascular necrosis (AVN). AVN was classified according to the method of Bucholz and Ogden [20].
Additional radiographic parameters measured were based on the patient’s underlying disease and age. The post-operative center–edge angle (CEA), as described by Wiberg [21], was measured in all patients who were at least 5 years of age at the latest follow-up. For patients with DDH, the pre-operative severity of dislocation was graded according to Tonnis [17], and the pre- and post-operative acetabular index were measured. In addition, the post-operative superior and lateral centering ratios were assessed according to the method of Smith et al. [22]. The Smith centering ratios indicate the position of the femoral head within the acetabulum, and can be used in infants and young children, whose skeletal immaturity precludes accurate measurement of the center–edge angle.
For patients with hip dislocation or subluxation due to spasticity or spina bifida, the post-operative migration percentage at the latest follow-up was measured according to Reimers [23]. Radiographic post-operative subluxation was determined for any case in which 33% of the femoral head remained lateral to the acetabulum on an AP pelvis radiograph, as defined by both Reimers [23] and Sharrard et al. [24].
Surgical technique
The surgical technique utilized in this series fell into two categories, based on the underlying pathology and age:
Medial open reduction with ligamentum teres transfer used in children under 24 months of age with dislocation due to DDH who had failed Pavlik harness treatment or closed reduction
- Ligamentum teres transfer combined with traditional anterior open reduction (plus associated procedures) utilized for:
- DDH dislocations in older children
- Dislocations due to spasticity or myelomeningocele
Medial open reduction with ligamentum teres transfer
We first utilized ligamentum teres transfer as part of the medial Ludloff-type open reduction for DDH [25]. We use a medial approach similar to that described by Mau et al. [19], which has been modified and popularized by Weinstein and Ponseti [11].
Through a careful medial approach, the psoas tendon is sectioned or lengthened intramuscularly. The capsule is then opened in a T-fashion, and the ligamentum teres is identified (Fig. 2a). The capsule may need to be opened slightly more superiorly and laterally to be certain that the ligamentum teres can be pulled into the wound, using a right-angle hemostat. The femoral head insertion of the ligamentum teres is left intact (in contrast to prior descriptions, in which it is excised). The ligament is then released from its origin on the cotyloid fossa and transverse acetabular ligament, and is tagged with a suture.
Fig. 2.
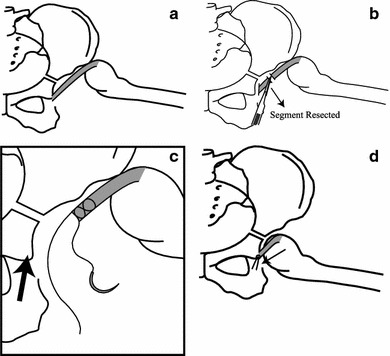
Sequence of drawings demonstrating the technique for ligamentum teres shortening and reattachment when performing the medial Ludloff open reduction. a Left femoral head in the dislocated position with elongated ligamentum teres. b Ligamentum teres detached from its origin from the inferior acetabulum, with a segment resected to normalize the ligamentum teres length (approximately 1 cm resected). c Non-absorbable suture placed in the ligamentum teres (Bunnell type suture pattern). The arrow indicates the planned ligament re-attachment site. d Shortened ligamentum teres sutured into the anterior-inferior acetabular rim
The transverse acetabular ligament is sectioned, with any redundant acetabular fat (pulvinar) removed from the base of the acetabulum. The ligamentum teres is then grasped with a Kocher clamp and is used as a tether to pull the displaced femoral head down over the labrum into a reduced position, which is confirmed with the image intensifier.
At this point, the ligamentum teres is found to be about 1–1.5 cm too long, depending on the severity of the hip dislocation. The most medial portion of the ligamentum teres is excised (Fig. 2b). A non-absorbable #1–0 suture is woven Bunnell style into the medial end of the shortened ligament (Fig. 2c) and is then firmly sutured into the periosteum at the anterior origin of the transverse acetabular ligament (Fig. 2d). The suture is tied with the hip in the typical post-Ludloff position (flexed above 90°, abducted approximately 50°). An additional capsular suture or two can be placed, although the Ludloff approach does not allow formal capsulorrhaphy.
Of note, the additional surgical time needed in order to perform ligament shortening and transfer is approximately 5–10 min. Post-operative casting and management are identical to that used for medial open reduction without ligamentum teres transfer (Fig. 3).
Fig. 3.
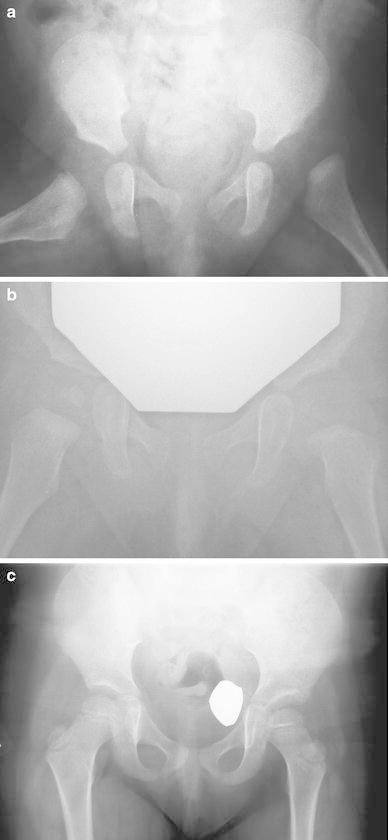
Series of films demonstrating the successful use of ligamentum teres transfer/tenodesis for correcting hip dislocation in a 4-month-old child who failed Pavlik harness treatment and closed reduction. a Dislocated left hip. b Film taken 6 months after Ludloff anterior approach plus ligamentum teres transfer. c Anterior-posterior (AP) view of the pelvis taken at 3 years follow-up (age 3.6 years)
Anterior open reduction that includes ligamentum teres transfer
Maintaining the ligamentum teres as a part of anterior open reduction is more challenging because of the poor visualization of the interior of the lower medial acetabular area. An additional medial incision is, therefore, necessary.
The anterior approach to the dislocated hip is performed using Salter’s method [9]. The hip capsule is opened in the usual T-shaped fashion with the ligamentum teres insertion carefully identified (Fig. 4a). The distal medial capsular opening is carried down to the transverse acetabular ligament.
Fig. 4.
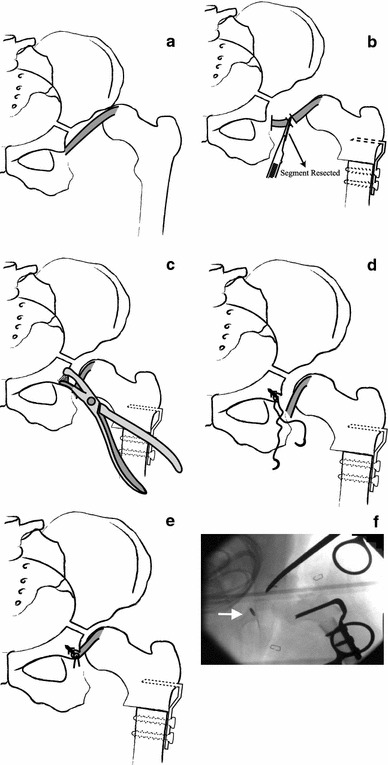
Series of drawings and radiographs demonstrating the technique for ligamentum teres transfer/tenodesis via an anterior approach to the hip. a Hip in dislocated position with an elongated ligamentum teres. b Detaching the elongated ligamentum teres from inside the inferior acetabulum (via separate medial adductor incision—similar approach as in a Ludloff procedure). An appropriate segment of ligamentum teres (often of size 1.5 cm) is excised. The femur has been shortened and de-rotated. c Use of a rongeur to create an area of decorticated bone at the antero-inferior border of the acetabulum ( arrow designates the proposed re-attachment site). d A suture anchor has been placed in the antero-inferior acetabulum just anterior and medial to the transverse acetabular ligamentum insertion. e The shortened ligamentum teres is attached to the suture anchor with the femoral head reduced. f Photograph of an intraoperative radiograph in a typical case with a suture anchor placed ( arrow)
Rather than excising the ligament, it is left intact on the femoral head and is followed down to its origin in the area of the transverse acetabular ligament. The ligament can either be sectioned at its acetabular origin at this time, or can be left attached until the separate medial incision has been made. If it is detached, a long suture tag is placed to make medial passage easier. (It should be noted that, in a few older children with DDH (often after the age of 3–4 years), the ligamentum teres may have spontaneously avulsed from the femoral insertion, making transfer impossible).
In the typical case (with the ligamentum insertion intact), at this stage, the femoral derotational shortening osteotomy is performed, which brings the femoral head into a more easily reduced position. A small groin incision is then made similar to that described for the Ludloff approach. The hip capsule is further opened inferiorly and the ligamentum teres is detached from its acetabular origin (alternatively, one could have already detached it via the anterior approach).
The detached ligament is grasped with a Kocher clamp, allowing the femoral head to be pulled medially and inferiorly into the true acetabulum. The ligament is then shortened (often by 1–2 cm) to allow normal tension at its new length (Fig. 4b). At this point, all remaining steps of the anterior approach are completed, including capsulorrhaphy and, if planned, concomitant femoral and/or acetabular osteotomies. This leaves re-attachment of the ligamentum teres as the final step in stabilizing the hip.
A rongeur is used to remove a small notch of cortical bone just anterior to the labrum at the anterior-inferior edge of the acetabulum (Fig. 4c). If one were to view the left acetabulum from the straight lateral view, this notching of the acetabulum is performed at approximately the 8 o’clock position. Initially, we simply sutured the shortened ligament into the periosteum in this area, but we now use a suture anchor for the re-attachment.
The suture anchor is introduced into the acetabular bone via this notched area, aiming about 30° towards the mid-line of the body to avoid acetabular penetration (Fig. 4d). The shortened ligamentum teres is then firmly re-attached by means of the suture anchor with the femoral head in the reduced position (Fig. 4e, f).
In comparison to a typical anterior open reduction, approximately 20 additional minutes are needed for ligament shortening and transfer. The post-operative spica cast and management are identical to that used for standard anterior open reductions.
Results
The patient data is shown in Table 1. We treated 23 hips (21 patients), including 12 hips with DDH, that had the procedure as part of an isolated medial Ludloff approach. Eleven hips had ligamentum teres transfer as part of an anterior open reduction of the hip, including osteotomies of either the femur and/or acetabulum, as well as capsulorrhaphy. In the anterior approach group, four had DDH, four had CP, two had myelomeningocele, and one had hip dislocation following a limb-lengthening procedure for proximal focal femoral deficiency.
Table 1 .
Patients treated with ligamentum teres transfer
| Patient | Sex | Diagnosis | Age at surgery | Surgical side | Concomitant procedures | Treatment prior to surgery |
|---|---|---|---|---|---|---|
| Medial approach | ||||||
| 1 | F | DDH | 5 months | Bilateral | T | H |
| 2 | F | DDH | 4 months | Left | A, T | H |
| 3 | F | DDH | 3 months | Left | T | H |
| 4 | M | DDH | 6 months | Left | A, T | H |
| 5 | M | DDH | 5 months | Bilateral | A, T | H |
| 6 | F | DDH | 15 months | Right | A, T | H |
| 7 | F | DDH | 2 months | Right | A, T | H |
| 8 | F | DDH | 6 months | Right | A, T | H |
| 9 | F | DDH | 2 months | Left | A, T | H |
| 10 | F | DDH | 21 months | Left | A, T, F | H |
| Anterior approach | ||||||
| 11 | F | DDH | 22 months | Left | T, F, P, C | None |
| 12 | M | DDH | 3.9 years | Left | T, F, P, C | P |
| 13 | F | DDH | 2.3 years | Right | T, F, P, C | None |
| 14 | F | DDH | 3.1 years | Left | T, F, P, C | None |
| 15 | M | CP | 4.5 years | Right | T, F, P, C | None |
| 16 | F | CP | 6.8 years | Left | T, F, P, C | None |
| 17 | F | CP | 13.9 years | Left | T, F, P, C | T, F |
| 18 | F | CP | 3.3 years | Right | T, F, P, C | T |
| 19 | F | Myelomeningocele | 2.6 years | Left | T, F, P, C | None |
| 20 | M | Myelomeningocele | 2.2 years | Left | T, F, P, C | None |
| 21 | M | PFFD | 8.2 years | Left | T, F, P, C | Limb lengthening (PFFD) |
PFFD proximal focal femoral deficiency, T tenotomy, A arthrogram, F femoral osteotomy, P pelvic osteotomy, C capsulorrhaphy, H Pavlik harness
The mean age at surgery for the entire group was 2.8 years (range 1.9 months to 13.9 years). For the DDH patients who underwent medial open reduction only, the mean age at surgery was 7.0 months (range 1.9–20.9 months). For the anterior reduction group, the mean age at surgery was 4.8 years (range 22.2 months to 13.9 years). All patients had a minimum one-year follow-up period. The mean post-operative follow-up period for the entire group was 33.4 months (range 1–9 years).
Concomitant procedures
Concomitant surgical procedures performed at the time of open reduction and ligamentum transfer are also listed in Table 1. Ten of the 12 hips with DDH that underwent medial open reduction had an arthrogram prior to reduction, which confirmed the failure of closed reduction. The other two failed closed reduction due to an unacceptable “safe zone” (too much abduction required to stabilize the hip).
All patients who had ligamentum teres transfer in the setting of anterior open reduction underwent concomitant femoral and pelvic osteotomy plus capsulorrhaphy. The type of femoral and pelvic osteotomy performed was based on surgeon preference and the nature of the case.
Clinical outcomes
There were no clinical post-operative complications noted in this series, with all patients noted to be pain-free at the most recent follow-up. In the DDH medial approach group, all had excellent hip motion without a limp. Two patients in the anterior open reduction group had a mild limp at the latest follow-up. One of these patients had undergone multiple procedures for DDH (#12), while the other (#14) had presented at an older age (3 years) for treatment.
Secondary procedures
One DDH patient who had a medial open reduction (#10) required subsequent acetabuloplasty two years later due to residual acetabular dysplasia. Seven of the 11 patients in the combined anterior/medial group underwent subsequent implant removal from the femoral or acetabular osteotomy sites.
Radiographic outcomes
The radiographic data is shown in Table 2.
Table 2.
Radiographic data
| Patient | Sex | Diagnosis | Pre-op. AI | Pre-op. Tonnis gradea | Post-op. AI | Post-op. superior centering ratio | Post-op. lateral centering ratio | Post-op. CEA | Post-op. MP | Post-op. AVN |
|---|---|---|---|---|---|---|---|---|---|---|
| Medial approach | ||||||||||
| 1 | F | DDH | 38 (R), 33 (L) | 4 (R), 3 (L) | 24 (R), 25 (L) | 0.17 (R), 0.14 (L) | 0.80 (R), 0.81 (L) | N/A | N/A | None |
| 2 | F | DDH | 39 | 2 | 17 | 0.13 | 0.65 | N/A | N/A | None |
| 3 | F | DDH | 40 | 3 | 27 | 0.15 | 0.91 | N/A | N/A | Yes (type 4)b |
| 4 | M | DDH | 35 | 4 | 34 | 0.11 | 0.6 | N/A | N/A | None |
| 5 | M | DDH | 32 (R), 30 (L) | 4 (R), 3 (L) | 29 (R), 27 (L) | 0.16 (R), 0.16 (L) | 0.76 (R), 0.76 (L) | N/A | N/A | None |
| 6 | F | DDH | 33 | 2 | 32 | 0.18 | 0.9 | N/A | N/A | None |
| 7 | F | DDH | 35 | 3 | 21 | 0.21 | 0.73 | N/A | N/A | None |
| 8 | F | DDH | 21 | 4 | 15 | 0.19 | 0.67 | N/A | N/A | None |
| 9 | F | DDH | 38 | 2 | 28 | 0.22 | 0.78 | N/A | N/A | None |
| 10 | F | DDH | 37 | 3 | 18 | 0.21 | 0.59 | N/A | N/A | None |
| Anterior approach | ||||||||||
| 11 | F | DDH | 48 | 3 | 16 | N/A | N/A | 43 | N/A | None |
| 12 | M | DDH | 21 | 2 | 15 | N/A | N/A | 37 | N/A | None |
| 13 | F | DDH | 40 | 4 | 19 | N/A | N/A | 32 | N/A | None |
| 14 | F | DDH | 37 | 3 | 15 | N/A | N/A | 38 | N/A | None |
| 15 | M | CP | 20 | N/A | 9 | N/A | N/A | 36 | 0 | None |
| 16 | F | CP | 25 | N/A | 4 | N/A | N/A | 51 | 0 | None |
| 17 | F | CP | 43 | N/A | 19 | N/A | N/A | 35 | 0 | None |
| 18 | F | CP | 33 | N/A | 19 | N/A | N/A | 21 | 0.12 | None |
| 19 | F | Myelomeningocele | 33 | N/A | 21 | N/A | N/A | 43 | 0 | None |
| 20 | M | Myelomeningocele | 35 | N/A | 10 | N/A | N/A | 30 | 0 | None |
| 21 | M | PFFD | 10 | N/A | 7 | N/A | N/A | 40 | 0.15 | None |
At the latest follow-up, no patient in the study had radiographic evidence of subluxation (as determined by a break in Shenton’s line) or dislocation. One patient (#3) who underwent medial open reduction for DDH at the age of 6 months had mild AVN of the femoral head at 25 months post-operatively (Ogden–Bucholz type 4) [20].
For the DDH patients who underwent medial open reduction, the pre-operative Tonnis grading [17] of dislocation was as follows: grade 2 in three hips, grade 3 in five hips, and grade 4 in four hips. For these patients, the mean post-operative superior centering ratio was 0.18 ± 0.04, with normal values being 0.1–0.2, as described by Smith et al. [22]. The mean post-operative lateral centering ratio was 0.74 ± 0.12, with normal values being 0.60–0.85 [22].
In the four patients with DDH who underwent an anterior approach with ligamentum teres transfer, the mean acetabular index was 36.5 ± 11.3 pre-operatively and 16.3 ± 1.9 post-operatively. The mean CEA at the latest follow-up was 37.5 ± 4.5°.
Of the seven patients who underwent an anterior approach with ligamentum teres transfer for conditions other than DDH, two had a migration percentage greater than zero at the latest follow-up. Neither had a break in Shenton’s line, and neither have required secondary procedures on the hip. The mean post-operative CEA for this group was 36.0 ± 10.4°.
Discussion
Re-dislocation after the surgical open reduction of infantile and early childhood hip dislocation remains a common problem, greatly distressing both the operating surgeon and the parents of the child. Evidence for its frequency includes the multitude of immediate post-operative imaging studies (computed tomography [CT] scans, magnetic resonance imaging [MRI] studies) designed to detect re-dislocation. Residual instability may be of particular concern following medial open reduction for DDH, since no capsulorrhaphy is performed. Kiely et al. [13] reported three repeat dislocations out of 49 hips reduced through a medial approach and repeat dislocations have been reported in other similar series [14, 26]. Although with anterior open reduction improved surgical stabilizing techniques have been employed (capsulorrhaphy, femoral and acetabular osteotomy), re-dislocation can still occur, thus, fueling our interest in maintaining the ligamentum teres as a stabilizer.
The anatomical, histological, and vascular characteristics of the ligamentum teres have been well-studied [1–4]. Based on cadaveric studies, the acetabular origin of the ligament has consistent attachments to the ischium from both sides of the cotyloid fossa, and to the medial side of the transverse acetabular ligament with a distinct insertion at the fovea of the femoral head [3]. The ligamentum teres carries an artery which appears to have a minimal contribution to the blood supply of the head itself [1]. Under normal circumstances, the ligamentum teres is conical in shape, and is taut when the hip is in flexion, adduction, and external rotation [27].
Previous animal studies have suggested the importance of the ligamentum teres in stabilizing the hip joint. Smith et al. [6] found a higher rate of hip dislocation in dogs in which the ligamentum teres was removed. Similarly, the effect of the ligamentum teres on chick hip joint stability was investigated by Li et al. [7], who found a significantly greater rate of hip dislocation when the ligamentum teres was cut. In a recent study from our institution, biomechanical studies of the porcine ligamentum teres found the ligament to have a mean ultimate load of 882 ± 168 N [8]. This was comparable to that of the human anterior cruciate ligament, which has been found to have an ultimate load ranging from 633 to 814 N [28, 29]. Although these findings characterize the strength of the ligamentum teres and its potential importance as a hip stabilizer, the exact biomechanical role of this ligament in the human hip remains poorly understood.
The structure and histology of the ligamentum teres in DDH has been described by several authors [3–5, 30, 31]. Ippolito et al. [3] examined the ligamentum teres in 12 surgical biopsies from children with DDH. On gross examination, they found that the ligament was longer and thicker than normal in most of the specimens. Their histologic analysis revealed cell atrophy and cartilaginous metaplasia in the ligamentum teres of younger children with DDH, and they theorized that these changes may lead to rupture of the ligament, which is seen at surgery in some cases. Michaels and Matles [5] also studied the ligamentum teres in DDH, and also noted that it is generally hypertrophied and elongated. However, they stated that the ligamentum teres exerts “ball and chain control” on the femoral head, which may spontaneously reduce a congenitally dislocated hip.
While these studies show that the ligamentum teres in DDH is abnormal, they do not exclude a role for the ligament to enhance stability during surgery for open reduction. In the literature describing open reduction of the hip in DDH, the predominant description of the ligamentum teres has been as a potential obstruction to concentric reduction. Numerous authors have recommended excision of the ligamentum teres during open reduction, especially if it appears hypertrophic [9–11]. Salter [9] advised that the hypertrophic ligamentum teres should be excised when performing an anterior open reduction in the dislocated hip, and advised that the ligament (after detachment from the femoral head) should be used as a guide to find the transverse acetabular ligament at the base of the acetabulum. The transverse acetabular ligament was then sectioned to allow room for the femoral head to be reduced in the depth of the true acetabulum.
It has become almost standard practice for the ligamentum teres to then be excised, with the transverse acetabular ligament sectioned prior to reduction of the femoral head. Morcuende et al., in their series of hips undergoing medial open reduction for DDH, found the ligamentum teres to be an obstacle to reduction and excised it in 87 of 93 hips [26].
The early clinical and radiographic results in the current study showed no residual subluxation or re-dislocation, indicating that the ligamentum teres may be a useful adjunct for stability in pediatric hip procedures. In the group of DDH patients who underwent medial open reduction with ligamentum teres transfer, the mean post-operative Smith centering ratios indicated good post-operative position of the femoral head. In addition, a mean overall improvement in the acetabular index was noted for all patient subgroups.
One hip out of the 12 that underwent medial open reduction with ligamentum teres transfer for DDH showed radiographic evidence of AVN at the latest follow-up. This AVN rate is comparable to that reported in other series of medial open reduction for DDH [13, 14, 26].
No head shape changes or “reverse break” in Shenton’s line were noted (which could occur if the ligament was shortened too much or sutured too tightly). Further follow-up will be needed to assess this issue, since we do not know how the ligament will grow (in both length and width) after shortening and re-insertion.
Although we do not have adequate data to compare the results of this method with our previous experience, we developed the ligamentum teres maintaining procedure because of early re-dislocations (at least one annually) that we experienced in our center, as well as having multiple cases of early “in cast” re-dislocation referred to us from other centers.
Summary
Although controversy remains regarding the evolutionarily determined stabilizing role of the ligamentum teres in the human hip, its size and strength suggest that it should be maintained in surgical reconstructions performed to stabilize a hip in childhood. In this series of 23 hips, with a minimum follow-up of one year, we found no residual subluxation or dislocation in either the Ludloff anteromedial approach group or in those reduced by anterior open reduction.
Based on these early positive results, we recommend that the technique presented be used in children treated with medial (Ludloff) open reduction. Techniques are evolving that allow ligament transfer as part of anterior open reduction as well. We have noted no negative sequelae from the procedure; however, long-term follow-up will be required to confirm the ultimate femoral head and acetabular development.
References
- 1.Trueta J, Harrison MHM. The normal vascular anatomy of the femoral head in adult man. J Bone Joint Surg Br. 1953;35:442–461. doi: 10.1302/0301-620X.35B3.442. [DOI] [PubMed] [Google Scholar]
- 2.Chen HH, Li AFY, Li KC, Wu JJ, Chen TS, Lee MC. Adaptations of ligamentum teres in ischemic necrosis of human femoral head. Clin Orthop Relat Res. 1996;328:268–275. doi: 10.1097/00003086-199607000-00041. [DOI] [PubMed] [Google Scholar]
- 3.Ippolito E, Ishi Y, Ponseti IV. Histologic, histochemical, and ultrastructural studies of the hip joint capsule and ligamentum teres in congenital dislocation of the hip. Clin Orthop Relat Res. 1980;146:246–258. [PubMed] [Google Scholar]
- 4.Calandriello B, Mignani G. The role of the ligamentum teres in congenital dislocation of the hip. Clin Orthop Relat Res. 1962;22:60–72. [Google Scholar]
- 5.Michaels G, Matles AL. The role of the ligamentum teres in congenital dislocation of the hip. Clin Orthop Relat Res. 1970;71:199–201. [PubMed] [Google Scholar]
- 6.Smith WS, Coleman CR, Olix ML, Slager RF. Etiology of congenital dislocation of the hip: an experimental approach to the problem using young dogs. J Bone Joint Surg Am. 1963;45:491–500. [Google Scholar]
- 7.Li AFY, Li KC, Chen HH, Chen TC, Wu JJ, Hsu HC, Lo WH (1993) Biomechanical functions of ligamentum teres. In: Proceedings of the 14th International Society of Biomechanics (ISB) Congress, Paris, France, July 1993
- 8.Wenger D, Miyanji F, Mahar A, Oka R. The mechanical properties of the ligamentum teres: a pilot study to assess its potential for improving stability in children’s hip surgery. J Pediatr Orthop. 2007;27(4):408–410. doi: 10.1097/01.bpb.0000271332.66019.15. [DOI] [PubMed] [Google Scholar]
- 9.Salter RB. Innominate osteotomy in the treatment of congenital dislocation and subluxation of the hip. J Bone Joint Surg Br. 1961;43:518–539. [PubMed] [Google Scholar]
- 10.Galpin RD, Roach JW, Wenger DR, Herring JA, Birch JG. One-stage treatment of congenital dislocation of the hip in older children, including femoral shortening. J Bone Joint Surg Am. 1989;71:734–741. [PubMed] [Google Scholar]
- 11.Weinstein SL, Ponseti IV. Congenital dislocation of the hip. Open reduction through a medial approach. J Bone Joint Surg Am. 1979;61:119–124. [PubMed] [Google Scholar]
- 12.Mubarak SJ, Valencia FG, Wenger DR. One-stage correction of the spastic dislocated hip. Use of pericapsular acetabuloplasty to improve coverage. J Bone Joint Surg Am. 1992;74:1347–1357. [PubMed] [Google Scholar]
- 13.Kiely N, Younis U, Day JB, Meadows TM. The Ferguson medial approach for open reduction of developmental dysplasia of the hip. A clinical and radiological review of 49 hips. J Bone Joint Surg Br. 2004;86:430–433. doi: 10.1302/0301-620X.86B3.14064. [DOI] [PubMed] [Google Scholar]
- 14.Konigsberg DE, Karol LA, Colby S, O’Brien S. Results of medial open reduction of the hip in infants with developmental dislocation of the hip. J Pediatr Orthop. 2003;23:1–9. [PubMed] [Google Scholar]
- 15.Weinstein SL. Congenital hip dislocation. Long-range problems, residual signs, and symptoms after successful treatment. Clin Orthop Relat Res. 1992;281:69–74. [PubMed] [Google Scholar]
- 16.McCluskey WP, Basset GS, Mora-Garcia G, MacEwen GD. Treatment of failed open reduction for congenital dislocation of the hip. J Pediatr Orthop. 1989;9:633–639. doi: 10.1097/01241398-198911000-00001. [DOI] [PubMed] [Google Scholar]
- 17.Tonnis D. Congenital dysplasia and dislocation of the hip in children and adults. Berlin: Springer; 1987. [Google Scholar]
- 18.McNerney NP, Mubarak SJ, Wenger DR. One-stage correction of the dysplastic hip in cerebral palsy with the San Diego acetabuloplasty: results and complications in 104 hips. J Pediatr Orthop. 2000;20:93–103. [PubMed] [Google Scholar]
- 19.Mau H, Dörr WM, Henkel L, Lutsche J. Open reduction of congenital dislocation of the hip by Ludloff’s method. J Bone Joint Surg Am. 1971;53:1281–1288. [PubMed] [Google Scholar]
- 20.Bucholz R, Ogden J (1978) Patterns of ischemic necrosis of the proximal femur in nonoperatively treated congenital hip diseases. In: Nelson CL (ed) The hip: Proceedings of the 6th Open Scientific Meeting of the Hip Society. CV Mosby, St. Louis p 43
- 21.Wiberg G. Studies on dysplastic acetabular and congenital subluxation of the hip joint with special reference to the complication of osteoarthritis. J Bone Joint Surg Am. 1933;15:6. [Google Scholar]
- 22.Smith WS, Badgley CE, Orwig JB, Harper JM. Correlation of postreduction roentgenograms and thirty-one-year follow-up in congenital dislocation of the hip. J Bone Joint Surg Am. 1968;50(6):1081–1098. [PubMed] [Google Scholar]
- 23.Reimers J. The stability of the hip in children. A radiological study of the results of muscle surgery in cerebral palsy. Acta Orthop Scand Suppl. 1980;184:1–100. doi: 10.3109/ort.1980.51.suppl-184.01. [DOI] [PubMed] [Google Scholar]
- 24.Sharrard WJ, Allen JM, Heaney SH. Surgical prophylaxis of subluxation and dislocation of the hip in cerebral palsy. J Bone Joint Surg Br. 1975;57(2):160–166. [PubMed] [Google Scholar]
- 25.Ludloff K. The open reduction of the congenital hip dislocation by an anterior incision. Am J Orthop Surg. 1913;10:438–454. [Google Scholar]
- 26.Morcuende JA, Meyer MD, Dolan LA, Weinstein SL. Long-term outcome after open reduction through an anteromedial approach for congenital dislocation of the hip. J Bone Joint Surg Am. 1997;79(6):810–817. doi: 10.2106/00004623-199706000-00002. [DOI] [PubMed] [Google Scholar]
- 27.Gray AJR, Villar RN. The ligamentum teres of the hip: an arthroscopic classification of its pathology. Arthroscopy. 1997;13:575–578. doi: 10.1016/S0749-8063(97)90182-1. [DOI] [PubMed] [Google Scholar]
- 28.Kennedy JC, Hawkins RJ, Willis RB, Danylchuck KD. Tension studies of human knee ligaments. Yield point, ultimate failure, and disruption of the cruciate and tibial collateral ligaments. J Bone Joint Surg Am. 1976;58:350–355. [PubMed] [Google Scholar]
- 29.Trent PS, Walker PS, Wolf B. Ligament length patterns, strength, and rotational axes of the knee joint. Clin Orthop Relat Res. 1976;117:263–270. [PubMed] [Google Scholar]
- 30.McKibbin B. Anatomical factors in the stability of the hip joint in the newborn. J Bone Joint Surg Br. 1970;52:148–159. [PubMed] [Google Scholar]
- 31.Sarban S, Baba F, Kocabey Y, Cengiz M, Isikan UE. Free nerve endings and morphological features of the ligamentum capitis femoris in developmental dysplasia of the hip. J Pediatr Orthop B. 2007;16(5):351–356. doi: 10.1097/01.bpb.0000243830.99681.3e. [DOI] [PubMed] [Google Scholar]